
Updated Edition!
 for Cancer")





")









![]()

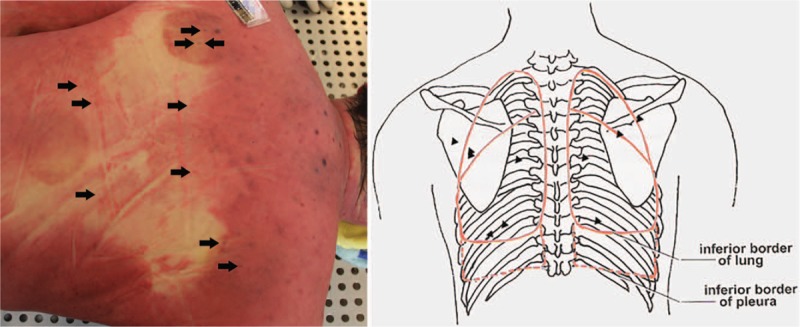
The most frequent of all potentially serious adverse events of acupuncture is pneumothorax. It happens when an acupuncture needle penetrates the lungs which subsequently deflate. The pulmonary collapse can be partial or complete as well as one or two sided. This new case-report shows just how serious a pneumothorax can be.
A 52-year-old man underwent acupuncture and cupping treatment at an illegal Chinese medicine clinic for neck and back discomfort. Multiple 0.25 mm × 75 mm needles were utilized and the acupuncture points were located in the middle and on both sides of the upper back and the middle of the lower back. He was admitted to hospital with severe dyspnoea about 30 hours later. On admission, the patient was lucid, was gasping, had apnoea and low respiratory murmur, accompanied by some wheeze in both sides of the lungs. Because of the respiratory difficulty, the patient could hardly speak. After primary physical examination, he was suspected of having a foreign body airway obstruction. Around 30 minutes after admission, the patient suddenly became unconscious and died despite attempts of cardiopulmonary resuscitation.
Whole-body post-mortem computed tomography of the victim revealed the collapse of the both lungs and mediastinal compression, which were also confirmed by autopsy. More than 20 pinprick injuries were found on the skin of the upper and lower back in which multiple pinpricks were located on the body surface projection of the lungs. The cause of death was determined as acute respiratory and circulatory failure due to acupuncture-induced bilateral tension pneumothorax.
The authors caution that acupuncture-induced tension pneumothorax is rare and should be recognized by forensic pathologists. Postmortem computed tomography can be used to detect and accurately evaluate the severity of pneumothorax before autopsy and can play a supporting role in determining the cause of death.
The authors mention that pneumothorax is the most frequent but by no means the only serious complication of acupuncture. Other adverse events include:
- central nervous system injury,
- infection,
- epidural haematoma,
- subarachnoid haemorrhage,
- cardiac tamponade,
- gallbladder perforation,
- hepatitis.
No other possible lung diseases that may lead to bilateral spontaneous pneumothorax were found. The needles used in the case left tiny perforations in the victim’s lungs. A small amount of air continued to slowly enter the chest cavities over a long period. The victim possibly tolerated the mild discomfort and did not pay attention when early symptoms appeared. It took 30 hours to develop into symptoms of a severe pneumothorax, and then the victim was sent to the hospital. There he was misdiagnosed, not adequately treated and thus died. I applaud the authors for nevertheless publishing this case-report.
This case occurred in China. Acupuncturists might argue that such things would not happen in Western countries where acupuncturists are fully trained and aware of the danger. They would be mistaken – and alarmingly, there is no surveillance system that could tell us how often serious complications occur.
The Spanish Ministries of Health and Sciences have announced their ‘Health Protection Plan against Pseudotherapies’. Very wisely, they have included chiropractic under this umbrella. To a large degree, this is the result of Spanish sceptics pointing out that alternative therapies are a danger to public health, helped perhaps a tiny bit also by the publication of two of my books (see here and here) in Spanish. Unsurprisingly, such delelopments alarm Spanish chiropractors who fear for their livelihoods. A quickly-written statement of the AEQ (Spanish Chiropractic Association) is aimed at averting the blow. It makes the following 11 points (my comments are below):
1. The World Health Organization (WHO) defines chiropractic as a healthcare profession. It is independent of any other health profession and it is neither a therapy nor a pseudotherapy.
2. Chiropractic is statutorily recognised as a healthcare profession in many European countries including Portugal, France, Italy, Switzerland, Belgium, Denmark, Sweden, Norway and the United Kingdom10, as well as in the USA, Canada and Australia, to name a few.
3. Chiropractic members of the AEQ undergo university-level training of at least 5 years full-time (300 ECTS points). Chiropractic training is offered within prestigious institutions such as the Medical Colleges of the University of Zurich and the University of Southern Denmark.
4. Chiropractors are spinal health care experts. Chiropractors practice evidence-based, patient-centred conservative interventions, which include spinal manipulation, exercise prescription, patient education and lifestyle advice.
5. The use of these interventions for the treatment of spine-related disorders is consistent with guidelines and is supported by high quality scientific evidence, including multiple systematic reviews undertaken by the prestigious Cochrane collaboration15, 16, 17.
6. The Global Burden of Disease study shows that spinal disorders are the leading cause of years lived with disability worldwide, exceeding depression, breast cancer and diabetes.
7. Interventions used by chiropractors are recommended in the 2018 Low Back Pain series of articles published in The Lancet and clinical practice guidelines from Denmark, Canada, the European Spine Journal, American College of Physicians and the Global Spine Care Initiative.
8. The AEQ supports and promotes scientific research, providing funding and resources for the development of high quality research in collaboration with institutions of high repute, such as Fundación Jiménez Díaz and the University of Alcalá de Henares.
9. The AEQ strenuously promotes among its members the practice of evidence-based, patient-centred care, consistent with a biopsychosocial model of health.
10. The AEQ demands the highest standards of practice and professional ethics, by implementing among its members the Quality Standard UNE-EN 16224 “Healthcare provision by chiropractors”, issued by the European Committee of Normalisation and ratified by AENOR.
11. The AEQ urges the Spanish Government to regulate chiropractic as a healthcare profession. Without such legislation, citizens of Spain cannot be assured that they are protected from unqualified practitioners and will continue to face legal uncertainties and barriers to access an essential, high-quality, evidence-based healthcare service.
END OF QUOTE
I think that some comments might be in order (they follow the numbering of the AEQ):
- The WHO is the last organisation I would consult for information on alternative medicine; during recent years, they have published mainly nonsense on this subject. How about asking the inventor of chiropractic? D.D. Palmer defined it as “a science of healing without drugs.” Chiropractors nowadays prefer to be defined as a profession which has the advantage that one cannot easily pin them down for doing mainly spinal manipulation; if one does, they indignantly respond “but we also use many other interventions, like life-style advice, for instance, and nobody can claim this to be nonsense” (see also point 4 below).
- Perfect use of a classical fallacy: appeal to authority.
- Appeal to authority, plus ignorance of the fact that teaching nonsense even at the highest level must result in nonsense.
- This is an ingenious mix of misleading arguments and lies: most chiros pride themselves of treating also non-spinal conditions. Very few interventions used by chiros are evidence-based. Exercise prescription, patient education and lifestyle advice are hardy typical for chiros and can all be obtained more authoratively from other healthcare professionals.
- Plenty of porkies here too. For instance, the AEQ cite three Cochrane reviews. The first concluded that high-quality evidence suggests that there is no clinically relevant difference between SMT and other interventions for reducing pain and improving function in patients with chronic low-back pain. The second stated that combined chiropractic interventions slightly improved pain and disability in the short term and pain in the medium term for acute/subacute LBP. However, there is currently no evidence that supports or refutes that these interventions provide a clinically meaningful difference for pain or disability in people with LBP when compared to other interventions. And the third concluded that, although support can be found for use of thoracic manipulation versus control for neck pain, function and QoL, results for cervical manipulation and mobilisation versus control are few and diverse. Publication bias cannot be ruled out. Research designed to protect against various biases is needed. Findings suggest that manipulation and mobilisation present similar results for every outcome at immediate/short/intermediate-term follow-up. Multiple cervical manipulation sessions may provide better pain relief and functional improvement than certain medications at immediate/intermediate/long-term follow-up. Since the risk of rare but serious adverse events for manipulation exists, further high-quality research focusing on mobilisation and comparing mobilisation or manipulation versus other treatment options is needed to guide clinicians in their optimal treatment choices. Hardly the positive endorsement implied by the AEQ!
- Yes, but that is not an argument for chiropractic; in fact, it’s another fallacy.
- Did they forget the many guidelines, institutions and articles that do NOT recommend chiropractic?
- I believe the cigarette industry also sponsors research; should we therefore all start smoking?
- I truly doubt that the AEQ strenuously promotes among its members the practice of evidence-based healthcare; if they did, they would have to discourage spinal manipulation!
- The ‘highest standards of practice and professional ethics’ are clearly not compatible with chiropractors’ use of spinal manipulation. In our recent book, we explained in full detail why this is so.
- An essential, high-quality, evidence-based healthcare service? Chiropractic is certainly not essential, rarely high-quality, and clearly not evidence-based.
Nice try AEQ.
But not good enough, I am afraid.
Many chiropractors tell new mothers that their child needs chiropractic adjustments because the birth is in their view a trauma for the new-born that causes subluxations of the baby’s spine. Without expert chiropractic intervention, they claim, the poor child risks serious developmental disorders.
 This article (one of hundreds) explains it well: Birth trauma is often overlooked by doctors as the cause of chronic problems, and over time, as the child grows, it becomes a thought less considered. But the truth is that birth trauma is real, and the impact it can have on a mother or child needs to be addressed. Psychological therapy, physical therapy, chiropractic care, acupuncture, and other healing techniques should all be considered following an extremely difficult birth.
This article (one of hundreds) explains it well: Birth trauma is often overlooked by doctors as the cause of chronic problems, and over time, as the child grows, it becomes a thought less considered. But the truth is that birth trauma is real, and the impact it can have on a mother or child needs to be addressed. Psychological therapy, physical therapy, chiropractic care, acupuncture, and other healing techniques should all be considered following an extremely difficult birth.
And another article makes it quite clear what intervention is required: Caesarian section or a delivery that required forceps or vacuum extraction procedures, in-utero constraint, an unusual presentation of the baby, and many more can cause an individual segment of the spine or a region to shift from its normal healthy alignment. This ‘shift’ in the spine is called a Subluxation, and it can happen immediately before, during, or after birth.
Thousands of advertisements try to persuade mothers to take their new-born babies to a chiropractor to get the problem sorted which chiropractors often call KISS (kinetic imbalance due to suboccipital strain-syndrome), caused by intrauterine-constraint or the traumas of birth.
This abundance of advertisements and promotional articles is in sharp contrast with the paucity of scientific evidence.
 A review of 1993 concluded that birth trauma remains an underpublicized and, therefore, an undertreated problem. There is a need for further documentation and especially more studies directed toward prevention. In the meantime, manual treatment of birth trauma injuries to the neuromusculoskeletal system could be beneficial to many patients not now receiving such treatment, and it is well within the means of current practice in chiropractic and manual medicine.
A review of 1993 concluded that birth trauma remains an underpublicized and, therefore, an undertreated problem. There is a need for further documentation and especially more studies directed toward prevention. In the meantime, manual treatment of birth trauma injuries to the neuromusculoskeletal system could be beneficial to many patients not now receiving such treatment, and it is well within the means of current practice in chiropractic and manual medicine.
A more critical assessment of … concluded that, given the absence of evidence of beneficial effects of spinal manipulation in infants and in view of its potential risks, manual therapy, chiropractic and osteopathy should not be used in infants with the kinetic imbalance due to suboccipital strain-syndrome, except within the context of randomised double-blind controlled trials.
So, what follows from all this?
How about this?
Chiropractors’ assumption of an obligatory birth trauma that causes subluxation and requires spinal adjustments is nothing more than a ploy by charlatans for filling their pockets with the cash of gullible parents.
It is time, I think, to express my gratitude to Dr Jens Behnke, a German homeopath employed by the pro-homeopathy lobby group the ‘Carstens Stiftung’, who diligently tweets trials of homeopathy which he obviously believes prove the value of his convictions.
The primary objective of this new study was to evaluate the efficacy of homoeopathy for women suffering from polycystic ovary syndrome. This condition is characterised by:
- irregular periods which means your ovaries don’t regularly release eggs,
- abnormally high levels of male hormones in the body, which may cause physical signs such as excess facial or body hair,
- polycystic ovaries – ovaries become enlarged and contain many fluid-filled sacs (follicles) which surround the eggs.

There’s no cure for PCOS, but the symptoms can usually be treated. As so often in such situations, homeopaths are happy to step into the fray.
This single-blind, randomised, placebo-controlled pilot study was conducted at two research centres in India. The cases fulfilling the eligibility criteria were enrolled (n = 60) and randomised to either the homoeopathic intervention (HI) (n = 30) or placebo (P) (n = 30) with uniform lifestyle modification (LSM) for 6 months.
The menstrual regularity with improvement in other signs/symptoms was observed in 60% of the cases (n = 18) in HI + LSM group and none (n = 0) in control group. Statistically significant difference was observed in the reduction of intermenstrual duration in HI + LSM in comparison to placebo + LSM group. Significant improvements were also observed in HI+LSM group in domains of weight, fertility, emotions and menstrual problems. No change was observed in respect of improvement in the ultrasound findings. Pulsatilla was the most frequently indicated homeopathic remedy.
The authors concluded that HI along with LSM has shown promising outcome; further comparative study with standard conventional treatment on adequate sample size is desirable.
This trial might convince believers (mostly because they do not even need convincing), but it cannot convince anybody capable of critical thinking. Here is why:
- According to its authors, this trial was a pilot study; this means it should not report any results and merely focus on the feasibility of a definitive trial.
- Researchers were not blinded, meaning that they might have influenced the outcome in more than one way.
- The primary endpoint was subjective and could have been influenced by the non-blinded researchers.
- 0% success rate in achieving the primary endpoint in the placebo group is not plausible.
- Compliance to LSM was not checked; as the homeopathy group lost more weight, these patients seemed to have complied better (probably due to being better motivated by the non-blinded researchers).
So?
My conclusion is not very original but all the more true: POORLY DESIGNED STUDIES USUALLY GENERATE UNRELIABLE RESULTS.
A pain in the neck is just that: A PAIN IN THE NECK! Unfortunately, this symptom is both common and often difficult to treat. Chiropractors pride themselves of treating neck pain effectively. Yet, the evidence is at best thin, the costs are high and, as often-discussed, the risks might be considerable. Thus, any inexpensive, effective and safe alternative would be welcome.
This RCT tested two hypotheses:
1) that denneroll cervical traction (a very simple device for the rehabilitation of sagittal cervical alignment) will improve the sagittal alignment of the cervical spine.
2) that restoration of normal cervical sagittal alignment will improve both short and long-term outcomes in cervical myofascial pain syndrome patients.

The study included 120 (76 males) patients with chronic myofascial cervical pain syndrome (CMCPS) and defined cervical sagittal posture abnormalities. They were randomly assigned to the control or an intervention group. Both groups received the Integrated neuromuscular inhibition technique (INIT); additionally, the intervention group received the denneroll cervical traction device. Alignment outcomes included two measures of sagittal posture: cervical angle (CV), and shoulder angle (SH). Patient relevant outcome measures included: neck pain intensity (NRS), neck disability (NDI), pressure pain thresholds (PPT), cervical range of motion using the CROM. Measures were assessed at three intervals: baseline, 10 weeks, and 1 year after the 10 week follow up.
After 10 weeks of treatment, between group statistical analysis, showed equal improvements for both the intervention and control groups in NRS and NDI. However, at 10 weeks, there were significant differences between groups favouring the intervention group for PPT and all measures of CROM. Additionally, at 10 weeks the sagittal alignment variables showed significant differences favouring the intervention group for CV and SH indicating improved CSA. Importantly, at the 1-year follow-up, between group analysis identified a regression back to baseline values for the control group for the non-significant group differences (NRS and NDI) at the 10-week mark. Thus, all variables were significantly different between groups favouring the intervention group at 1-year follow up.
The authors concluded that the addition of the denneroll cervical orthotic to a multimodal program positively affected CMCPS outcomes at long term follow up. We speculate the improved sagittal cervical posture alignment outcomes contributed to our findings.
Yes, I know, this study is far from rigorous or conclusive. And the evidence for traction is largely negative. But the device has one huge advantage over chiropractic: it cannot cause much harm. The harm to the wallet is less than that of endless sessions chiropractors or other manual therapists (conceivably, a self-made cushion will have similar effects without any expense); and the chances that patients suffer a stroke are close to zero.
I have repeatedly discussed the risks of chiropractic manipulation. Sadly, when doing so, we have to rely mostly on case reports (there is no monitoring system that would record such events, reliable incidence figures are therefore not available). This means every new case report is of considerable importance.
Korean neurosurgeons recently reported the case of a patient who had an infarction of the posterior inferior cerebellar artery (PICA) after a chiropractic cervical manipulation. A 39-year-old man visited the emergency room with signs of cerebellar dysfunction, presenting with a 6-hour history of vertigo and imbalance. Two weeks before, he had been treated by a chiropractor for intermittent neck pain. At the time of admission, brain computed tomography, magnetic resonance imaging, and angiography revealed an acute infarction in the left PICA territory and occlusion of the extracranial vertebral artery (VA; V1/2 junction) as a result of a dissection of the VA. Angiography revealed complete occlusion of the left PICA and arterial dissection was shown in the extracranial portion of the VA. The patient was treated with antiplatelet therapy. Three weeks later, he was discharged without any sequelae.
The authors concluded that the possibility of VA dissection should be considered at least once in patients presenting with cerebellar dysfunctions with a recent history of chiropractic cervical manipulation.
In the discussion section, the authors leave little doubt about the question of causality: damage to the V3 portion is the most common injury that may occur after chiropractic manipulation related to anatomical structures. The VA is located horizontally in a groove in the upper side of the atlas’ posterior arch. During abruptly forced neck rotation and stretching, the gap between the atlas and the atlanto-occipital membrane, which the VA penetrates, can be stretched, resulting in dissection. In our case, it appeared that the V1/2 junction had been dissected due to excessive lateral bending of the neck, thought to be caused by an impact to the left transverse foramen of the sixth cervical spine, through which the left VA passes. It is presumed that there was a mechanical injury to the vessel wall at the time of the procedure, which caused dissection and then the thrombus generated, and two weeks after small emboli caused the occlusion of PICA. Low-speed, high-amplitude manipulations that consist of a series of smooth, repetitive movements are configured in certain areas of the neck, and this does not often cause damage. However, a sudden thrust or high-speed, low-amplitude manipulation is often considered the cause of VA dissection. In particular, this type of manipulation can be theorized to result in a sudden, symmetrical rotation of the extended cervical vertebrae, leading to damage to the high cervical and proximal parts of the carotid artery and VA.
It is high time, I think, that chiropractors take such events seriously. At the very minimum, we need a system of monitoring such cases, so that – eventually – we will be able to define their frequency. In this context, it is obviously important to remember that there is precious little evidence to suggest that neck manipulations are effective for any condition. What inescapably follows is clear: until we have reliable incidence data, it is wise to avoid chiropractic neck manipulations altogether.
For some researchers, the question whether homeopathy works beyond a placebo effect is not as relevant as the question whether it works as well as an established treatment. To answer it, they must conduct RCTs comparing homeopathy with a therapy that has been shown beyond reasonable doubt to be effective, i.e better than placebo. Such a drug is, for instance, Ibuprofen.
The purpose of this study was to compare the efficacy of Ibuprofen and homeopathic Belladonna for orthodontic pain. 51 females and 21 males, were included in this study. Cases with non-extraction treatment plan having proper contacts’ mesial and distal to permanent first molar and currently not taking any analgesics or antibiotics were included in the study. They were randomly divided into two groups; one group was assigned to ibuprofen 400 mg and second group took Belladonna 6C (that’s a dilution of 1: 1000000000000). Patients were given two doses of medication of their respective remedies one hour before placement of elastomeric separators (Ormco Separators, Ormco Corporation, CA, USA) and one dose 6 h after the placement. Pain scores were recorded on a visual analogue scale (VAS) 2 h after placement, 6 h after placement, bedtime, day 1 morning, day 2 morning, day 3 morning and day 5 morning.
The comparisons showed that there were no differences between the two groups at any time point.

(Mean visual analogue scale pain score at different time intervals after separator placement in Ibuprofen and Belladonna group)
The authors concluded that Ibuprofen and Belladonna 6C are effective and provide adequate analgesia with no statistically significant difference. Lack of adverse effects with Belladonna 6C makes it an effective and viable alternative.
FINALLY, THE PROOF HOMEOPATHS HAVE BEEN WAITING FOR: HOMEOPATHY DOES WORK AFTER ALL!
Not so fast – before we draw any conclusions, let’s have a closer look at this study. Here are a few of its limitations (apart from the fact that it was published in a journal that does not exactly belong to the ‘crème de la crème’ of medical publications):
- Patients obviously knew which group they were assigned to; thus their expectations would have influenced the outcome.
- The same applies to the researchers (the study could have been ‘blind’ using a ‘double dummy’ method, but the researchers did not use it).
- The study was an equivalence trial (it did not test whether homeopathy is superior to placebo, but whether its effects are equivalent to Ibuprofen); such studies need sample sizes that are about one dimension larger than was the case here.
Therefore, all this trial does demonstrate that the sample was too small for an existing group difference in favour of Ibuprofen to show.
So sorry, my homeopathic friends!
Acupressure is the stimulation of acu-points by using pressure instead of needles, as in acupuncture. The evidence for or against acupressure mirrors that of acupuncture, except there is far less of it. This is why this new trial might be important.
The aim of this RCT was to determine the effect of self-acupressure on fasting blood sugar (FBS) and insulin level in type 2 diabetes patients. A total of 60 diabetic patients were selected from diabetes clinic in Rafsanjan in Iran, and assigned to 2 groups, 30 in the acupressure and 30 in the control-group. The intervention group received acupressure at ST-36, LIV-3, KD-3 and SP-6 points bilaterally for 5 minutes at each point in 10 seconds pressure and 2 seconds rest periods. Subjects in the control group received no intervention. The FBS and insulin levels were measured before and after the intervention for both groups.
There were no significant differences between the acupressure and control group regarding age, sex and level of education. The insulin level significantly increased after treatment in the acupressure group (p=0.001). There were no significant differences between the levels of insulin in study or control groups. Serum FBS level decreased significantly after intervention in the acupressure group compared to the control group (p=0.02).
The authors concluded that self-acupressure as a complementary alternative medicine can be a helpful complementary method in reducing FBS and increasing insulin levels in type 2 diabetic patients.
I do not want to go into the methodological details of this study; suffice to say that it was less than rigorous and that its findings are therefore not trustworthy (never mind the fact that the results are biologically implausible). Even if that had not been the case, a single study would certainly not be sufficient reason to reach the conclusion that acupressure is helpful to control diabetes. For that, I am sure, we would need at least half a dozen independent replications.
Like most people, I have several non-medical friends who suffer from diabetes. They would love nothing better than having a simple, safe and effective method applying pressure to their skin in order to manage their disease. If they read this paper, some of them might conclude that acupressure is the answer to their problems and use it to control their condition. One does not need all that much imagination to see that this could seriously harm them, or even cost several lives.
Acupressure might be virtually free of risks, but with a bit of ill advice, even seemingly harmless treatments can kill.
Personally, I like sauna bathing. It makes me feel fine. But is it healthy? More specifically, is it good for the cardiovascular system?
Finnish researchers had already shown in a large cohort study with 20 years of follow-up that increased frequency of sauna bathing is associated with a reduced risk of sudden cardiac death (SCD), fatal coronary heart disease (CHD), fatal cardiovascular disease (CVD), and all-cause mortality. Now the same group of researchers report more encouraging news for sauna-fans.
The aim of their new study was to investigate the relationship between sauna habits and CVD mortality in men and women, and whether adding information on sauna habits to conventional cardiovascular risk factors is associated with improvement in prediction of CVD mortality risk.
Sauna bathing habits were assessed at baseline in a sample of 1688 participants (mean age 63; range 53-74 years), of whom 51.4% were women. Multivariable-adjusted hazard ratios (HRs) were calculated to investigate the relationships of frequency and duration of sauna use with CVD mortality.
A total of 181 fatal CVD events occurred during a median follow-up of 15.0 years (interquartile range, 14.1-15.9). The risk of CVD mortality decreased linearly with increasing sauna sessions per week with no threshold effect. In age- and sex-adjusted analysis, compared with participants who had one sauna bathing session per week, HRs (95% CIs) for CVD mortality were 0.71 (0.52 to 0.98) and 0.30 (0.14 to 0.64) for participants with two to three and four to seven sauna sessions per week, respectively. After adjustment for established CVD risk factors, potential confounders including physical activity, socioeconomic status, and incident coronary heart disease, the corresponding HRs (95% CIs) were 0.75 (0.52 to 1.08) and 0.23 (0.08 to 0.65), respectively. The duration of sauna use (minutes per week) was inversely associated with CVD mortality in a continuous manner. Addition of information on sauna bathing frequency to a CVD mortality risk prediction model containing established risk factors was associated with a C-index change (0.0091; P = 0.010), difference in - 2 log likelihood (P = 0.019), and categorical net reclassification improvement (4.14%; P = 0.004).

(Hazard ratios for cardiovascular mortality by quartiles of the duration of sauna bathing. a Adjusted for age and gender. b Adjusted for age, gender, body mass index, smoking, systolic blood pressure, serum low-density lipoprotein cholesterol, alcohol consumption, previous myocardial infarction, and type 2 diabetes. CI, confidence interval.)
The authors concluded that higher frequency and duration of sauna bathing are each strongly, inversely, and independently associated with fatal CVD events in middle-aged to elderly males and females. The frequency of sauna bathing improves the prediction of the long-term risk for CVD mortality.
These results are impressive. What could be the underlying mechanisms? The authors offer plenty of explanations: Dry and hot sauna baths have been shown to increase the demands of cardiovascular function. Sauna bathing causes an increase in heart rate which is a reaction to the body heat load. Heart rate may be elevated up to 120–150 beats per minute during sauna bathing, corresponding to low- to moderate-intensity physical exercise training for the circulatory system without active muscle work. Acute sauna exposure has been shown to produce blood pressure lowering effects, decrease peripheral vascular resistance and arterial stiffness, and improve arterial compliance. Short-term sauna exposure also activates the sympathetic nervous and the renin-angiotensin-aldosterone systems and the hypothalamus-pituitary-adrenal hormonal axis, and short-term increases in levels of their associated hormones have been reported. Repeated sauna exposure improves endothelial function, suggesting a beneficial role of thermal therapy on vascular function. Long-term sauna bathing habit may be beneficial in the reduction of high systemic blood pressure, which is in line with previous evidence showing that blood pressure may be lower among those who are living in warm conditions with higher ambient temperature. Regular sauna bathing is associated with a lowered risk of future hypertension. Typical hot and dry Finnish sauna increases body temperature which causes more efficient skin blood flow, leading to a higher cardiac output, whereas blood flow to internal organs decreases. Sweat is typically secreted at a rate which corresponds to an average total secretion of 0.5 kg during a sauna bathing session. Increased sweating is accompanied by a reduction in blood pressure and higher heart rate, while cardiac stroke volume is largely maintained, although a part of blood volume is diverted from the internal organs to body peripheral parts with decreasing venous return which is not facilitated by active skeletal muscle work. However, it has been proposed that muscle blood flow may increase to at least some extent in response to heat stress, although sauna therapy-induced myocardial metabolic adaptations are largely unexplored. There is also evidence that regular long-term sauna bathing (average of two sessions per week) increases left ventricular ejection fraction. Heat therapy may improve left ventricular function with decreased cardiac pre- and afterload, thereby maintaining appropriate stroke volume despite large reductions in ventricular filling pressures. Additionally, previous studies have demonstrated a positive alteration of the autonomic nervous system and reduced levels of natriuretic peptides, oxidative stress, inflammation, and norepinephrine due to regular sauna therapy.
It is possible that the results are influenced by confounding factors that the researchers were unable to account for. It is also possible that people who are already ill avoid sauna bathing and that this contributed to the findings. However, the authors did their best to explore such phenomena in sub-group analysis and found that a causal relationship between sauna and CVD risk is still very likely. As a sauna-fan, I am inclined to believe them and the sceptic in me tends to agree.
Ginkgo biloba is a well-researched herbal medicine which has shown promise for a number of indications. But does this include coronary heart disease?
The aim of this systematic review was to provide information about the effectiveness and safety of Ginkgo Leaf Extract and Dipyridamole Injection (GD) as one adjuvant therapy for treating angina pectoris (AP) and to evaluate the relevant randomized controlled trials (RCTs) with meta-analysis. (Ginkgo Leaf Extract and Dipyridamole Injection is a Chinese compound preparation, which consists of ginkgo flavone glycosides (24%), terpene lactones (ginkgolide about 13%, ginkgolide about 2.9%) and dipyridamole.)
RCTs concerning AP treated by GD were searched and the Cochrane Risk Assessment Tool was adopted to assess the methodological quality of the RCTs. A total of 41 RCTs involving 4,462 patients were included in the meta-analysis. The results indicated that the combined use of GD and Western medicine (WM) against AP was associated with a higher total effective rate [risk ratio (RR)=1.25, 95% confidence interval (CI): 1.21–1.29, P<0.01], total effective rate of electrocardiogram (RR=1.29, 95% CI: 1.21–1.36, P<0.01). Additional, GD combined with WM could decrease the level of plasma viscosity [mean difference (MD)=–0.56, 95% CI:–0,81 to–0.30, P<0.01], fibrinogen [MD=–1.02, 95% CI:–1.50 to–0.54, P<0.01], whole blood low shear viscosity [MD=–2.27, 95% CI:–3.04 to–1.49, P<0.01], and whole blood high shear viscosity (MD=–0.90, 95% CI: 1.37 to–0.44, P<0.01).
The authors concluded that comparing with receiving WM only, the combine use of GD and WM was associated with a better curative effect for patients with AP. Nevertheless, limited by the methodological quality of included RCTs more large-sample, multi-center RCTs were needed to confirm our findings and provide further evidence for the clinical utility of GD.
If one reads this conclusion, one might be tempted to use GD to cure AP. I would, however, strongly warn everyone from doing so. There are many reasons for my caution:
- All the 41 RCTs originate from China, and we have repeatedly discussed that Chinese TCM trials are highly unreliable.
- The methodological quality of the primary RCTs was, according to the review authors ‘moderate’. This is not true; it was, in fact, lousy.
- Dipyridamole is not indicated in angina pectoris.
- To the best of my knowledge, there is no good evidence from outside China to suggest that Ginkgo biloba is effective for angina pectoris.
- Angina pectoris is caused by coronary artery disease (a narrowing of one or more coronary arteries due to atherosclerosis), and it seems implausible that this condition can be ‘cured’ with any medication.
So, what we have here is yet another nonsensical paper, published in a dubious journal, employing evidently irresponsible reviewers, run by evidently irresponsible editors, hosted by a seemingly reputable publisher (Springer). This is reminiscent of my previous post (and many posts before). Alarmingly, it is also what I encounter on a daily basis when scanning the new publications in my field.
The effects of this incessant stream of nonsense can only have one of two effects:
- People take this ‘evidence’ seriously. In this case, many patients might pay with their lives for this collective incompetence.
- People conclude that alt med research cannot be taken seriously. In this case, we are unlikely to ever see anything useful emerging from it.
Either way, the result will be profoundly negative!
It is high time to stop this idiocy; but how?
I wish, I knew the answer.