Monthly Archives: July 2021
I have often warned that, even if chiropractic manipulations were harmless (which they are clearly not), this would not necessarily apply to those who administer them, the chiropractors. They can do harm via interfering or advising against conventional interventions (the best-research example is immunization) or by treating conditions that they are not competent to tackle (like ear infections), or giving advice that endangers the health of the patient.
Italian authors reported the case of a 67-year-old woman, who had been suffering from low back pain due to herniated discs, decided to undergo chiropractic treatment. According to the chiropractor’s prescription, the patient drank about 8 liters of water in a day. During the afternoon, she developed headaches, nausea, vomiting, and fatigue, for which reason she consulted the chiropractor, who reassured the patient and suggested continuing the treatment in order to purify the body. The next day, following the intake of another 6 liters of water, the patient developed sudden water retention, loss of consciousness, and tonic-clonic seizures; for this reason, she was admitted to the Intensive Care Unit with a coma from electrolyte alterations.
The diagnosis of water intoxication was stated based on the history reported by the family members; according to the clinical findings, the hydro-electrolytic alterations were adequately corrected, allowing the disease resolution. Once resolved the intoxication, the patient underwent surgery to treat a shoulder dislocation and a humerus fracture which occurred due to a fall consequent to the tonic-clonic seizures.
The Judicial Authority thus ordered a medico-legal evaluation of the chiropractor’s behavior in order to identify any professional liability issue.
The Italian authors commented that this case is peculiar since it shows the dangerous implications for the patients’ health and safety deriving from the prescription of a large quantity of water intake, without any control by the chiropractor, and thus underestimating the risks of such a practice, as evidenced by the suggestion to continue the water intake aiming to detoxify the body from pharmacological substances. As a consequence, the patient developed a severe form of hyponatremia, leading to life-threatening complications that could have been otherwise avoided.
The medico-legal evaluation of the case led to the admission of professional liability of the chiropractor, who
thus had to pay the damages to the patient.
It is, of course, tempting to argue that the patient was not very clever to follow this ridiculous advice (and that the chiropractor was outright stupid to give it). One might even go further and argue that most patients trusting chiros are not all that smart … one could … but it is far from me to do so.
Chinese researchers evaluated the effect of Chinese medicine (CM) on survival time and quality of life (QoL) in patients with small-cell lung cancer (SCLC). They conducted an exploratory and prospective clinical observation. Patients diagnosed with SCLC receiving CM treatment as an add-on to conventional cancer therapies were included and followed up every 3 months. The primary outcome was overall survival (OS), and the secondary outcomes were progression-free survival (PFS) and QoL.
A total of 136 patients including 65 limited-stage SCLC (LS-SCLC) patients and 71 extensive-stage SCLC (ES-SCLC) patients were analyzed. The median OS of ES-SCLC patients was 17.27 months, and the median OS of LS-SCLC was 40.07 months. The survival time was 16.27 months for SCLC patients with brain metastasis, 9.83 months for liver metastasis, 13.43 months for bone metastasis, and 18.13 months for lung metastasis. Advanced age, pleural fluid, liver, and brain metastasis were risk factors, while longer CM treatment duration was a protective factor. QoL assessment indicated that after 6 months of CM treatment, scores increased in function domains and decreased in symptom domains.
The authors concluded that CM treatment might help prolong OS of SCLC patients. Moreover, CM treatment brought the trend of symptom amelioration and QoL improvement. These results provide preliminary evidence for applying CM in SCLC multi-disciplinary treatment.
Sorry, but these results provide NO evidence for applying CM in SCLC multi-disciplinary treatment! Even if the findings were a bit better than those reported for SCLC in the literature – and I am not sure they are – it is simply not possible to say with any degree of certainty what effect the CM had. For that, we would obviously need a proper control group.
The study was supported by the National Natural Science Foundation of China (No. 81673797), and Beijing Municipal Natural Science Foundation (No. 7182142). In my view, this paper is an example for showing how the relentless promotion of dubious Traditional Chinese Medicine by Chinese officials might cost lives.
I feel that it is time to do something about it.
But what precisely?
Any ideas anyone?
By guest blogger Hans-Werner Bertelsen
Veronika Hackenbroch wrote in an article for the German news website Der Spiegel about clusters of cases where children were born with severe birth deformities. (1) The only common factor that researchers in the Paediatrics department of the University Medical Center Mainz were able to identify through intensive communication with the mothers was that they had all visited a dentist whilst pregnant. The fetus is particularly sensitive to exogenous stimuli during early pregnancy, which is why this period is also known as the “teratogenetic determination period” (Koberg).
The data regarding the workplace exposure limit for mercury is outdated – it is based on information collected about 50 years ago in some cases. Since that time, there have been considerable advances, in particular in the fields of measuring technology and analysis. Unfortunately, these advances have yet to be utilized to provide meaningful figures on exposure to mercury vapour when removing old fillings or drilling into teeth with mercury amalgam fillings for the purpose of acute pain management. In addition to patient protection, the focus when processing existing mercury amalgam fillings is therefore also on occupational health and safety. This has not gone unnoticed by many female employees in dental surgeries that mercury amalgam can pose serious risks to unborn children. For example, a study in Norway reported an increased risk of perinatal death associated with a high number of mercury amalgam fillings. (2)
Sylvia Gabel from the German Association of Medical Professions (Verband medizinischer Fachberufe e.V.) even called for an immediate ban on toxic mercury amalgam: “Vapours pose a danger to dental professionals’ health!”. Mrs Gabel added: “The processing of amalgam in dental surgery releases mercury vapour. As 99 per cent of the dental nurses and hygienists in Germany are female and mercury has harmful effects on both fertility and the unborn child, we are exposed to a particular risk.”(3)
Researchers in Norway documented a considerable increase in the concentration of mercury in the blood after the removal of fillings as far back as 2006. (4) Toxicologists are in unanimous agreement that these peaks, which are the result of inhalation, are extremely harmful and may well have a teratogenetic effect in early pregnancy. (5) Consequently, what I am calling for is this: until such time as we know how high the mercury vapour concentrations are and as long as we “remain in the dark”, we should refrain from removing existing fillings containing mercury and performing dental drilling procedures in women of child-bearing age for ethical reasons so as to exclude the risk of deformities (see Der Spiegel article: “Waren die Schwangeren beim Zahnarzt?”, V. Hackenbroch, 20.09.19). (6)
An immediate ban on the use of mercury amalgam would be advantageous not solely with regard to the exposure to toxins of cancer patients, as the field of “alternative medicine” often recommends expensive, unnecessary and subsequently also very harmful “detox” treatments. (7) A more than questionable business from an ethical perspective: cancer patients are often looking for additional, so-called complementary therapy methods. This often sees them fall into the clutches of healers and doctors, who have no dental expertise but can identify mercury amalgam fillings very easily due to their dark colour. As I myself experienced in a so-called “alternative” dental surgery, the frightened patients, who are often in the middle of chemotherapy cycles, are then informed that they absolutely must have the mercury amalgam removed and then undergo a “detoxification therapy”. Introjects are not spared in the process: “Your body, already devastated by the chemotherapy, should not be subjected to additional chemicals.” Of course, this “detoxification” will be performed (with maximum consideration!) as a “homoeopathic” therapy. I had to observe this very lucrative “business model” often enough – and not once has a cancer patient objected. Once they fall under the charlatan’s spell, patients will allow themselves to be treated with all manner of things. Even live cells. In one patient, a single mother of two, this method triggered a fatal anaphylactic shock. (8) However, cancers and other chronic diseases are not the only reasons that bring patients with mercury amalgam fillings within the reach of dubious individuals with promises of salvation and charlatans. (9) An unfulfilled desire to have children has also led countless desperate women to ask to be parted irrevocably from their mercury-containing fillings. German health insurance companies approve these interventions, which appear logical from a toxicological perspective, and thus contribute not only to the replacement of the fillings but also to the release of mercury vapours and thus toxic peaks resulting from inhalation. Such actions can even have fatal consequences in the early stages of pregnancy.
However, the focus with mercury amalgam is not only on protecting patients from dishonest therapists and unnecessary teratogenetic risks – female staff could also benefit in general. For example, an immediate ban of the use of mercury amalgam could significantly increase job satisfaction among female employees in the dental surgery. According to Sylvia Gabel: “Strike measures were considered in the surgeries continuing use.”(10)
Each new mercury amalgam filling brings with it numerous side effects. It:
- – increases the risk of toxic exposure resulting from inhalation during removal;
- – increases the risk of corrosion products developing in the long term;
- – increases demand in the field of detox beliefs and homoeopathic charlatanry;
- – promotes the conspiracy narrative of “the dangers of conventional medicine”; and, in doing so,
- – often undermines patients’ confidence in treatments appropriate for the indication and, along with it, the often-vital compliance;
- – fills not only the cavity in the tooth but also the charlatans’ pockets.
I believe it is time to give dental health a helping hand with an intelligent combination of contemporary prevention concepts and harmless filling materials. Currently, the political will is merely a small seed. The seed must now germinate and grow.
REFERENCES
1. “Waren die Schwangeren beim Zahnarzt?”, V. Hackenbroch, 20.09.19 2. https://www.zwp-online.info/zwpnews/dental-news/wissenschaft-und-forschung/schwangerschaft-und-amalgam-risiken-bei-hohen-mengen 3. https://www.dzw.de/amalgam-ausstieg-ngo 4. https://pubmed.ncbi.nlm.nih.gov/29320025/
5. Prof. Eschenhagen, Toxicology Hamburg-Eppendorf in personal correspondence dated 23.01.2020 6. Comment dated 05.07. https://onkelmichael.blog/2021/07/03/ist-eine-entfernung-bestehender- amalgam-restaurationen-problemlos-und-bedenkenlos-durchfuhrbar/comment-page-1/? unapproved=4000&moderation-hash=d5b63e66f5045bfa12d829a88eddf1b0#comment- 4000 7. Prof. E. Ernst: https://www.theguardian.com/lifeandstyle/2014/dec/05/detox-myth-health-diet-science-ignorance 8. http://scienceblogs.de/kritisch-gedacht/2012/02/08/insider-bericht/
9. Prof. Jutta Hübner (Oncology, Jena) in personal correspondence dated 21.01.2020
10. Sylvia Gabel in personal correspondence dated 18.06.21
Prof Harald Walach has had a few rough weeks. First, he published his paper suggesting that Covid vaccinations do more harm than good which was subsequently retracted as flawed, if not fraudulent. Next, he published a paper showing that children are put in danger when wearing face masks suggesting that “decision-makers weigh the hard evidence produced by these experimental measurements accordingly, which suggest that children should not be forced to wear face masks.” Now, the journal put out the following announcement about it:
The Research Letter, “Experimental Assessment of Carbon Dioxide Content in Inhaled Air With or Without Face Masks in Healthy Children: A Randomized Clinical Trial,” by Harald Walach, PhD, and colleagues published online in JAMA Pediatrics on June 30, 2021,1 is hereby retracted.
Following publication, numerous scientific issues were raised regarding the study methodology, including concerns about the applicability of the device used for assessment of carbon dioxide levels in this study setting, and whether the measurements obtained accurately represented carbon dioxide content in inhaled air, as well as issues related to the validity of the study conclusions. In their invited responses to these and other concerns, the authors did not provide sufficiently convincing evidence to resolve these issues, as determined by editorial evaluation and additional scientific review. Given fundamental concerns about the study methodology, uncertainty regarding the validity of the findings and conclusions, and the potential public health implications, the editors have retracted this Research Letter.
To make things even worse, Walach’s University fired him because of his fraudulent anti-vax research. Poznan University of Medical Sciences tweeted on 6 July:
We wish to emphasize that the claims included in dr Harald Walach’s recent article in @Vaccines_MDPI do not represent the position of @PUMS_tweets . We find that the article lacked scientific diligence and proper methodology. Dr. Walach’s affiliation with PUMS was now terminated. Throughout the pandemic PUMS has actively promoted vaccination programs, offering scientific expertise in the media, broadcasting seminars, and reported on progress of the vaccination program. We consider vaccinations as the paramount tool in the global fight against the pandemic. We consider vaccinations as the paramount tool in the global fight against the #pandemic. Over 85% of our own academic community has already been vaccinated with support and encouragement from the University.
As I said, this is truly unlucky …
.. or perhaps not?
Come to think of it, it is lucky when pseudo-science and fraud are called out. It means that the self-cleaning mechanisms of science are working and we are protected from the harm done by charlatans.
Myofascial release (also known as myofascial therapy or myofascial trigger point therapy) is a type of low-load stretch therapy that is said to release tightness and pain throughout the body caused by the myofascial pain syndrome, a chronic muscle pain that is worse in certain areas known as trigger points. Various types of health professionals provide myofascial release, e.g. osteopaths, chiropractors, physical or occupational therapists, massage therapists, or sports medicine/injury specialists. The treatment is usually applied repeatedly, but there is also a belief that a single session of myofascial release is effective. This study was a crossover clinical trial aimed to test whether a single session of a specific myofascial release technique reduces pain and disability in subjects with chronic low back pain (CLBP).
A total of 41 participants were randomly enrolled into 3 situations in a balanced and crossover manner:
- experimental,
- placebo,
- control.
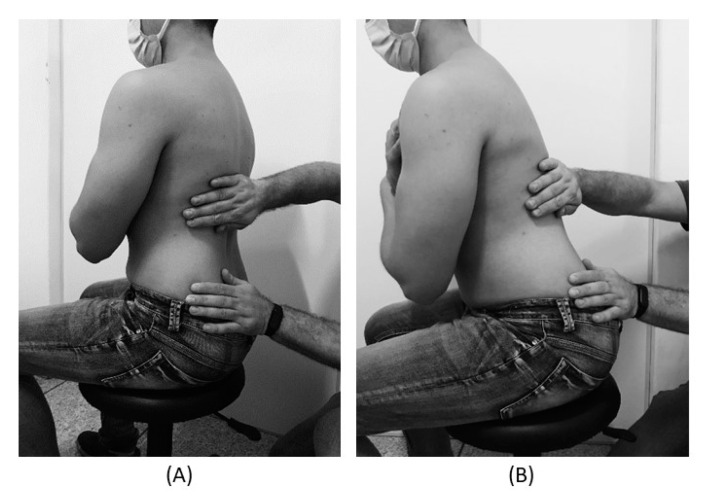
The subjects underwent a single session of myofascial release on thoracolumbar fascia and the results were compared with the control and placebo groups. A single trained and experienced therapist applied the technique.
For the control treatment, the subjects were instructed to remain in the supine position for 5 minutes. For the muscle release session, the subjects were in a sitting position with feet supported and the thoracolumbar region properly undressed. The trunk flexion goniometry of each participant was performed and the value of 30° was marked with a barrier to limit the necessary movement during the technique. The trained researcher positioned their hands on all participants without sliding over the skin or forcing the tissue, with the cranial hand close to the last rib and at the T12–L1 level on the right side of the individual’s body and the caudal hand on the ipsilateral side between the iliac crest and the sacrum. Then, the researcher caused slight traction in the tissues by moving their hands away from each other in a longitudinal direction. Then, the participant was instructed to perform five repetitions of active trunk flexion-extension (30°), while the researcher followed the movement with both hands simultaneously positioned, without losing the initial tissue traction and position. The same technique and the same number of repetitions of active trunk flexion-extension were repeated with the researcher’s hands positioned on the opposite sides. This technique lasted approximately five minutes.
For the placebo treatment, the subjects were not submitted to the technique of manual thoracolumbar fascia release, but they slowly performed ten repetitions of active trunk flexion-extension (30°) in the same position as the experimental situation. Due to the fact that touch can provide not only well-recognized discriminative input to the brain, but also an affective input, there was no touch from the researcher at this stage.
The outcomes, pain, and functionality, were evaluated using the numerical pain rating scale (NPRS), pressure pain threshold (PPT), and Oswestry Disability Index (ODI).
The results showed no effects between-tests, within-tests, nor for interaction of all the outcomes, i.e., NPRS (η 2 = 0.32, F = 0.48, p = 0.61), PPT (η2 = 0.73, F = 2.80, p = 0.06), ODI (η2 = 0.02, F = 0.02, p = 0.97).
The authors concluded that a single trial of a thoracolumbar myofascial release technique was not enough to reduce pain intensity and disability in subjects with CLBP.
Surprised?
I’m not!
Recently, I received this comment from a reader:
Edzard-‘I see you do not understand much of trial design’ is true BUT I wager that you are in the same boat when it comes to a design of a trial for LBP treatment: not only you but many other therapists. There are too many variables in the treatment relationship that would allow genuine , valid criticism of any design. If I have to pick one book of the several listed elsewhere I choose Gregory Grieve’s ‘Common Vertebral Joint Problems’. Get it, read it, think about it and with sufficient luck you may come to realize that your warranted prejudices against many unconventional ‘medical’ treatments should not be of the same strength when it comes to judging the physical therapy of some spinal problems as described in the book.
And a chiro added:
EE: I see that you do not understand much of trial design
Perhaps it’s Ernst who doesnt understand how to research back pain.
“The identification of patient subgroups that respond best to specific interventions has been set as a key priority in LBP research for the past 2 decades.2,7 In parallel, surveys of clinicians managing LBP show that there are strong views against generic treatment and an expectation that treatment should be individualized to the patient.6,22.”
Journal of Orthopaedic & Sports Physical Therapy
Published Online:January 31, 2017Volume47Issue2Pages44-48
Do I need to explain why the Grieve book (yes, I have it and yes, I read it) is not a substitute for evidence that an intervention or technique is effective? No, I didn’t think so. This needs to come from a decent clinical trial.
And how would one design a trial of LBP (low back pain) that would be a meaningful first step and account for the “many variables in the treatment relationship”?
How about proceeding as follows (the steps are not necessarily in that order):
- Study the previously published literature.
- Talk to other experts.
- Recruit a research team that covers all the expertise you need (and don’t have yourself).
- Formulate your research question. Mine would be IS THERAPY XY MORE EFFECTIVE THAN USUAL CARE FOR CHRONIC LBP? I know LBP is but a vague symptom. This does, however, not necessarily matter (see below).
- Define primary and secondary outcome measures, e.g. pain, QoL, function, as well as the validated methods with which they will be quantified.
- Clarify the method you employ for monitoring adverse effects.
- Do a small pilot study.
- Involve a statistician.
- Calculate the required sample size of your study.
- Consider going multi-center with your trial if you are short of patients.
- Define chronic LBP as closely as you can. If there is evidence that a certain type of patient responds better to the therapy xy than others, that might be considered in the definition of the type of LBP.
- List all inclusion and exclusion criteria.
- Make sure you include randomization in the design.
- Randomization should be to groups A and B. Group A receives treatment xy, while group B receives usual care.
- Write down what A and B should and should not entail.
- Make sure you include blinding of the outcome assessors and data evaluators.
- Define how frequently the treatments should be administered and for how long.
- Make sure all therapists employed in the study are of a high standard and define the criteria of this standard.
- Train all therapists of both groups such that they provide treatments that are as uniform as possible.
- Work out a reasonable statistical plan for evaluating the results.
- Write all this down in a protocol.
Such a trial design does not need patient or therapist blinding nor does it require a placebo. The information it would provide is, of course, limited in several ways. Yet it would be a rigorous test of the research question.
If the results of the study are positive, one might consider thinking of an adequate sham treatment to match therapy xy and of other ways of firming up the evidence.
As LBP is not a disease but a symptom, the study does not aim to include patients that all are equal in all aspects of their condition. If some patients turn out to respond better than others, one can later check whether they have identifiable characteristics. Subsequently, one would need to do a trial to test whether the assumption is true.
Therapy xy is complex and needs to be tailored to the characteristics of each patient? That is not necessarily an unsolvable problem. Within limits, it is possible to allow each therapist the freedom to chose the approach he/she thinks is optimal. If the freedom needed is considerable, this might change the research question to something like ‘IS THAT TYPE OF THERAPIST MORE EFFECTIVE THAN THOSE EMPLOYING USUAL CARE FOR CHRONIC LBP?’
My trial would obviously not answer all the open questions. Yet it would be a reasonable start for evaluating a therapy that has not yet been submitted to clinical trials. Subsequent trials could build on its results.
I am sure that I have forgotten lots of details. If they come up in discussion, I can try to incorporate them into the study design.
Acupuncture is a veritable panacea; it cures everything! At least this is what many of its advocates want us to believe. Does it also have a role in supportive cancer care?
Let’s find out.
This systematic review evaluated the effects of acupuncture in women with breast cancer (BC), focusing on patient-reported outcomes (PROs).
A comprehensive literature search was carried out for randomized controlled trials (RCTs) reporting PROs in BC patients with treatment-related symptoms after undergoing acupuncture for at least four weeks. Literature screening, data extraction, and risk bias assessment were independently carried out by two researchers. The authors stated that they followed the ‘Preferred Reporting Items for Systematic Review and Meta-Analyses’ (PRISMA) guidelines.
Out of the 2, 524 identified studies, 29 studies representing 33 articles were included in this meta-analysis. The RCTs employed various acupuncture techniques with a needle, such as hand-acupuncture and electroacupuncture. Sham/placebo acupuncture, pharmacotherapy, no intervention, or usual care were the control interventions. About half of the studies lacked adequate blinding.
At the end of treatment (EOT), the acupuncture patients’ quality of life (QoL) was measured by the QLQ-C30 QoL subscale, the Functional Assessment of Cancer Therapy-Endocrine Symptoms (FACT-ES), the Functional Assessment of Cancer Therapy–General/Breast (FACT-G/B), and the Menopause-Specific Quality of Life Questionnaire (MENQOL), which depicted a significant improvement. The use of acupuncture in BC patients lead to a considerable reduction in the scores of all subscales of the Brief Pain Inventory-Short Form (BPI-SF) and Visual Analog Scale (VAS) measuring pain. Moreover, patients treated with acupuncture were more likely to experience improvements in hot flashes scores, fatigue, sleep disturbance, and anxiety compared to those in the control group, while the improvements in depression were comparable across both groups. Long-term follow-up results were similar to the EOT results. Eleven RCTs did not report any information on adverse effects.
The authors concluded that current evidence suggests that acupuncture might improve BC treatment-related symptoms measured with PROs including QoL, pain, fatigue, hot flashes, sleep disturbance and anxiety. However, a number of included studies report limited amounts of certain subgroup settings, thus more rigorous, well-designed and larger RCTs are needed to confirm our results.
This review looks rigorous on the surface but has many weaknesses if one digs only a little deeper. To start with, it has no precise research question: is any type of acupuncture better than any type of control? This is not a research question that anyone can answer with just a few studies of mostly poor quality. The authors claim to follow the PRISMA guidelines, yet (as a co-author of these guidelines) I can assure you that this is not true. Many of the included studies are small and lacked blinding. The results are confusing, contradictory and not clearly reported. Many trials fail to mention adverse effects and thus violate research ethics, etc., etc.
The conclusion that acupuncture might improve BC treatment-related symptoms could be true. But does this paper convince me that acupuncture DOES improve these symptoms?
No!
Two chiropractors conducted a retrospective review of publicly available data from the California Board of Chiropractic Examiners. Their aim was to determine categories of offense, experience, and gender of disciplined doctors of chiropractic (DC) in California and compare them with disciplined medical physicians in California.
Retrospective reviews of publicly available data from the California Board of Chiropractic Examiners.
The DC disciplinary categories, in descending order, were
- fraud (44%),
- sexual boundary issues (22%),
- other offences (13%),
- abuse of alcohol or drugs (10%),
- negligence or incompetence (6%),
- poor supervision (2%),
- mental impairment (.3%).
The authors concluded that the professions differ in the major reasons for disciplinary actions. Two thirds (67%) of the doctors of chiropractic were disciplined for fraud and sexual boundary issues, compared with 59% for negligence and substance misuse for medical physicians. Additional study in each profession may reveal methods to identify causes and possible intervention for those who are at high risk.
The two authors of this paper should be congratulated for their courage to publish such a review. These figures seem shocking. But I think that in reality some of them might be far higher. Take the important matter of competence, for instance. If you consider it competent that chiropractors treat conditions other than back pain, you might arrive at the above-mentioned figure of 6%. If you consider this as incompetent, as I do, the figure might be one order of magnitude higher (for more on unprofessional conduct by chiropractors see here).
The abstract of the paper does not provide comparisons to the data related to the medical profession. Here they are; relative to doctors, chiropractors are:
- 2x more likely to be involved in malpractice,
- 9x more likely to be practising fraud,
- 2x more likely to transgress sexual boundaries.
The frequency of fraud is particularly striking. Come to think of it, however, it is not all that amazing. I have said it before: chiropractic is in my view mostly about money.
It has been reported that B.C.’s chiropractors are deeply divided about the future of their profession, disagreeing on everything from false advertising to the use of routine X-rays.
Chiropractors attending an extraordinary general meeting of the College of Chiropractors of B.C. were split nearly down the middle on a series of non-binding resolutions addressing actions the College has taken in recent years. By the narrowest of margins, with at most 54% support, the members voted in favor of the college’s moves to limit the use of diagnostic X-rays and ban claims that aren’t supported by scientific evidence. The question that remains is who represents the bulk of the profession in B.C. — chiropractors advocating for what they describe as evidence-based practice targeting the musculoskeletal system, or “vitalists” who argue that chiropractic treatment can help with everything from immunity to brain function.
The modernizers see it as “a deliberate attempt to take over the college by a small group of chiropractors with no respect or knowledge of regulation … funded by organizations out of the province and out of the country,” Victoria chiropractor Clark Konczak told the virtual meeting.
At issue was a series of policies the college introduced in the wake of what Konczak called “the smoothie episode.” He was referring to a video posted on Facebook in 2017 by the then-vice chair of the college’s board, Avtar Jassal, in which he falsely suggested fruit smoothies are better than vaccines at preventing the flu.
Earlier this year, the college introduced amendments that bar chiropractors from performing routine and repeat X-rays, saying radiography is only scientifically supported when there are red flags that something is seriously wrong. The policy change on X-rays was the flashpoint in the long-simmering tension within the profession. A group of chiropractors has filed a petition in B.C. Supreme Court, alleging the college is preventing them from providing “safe, ethical, and effective care to their patients.” Their legal action has backing from national and international vitalistic organizations. During the recent meeting, a group of chiropractors argued unsuccessfully for the new X-ray policy to be tossed. Some suggested that chiropractors who don’t perform X-rays as a matter of routine are actually harming their patients. Another extraordinary general meeting has been called for July 20 to vote on resolutions calling for the removal of four college board members.
As I have often pointed out, chiropractic is all about money. The ‘chiro-wars’ have been going on for quite a while now, and they are by no means confined to B. C. or Canada. In a nutshell, they suggest to me that a significant proportion of chiropractors prefer money to progress.
Bernie Garrett is a professor of nursing at the University of British Columbia. He is being mentioned here because he has written a book entitled THE NEW ALCHEMISTS which deals (mostly) with so-called alternative medicine (SCAM). It is a well-written, informative, critical, and evidence-based text that I can recommend wholeheartedly. It will be available in the UK on 29 July but you can pre-order it already.
On Amazon, It is being advertised with the following words:

How to identify and see through deceptive and unethical health marketing practices Health scams come in all shapes and sizes-from the suppression of side-effects from prescription drugs to the unproven benefits of ‘traditional’ health practices-taking advantage of the human tendency to assume good intentions in others. So how do we avoid being deceived? Professor of Nursing, Bernie Garrett explores real-world examples of medical malpractice, pseudo and deceptive health science, dietary and celebrity health fads, deception in alternative medicine and problems with current healthcare regulation, ending with a simple health-scam detection kit. And he looks at how these practices and ineffective regulations affect our lives.
The book is written for the interested layperson. But I am sure that healthcare professionals will like it too, not least because it is fully referenced. Its aim is to inform and prevent consumers from being deceived and exploited by charlatans, an aim shared with this blog – while reading the book, I often got the impression that Bernie Garrett might be a regular reader of my blog.
This does not mean that I did not learn a lot from reading Bernie’s book. On the contrary, there was a lot that I did not know before and that is worth knowing. For instance, were you aware that you can earn a ‘Doctor of Naturopathic Medicine, Advanced Diploma’ or Reiki master qualification for $ 12.99 in a 6-hour online course (if you want to know where you’ll have to get Bernie’s book)? Well, I didn’t.
Yes, I did enjoy reading this book, and I share Bernie’s views on SCAM. In his overall conclusions, he writes: “The sad truth is, many health fraudsters are highly skilled manipulators, and do not always end up being held to account for their crimes, and many continue to profit from them.” Because this is so, it is good to have another splendid book that will help us in our struggle to inform the public responsibly.