vaccination
Numerous qualitative studies and a few quantitative studies have linked vaccine hesitancy or refusal with the belief in the efficacy of so-called alternative medicine (SCAM). Yet, large-scale data on this topic are scarce. In this study, the French researchers investigated the factors associated with the coverage rates of seven childhood vaccines or vaccine groups in the ninety-six metropolitan French departments. One of the factors investigated was the local interest in SCAM. In order to assess this interest, they built an Alternative Medicine Index based on departmental internet searches regarding SCAM—internet searches being a reliable indicator of the public’s actual interest in a given topic. They then conducted multiple regression analyses, which showed that this Index is a significant explanatory factor for the departmental variance in vaccination coverage rates, exceeding in importance the effect of other relevant local sociodemographic factors.
A further recent study from France adds to the picture. It presents the results of a survey conducted in July 2021 among a representative sample of the French mainland adult population (n = 3087). Using cluster analysis, the researchers identified five profiles of SCAM attitudes and found that even among the most pro-SCAM group, very few respondents disagreed with the idea that SCAM should only be used as a complement to conventional medicine. They then compared these SCAM attitudes to vaccine attitudes. Attitudes to SCAM had a distinct impact as well as a combined effect on attitudes to different vaccines and vaccines in general. They found that:
- attitudes to SCAM provide a very limited explanation of vaccine hesitancy;
- among the hesitant, pro-SCAM attitudes are often combined with other traits associated with vaccine hesitancy such as distrust of health agencies, radical political preferences, and low income.
Both SCAM endorsement and vaccine hesitancy are more prevalent among the socially disadvantaged. Drawing on these results, the researchers argue that, to better understand the relationship between SCAM and vaccine hesitancy, it is necessary to look at how both can reflect a lack of access and recourse to mainstream medicine and distrust of public institutions.
 The fact that the enthusiasm for SCAM is associated with vaccine hesitancy has been discussed on this blog many times before, e.g.:
The fact that the enthusiasm for SCAM is associated with vaccine hesitancy has been discussed on this blog many times before, e.g.:
- Preference of so-called alternative medicine predicts negative attitudes to vaccination
- What are the reasons for opposing COVID vaccinations?
- Intelligence, Religiosity, SCAM, Vaccination Hesitancy – are there links?
- More information on homeopaths’ and anthroposophic doctors’ attitude towards vaccinations
- The anti-vaccination movement is financed by the dietary supplement industry
- Sorry, I was wrong about homeopathy and vaccination
- The UK Society of Homeopaths, a hub of anti-vaccination activists?
- HOMEOPATHY = “the complete alternative to vaccination” ?!?!
- Are anthroposophy-enthusiasts for or against vaccinations?
- Far too many chiropractors believe that vaccinations do not have a positive effect on public health
- Naturopaths’ counselling against vaccinations could be criminally negligent
- HOMEOPATHS AGAINST VACCINATION: “The decision to vaccinate and how you implement that decision is yours and yours alone”
- Use of alternative medicine is associated with low vaccination rates
- Integrative medicine physicians tend to harbour anti-vaccination views
- Vaccination: chiropractors “espouse views which aren’t evidence based”
What seems fairly clear to me is that a cross-correlation exists: an attitude against modern medicine and the ‘scientific establishment’ determines both the enthusiasm for SCAM and the aversion to vaccination. What is, however, far from clear to me is what we could do about it.
Yes, better education seems important – and that’s precisely what I aim at achieving with this blog. Sadly, judging from some of the comments we receive, it does not seem crowned with much success.
Any other ideas?
On this blog, we have some people who continue to promote conspiracy theories about Covid and Covid vaccinations. It is, therefore, time, I feel, to present them with some solid evidence on the subject (even though it means departing from our usual focus on SCAM).
This Cochrane review assessed the efficacy and safety of COVID‐19 vaccines (as a full primary vaccination series or a booster dose) against SARS‐CoV‐2. An impressive team of investigators searched the Cochrane COVID‐19 Study Register and the COVID‐19 L·OVE platform (last search date 5 November 2021). They also searched the WHO International Clinical Trials Registry Platform, regulatory agency websites, and Retraction Watch. They included randomized controlled trials (RCTs) comparing COVID‐19 vaccines to placebo, no vaccine, other active vaccines, or other vaccine schedules.
A total of 41 RCTs could be included and analyzed assessing 12 different vaccines, including homologous and heterologous vaccine schedules and the effect of booster doses. Thirty‐two RCTs were multicentre and five were multinational. The sample sizes of RCTs were 60 to 44,325 participants. Participants were aged: 18 years or older in 36 RCTs; 12 years or older in one RCT; 12 to 17 years in two RCTs; and three to 17 years in two RCTs. Twenty‐nine RCTs provided results for individuals aged over 60 years, and three RCTs included immunocompromised patients. No trials included pregnant women. Sixteen RCTs had two‐month follow-ups or less, 20 RCTs had two to six months, and five RCTs had greater than six to 12 months or less. Eighteen reports were based on preplanned interim analyses. The overall risk of bias was low for all outcomes in eight RCTs, while 33 had concerns for at least one outcome. 343 registered RCTs with results not yet available were identified.The evidence for mortality was generally sparse and of low or very low certainty for all WHO‐approved vaccines, except AD26.COV2.S (Janssen), which probably reduces the risk of all‐cause mortality (risk ratio (RR) 0.25, 95% CI 0.09 to 0.67; 1 RCT, 43,783 participants; high‐certainty evidence).High‐certainty evidence was found that BNT162b2 (BioNtech/Fosun Pharma/Pfizer), mRNA‐1273 (ModernaTx), ChAdOx1 (Oxford/AstraZeneca), Ad26.COV2.S, BBIBP‐CorV (Sinopharm‐Beijing), and BBV152 (Bharat Biotect) reduce the incidence of symptomatic COVID‐19 compared to placebo (vaccine efficacy (VE): BNT162b2: 97.84%, 95% CI 44.25% to 99.92%; 2 RCTs, 44,077 participants; mRNA‐1273: 93.20%, 95% CI 91.06% to 94.83%; 2 RCTs, 31,632 participants; ChAdOx1: 70.23%, 95% CI 62.10% to 76.62%; 2 RCTs, 43,390 participants; Ad26.COV2.S: 66.90%, 95% CI 59.10% to 73.40%; 1 RCT, 39,058 participants; BBIBP‐CorV: 78.10%, 95% CI 64.80% to 86.30%; 1 RCT, 25,463 participants; BBV152: 77.80%, 95% CI 65.20% to 86.40%; 1 RCT, 16,973 participants).Moderate‐certainty evidence was found that NVX‐CoV2373 (Novavax) probably reduces the incidence of symptomatic COVID‐19 compared to placebo (VE 82.91%, 95% CI 50.49% to 94.10%; 3 RCTs, 42,175 participants).There is low‐certainty evidence for CoronaVac (Sinovac) for this outcome (VE 69.81%, 95% CI 12.27% to 89.61%; 2 RCTs, 19,852 participants).High‐certainty evidence was found that BNT162b2, mRNA‐1273, Ad26.COV2.S, and BBV152 result in a large reduction in the incidence of severe or critical disease due to COVID‐19 compared to placebo (VE: BNT162b2: 95.70%, 95% CI 73.90% to 99.90%; 1 RCT, 46,077 participants; mRNA‐1273: 98.20%, 95% CI 92.80% to 99.60%; 1 RCT, 28,451 participants; AD26.COV2.S: 76.30%, 95% CI 57.90% to 87.50%; 1 RCT, 39,058 participants; BBV152: 93.40%, 95% CI 57.10% to 99.80%; 1 RCT, 16,976 participants).
Moderate‐certainty evidence was found that NVX‐CoV2373 probably reduces the incidence of severe or critical COVID‐19 (VE 100.00%, 95% CI 86.99% to 100.00%; 1 RCT, 25,452 participants).
Two trials reported high efficacy of CoronaVac for severe or critical disease with wide CIs, but these results could not be pooled.
mRNA‐1273, ChAdOx1 (Oxford‐AstraZeneca)/SII‐ChAdOx1 (Serum Institute of India), Ad26.COV2.S, and BBV152 probably result in little or no difference in serious adverse events (SAEs) compared to placebo (RR: mRNA‐1273: 0.92, 95% CI 0.78 to 1.08; 2 RCTs, 34,072 participants; ChAdOx1/SII‐ChAdOx1: 0.88, 95% CI 0.72 to 1.07; 7 RCTs, 58,182 participants; Ad26.COV2.S: 0.92, 95% CI 0.69 to 1.22; 1 RCT, 43,783 participants); BBV152: 0.65, 95% CI 0.43 to 0.97; 1 RCT, 25,928 participants). In each of these, the likely absolute difference in effects was fewer than 5/1000 participants.
Evidence for SAEs is uncertain for BNT162b2, CoronaVac, BBIBP‐CorV, and NVX‐CoV2373 compared to placebo (RR: BNT162b2: 1.30, 95% CI 0.55 to 3.07; 2 RCTs, 46,107 participants; CoronaVac: 0.97, 95% CI 0.62 to 1.51; 4 RCTs, 23,139 participants; BBIBP‐CorV: 0.76, 95% CI 0.54 to 1.06; 1 RCT, 26,924 participants; NVX‐CoV2373: 0.92, 95% CI 0.74 to 1.14; 4 RCTs, 38,802 participants).
The authors’ conclusions were as follows: Compared to placebo, most vaccines reduce, or likely reduce, the proportion of participants with confirmed symptomatic COVID‐19, and for some, there is high‐certainty evidence that they reduce severe or critical disease. There is probably little or no difference between most vaccines and placebo for serious adverse events. Over 300 registered RCTs are evaluating the efficacy of COVID‐19 vaccines, and this review is updated regularly on the COVID‐NMA platform (covid-nma.com).
_____________________
As some conspiratorial loons will undoubtedly claim that this review is deeply biased; it might be relevant to add the conflicts of interest of its authors:
- Carolina Graña: none known.
- Lina Ghosn: none known.
- Theodoros Evrenoglou: none known.
- Alexander Jarde: none known.
- Silvia Minozzi: no relevant interests; Joint Co‐ordinating Editor and Method editor of the Drugs and Alcohol Group.
- Hanna Bergman: Cochrane Response – consultant; WHO – grant/contract (Cochrane Response was commissioned by the WHO to perform review tasks that contribute to this publication).
- Brian Buckley: none known.
- Katrin Probyn: Cochrane Response – consultant; WHO – consultant (Cochrane Response was commissioned to perform review tasks that contribute to this publication).
- Gemma Villanueva: Cochrane Response – employment (Cochrane Response has been commissioned by WHO to perform parts of this systematic review).
- Nicholas Henschke: Cochrane Response – consultant; WHO – consultant (Cochrane Response was commissioned by the WHO to perform review tasks that contributed to this publication).
- Hillary Bonnet: none known.
- Rouba Assi: none known.
- Sonia Menon: P95 – consultant.
- Melanie Marti: no relevant interests; Medical Officer at WHO.
- Declan Devane: Health Research Board (HRB) – grant/contract; registered nurse and registered midwife but no longer in clinical practice; Editor, Cochrane Pregnancy and Childbirth Group.
- Patrick Mallon: AstraZeneca – Advisory Board; spoken of vaccine effectiveness to media (print, online, and live); works as a consultant in a hospital that provides vaccinations; employed by St Vincent’s University Hospital.
- Jean‐Daniel Lelievre: no relevant interests; published numerous interviews in the national press on the subject of COVID vaccination; Head of the Department of Infectious Diseases and Clinical Immunology CHU Henri Mondor APHP, Créteil; WHO (IVRI‐AC): expert Vaccelarate (European project on COVID19 Vaccine): head of WP; involved with COVICOMPARE P et M Studies (APHP, INSERM) (public fundings).
- Lisa Askie: no relevant interests; Co‐convenor, Cochrane Prospective Meta‐analysis Methods Group.
- Tamara Kredo: no relevant interests; Medical Officer in an Infectious Diseases Clinic at Tygerberg Hospital, Stellenbosch University.
- Gabriel Ferrand: none known.
- Mauricia Davidson: none known.
- Carolina Riveros: no relevant interests; works as an epidemiologist.
- David Tovey: no relevant interests; Emeritus Editor in Chief, Feedback Editors for 2 Cochrane review groups.
- Joerg J Meerpohl: no relevant interests; member of the German Standing Vaccination Committee (STIKO).
- Giacomo Grasselli: Pfizer – speaking engagement.
- Gabriel Rada: none known.
- Asbjørn Hróbjartsson: no relevant interests; Cochrane Methodology Review Group Editor.
- Philippe Ravaud: no relevant interests; involved with Mariette CORIMUNO‐19 Collaborative 2021, the Ministry of Health, Programme Hospitalier de Recherche Clinique, Foundation for Medical Research, and AP‐HP Foundation.
- Anna Chaimani: none known.
- Isabelle Boutron: no relevant interests; member of Cochrane Editorial Board.
___________________________
And as some might say this analysis is not new, here are two further papers just out:
Objectives To determine the association between covid-19 vaccination types and doses with adverse outcomes of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection during the periods of delta (B.1.617.2) and omicron (B.1.1.529) variant predominance.
Design Retrospective cohort.
Setting US Veterans Affairs healthcare system.
Participants Adults (≥18 years) who are affiliated to Veterans Affairs with a first documented SARS-CoV-2 infection during the periods of delta (1 July-30 November 2021) or omicron (1 January-30 June 2022) variant predominance. The combined cohorts had a mean age of 59.4 (standard deviation 16.3) and 87% were male.
Interventions Covid-19 vaccination with mRNA vaccines (BNT162b2 (Pfizer-BioNTech) and mRNA-1273 (Moderna)) and adenovirus vector vaccine (Ad26.COV2.S (Janssen/Johnson & Johnson)).
Main outcome measures Stay in hospital, intensive care unit admission, use of ventilation, and mortality measured 30 days after a positive test result for SARS-CoV-2.
Results In the delta period, 95 336 patients had infections with 47.6% having at least one vaccine dose, compared with 184 653 patients in the omicron period, with 72.6% vaccinated. After adjustment for patient demographic and clinical characteristics, in the delta period, two doses of the mRNA vaccines were associated with lower odds of hospital admission (adjusted odds ratio 0.41 (95% confidence interval 0.39 to 0.43)), intensive care unit admission (0.33 (0.31 to 0.36)), ventilation (0.27 (0.24 to 0.30)), and death (0.21 (0.19 to 0.23)), compared with no vaccination. In the omicron period, receipt of two mRNA doses were associated with lower odds of hospital admission (0.60 (0.57 to 0.63)), intensive care unit admission (0.57 (0.53 to 0.62)), ventilation (0.59 (0.51 to 0.67)), and death (0.43 (0.39 to 0.48)). Additionally, a third mRNA dose was associated with lower odds of all outcomes compared with two doses: hospital admission (0.65 (0.63 to 0.69)), intensive care unit admission (0.65 (0.59 to 0.70)), ventilation (0.70 (0.61 to 0.80)), and death (0.51 (0.46 to 0.57)). The Ad26.COV2.S vaccination was associated with better outcomes relative to no vaccination, but higher odds of hospital stay and intensive care unit admission than with two mRNA doses. BNT162b2 was generally associated with worse outcomes than mRNA-1273 (adjusted odds ratios between 0.97 and 1.42).
Conclusions In veterans with recent healthcare use and high occurrence of multimorbidity, vaccination was robustly associated with lower odds of 30 day morbidity and mortality compared with no vaccination among patients infected with covid-19. The vaccination type and number of doses had a significant association with outcomes.
SECOND EXAMPLE Long COVID, or complications arising from COVID-19 weeks after infection, has become a central concern for public health experts. The United States National Institutes of Health founded the RECOVER initiative to better understand long COVID. We used electronic health records available through the National COVID Cohort Collaborative to characterize the association between SARS-CoV-2 vaccination and long COVID diagnosis. Among patients with a COVID-19 infection between August 1, 2021 and January 31, 2022, we defined two cohorts using distinct definitions of long COVID—a clinical diagnosis (n = 47,404) or a previously described computational phenotype (n = 198,514)—to compare unvaccinated individuals to those with a complete vaccine series prior to infection. Evidence of long COVID was monitored through June or July of 2022, depending on patients’ data availability. We found that vaccination was consistently associated with lower odds and rates of long COVID clinical diagnosis and high-confidence computationally derived diagnosis after adjusting for sex, demographics, and medical history.
_______________________________________
There are, of course, many more articles on the subject for anyone keen to see the evidence. Sadly, I have little hope that the COVID loons will be convinced by any of them. Yet, I thought I should give it nevertheless a try.
In response to yesterday’s post, I received a lengthy comment from ‘Stan’. Several readers have already commented on it. Therefore, I can make my arguments short. In this post, will repeat Stan’s points each followed by my comments (in bold). Here we go:
Seven Reasons Homœopathy is Not Placebo Effect
Sorry, Stan, but your heading is not proper English; I have therefore changed it for the title of this post.
1. Homeopathic remedies work on babies, animals, plants and people in a coma. Biodynamic farmers use homeopathic remedies to repel pests and treat plant diseases. Some organic ranchers rely on homeopathic remedies to treat their herds. Some “placebo by proxy” effect has been shown for children but its doubtful that it could be shown for a herd of cattle or crops in a field. Farmers can’t rely on wishful thinking to stay in business.
As discussed ad nauseam on this blog, homeopathic remedies do not work on babies or animals better than placebos. I don’t know of any studies with “people in a coma” (if you do, Stan, please let me know). The fact that ranchers rely on homeopathy is hilarious but does not prove anything.
2. The correct curative remedy will initially cause a worsening of the condition being cured if it is given in too strong (i.e. too dilute) a dose. A placebo might only cause a temporary improvement of the condition being treated; certainly not an aggravation.
The ‘homeopathic aggravation’ is a myth created by homeopaths. It disappears if we try to systematically research it; see here, for instance.
3. One can do a “proving” of an unknown homeopathic remedy by taking it repeatedly over several days and it will temporarily cause symptoms that one has never experienced previously – symptoms it will cure in a sick person. This is a repeatable scientific experiment used to determine the scope of a new remedy, or confirm the effects of an already proven remedy. A placebo might possibly have an effect if the individual taking it has been “prepared” by being told what they are taking but it likely wouldnt match previously recorded symptoms in the literature.
Homeopathic provings are rubbish and not reproducible when done rigorously; see here.
4. One can treat simple acute (self-limiting) conditions (e.g. minor burns, minor injuries, insect bites, etc.) and see unusually rapid cures with homeopathic remedies. A placebo might only cause a temporary improvement of the condition being treated while taken. Placebos have been found mostly effective in conditions with a strong psychological component like pain.
You mean like using Arnica for cuts and bruises? Sadly, it does not work.
5. One can get homeopathic treatment for long term chronic (non self-limiting) conditions and see a deep lasting cure, as has been documented clinically for a couple centuries. A placebo might only cause a temporary partial improvement of the condition being treated while the placebo is being taken.
You mean like asthma, eczema, or insomnia?
6. There is over 200 years worth of extensive documentation from around the world, of the clinical successes of homeopathy for both acute and chronic conditions of all types. As Dr Hahn has said you have throw out 90% of the evidence to conclude that homeopathy doesnt work. The Sheng et al meta-analysis in 2005 Lancet that was supposedly the death knell of homeopathy used only 8 studies, excluding hundreds of others. Unsurprisingly homeopathy was found wanting. So-called Skeptics see what they want to see in the science. There is relatively little documentation of placebo usage. A few recent studies have been done showing the limited temporary benefits of placebos.
What Hahn wrote is understandably liked by homeopaths but it nevertheless is BS. If you don’t trust me, please rely on independent bodies from across the world.
7. Homeopathic remedies have been shown to have a very weak electromagnetic signature and contain some nano-particles. Some believe this explains their mechanism. An exciting new potential field of research is the subtle cell signalling that has been found to direct the development of stem cells. Scientists have created double-headed planeria worms and this trait has been found to be inherited by their offspring without any change in the genes or epigenetics. Until now we had no idea how a single fertilized ovum could evolve into a complex creature that is bilateral and has multiple cell types. It is possible that the very subtle electromagnetic signature or some other unknown effect of homeopathic remedies is effecting this subtle cell signalling.
The homeopathic nano-myth is nonsense. And so is the rest of your assumptions.
Every conventional drug has “side effects” that match the symptoms for which it is indicated! Aspirin can cause headaches and fever, ritalin can cause hyperactive effects, radiation can cause cancer. Conventional doctors are just practicing bad homeopathy. They are prescribing Partially similar medicines. If their drugs were homeopathic (i.e. similar) to the patients symptoms on all levels they would be curative. Radiation sometimes does cure cancer instead of just suppressing it per usual.
Even if this were true, what would it prove? Certainly not that homeopathy works!
Dr Hahneman did forbid mixing homeopathy and conventional medicine. In his day doctors commonly used extensive blood letting and extreme doses of mercury. Its not Quite as bad now.
You evidently did not read Hahnemann’s writings.
Just because we dont know how extremely dilute homeopathic remedies work, doesn’t discount that they Do work. Homeopathy seems to fly in the face of Known science. In no way is it irrational or unscientific. There are lots of phenomena in the universe that cant be explained yet, like dark energy and dark matter effects and even consciousness!
Not knowing how a treatment works has not stopped science to test whether it works (e.g. Aspirin). In the case of homeopathy, the results of these endeavors were not positive.
The assumption that the moon is made of cheese also flies in the face of science; do you perhaps think that this makes it true?
The actions of homeopathy can and have been well-explained: they are due to placebo effects.
________________________
Stan, thank you for this entertaining exercise. But, next time, please remember to supply evidence for your statements.
Conspiracy beliefs have become a major issue and obstacle to progress. While holding conspiracy beliefs has been associated with several detrimental social, personal, and health consequences, little research has been dedicated to systematically reviewing the methods that could reduce conspiracy beliefs.
A team of researchers conducted a systematic review to identify and assess interventions that have sought to counter conspiracy beliefs. They included 25 studies (total N = 7179) and discovered that, while the majority of interventions were ineffective in terms of changing conspiracy beliefs, several interventions were particularly effective. Interventions that fostered an analytical mindset or taught critical thinking skills were found to be the most effective in terms of changing conspiracy beliefs.
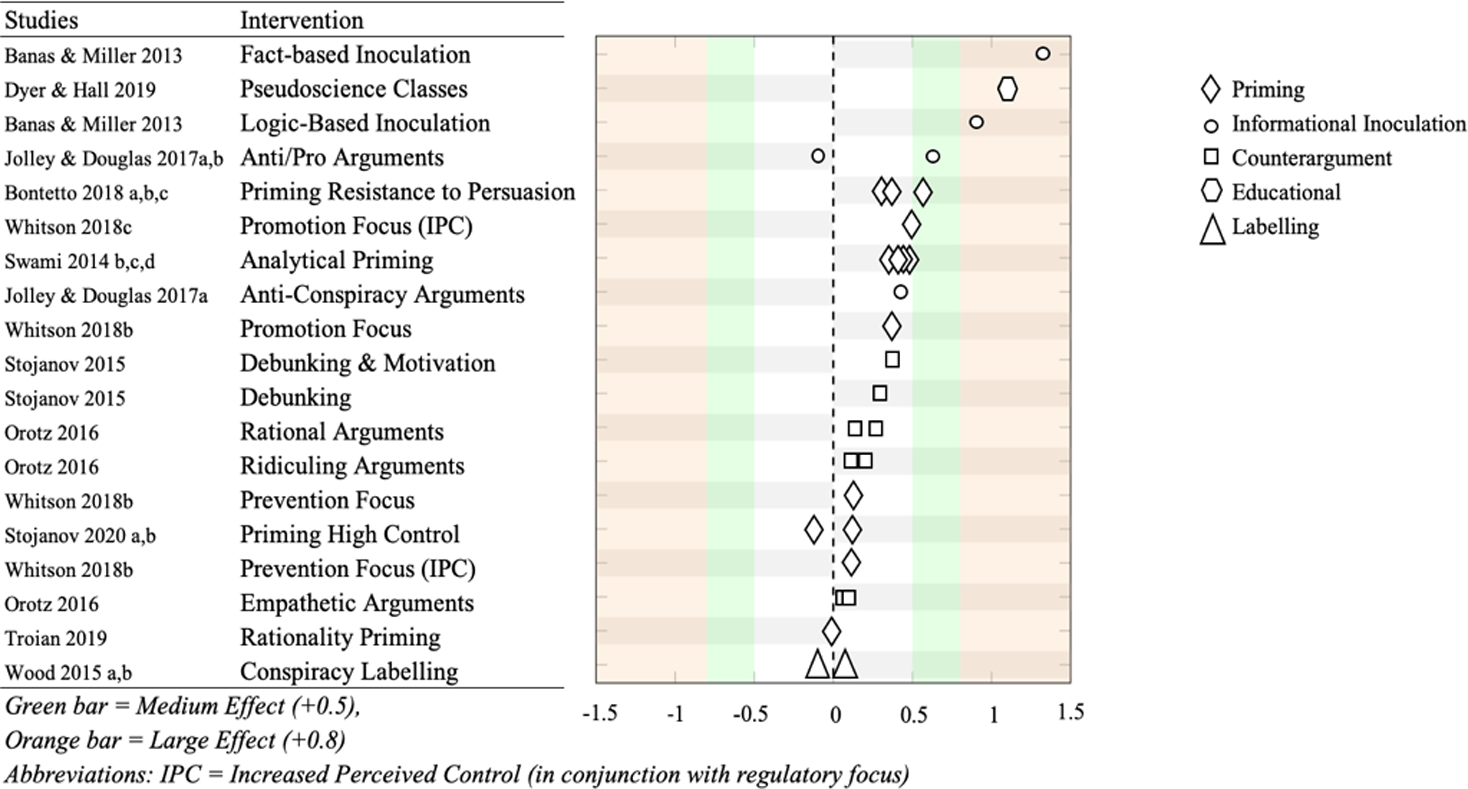
Approximately half of the examined interventions consisted of priming-based tasks. The majority of these interventions demonstrated a significant change in conspiracy beliefs. The effects were all either small or very small. Participants who were primed to be less susceptible to persuasion tactics showed significantly lower conspiracy beliefs when compared to controls among three experimental comparisons. These effects were shown to range from small to medium.
Interventions that primed participants to engage in analytical thinking resulted in primed participants having lower conspiracy beliefs than controls. However, the effects of these differences were small. Other priming interventions focused on manipulating participants’ sense of control. They had mixed results, either increasing or decreasing conspiracy beliefs with very small effects.
About a sixth of all interventions used inoculation methods. All successfully reduced conspiracy beliefs, relative to controls, all with either medium or large effects. Inoculations that identified the factual inaccuracies of conspiracy beliefs were found to be the most effective of all the interventions in the review. Inoculations that demonstrated the logical fallacies of conspiracy beliefs were found to be the second most effective intervention.
The authors concluded that their review found that overall, the majority of current conspiracy interventions are ineffective in terms of changing conspiracy beliefs. Despite this, we have identified several promising interventions that may be fruitful to pursue in future studies. We propose that a focus on inoculation-based and critical thinking interventions will bear more promising results for future research, though further efforts are needed to reduce participant burden and more easily implement these interventions in the real world.
The identification of the factual inaccuracies of conspiracy beliefs plus the stimulation of critical thinking are two aims I actively pursue with this blog. Thus, one might hope that I do make a small contribution to the reduction of conspiracy beliefs.
Yes, one might hope – but judging from many comments posted in the discussion sections, one could easily get a different impression.
It has been reported that the PLASTIC SURGERY INSTITUTE OF ·UTAH, INC.; MICHAEL KIRK MOORE JR.; KARI DEE BURGOYNE; KRISTIN JACKSON ANDERSEN; AND SANDRA FLORES, stand accused of running a scheme out of the Plastic Surgery Institute of Utah, Inc. to defraud the United States and the Centers for Disease Control and Prevention.
Dr. Michael Kirk Moore, Jr. and his co-defendants at the Plastic Surgery Institute of Utah have allegedly given falsified vaccine cards to people in exchange for their donating $50 to an unnamed organization, one which exists to “liberate the medical profession from government and industry conflicts of interest.” As part of the scheme, Moore and his co-defendants are accused of giving children saline injections so that they would believe they were really being vaccinated.
The co-defendants are Kari Dee Burgoyne, an office manager at the Plastic Surgery Institute of Utah; Sandra Flores, the office’s receptionist; and, strangest of all, a woman named Kristin Jackson Andersen, who according to the indictment is Moore’s neighbor. Andersen has posted copious and increasingly conspiratorial anti-vaccine content on Facebook and Instagram; Dr. Moore himself was a signatory on a letter expressing support for a group of COVID-skeptical doctors whose certification was under review by their respective medical boards. The letter expresses support for ivermectin, a bogus treatment for COVID.
According to the indictment, the Plastic Surgery Center of Utah was certified as a real vaccine provider and signed a standard agreement with the CDC, which among other things requires doctor’s offices not to “sell or seek reimbursement” for vaccines.
Prosecutors allege that, when people seeking falsified vaccine cards contacted the office, Burgoyne, the office manager, referred them to Andersen, Dr. Moore’s neighbor. Andersen, according to the indictment, would ask for the name of someone who’d referred them—it had to be someone who’d previously received a fraudulent vaccine card, per the indictment—then direct people to make a $50 donation to a charitable organization, referred to in the indictment only as “Organization 1.” Each vaccine card seeker was required to put an orange emoji in the memo line of their donation.
After making a donation to the unnamed charitable organization, prosecutors allege, Andersen would send a link to vaccine card seekers to enable them to make an appointment at the Plastic Surgery Institute. With adult patients, Moore would allegedly use a real COVID vaccine dose in a syringe, but squirt it down the drain. Flores, the office’s receptionist, gave an undercover agent a note, reading “with 18 & younger, we do a saline shot,” meaning that kids were injected with saline instead of a vaccine. Prosecutors allege the team thus disposed of at least 1,937 doses of COVID vaccines.
All four people are charged with conspiracy to defraud the United States; conspiracy to convert, sell, convey, and dispose of government property; and conversion, sale, conveyance, and disposal of government property and aiding and abetting.
Throughout the scheme, the group reported the names of all the vaccine seekers to the Utah Statewide Immunization Information System, indicating that the practice had administered 1,937 doses of COVID-19 vaccines, which included 391 pediatric doses. The value of all the doses totaled roughly $28,000. With the money from the $50 vaccination cards totaling nearly $97,000, the scheme was valued at nearly $125,000, federal prosecutors calculated.
“By allegedly falsifying vaccine cards and administering saline shots to children instead of COVID-19 vaccines, not only did this provider endanger the health and well-being of a vulnerable population, but also undermined public trust and the integrity of federal health care programs,” Curt Muller, special agent in charge with the Department of Health and Human Services for the Office of the Inspector General, said in a statement.
_________________________________
I am already baffled by anti-vax attitudes when they originate from practitioners of so-called alternative medicine (SCAM). When they come from real physicians and are followed by real actions, I am just speechless. As I stated many times before: studying medicine does unfortunately not protect you from recklessness, greed, or stupidity.
It has been reported that a well-known conservative activist, Kelly Canon, from Arlington, Texas, USA, has tragically died. She was famous for peddling COVID-19 vaccine misinformation. The complications caused by the virus—just a few weeks after attending a “symposium” against the vaccines – have killed her. 
“Another tragedy and loss for our Republican family. Our dear friend Kelly Canon lost her battle with pneumonia today. Kelly will be forever in our hearts as a loyal and beloved friend and Patriot. Gone way too soon We will keep her family in our prayers,” the Arlington Republican Club said in a statement.
Her death was said to be “from COVID-related pneumonia.” Canon had announced on Facebook in November that her employer had granted her a religious exemption for the COVID-19 vaccine. “No jabby-jabby for me! Praise GOD!” she wrote at the time.
Canon had been an outspoken critic of COVID-19 vaccine mandates and pandemic-related restrictions. In one of her final Facebook posts, Canon shared several links to speeches she attended at a “COVID symposium” in Burleson in early December devoted to dissuading people from getting the COVID-19 vaccines that are currently available. The event was organized by God Save Our Children, which bills itself as “a conservative group that is fighting against the use of experimental vaccines on our children.”
Canon had shared similar content on Twitter, where her most recent post was a YouTube video featuring claims that the coronavirus pandemic was “planned” in advance and part of a global conspiracy.
As news of her death spread Tuesday, pro-vaccine commentators flooded her Facebook page with cruel comments and mocking memes, while her supporters unironically praised her for being a “warrior for liberty” to the very end.
___________________________
A religious exemption?
What for heaven’s sake is that?
I feel sad for every death caused by COVID and its complications. If the death is caused by ignorance, it renders the sadness all the more profound.
The UK medical doctor, Sarah Myhill, has a website where she tells us:
Everyone should follow the general approach to maintaining and restoring good health, which involves eating a paleo ketogenic diet, taking a basic package of nutritional supplements, ensuring a good night’s sleep on a regular basis and getting the right balance between work, exercise and rest. Because we live in an increasingly polluted world, we should probably all be doing some sort of detox regime.
She also happens to sell dietary supplements of all kinds which must surely be handy for all who want to follow her advice. Dr. Myhill boosted her income even further by putting false claims about Covid-19 treatments online. And that got her banned from practicing for nine months after a medical tribunal.
She posted videos and articles advocating taking vitamins and other substances in high doses, without evidence they worked. The General Medical Council (GMC) found her recommendations “undermined public health” and found some of her recommendations had the potential to cause “serious harm” and “potentially fatal toxicity”. The tribunal was told she uploaded a series of videos and articles between March and May 2020, describing substances as “safe nutritional interventions” which she said meant vaccinations were “rendered irrelevant”. But the substances she promoted were not universally safe and have potentially serious health risks associated with them, the panel was told. The tribunal found Dr. Myhill “does not practice evidence-based medicine and may encourage false reassurance in her patients who may believe that they will not catch Covid-19 or other infections if they follow her advice”.
Dr. Myhill previously had a year-long ban lifted after a General Medical Council investigation into her claims of being a “pioneer” in the treatment of chronic fatigue syndrome. In fact, the hearing was told there had been 30 previous GMC investigations into Dr. Myhill, but none had resulted in findings of misconduct.
Dr. Myhill is also a vocal critic of the PACE trial and biopsychosocial model of ME/CFS. Dr. Myhill’s GMC complaint regarding a number of PACE trial authors was first rejected without investigation by the GMC, after Dr. Myhill appealed the GMC stated they would reconsider. Dr. Myhill’s action against the GMC for failing to provide reasoning for not investigating the PACE trial authors is still continuing and began a number of months before the most recent GMC instigation of her practice started.
The recent tribunal concluded: “Given the circumstances of this case, it is necessary to protect members of the public and in the public interest to make an order suspending Dr. Myhill’s registration with immediate effect, to uphold and maintain professional standards and maintain public confidence in the profession.”
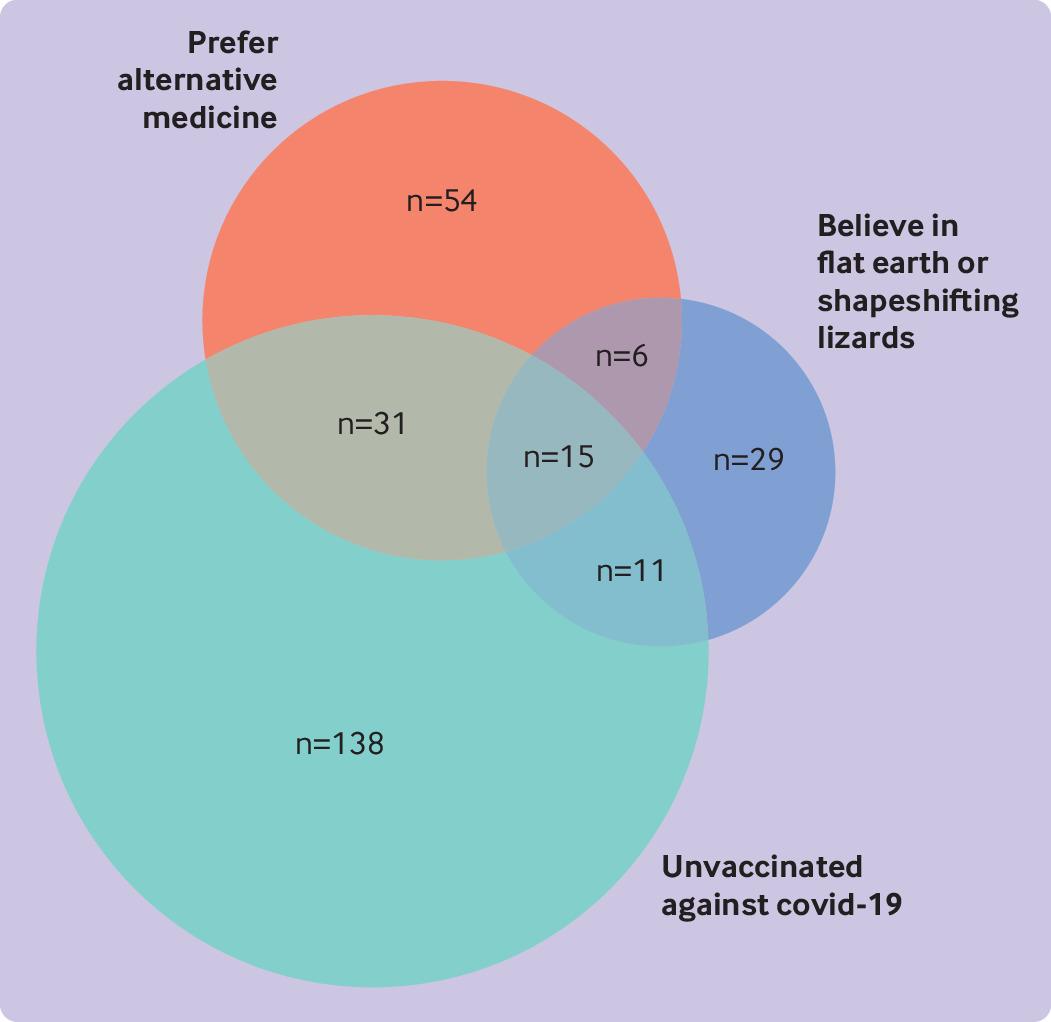
The objective of this cross-sectional survey was to evaluate the beliefs about and attitudes toward cancer prevention of people professing vaccination skepticism or conspiracy theories. Data were collected mainly from a well-known Spanish forum and other platforms, including Reddit (English), 4Chan (English), HispaChan (Spanish), and a Spanish-language website for cancer prevention (mejorsincancer.org) from January to March 2022.
Among 1494 responders, 209 were unvaccinated against covid-19, 112 preferred so-called alternative rather than conventional medicine, and 62 reported flat earth or reptilian beliefs. Cancer beliefs were assessed using the Cancer Awareness Measure (CAM) and Cancer Awareness Measure Mythical Causes Scale (CAM-MYCS), both validated tools.
Awareness of the actual causes of cancer was greater (median CAM score 63.6%) than that of mythical causes (41.7%). The most endorsed mythical causes of cancer were:
- eating food containing additives or sweeteners,
- feeling stressed,
- eating genetically modified food.
Awareness of the actual and mythical causes of cancer among the unvaccinated, alternative medicine, and conspiracy groups was lower than among their counterparts. A median of 54.5% of the actual causes was accurately identified among each of the unvaccinated, alternative medicine, and conspiracy groups, and a median of 63.6% was identified in each of the three corresponding counterparts (P=0.13, 0.04, and 0.003, respectively). For mythical causes, medians of 25.0%, 16.7%, and 16.7% were accurately identified in the unvaccinated, alternative medicine, and conspiracy groups, respectively; a median of 41.7% was identified in each of the three corresponding counterparts (P<0.001 in adjusted models for all comparisons).
In total, 673 (45.0%) participants agreed with the statement “It seems like everything causes cancer.” No significant differences were observed among the unvaccinated (44.0%), conspiracist (41.9%), or alternative medicine groups (35.7%), compared with their counterparts (45.2%, 45.7%, and 45.8%, respectively).

The authors’ conclusions were as follows: we evaluated the patterns of beliefs about cancer among people who believed in conspiracies, rejected the covid-19 vaccine, or preferred alternative medicine. We observed that the participants who belonged to these groups were more likely to endorse mythical causes of cancer than were their counterparts but were less likely to endorse the actual causes of cancer. Almost half of the participants, whether
conspiracists or not, agreed with the statement “It seems like everything causes cancer,” which highlights the difficulty that society encounters in differentiating actual causes of cancer from mythical causes owing to mass (veridical or not) information. This suggests a direct connection between digital misinformation and consequent potential erroneous health decisions, which may represent a further preventable fraction of cancer. Cultivating oriented medical education and scientific literacy, improving online ranking algorithms, building trust, and using effective health communication and social marketing campaigns may be possible ways to tackle this complex public health threat.
This is yet another study showing that so-called alternative medicine (SCAM) usage is linked to misinformation and conspiratorial thinking in other areas. We have discussed similar findings all too often. They are hardly surprising, in my view. As I have repeatedly been trying to point out:
- SCAM use is based mainly on misinformation
- And, to a large extent, SCAM is little more than a conspiracy theory in disguise.
The best way to prevent harm must therefore be to educate the public responsibly (which, of course, is one of the main aims of this blog.
The INDY and many other news outlets reported that the British Tory MP, Andrew Bridgen, has called on prime minister Rishi Sunak to suspend mRNA covid vaccines after alleging they are “not safe, not effective and not necessary”.
During Wednesday’s PMQs (13 December), Bridgen stated that “since the rollout in the UK of the BioNTech-Pfizer mRNA vaccine, we have had almost half a million reports of adverse effects from the public”, a message he later reiterated on Twitter.
Posting a snippet from his debate, Bridgen tweeted: “Almost half a million yellow card reports of adverse effects following administration of the Biotech Pfizer mRNA vaccine in the UK alone! Answers are desperately needed. #completelyunprecedented”.
Bridgen also claimed that a leading figure in the British Heart Foundation is suppressing evidence that the Covid vaccines cause heart damage, even sending non-disclosure agreements to his research team.
Facebook flagged his post with a notice urging users to ensure that they share “reliable information.” It included two links to “continue sharing” or “get vaccine info.”

The scandals Bridgen has been involved in seem too numerous to mention (e.g. violation of parliamentary standards, homophobic remarks, antisemitic statements). Here is just one of the most recent:
A Leicestershire MP has been ordered to pay £800,000 and been evicted from his five bedroom home by a judge following a legal dispute involving the family vegetable business. It is currently unknown where Andrew Bridgen, Conservative MP for North West Leicestershire, lives after being given final deadline of August 24 to vacate the premises in Coleorton, near Coalville.
The 57-year-old was branded “dishonest” by a High Court judge in March – who ruled that Bridgen “lied” under oath. Judge Brian Rawlings said he was so dishonest that nothing he said about the dispute with AB Produce, a vegetable and potato supplier based in Measham, could be taken at face value.
Bridgen was also said to have behaved in an “abusive”, “arrogant” and “aggressive” way during the dispute, in which he has spent years suing the firm. A later judgment in June, reported by the Times on Sunday, forced the MP to vacate the £1.5 million-valued property owned by AB Produce that he has lived in since 2015…
For a fact check on Bridgeon’s vaccine claims, see here. And below are a few reactions from Twitter users to Bridgen’s Covid proctophsia:
First a High Court judge says Tory MP, Andrew Bridgen, lied under oath, then he evicts him from his home and orders him to pay £800,000 now Facebook flags his posts as Covid misinformation. How’s your week going?
Andrew Bridgen MP now promoting Dr David Cartland, a man who aligns himself with claims that Freemasons rule the world; that Covid doesn’t exist; and that medical doctors who don’t share his views should be executed (screenshots H/T
Andrew Bridgen MP now promoting Dr David Cartland, a man who aligns himself with claims that Freemasons rule the world; that Covid doesn’t exist; and that medical doctors who don’t share his views should be executed.
This Andrew Bridgen? ‘A Conservative MP lied under oath, behaved in an abusive, arrogant and aggressive way, and was so dishonest that his claims about a multimillion-pound family dispute could not be taken at face value, a high court judge has ruled.’
Proper tinfoil-hat stuff from Andrew Bridgen, suggesting Covid vaccines are unsafe, misrepresenting data, and implying some sort of conspiracy between ‘Big Pharma’ and MHRA.

It has been reported that a naturopath from the US who sold fake COVID-19 immunization treatments and fraudulent vaccination cards during the height of the coronavirus pandemic has been sentenced to nearly three years in prison. Juli A. Mazi pleaded guilty last April in federal court in San Francisco to one count of wire fraud and one count of false statements related to health care matters. Now District Judge Charles R. Breyer handed down a sentence of 33 months, according to Joshua Stueve, a spokesperson for the U.S. Department of Justice. Mazi, of Napa, was ordered to surrender to the Bureau of Prisons on or before January 6, 2023.
The case is the first federal criminal fraud prosecution related to fraudulent Centers for Disease Control and Prevention vaccination cards for COVID-19, according to the U.S. Department of Justice. In August, Breyer denied Mazi’s motion to withdraw her plea agreement after she challenged the very laws that led to her prosecution. Mazi, who fired her attorneys and ended up representing herself, last week filed a letter with the court claiming sovereign immunity. Mazi said that as a Native American she is “immune to legal action.”

She provided fake CDC vaccination cards for COVID-19 to at least 200 people with instructions on how to complete the cards to make them look like they had received a Moderna vaccine, federal prosecutors said. She also sold homeopathic pellets she fraudulently claimed would provide “lifelong immunity to COVID-19.” She told customers that the pellets contained small amounts of the virus and would create an antibody response. Mazi also offered the pellets in place of childhood vaccinations required for attendance at school and sold at least 100 fake immunization cards that said the children had been vaccinated, knowing the documents would be submitted to schools, officials said. Federal officials opened an investigation against Mazi after receiving a complaint in April 2021 to the Department of Health and Human Services Office of Inspector General hotline.
_______________________
On her website, Mazi states this about herself:
Juli Mazi received her doctorate in Naturopathic Medicine from the National University of Natural Medicine in Portland, Oregon where she trained in the traditional medical sciences as well as ancient and modern modalities that rely on the restorative power of Nature to heal. Juli Mazi radiates the vibrant health she is committed to helping her patients achieve. Juli’s positive outlook inspires confidence; her deep well of calm puts people at immediate ease. The second thing they notice is that truly she listens. Dr. Mazi’s very presence is healing.
On this site, she also advocates all sorts of treatments and ideas which I would call more than a little strange, for instance, coffee enemas:
Using a coffee enema is a time-tested remedy for detoxification, but it is not without risks. If you are not careful, the process can cause internal burns. In addition, improperly brewed coffee can lead to electrolyte imbalances and dehydration, and coffee enemas are not recommended for pregnant women or young children.
To make coffee enemas safe and effective, always choose quality organic coffee. A coffee enema should be free of toxins and pesticides. Use a reusable enema kit with stainless steel or silicone hosing for safety. Moreover, do not use a soft plastic or latex enema bags. It is also essential to limit the length of time that the coffee spends in the container.
A coffee enema should be held for 12 to 15 minutes and then released in the toilet. You may repeat the process as necessary. Usually, the procedure should be done once or twice a day. However, if you are experiencing acute toxicity, you can use a coffee enema as often as needed. Make sure you have had a bowel movement before making the coffee enema. Otherwise, the process may be hindered.
Perhaps the most interesting thing on her website is her advertisement of the fact that her peers not just tolerate such eccentricities but gave Mazi an award for ‘BEST ALTERNATIVE HEALTH & BEST GENERAL PRACTITIONER’.

To me, this suggests that US ‘doctors of naturopathy’ and their professional organizations live on a different planet, a planet where evidence counts for nothing and dangerously misleading patients seems to be the norm.