Uncategorized
Yes, I have just published another book! It is entitled ALTERNATIVE MEDICINE, A CRITICAL ASSESSMENT OF 150 MODALITIES.
And yes, I would like you to read it! (You don’t need to buy it, go to your library and ask them to order it.)
Therefore, allow me to try and whet your appetite by simply copying the preface of my book here:

In their famous editorial of 1998, Angell and Kassirer concluded that “It is time for the scientific community to stop giving alternative medicine a free ride. There cannot be two kinds of medicine — conventional and alternative. There is only medicine that has been adequately tested and medicine that has not, medicine that works and medicine that may or may not work. Once a treatment has been tested rigorously, it no longer matters whether it was considered alternative at the outset. If it is found to be reasonably safe and effective, it will be accepted. But assertions, speculation, and testimonials do not substitute for evidence. Alternative treatments should be subjected to scientific testing no less rigorous than that required for conventional treatments.”[1]
Twenty years later, alternative medicine remains popular and assertions, speculation, and testimonials still substitute for evidence. We are still being inundated with misleading advice, biased opinions, uncritical evaluations, commercially-driven promotion and often even fraudulently wrong conclusions. Consequently, consumers find it hard to access reliable data. As a result, they often make misguided, sometimes even dangerously wrong decisions.
I have researched alternative medicine for more than 25 years. Through this work, I have gathered a wealth of knowledge, facts and experience. In this book, I have summarised the essentials into an easily accessible text. My book offers an introduction into the most important issues around alternative medicine as well as a concise, evidence-based analysis of 150 alternative therapies and diagnostic techniques.
Such information is surely a good thing, but it should nevertheless come with a warning: it may not please everybody! If you are a believer in alternative medicine who does not care about the facts, or an enthusiast for whom alternative medicine has become some sort of a religion, or a person who thinks that science is less important than anecdote, you better return this book to its shelf; reading it will only disquiet you.
If, however, you are looking for the facts about alternative medicine, trust in science, prefer critical assessment to commercial promotion, it might well be a book for you.
I hope that you belong to the latter group and trust it will help you making the right therapeutic decisions for yourself and your family.
[1] http://www.kitsrus.com/pdf/nejm_998.pdf
PS
If you want to publish a book review, please contact me and I will see that you get a free e-book.
The use of so-called alternative medicine (SCAM) for changing the natural history of cancer (rather than for alleviating symptoms) is a dangerous thing. Here is yet another study confirming this statement.
The purpose of this cross-sectional study was to investigate the patterns of SCAM use and its association with time to conventional treatment. The study was performed in Thailand at the Chonburi Cancer Hospital. Chart reviews and interviews were performed for 426 patients with various cancers between May and December 2018.
The results indicated that 45% of all patients reported using SCAMs; herbal products were the most common type. Approximately 34% of these medicines involved unlabelled herbal products with unidentifiable components. The rates of SCAM use were significantly elevated for men and for patients with stage IV cancer. The multivariable linear regression analysis of the relationship between factors and the time until conventional treatment was received revealed that the regression coefficient of the use of SCAM was 56.3 (95% confidence interval [27.9-84.6]). This coefficient corresponded to an additional 56.3 days of time until conventional treatment, relative to patients who did not use SCAM.
The authors concluded that these findings demonstrated that there is a relatively moderate prevalence of CAM use among Thai cancer patients, with most of the CAM treatments involving homemade herbal products. The use of CAM was significantly associated with a prolonged time to conventional treatment. Nevertheless, these findings do not imply that CAM should be banned for all patients, although healthcare providers should recommend that patients aim to use CAM treatments that are considered safe and will not interfere with conventional treatments.
This study would in itself not be very important. Its relevance, in my view, lies in the fact that it is an independent confirmation of many studies published previously showing that cancer patients ought to be cautious about SCAM; for instance:
- Patients who received CM were more likely to refuse additional CCT, and had a higher risk of death. The results suggest that mortality risk associated with CM was mediated by the refusal of CCT.
- The use of CAM had significantly associated with delay in presentation and resolution of diagnosis.
- CAM did not provide any definite survival benefit, CAM users reported clinically significant worse health-related quality of life.
My recommendation to people who have been diagnosed with cancer is to resist the many temptations and promises of SCAM, discuss the issues with their oncology team, and follow their advice. This may sound a little boring, but it just might save your life.
Researchers from the National Institute of Homoeopathy (an autonomous organisation under the Ministry of Ayurveda, Yoga & Naturopathy, Unani, Siddha and Homeopathy, Government of India) tested a Dysentery Compound (DC), a ‘bowel nosode’, against individualized homeopathy (IH) in the treatment of irritable bowel syndrome (IBS). For this purpose, they used an open, randomized (1:1), parallel arms, pragmatic, non-inferiority, pilot trial with 60 IBS patients. IBS Quality of Life (IBS-QOL) questionnaire was used as the primary outcome measure; assessed at baseline and after 3 months.
Six subjects dropped out. Groups were comparable at baseline (all p>0.01). Though intra-group changes were higher favouring IH over DC, group differences were statistically non-significant (all p>0.01). Non-inferiority was not demonstrated by DC against IH over 3 months (mean difference= −3.3, SE=5.2, lower 95% confidence limit −11.9, t= −0.453, p=0.674). No adverse events were reported from either group.
The authors concluded that non-inferiority of DC against IH in treatment of IBS was not demonstrated though it appeared as safe; still, being a pilot trial, no definite conclusion could be drawn. Further exploration of both efficacy and effectiveness of either of the therapies is necessary by adequately powered trials and independent replications.
This trial is a treasure trove of methodological flaws. Here I want to focus on merely one of them: The idea of conducting a non-inferiority study of two treatments, none of which have previously been shown to be effective.
Most clinical trials are ‘superiority studies’ designed to test whether one treatment is more effective than another one. This is fundamentally different in non-inferiority or equivalence studies. They aim to test whether one treatment is as effective as another therapy that has already been fully researched and is generally accepted to be effective for the condition in question. This approach avoids the ethical problems that can arise in superiority studies from giving placebos to patients who require an effective treatment for their condition. Equivalence studies can have many of the features of superiority studies but require a different statistical approach and usually need much larger sample sizes.
This means that the new study never had the slightest chance to generate a result that was in any way meaningful. Such a waste of resources is hardly surprising in the realm of homeopathy; over the years, we have become used to it. But, coming from the National Institute of Homeopathy, it is significant. On their website, the Institute claims this:
The mission of National Institute of Homoeopathy is to foster excellence in Homoeopathic Medical Education and Research, to educate and train undergraduate, post graduate students and research scholars of homoeopathy in accordance with highest professional standards and ethical values unfettered by the barriers of nationality, language, culture, plurality, religion and to meet the healthcare needs of the community through dissemination of knowledge and service.
Excellence in homeopathic research?
Well, you could have fooled me!
I was alerted to this recent and most interesting announcement by the Australian Government:
From 1 April 2019 the following natural therapies will be excluded from the definition of private health insurance general treatment and will no longer receive the private health insurance rebate as part of a general treatment policy: Alexander technique, aromatherapy, Bowen therapy, Buteyko, Feldenkrais, Western herbalism, homeopathy, iridology, kinesiology, naturopathy, Pilates, reflexology, Rolfing, shiatsu, tai chi, and yoga.
Rules have been made to exclude these natural therapies from the definition of general treatment under section 121-10 of the Private Health Insurance Act 2007. Insurers will then not be able to offer benefits for these therapies as part of a complying health insurance policy.
Insurers can offer incentives to purchasers of private health insurance as long as the incentives meet the requirements of the Private Health Insurance (Complying Product) Rules. These incentives could include services provided by a natural therapist. It will be up to each insurer to decide whether to offer this type of incentive.
Consumers will still be able to choose to access these natural therapies outside the private health insurance system.
Why is this important?
A review chaired by the former Commonwealth Chief Medical Officer found there is no clear evidence demonstrating the efficacy of the excluded natural therapies.
This review was informed by an evaluation of the evidence undertaken by the National Health and Medical Research Council (NHMRC). NHMRC was tasked with reviewing scientific literature examining the effectiveness and, where available, the safety and cost effectiveness of 17 natural therapies. This was conducted in line with NHMRC’s approach to assessing evidence, and was undertaken for the specific purpose of informing the Australian Government’s Natural Therapies Review.
Changing coverage for the excluded natural therapies will ensure taxpayer funds are spent appropriately and are not directed to therapies that do not demonstrate evidence of clinical efficacy.
Who will benefit?
Around 54 per cent of the Australian population is covered by general treatment (extras) insurance. Changing coverage for the excluded natural therapies will remove costs from the system and contribute to reducing private health insurance premium growth.
What impact will this change have on private health insurance?
This change will contribute to reducing private health insurance premium price increases.
_____________________________________________________________________
The attempt to make health insurance more evidence based is no doubt laudable. I therefore commend this decision and hope other countries are following suit. Despite my general agreement, I feel compelled to make a few critical comments:
- Some of the banned treatments are not entirely devoid of good evidence. I am thinking of herbalism and tai chi, for instance.
- Iridology is a diagnostic technique and not a ‘natural therapy’.
- The term ‘natural therapy’ is of debatable value: not all of the listed modalities are natural (nothing natural about homeopathy, for instance). Personally, I much prefer ‘so-called alternative medicine (SCAM).
- I can think of many more SCAMs that should be on this list.
It will be fascinating to see whether the stated prediction that the ban will reduce health insurance premiums will be borne out by data. Many SCAM enthusiasts have in the past argued that it will have the opposite effect. Therefore, it would seem very important that the economic effects of this decision are being accurately monitored and that, in time, the results are analysed and published.
This article reports that Medicare is exploring whether to pay for acupuncture. Coverage would be for chronic low-back pain only. In its request for comments on acupuncture, the Department of Health and Human Services said that “in response to the U.S. opioid crisis, HHS is focused on preventing opioid use disorder and providing more evidence-based non-pharmacologic treatment options for chronic pain.” The agency said it hopes “to determine if acupuncture for [chronic low-back pain] is reasonable and necessary under the Medicare program.” A proposal is due by July 15, with a final decision by Oct. 13.
Medicare coverage “is long overdue,” said Tony Y. Chon, director of integrative medicine and health at the Mayo Clinic in Minnesota. “The opioid epidemic is going to be the momentum that’s really needed to push not just acupuncture but other kinds of non-pharmacological interventions to the forefront.”
Some proponents also note that acupuncture is one of the safest interventions available for pain — though some accidents have been reported. Even if it works only for some people, they argue, there is little harm in trying it when other options are not effective.
However, research shows that acupuncture is little more effective than placebo in many cases. When the government’s Agency for Healthcare Research and Quality reviewed research on a wide range of therapies for chronic pain in 2018, it found the “strength of evidence” that acupuncture works for chronic low-back pain is “low.”
The National Center for Complementary and Integrative Health, part of NIH, says “research suggests that acupuncture can help manage certain pain conditions, but evidence about its value for other health issues is uncertain.”
Critics go further, noting that hundreds of years of anatomical studies have not found evidence of the points in the body linked to the “energy channels” that acupuncture claims to be stimulating to provide pain relief. They contend that acupuncture shows all the signs of the placebo effect, with providers and recipients who believe it works and the elaborate ritual of placing the needles in specially selected spots. “The whole thing is a big scam,” said Steven Novella, an assistant professor of neurology at the Yale School of Medicine and editor of the “Science-Based Medicine” website. “The only honest interpretation of the data is that acupuncture is a theatrical placebo.” Novella said that the efficacy attributed to acupuncture could easily be explained by various research biases and that no drug would be allowed on the market based on that level of proof. “We never get that threshold of evidence that you need in medicine, where you get that persistent effect, and it’s replicable” across numerous studies, he said.
The evidence is indeed far from clear. NICE stated that it no longer recommends acupuncture because the evidence is not strong. Others have shown that acupuncture is superior to sham as well as no acupuncture control for back pain, with differences between groups close to .5 SDs compared with no acupuncture control, and close to .2 SDs compared with sham.
A further systematic review stated that acupuncture provides a short-term clinically relevant effect when compared with a waiting list control or when acupuncture is added to another intervention. Yet another systematic review found that acupuncture for chronic nonspecific low back pain was associated with significantly lower pain intensity than placebo but only immediately post-treatment (VAS: -0.59, 95 percent CI: -0.93, -0.25). However, acupuncture was not different from placebo in post-treatment disability, pain medication intake, or global improvement in chronic nonspecific low back pain. Acupuncture did not differ from sham-acupuncture in reducing chronic non-specific neck pain immediately after treatment (VAS: 0.24, 95 percent CI: -1.20, 0.73). Acupuncture was superior to no treatment in improving pain intensity (VAS: -1.19, 95 percent CI: 95 percent CI: -2.17, -0.21), disability (PDI), functioning (HFAQ), well-being (SF-36), and range of mobility (extension, flexion), immediately after the treatment. In general, trials that applied sham-acupuncture tended to produce negative results (i.e., statistically non-significant) compared to trials that applied other types of placebo (e.g., TENS, medication, laser). Results regarding comparisons with other active treatments (pain medication, mobilization, laser therapy) were less consistent Acupuncture was more cost-effective compared to usual care or no treatment for patients with chronic back pain.
The recent Lancet papers excited alternative therapists and their organisations who quickly jumped on the LBP bandwagon. Others have claimed that my often critical verdicts of alternative therapies for LBP are out of line with this evidence. I am broadly in agreement with the evidence presented in Lancet-paper! But I also want to caution that things are complex.
I have therefore copied the non-pharmacological, non-operative treatments listed in the Lancet-paper together with the authors’ verdicts regarding their effectiveness for both acute and persistent LBP. I feel compelled to point out that the Lancet-paper merely lists the effectiveness of several therapeutic options, and that the value of a treatment is not only determined by its effectiveness. Crucial further elements are a therapy’s cost and its risks, the latter of which also determines the most important criterion: the risk/benefit balance. In my version of the Lancet table, I have therefore added these three variables for non-pharmacological and non-surgical options:
| EFFECTIVENESS ACUTE LBP | EFFECTIVENESS PERSISTENT LBP | RISKS | COSTS | RISK/BENEFIT BALANCE | |
| Advice to stay active | +, routine | +, routine | None | Low | Positive |
| Education | +, routine | +, routine | None | Low | Positive |
| Superficial heat | +/- | Ie | Very minor | Low to medium | Positive (aLBP) |
| Exercise | Limited | +/-, routine | Very minor | Low | Positive (pLBP) |
| CBT | Limited | +/-, routine | None | Low to medium | Positive (pLBP) |
| Spinal manipulation | +/- | +/- | vfbmae sae |
High | Negative |
| Massage | +/- | +/- | Very minor | High | Positive |
| Acupuncture | +/- | +/- | sae | High | Questionable |
| Yoga | Ie | +/- | Minor | Medium | Questionable |
| Mindfulness | Ie | +/- | Minor | Medium | Questionable |
| Rehab | Ie | +/- | Minor | Medium to high | Questionable |
Routine = consider for routine use
+/- = second line or adjunctive treatment
Ie = insufficient evidence
Limited = limited use in selected patients
vfbmae = very frequent, minor adverse effects
sae = serious adverse effects, including deaths, are on record
aLBP = acute low back pain
So, should Medicare pay for acupuncture or any other SCAM? Please advise!
This 25/6/2019 press release (distributed by ResponseSource Press Release Wire on behalf of The Faculty of Homeopathy) is today the topic of several UK newspaper articles. Here it is in its full beauty and without any change:
The Faculty of Homeopathy is delighted to announce His Royal Highness The Prince of Wales as Patron of the Faculty of Homeopathy.
Dr Gary Smyth, President of the Faculty of Homeopathy comments, “As the Faculty celebrates its 175th anniversary this year, it is an enormous honour for us to receive the Patronage of His Royal Highness The Prince of Wales and I am delighted to announce this news today. This news is also a fitting memorial to our late friend, colleague and former Faculty President, Dr Peter Fisher, who was a global champion of Homeopathy. I look forward to working with members, friends and supporters of the Faculty, continuing our important work, promoting Homeopathy within both public and professional circles and maintaining awareness of this system of medicine”.
About the Faculty of Homeopathy
Founded in 1844 and incorporated by Act of Parliament in 1950, the Faculty of Homeopathy is one of the longest established Homeopathic organisations in the world. The Faculty has long been recognised as the preeminent membership organisation for statutorily regulated healthcare professionals who integrate Homeopathy within their practice. The Faculty’s mission statement is “To promote and support the highest standards of practice, education and research in Homeopathy”.
The Faculty is an international and multidisciplinary organisation, embracing a wide range of healthcare professionals. The Faculty provides internationally recognised training pathways in Homeopathy for Doctors, Dentists, Pharmacists, Veterinary Surgeons, Nurses and other statutorily regulated healthcare professionals. Faculty members are medical professionals who are qualified and trained in both conventional medicine and Homeopathic medicine. This provides them with a unique perspective on healthcare and allows them to effectively integrate these various disciplines.
In addition to Membership and Academic activities, the Faculty’s other key areas of work include Promotion, Quality Assurance, and Publication of the international research journal, Homeopathy.
About homeopathy
Homeopathy is a natural form of medicine used by over 200 million people worldwide for both acute and chronic conditions. It is based on the principle of treating “like with like”. That is, a substance which causes symptoms when taken in large doses, can be used in small amounts to treat those same symptoms.
For example, drinking too much coffee can cause sleeplessness and agitation. According to this principle, when made into a Homeopathic medicine, this could be used to treat people with those symptoms. However, Homeopathic medicines use minimum doses of the active substance, which results in the medicines being non-toxic.
Homeopathy should be seen as a complementary treatment rather than an alternative to conventional medicine. Despite the differences in approach, Homeopathic and conventional treatments can work very well together and are frequently used as part of an integrative approach. Consulting a medical doctor who is trained in Homeopathy allows patients more treatment choices. www.facultyofhomeopathy.org
For more information or to arrange an interview with a member of the Faculty of Homeopathy please contact Chris Burton: [email protected] or telephone : 07533 913589
________________________________________________________
I did take up the kind offer to arrange an interview to be published on this blog. Yesterday early afternoon, I thus emailed Chris Burton. Sadly, this did not (yet?) result in a response. If he still does come back, I will post an interview at a later date.
Therefore, I have to leave you with the comment I gave to THE TIMES yesterday; part of which is in today’s paper together with quotes from two other critics of homeopathy:
Prince Charles’ endorsement might turn out to be a poisoned chalice. His reputation in science is not exactly the best, and his patronage will simply re-emphasise the many negative verdicts of independent experts on homeopathy. The European Academies Science Advisory Council, for instance, stated recently this: “… we acknowledge that a placebo effect may appear in individual patients but we agree with previous extensive evaluations concluding that there are no known diseases for which there is robust, reproducible evidence that homeopathy is effective beyond the placebo effect.”
I have recently been alerted to this remarkable article. It starts by telling the story of a patient who got rid of his alcohol addiction by using a homeopathic remedy. The story ends with these words: “It’s been two years now since I have been sober and I have no plans to consume alcohol ever gain.” Then the article continues:
This was Rahul’s story. Do you find your story quite similar to Rahul’s? Do you feel yourself falling down the abyss of addiction? Like you’ve lost control over your actions? Then Be like Rahul and take the first step. Join the 45 day No Alcohol challenge and see the difference for yourself.
There are Homeopathic Ingredients which work wonders in Getting You Rid of Addiction to Alcohol. Alcoban is a Homeopathic Anti-Addiction Treatment that helps you Overcome Addiction Using Homeopathy. It is one of the Most Trusted Homeopathic Anti-Addiction Treatment in the world. It can help an addict Beat Any Type of Addiction whether its tobacco, alcohol, drugs or anything else. Regular intake of this homeopathic formula gradually decreases the cravings of drinking. Continuous and prolonged use of Alcoban drop decreases cravings of bad things. You can Get Rid of Alcoholism with Alcoban Homeopathic Drop.
All the Effective Homeopathic Ingredients For Anti-Addiction present in Alcoban are individually quite effective in dealing with various symptoms of addiction but when combined together they form a potent formula that can Curb Tobacco Craving, Treat Alcohol Withdrawal Symptoms, make you Stop Using Drugs. Alcoban is also tasteless and colorless which means that it can be given without addict’s knowledge.
______________________________________________________________
Naturally, I was interested, not because I am an alcoholic but because I was intrigued by the homeopathic remedy and what it might contain. The Alcoban website itself informs us that:
Alcoban Drop is homeopathic anti-addiction formulation made utilizing the benefits of selective homeopathic ingredients, which are further processed as defined in Homeopathy to induce reluctance towards habit-forming mood-altering substances. The substances used in Alcoban detoxify the body for toxic materials deposited in the system from prolonged use of any such substance.
Alcoban is a potent remedy to stop and recover from substance abuse without facing the extreme withdrawal symptoms.
- Alcoban treatment suppresses cravings naturally.
- Alcoban helps in anxiety as well as yearnings.
- Alcoban is well suited to outpatient treatment.
- Alcoban acts as an anti-addiction treatment for tobacco, alcohol, drug, and smoking addiction.
- Alcoban treatment is holistic.
Precautions while using:
- People with severe heart ailments or any other major disease should use Alcoban only after consulting their physician.
- Pregnant or lactating females should avoid using it.
- If there is excessive vomiting on using Alcoban, the doses should be reduced. If there is still no change, then it should be stopped completely.
______________________________________________________________
Sadly, I could not find any information about Alcoban’s ingredients. Nor did I find any evidence that the product is effective. But I don’t give up that easily. A Medline search produced one paper on homeopathy for alcoholism:
This paper discusses the use of homoeopathy in the work of a community alcohol team, focusing on the application of homoeopathy for treating sleep disorder in alcohol-dependent clients. This work is placed in the context of the historical use of homoeopathy for treating ‘alcoholism’ and of the increasing use of complementary therapies in mainstream health care and in drug and alcohol agencies. Issues of research methodology and measurement of outcomes are examined. Examples of some specific homoeopathic treatments, together with a case report, are given to illustrate the potential uses of this form of therapy. It is concluded that homoeopathy can provide a valid and effective therapy to help clients break the cycle of dependence on alcohol. A number of further research questions arise and much clinical and research work needs to be done by those attempting to bring complementary therapies into drug and alcohol treatment.
The article is 22 years old and tells us very little. In particular it does not amount to anything like evidence of efficacy, nor does this indicate that there is much research going on in this area.
What can we conclude from all this?
Not a lot!
Perhaps that Alcoban is not just tasteless and colourless, as the Indian manufacturer proudly points out, but also useless?
In 2010, we published an investigation which revealed that the majority of chiropractors and their associations in the English speaking world seem to make therapeutic claims that are not supported by sound evidence, whilst only 28% of chiropractor websites promote lower back pain, which is supported by some evidence. If you go on the Internet (or just study this blog), you can easily see that the advertising of chiropractors is still far from adequate. Recently, a researcher investigated this issue systematically.
The aims of this survey were to determine the frequency, type and nature of at-risk advertising by Australian chiropractors and physiotherapists and whether there is a correlation between professional association membership and advertising guideline compliance. A cross sectional audit examining practitioner advertising was performed on representative samples of Australian chiropractors and physiotherapists. Two auditors examined advertising by 380 physiotherapists and 359 chiropractors for material potentially in breach of the regulatory authorities’ advertising guidelines. The advertising appeared on practitioner websites and linked Facebook pages.
Two-hundred and fifty-eight (72%) audited chiropractors and 231 (61%) audited physiotherapists had breaches of the Advertising Guidelines on their websites and linked Facebook pages. The frequency of breaches by chiropractors was higher. The type and nature of the breaches by chiropractors was potentially more harmful. Membership in a professional association influenced neither the frequency nor the severity of breaches with chiropractors.
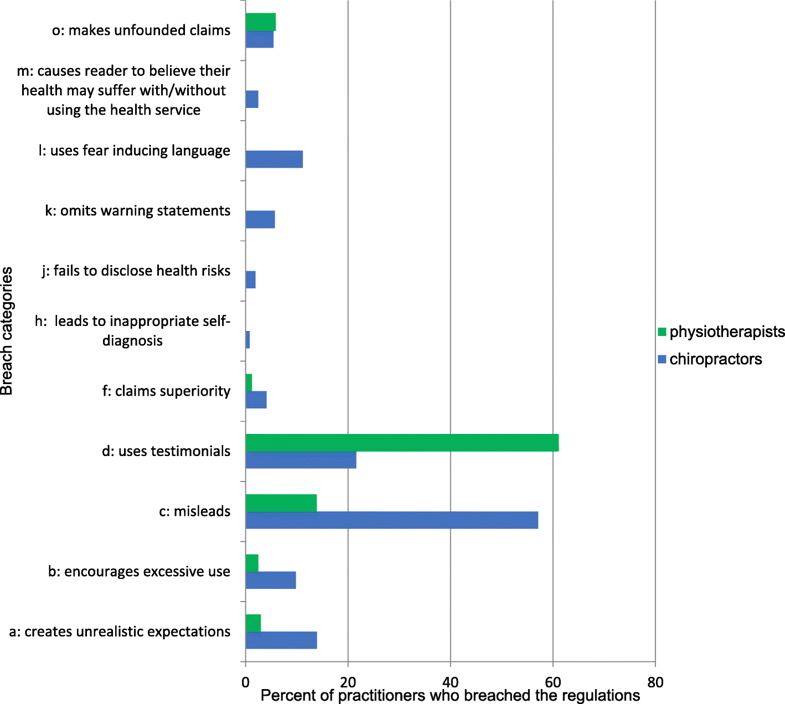 The nature (top graph) and the severity (bottom graph) of the false claims.
The nature (top graph) and the severity (bottom graph) of the false claims.
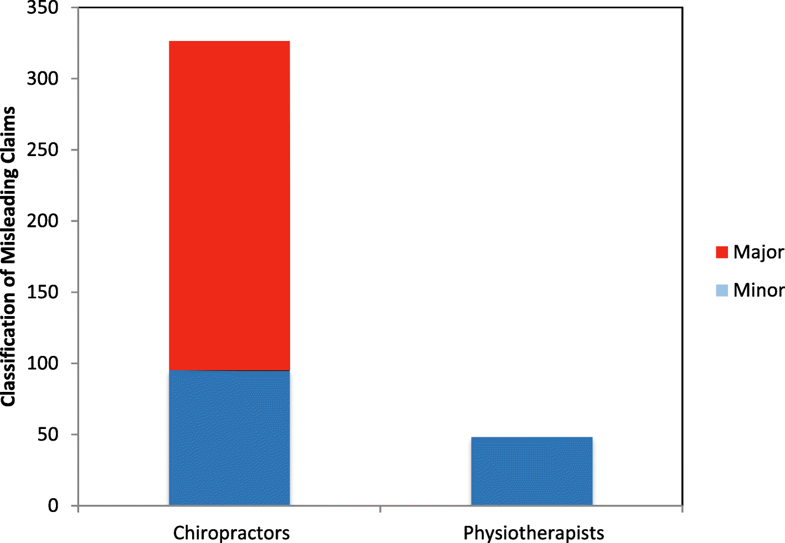 The author (who is affiliated with the Murdoch University, School of Chiropractic, Murdoch, Australia) concluded that advertising breaches were common in both samples even though regulators and professional associations provide practitioners with explicit information on how to comply with advertising guidelines. Breaches by chiropractors were more numerous and more serious due to their greater potential to lead consumers to make inappropriate and potentially harmful healthcare decisions.
The author (who is affiliated with the Murdoch University, School of Chiropractic, Murdoch, Australia) concluded that advertising breaches were common in both samples even though regulators and professional associations provide practitioners with explicit information on how to comply with advertising guidelines. Breaches by chiropractors were more numerous and more serious due to their greater potential to lead consumers to make inappropriate and potentially harmful healthcare decisions.
In the discussion section of the paper, the author makes this important comment:
The chiropractic findings are of major concern for two reasons, the first being public safety. Society expects and accepts that professionals advertise their services to assist consumers in making informed choices. To meet societal expectations and legal obligations, advertising must be socially responsible, truthful, appropriate and not misleading or deceptive. Advertising that fails to meet these expectations has the potential to harm. To assist practitioners in fulfilling their obligations, regulators formulated specific rules about advertising of health services to protect the rights of consumers however the data indicate that both professions and chiropractors in particular are not fulfilling their obligations.
The second reason is the high percentage of chiropractors advertising in an unacceptable manner. This raises questions about the profession’s culture and understanding of its obligations under the social contract. It is beyond the scope of this paper to examine this; however, this topic has been the subject of papers by observers both within the profession and external to it over several decades. The consensus is, although the profession has many of the trappings of a mainstream healthcare provider, (legislative recognition, high utilization rates, growing global footprint etc.), it is lacking in other key areas such as civic professionalism and upholding the social contract, both of which are critical components within health care. This research reinforces that position.
You might say that the findings of this investigation apply only to Australia. This is true, of course, but I see so much nonsense in advertisements by chiropractors from any country, that I very much doubt that elsewhere the situation is any better.
New evidence on adverse effects of manual therapy comes from an unexpected source. Here is the abstract of the paper:
The aim of this study was to investigate if mild or moderate adverse events after manual therapy has an impact on the chance to recover from back/neck pain in men and women. A prospective cohort study of 771 patients with at least three treatment sessions in a randomized controlled trial performed in January 2010 – December 2013. Adverse events within 24 h after each treatment were measured with questionnaires and categorized as: no, mild or moderate, based on bothersomeness. Outcome measure was the perceived recovery at seven weeks and at three months follow-up. Odds Ratios (OR) and 95% confidence intervals (CI) were calculated by Logistic regression to investigate the associations between the exposure and outcome, and to test and adjust for potential confounding. There were no statistically significant associations observed between the experience of mild or moderate adverse events and being recovered at the seven weeks follow-up. The only statistically significant association observed at the three months follow-up was for mild adverse events in men with an OR of 2.44, 95% CI: 1.24–4.80 in comparison to men with no adverse events. This study indicates that mild adverse events after manual therapy may be related to a better chance to recover in men.
________________________________________________
In my view this is a rather boring analysis of a bizarre hypothesis … were it not for a result that cropped up almost unintendedly: AE were reported in 81% of women and 66% of men. No severe irreversible AE were reported, but 178 AEs were rated as moderate to severe. As only symptoms within 24 h after the first three treatment session were reported, the true figures might even be larger.
These figures are considerably higher than previously reported. Our own systematic review of prospective studies suggested that AEs occur in approximately half of all patients receiving spinal manipulation. It follows, I think, that we have to discuss the question about risk versus benefit of manual treatments (such as spinal manipulations) even more critically than before.
I have recently given interviews to German, Austrian, French and Canadian journalists. They all had different perspectives, but they all had one question in common:
YOU ARE RETIRED AND COULD BE ENJOYING LIFE, WHY DO YOU CARRY ON WORKING?
And every time I was asked this question, I was surprised. To me, it seems perfectly natural to carry on. But having been asked several times, I did ponder: why do I do it? Here are some answers found through this exercise of introspection.
First let me list three reasons that my detractors regularly imply which, however, are all false:
- I do not do it for the money. In fact, I earn nothing from writing this blog and even have to pay for the pleasure.
- I do not do it because of a bad personal experience; such an event does simply not exist.
- I do not do it because I want to be famous.
So, why then?
The best reason I can give is that I feel a responsibility to do what I do. I am perhaps the only person on the planet who has studied so-called alternative medicine (SCAM) extensively and who, at the same time, has been critical about it. Practically all other full-time SCAM researchers are demonstrably less than critical about their subject (in case you know someone who isn’t, please tell me). And other SCAM critics are often (rightly or wrongly) dismissed by SCAM enthusiasts because they have never done original research on the subject. This does not easily work in my case.
The responsibility I feel relates to the abominable amount of false or unreliable information that is being published every day about SCAM. In my view, it harms and even endangers the life of many consumers and patients (see, for instance, this recent case). Confronted with this endless flow of seriously misleading information, I feel unable not to do anything about it. I thus see my work since retirement as an attempt to counter-balance this danger and to make a small contribution to progress.
If I am honest, I also have to admit that I am enjoying what I do. Thus the question ‘why don’t you enjoy life…?’ entirely misses the point. I have enough time to pursue my hobbies and, when I work on SCAM, I usually have plenty of fun.
In conclusion, I am retired and I enjoy life!