TCM
Acupuncture is usually promoted as a safe therapy. This may be good marketing but, sadly, it is not the truth. About 10% of all patients experience mild to moderate adverse effects such as pain or bleeding. In addition, there are well-documented complications, for instance:
However, there have been few reports of deaths due to pneumothorax after acupuncture treatment, especially focused on electroacupuncture.
Japanese authors recently reported an autopsy case of a man in his 60s who went into cardiopulmonary arrest and died immediately after receiving electroacupuncture. Postmortem computed tomography (PMCT) showed bilateral pneumothoraces, as well as the presence of numerous gold threads embedded subcutaneously. An autopsy revealed two ecchymoses in the right thoracic cavity and a pinhole injury on the lower lobe of the right lung, suggesting that the needles had penetrated the lung. There were marked emphysematous changes in the lung, suggesting that rupture of bullae might also have contributed to bilateral pneumothoraces and fatal outcomes. The acupuncture needles may have been drawn deeper into the body than at the time of insertion due to electrical pulses and muscle contraction, indicating the need for careful determination of treatment indications and technical safety measures, such as fail-safe mechanisms.
This is the first case report of fatal bilateral pneumothoraces after electroacupuncture reported in the English literature. This case sheds light on the safety of electroacupuncture and the need for special care when administering it to patients with pulmonary disease who may be at a higher risk of pneumothorax. This is also the first report of three-dimensional reconstructed PMCT images showing the whole-body distribution of embedded gold acupuncture threads, which is unusual.
One-sided pneumothoraxes are common events after acupuncture. Several hundred cases have been published and the vast majority of such incidents remain unpublished or even unnoticed. These events are not normally life-threatening. If ‘only’ one lung is punctured, the patient may experience breathing difficulties, but in many cases these are temporary and the patient soon recovers.
Yet a bilateral pneumothorax is an entirely different affair. If both lungs malfunction, the patient’s chances of survival are slim unless he/she is close to an intensive care unit.
You might think that it needs an especially ungifted acupuncturist to manage to puncture both lungs simultaneously. I might agree, but we need to consider that acupuncture needles are often inserted in a symmetrical fashion into the patient’s body. This means that, if the therapist puts a needle at one point of the thorax that is close to a lung, he is not unlikely to do the same on the other side.
And how does one prevent such disasters?
Easy:
- train acupuncturists properly,
- avoid needles on the upper thorax,
- or refuse acupuncture altogether.
This multicenter, randomized, sham-controlled trial was aimed at assessing the long-term efficacy of acupuncture for chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS). Men with moderate to severe CP/CPPS were recruited, regardless of prior exposure to acupuncture. They received sessions of acupuncture or sham acupuncture over 8 weeks, with a 24-week follow-up after treatment. Real acupuncture treatment was used to create the typical de qi sensation, whereas the sham acupuncture treatment (the authors state they used the Streitberger needle, but the drawing looks more as though they used our device) does not generate this feeling.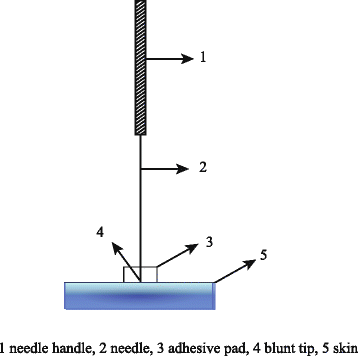
The primary outcome was the proportion of responders, defined as participants who achieved a clinically important reduction of at least 6 points from baseline on the National Institutes of Health Chronic Prostatitis Symptom Index at weeks 8 and 32. Ascertainment of sustained efficacy required the between-group difference to be statistically significant at both time points.
A total of 440 men (220 in each group) were recruited. At week 8, the proportions of responders were:
- 60.6% (95% CI, 53.7% to 67.1%) in the acupuncture group
- 36.8% (CI, 30.4% to 43.7%) in the sham acupuncture group (adjusted difference, 21.6 percentage points [CI, 12.8 to 30.4 percentage points]; adjusted odds ratio, 2.6 [CI, 1.8 to 4.0]; P < 0.001).
At week 32, the proportions were:
- 61.5% (CI, 54.5% to 68.1%) in the acupuncture group
- 38.3% (CI, 31.7% to 45.4%) in the sham acupuncture group (adjusted difference, 21.1 percentage points [CI, 12.2 to 30.1 percentage points]; adjusted odds ratio, 2.6 [CI, 1.7 to 3.9]; P < 0.001).
Twenty (9.1%) and 14 (6.4%) adverse events were reported in the acupuncture and sham acupuncture groups, respectively. No serious adverse events were reported. No significant difference was found in changes in the International Index of Erectile Function 5 score at all assessment time points or in peak and average urinary flow rates at week 8.
The authors concluded that, compared with sham therapy, 20 sessions of acupuncture over 8 weeks resulted in greater improvement in symptoms of moderate to severe CP/CPPS, with durable effects 24 weeks after treatment.
The study was sponsored by the China Academy of Chinese Medical Sciences and the National Administration of Traditional Chinese Medicine. The trialists originate from the following institutions:
- 1Guang’anmen Hospital, China Academy of Chinese Medical Sciences, Beijing, China (Y.S., B.L., Z.Q., J.Z., J.W., X.L., W.W., R.P., H.C., X.W., Z.L.).
- 2Key Laboratory of Chinese Internal Medicine of Ministry of Education, Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, China (Y.L.).
- 3ThedaCare Regional Medical Center – Appleton, Appleton, Wisconsin (K.Z.).
- 4Hengyang Hospital Affiliated to Hunan University of Chinese Medicine, Hengyang, China (Z.Y.).
- 5The First Hospital of Hunan University of Chinese Medicine, Changsha, China (W.Z.).
- 6Guangdong Provincial Hospital of Traditional Chinese Medicine, Guangzhou, China (W.F.).
- 7The First Affiliated Hospital of Anhui University of Chinese Medicine, Hefei, China (J.Y.).
- 8West China Hospital of Sichuan University, Chengdu, China (N.L.).
- 9China Academy of Chinese Medical Sciences, Beijing, China (L.H.).
- 10Yantai Hospital of Traditional Chinese Medicine, Yantai, China (Z.Z.).
- 11Shaanxi Provincial Hospital of Traditional Chinese Medicine, Xi’an, China (T.S.).
- 12The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, China (J.F.).
- 13Beijing Fengtai Hospital of Integrated Traditional and Western Medicine, Beijing, China (Y.D.).
- 14Xi’an TCM Brain Disease Hospital, Xi’an, China (H.S.).
- 15Dongfang Hospital Beijing University of Chinese Medicine, Beijing, China (H.H.).
- 16Luohu District Hospital of Traditional Chinese Medicine, Shenzhen, China (H.Z.).
- 17Guizhou University of Traditional Chinese Medicine, Guiyang, China (Q.M.).
These facts, together with the previously discussed notion that clinical trials from China are notoriously unreliable, do not inspire confidence. Moreover, one might well wonder about the authors’ claim that patients were blinded. As pointed out above, the real and sham acupuncture were fundamentally different: the former did generate de qi, while the latter did not! A slightly pedantic point is my suspicion that the trial did not test the efficacy but the effectiveness of acupuncture, if I am not mistaken. Finally, one might wonder what the rationale of acupuncture as a treatment of CP/CPPS might be. As far as I can see, there is no plausible mechanism (other than placebo) to explain the effects.
So, is the evidence that emerged from the new study convincing?
No, in my view, it is not!
In fact, I am surprised that a journal as reputable as the Annals of Internal Medicine published it.
This retrospective electronic medical record data analysis compared the characteristics and outcomes of drug-induced liver injury (DILI) caused by paracetamol and non-paracetamol medications, particularly herbal and dietary supplements. Adults admitted with DILI to the Gastroenterology and Liver Centre at the Royal Prince Alfred Hospital, Sydney (a quaternary referral liver transplantation centre), 2009-2020 were included. The 90-day transplant-free survival and the drugs implicated as causal agents in DILI were extracted from the records.
A total of 115 patients with paracetamol-related DILI and 69 with non-paracetamol DILI were admitted to our centre. The most frequently implicated non-paracetamol medications were:
- antibiotics (19, 28%),
- herbal and dietary supplements (15, 22%),
- anti-tuberculosis medications (6, 9%),
- anti-cancer medications (5, 7%).
The number of non-paracetamol DILI admissions was similar across the study period, but the proportion linked with herbal and dietary supplements increased from 2 of 11 (15%) during 2009-11 to 10 of 19 (47%) during 2018-20 (linear trend: P = 0.011). Despite higher median baseline model for end-stage liver disease (MELD) scores, 90-day transplant-free survival for patients with paracetamol-related DILI was higher than for patients with non-paracetamol DILI (86%; 95% CI, 79-93% v 71%; 95% CI, 60-82%) and herbal and dietary supplement-related cases (59%; 95% CI, 34-85%). MELD score was an independent predictor of poorer 90-day transplant-free survival in both paracetamol-related (per point increase: adjusted hazard ratio [aHR], 1.19; 95% CI, 1.09-3.74) and non-paracetamol DILI (aHR, 1.24; 95% CI, 1.14-1.36).
The authors concluded that, in our single centre study, the proportion of cases of people hospitalised with DILI linked with herbal and dietary supplements has increased since 2009. Ninety-day transplant-free survival for patients with non-paracetamol DILI, especially those with supplement-related DILI, is poorer than for those with paracetamol-related DILI.
A co-author of the paper, specialist transplant hepatologist Dr Ken Liu, was quoted in the Guardian saying he felt compelled to conduct the study because he was noticing more patients with liver injuries from drugs not typically associated with liver harm. “I was starting to see injury in patients admitted with liver injury after using bodybuilding supplements for males or weight loss supplements in females,” he said. “I just decided I better do a study on it to see if my hunch that more of these substances were causing these injuries was true.”
Liu and his colleagues said there needed to be more rigorous regulatory oversight for supplements and other alternative and natural therapies. They also noticed almost half the patients with supplement-induced severe liver injury had non-European ethnic backgrounds. Liu said more culturally appropriate community education about the risks of supplements was needed.
Dr Ken Harvey, public health physician and president of Friends of Science in Medicine, said it was important to note that Liu’s study only examined the most severe cases of supplement-induced liver harm and that the actual rate of harm was likely much higher. “The study only examines severe cases admitted to a specialised liver unit; they cannot be extrapolated to the overall incidence of complementary medicine associated liver injury in Australia,” Harvey said.
The Royal Australian College of General Practitioners, Choice, Friends of Science in Medicine and others have called for an educational statement on the pack and promotional material of medicines making traditional claims, for example saying “This product is based on traditional beliefs and not modern scientific evidence”.
“This was opposed by industry and the TGA,” Harvey said. “But is still needed.”
This overview was aimed at critically appraising the best available systematic review (SR) evidence on the health
effects of Tai Chi. Nine databases (English and Chinese languages) were searched for SRs of controlled clinical trials of Tai Chi interventions published between Jan-2010 and Dec-2020 in any language. Excluded were primary studies and meta-analyses that combined Tai Chi with other interventions. To minimize overlap, effect estimates were extracted from the most recent, comprehensive, highest quality SR for each population, condition, and outcome. SR quality was appraised using AMSTAR 2 and effect estimates with GRADE.
Of the 210 included SRs, 193 only included randomized controlled trials, one only included non-randomized
studies of interventions, and 16 included both. The most common conditions were neurological (18.6%), falls/balance (14.7%), cardiovascular (14.7%), musculoskeletal (11.0%), cancer (7.1%) and diabetes mellitus (6.7%). Except for stroke, no evidence for disease prevention was found, instead, proxy-outcomes/risks factors were evaluated. 114 effect estimates were extracted from 37 SRs (2 high quality, 6 moderate, 18 low, and 11 critically low), representing 59,306 adults. Compared to active and/or inactive controls, a clinically important benefit from Tai Chi was reported for 66 effect estimates; 53 reported an equivalent or marginal benefit, and 6 had an equivalent risk of adverse events. Eight effect estimates (7.0%) were graded as high certainty evidence, 43 (37.7%) moderate, 36 (31.6%) low, and 27 (23.7%) very low. This was due to concerns with risk of bias in 92 (80.7%) effect estimates, imprecision in 43 (37.7%), inconsistency in 37 (32.5%), and publication bias in 3 (2.6%). SR quality was limited by the search strategies, language bias, inadequate consideration of clinical, methodological, and statistical heterogeneity, poor reporting standards, and/or no registered protocol.
The authors concluded that the findings suggest Tai Chi has multisystem effects with physical, psychological, and quality of life benefits for a wide range of conditions, including individuals with multiple health problems. Clinically important benefits were most consistently reported for Parkinson’s disease, falls risk, knee osteoarthritis, low back pain, cardiovascular diseases including hypertension, and stroke. Notwithstanding, for most conditions, higher quality primary studies and SRs are required.
The authors start the discussion section by stating: This critical overview comprehensively identified SRs of Tai Chi published in English, Chinese and Korean languages that evaluated the effectiveness and safety of Tai Chi for health promotion, and disease prevention and management.
I must say that I do not find the overview all that ,critical’. The authors admit that the primary studies often lacked scientific rigor. Yet they draw firm positive conclusions from the data. I think that this is wrong.
Most of the authors of this overview come from Chinese institutions dedicated to promoting TCM. Yet there is no declaration that this fact might constitute a conflict of interest.
I also miss critical comments on two important questions:
- Are the positive effects of Tai chi superior to conventional treatments of the respective conditions?
- Are the effects of Tai chi really due to the treatment per see or might they be largely caused by context effects (which, considering the nature of the therapy, might be substantial)?
Acupuncture is a veritable panacea; it cures everything! At least this is what many of its advocates want us to believe. Does it also have a role in supportive cancer care?
Let’s find out.
This systematic review evaluated the effects of acupuncture in women with breast cancer (BC), focusing on patient-reported outcomes (PROs).
A comprehensive literature search was carried out for randomized controlled trials (RCTs) reporting PROs in BC patients with treatment-related symptoms after undergoing acupuncture for at least four weeks. Literature screening, data extraction, and risk bias assessment were independently carried out by two researchers. The authors stated that they followed the ‘Preferred Reporting Items for Systematic Review and Meta-Analyses’ (PRISMA) guidelines.
Out of the 2, 524 identified studies, 29 studies representing 33 articles were included in this meta-analysis. The RCTs employed various acupuncture techniques with a needle, such as hand-acupuncture and electroacupuncture. Sham/placebo acupuncture, pharmacotherapy, no intervention, or usual care were the control interventions. About half of the studies lacked adequate blinding.
At the end of treatment (EOT), the acupuncture patients’ quality of life (QoL) was measured by the QLQ-C30 QoL subscale, the Functional Assessment of Cancer Therapy-Endocrine Symptoms (FACT-ES), the Functional Assessment of Cancer Therapy–General/Breast (FACT-G/B), and the Menopause-Specific Quality of Life Questionnaire (MENQOL), which depicted a significant improvement. The use of acupuncture in BC patients lead to a considerable reduction in the scores of all subscales of the Brief Pain Inventory-Short Form (BPI-SF) and Visual Analog Scale (VAS) measuring pain. Moreover, patients treated with acupuncture were more likely to experience improvements in hot flashes scores, fatigue, sleep disturbance, and anxiety compared to those in the control group, while the improvements in depression were comparable across both groups. Long-term follow-up results were similar to the EOT results. Eleven RCTs did not report any information on adverse effects.
The authors concluded that current evidence suggests that acupuncture might improve BC treatment-related symptoms measured with PROs including QoL, pain, fatigue, hot flashes, sleep disturbance and anxiety. However, a number of included studies report limited amounts of certain subgroup settings, thus more rigorous, well-designed and larger RCTs are needed to confirm our results.
This review looks rigorous on the surface but has many weaknesses if one digs only a little deeper. To start with, it has no precise research question: is any type of acupuncture better than any type of control? This is not a research question that anyone can answer with just a few studies of mostly poor quality. The authors claim to follow the PRISMA guidelines, yet (as a co-author of these guidelines) I can assure you that this is not true. Many of the included studies are small and lacked blinding. The results are confusing, contradictory and not clearly reported. Many trials fail to mention adverse effects and thus violate research ethics, etc., etc.
The conclusion that acupuncture might improve BC treatment-related symptoms could be true. But does this paper convince me that acupuncture DOES improve these symptoms?
No!
Qigong can be described as a mind-body-spirit practice that improves one’s mental and physical health by integrating posture, movement, breathing technique, self-massage, sound, and focused intent. But does it really improve health?
The purpose of this review was to evaluate the effectiveness of Qigong in improving the quality of life and relieving fatigue, sleep disturbance, and cancer-related emotional disturbances (distress, depression, and anxiety) in women with breast cancer.
The PubMed, Cochrane Central Register of Controlled Trials, Web of Science, Sinomed, Wanfang, VIP, and China National Knowledge Infrastructure databases were searched from their inceptions to March 2020 for controlled clinical trials. Two reviewers selected relevant trials that assessed the benefit of Qigong for breast cancer patients independently. A methodological quality assessment was conducted according to the criteria of the 12 Cochrane Back Review Group for risk of bias independently. A meta-analysis was performed using Review Manager 5.3.
A total of 17 trials were found in which 1236 cases were enrolled. The quality of the included trials was generally low, as only 5 of them were rated high quality. 14 studies were conducted in China. The types of qigong included Baduanjin Qigong (9 trials), Chan-Chuang Qigong (1 trial), Goulin New Qigong (2 Trials), Tai Chi Qigong (2 Trials), and Kuala Lumpur Qigong (1 trial). The course of qigong ranged from 21 days to more than 6 months. Four trials compared qigong to no treatment, one sham Qigong, seven compared to other types of exercise, and 6 to usual care.
The results showed significant positive effects of Qigong on quality of life (n = 950, standardized mean difference (SMD), 0.65, 95 % confidence interval (CI) 0.23–1.08, P = 0.002). Depression (n = 540, SMD = −0.32, 95 % CI −0.59 to −0.04, P = 0.02) and anxiety (n = 439, SMD = −0.71, 95 % CI −1.32 to −0.10, P = 0.02) were also significantly relieved in the Qigong group. There was no significant benefit on fatigue (n = 401, SMD = −0.32, 95 % CI 0.71 to 0.07, P = 0.11) or sleep disturbance relief compared to that observed in the control group (n = 298, SMD = −0.11, 95 % CI 0.74 to 0.52, P = 0.73). 
The authors concluded that this review shows that Qigong is beneficial for improving quality of life and relieving depression and anxiety; thus, Qigong should be encouraged in women with breast cancer.
No, this review does not show that Qigong is beneficial for improving quality of life and relieving depression and anxiety!
Why?
- Most primary studies were of very poor quality.
- Most were from China, and we know (and have often discussed) that such trials are most unreliable.
- No trial even attempted to control for placebo effects.
A better conclusion would therefore be something like this:
Even though most trials conclude positively, the value of Qigong can, for a range of reasons, not be determined on the basis of the evidence available to date.
Tai chi is a form of exercise that combines deep breathing and relaxation with meditative, slow movements. Originally developed as a martial art in 13th-century China, tai chi is now practised around the world as a health-promoting exercise. Despite its popularity, its therapeutic value is not clear. 
This randomized, assessor-blinded trial examined the therapeutic efficacy of tai chi for the management of central obesity. A total of 543 participants with central obesity were randomly assigned in a 1:1:1 ratio to:
- a control group with no exercise intervention (n = 181),
- conventional exercise consisting of aerobic exercise and strength training (EX group) (n = 181),
- a tai chi group (TC group) (n = 181). Interventions lasted 12 weeks.
Outcomes were assessed at baseline, week 12, and week 38. The primary outcome was waist circumference (WC). Secondary outcomes were body weight; body mass index; high-density lipoprotein cholesterol (HDL-C), triglyceride, and fasting plasma glucose levels; blood pressure; and incidence of remission of central obesity.
The adjusted mean difference in WC from baseline to week 12 in the control group was 0.8 cm (95% CI, -4.1 to 5.7 cm). Both intervention groups showed reductions in WC relative to control (adjusted mean differences: TC group vs. control, -1.8 cm [CI, -2.3 to -1.4 cm]; P < 0.001; EX group vs. control: -1.3 cm [CI, -1.8 to -0.9 cm]; P < 0.001); both intervention groups also showed reductions in body weight (P < 0.05) and attenuation of the decrease in HDL-C level relative to the control group. The favorable changes in WC and body weight were maintained in both the TC and EX groups, whereas the beneficial effect on HDL-C was only maintained in the TC group at week 38.
The authors concluded that Tai chi is an effective approach to reduce WC in adults with central obesity aged 50 years or older.
This is a decent trial with an odd conclusion: it is not just the Tai chi intervention but both types of exercise that yield significantly positive effects on the primary outcome measure. So, why did the authors not conclude exercise is an effective approach to reduce WC in adults with central obesity aged 50 years or older?
Could it be that such a conclusion would have meant stating the obvious?
Neuropathic pain is difficult to treat. Luckily, we have acupuncture! Acupuncturists leave us in no doubt that their needles are the solution. But are they correct or perhaps victims of wishful thinking?
This review was aimed at determining the proportion of patients with neuropathic pain who achieve a clinically meaningful improvement in their pain with the use of different pharmacologic and nonpharmacologic treatments.
Randomized controlled trials were included that reported a responder analysis of adults with neuropathic pain-specifically diabetic neuropathy, postherpetic neuralgia, or trigeminal neuralgia-treated with any of the following 8 treatments: exercise, acupuncture, serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), topical rubefacients, opioids, anticonvulsant medications, and topical lidocaine.
A total of 67 randomized controlled trials were included. There was moderate certainty of evidence that anticonvulsant medications (risk ratio of 1.54; 95% CI 1.45 to 1.63; number needed to treat [NNT] of 7) and SNRIs (risk ratio of 1.45; 95% CI 1.33 to 1.59; NNT = 7) might provide a clinically meaningful benefit to patients with neuropathic pain. There was low certainty of evidence for a clinically meaningful benefit for rubefacients (ie, capsaicin; NNT = 7) and opioids (NNT = 8), and very low certainty of evidence for TCAs. Very low-quality evidence demonstrated that acupuncture was ineffective. All drug classes, except TCAs, had a greater likelihood of deriving a clinically meaningful benefit than having withdrawals due to adverse events (number needed to harm between 12 and 15). No trials met the inclusion criteria for exercise or lidocaine, nor were any trials identified for trigeminal neuralgia.
The authors concluded that there is moderate certainty of evidence that anticonvulsant medications and SNRIs provide a clinically meaningful reduction in pain in those with neuropathic pain, with lower certainty of evidence for rubefacients and opioids, and very low certainty of evidence for TCAs. Owing to low-quality evidence for many interventions, future high-quality trials that report responder analyses will be important to strengthen understanding of the relative benefits and harms of treatments in patients with neuropathic pain.
This review was published in a respected mainstream journal and conducted by a multidisciplinary team with the following titles and affiliations:
- Associate Professor in the College of Pharmacy at the University of Manitoba in Winnipeg.
- Pharmacist in Edmonton, Alta, and Clinical Evidence Expert for the College of Family Physicians of Canada.
- Family physician and Assistant Professor at the University of Alberta.
- Family physician and Associate Professor in the Department of Family Medicine at the University of Alberta.
- Pharmacist, Clinical Evidence Expert Lead for the College of Family Physicians of Canada, and Associate Clinical Professor in the Department of Family Medicine at the University of Alberta.
- Pharmacist in Edmonton and Clinical Evidence Expert for the College of Family Physicians of Canada.
- Pharmacist and Clinical Evidence Expert at the College of Family Physicians of Canada.
- Family physician, Director of Programs and Practice Support at the College of Family Physicians of Canada, and Adjunct Professor in the Department of Family Medicine at the University of Alberta.
- Professor in the Faculty of Pharmaceutical Sciences at the University of British Columbia in Vancouver.
- Pharmacist at the CIUSSS du Nord-de-l’lle-de-Montréal and Clinical Associate Professor in the Faculty of Pharmacy at the University of Montreal in Quebec.
- Care of the elderly physician and Assistant Professor in the Department of Family Medicine at the University of Alberta.
- Family physician and Professor in the Department of Family Medicine at the University of Alberta.
- Assistant Professor in the Department of Family Medicine at Queen’s University in Kingston, Ont.
- Research assistant at the University of Alberta.
- Medical student at the University of Alberta.
- Nurse in Edmonton and Clinical Evidence Expert for the College of Family Physicians of Canada.
As far as I can see, the review is of sound methodology, it minimizes bias, and its conclusions are therefore trustworthy. They suggest that acupuncture is not effective for neuropathic pain.
But how can this be? Do the authors not know about all the positive evidence on acupuncture? A quick search found positive recent reviews of acupuncture for all of the three indications in question:
- Diabetic neuropathy: Acupuncture alone and vitamin B combined with acupuncture are more effective in treating DPN compared to vitamin B.
- Herpes zoster: Acupuncture may be effective for patients with HZ.
- Trigeminal neuralgia: Acupuncture appears more effective than pharmacotherapy or surgery.
How can we explain this obvious contradiction?
Which result should we trust?
Do we believe pro-acupuncture researchers who published their papers in pro-acupuncture journals, or do we believe the findings of researchers who could not care less whether their work proves or disproves the effectiveness of acupuncture?
I think that these papers offer an exemplary opportunity for us to study how powerful the biases of researchers can be. They also remind us that, in the realm of so-called alternative medicine (SCAM), we should always be very cautious and not accept every conclusion that has been published in supposedly peer-reviewed medical journals.
Qigong is a branch of Traditional Chinese Medicine using meditation, exercise, deep breathing, and other techniques with a view of strengthening the assumed life force ‘qi’ and thus improving health and prolong life. There are several distinct forms of qigong which can be categorized into two main groups, internal qigong, and external qigong. Internal qigong refers to a physical and mental training method for the cultivation of oneself to achieve optimal health in both mind and body. Internal qigong is not dissimilar to tai chi but it also employs the coordination of different breathing patterns and meditation. External qigong refers to a treatment where qigong practitioners direct their qi-energy to the patient with the intention to clear qi-blockages or balance the flow of qi within that patient. According to Taoist and Buddhist beliefs, qigong allows access to higher realms of awareness. The assumptions of qigong are not scientifically plausible and its clinical effectiveness remains unproven.
The aim of this study was to investigate the effects of internal Qigong for the management of a symptom cluster comprising fatigue, dyspnea, and anxiety in patients with lung cancer.
A total of 156 lung cancer patients participated in this trial, and they were randomized to a Qigong group (6 weeks of intervention) or a waitlist control group receiving usual care. A professional coach with 12 years of experience in teaching Qigong was employed to guide the participants’ training. The training protocol was developed according to the “Qigong Standard” enacted by the Chulalongkorn University, Thailand. The training involved a series of simple, repeated practices including body posture/movement, breathing practice, and meditation performed in synchrony. It mainly consisted of gentle movements designed to bring about a deep state of relaxation and included 7 postures. The symptom cluster was assessed at baseline, at the end of treatment (primary outcome), and at 12 weeks, alongside measures of cough and quality of life (QOL).
The results showed no significant interaction effect between group and time for the symptom cluster, the primary outcome measure of this study, overall and for fatigue and anxiety. However, a significant trend towards improvement was observed on fatigue (P = .004), dyspnea (P = .002), and anxiety (P = .049) in the Qigong group from baseline assessment to the end of intervention at the 6th week (within-group changes). Improvements in dyspnea and in the secondary outcomes of cough, global health status, functional well-being and QOL symptom scales were statistically significant between the 2 groups (P = .001, .014, .021, .001, and .002, respectively).
The authors concluded that Qigong did not alleviate the symptom cluster experience. Nevertheless, this intervention was effective in reducing dyspnea and cough, and improving QOL. More than 6 weeks were needed, however, for detecting the effect of Qigong on improving dyspnea. Furthermore, men benefited more than women. It may not be beneficial to use Qigong to manage the symptom cluster consisting of fatigue, dyspnea, and anxiety, but it may be effective in managing respiratory symptoms (secondary outcomes needing further verification in future research). Future studies targeting symptom clusters should ensure the appropriateness of the combination of symptoms.
I am getting very tired of negative trials getting published as (almost) positive ones. The primary outcome measure of this study did not yield a positive result. The fact that some other endpoints suggested a positive might provide an impetus for further study but does not demonstrate Qigong to be effective. I know the first author of this study is a fan of so-called alternative medicine (SCAM), but this should not stop him from doing proper science.
Thread embedding acupuncture therapy (TEAT) involves the insertion of thread at specific points on the body surface. The claim is that TEAT provides a sustained stimulation of acupoints and is therefore superior to needle acupuncture. Initially, TEAT was used in China to treat obesity, today it is employed to treat many conditions, including musculoskeletal conditions such as ankle sprain, shoulder pain, lumbar intervertebral disc herniation, and plantar fasciitis. Its effectiveness is, however, doubtful and so is its safety.
This review evaluated the safety of thread embedding acupuncture therapy (TEAT) and discuss the prevention and treatment of some adverse events (AEs).
Databases, including China National Knowledge Infrastructure (CNKI), CBMdisc, Wanfang, VIP databases and PubMed, MEDLINE, EMBASE, and Web of Science, were searched from their inception to January 2020. Included were randomized controlled trials (RCTs) and case reports in which AEs with TEAT were reported. Cochrane Collaboration’s tool and RevMan V.5.3.3 software were used to evaluate the quality of the studies.
A total of 61 articles (45 RCTs and 16 case reports) with a total of 620 cases of AEs were included in this review. These studies were published in two countries: China and South Korea. Twenty-eight kinds of AEs were noted. The most common AEs were induration, bleeding and ecchymosis, redness and swelling, fever, and pain. They accounted for 75.35% of all AEs. Most AEs were mild.; The rarest AEs were epilepsy, irregular menstruation, skin ulcer, thread malabsorption, and fat liquefaction, with 1 case each. Not all of them had a clear causal relationship with TEAT. Most of the AEs were local reactions and systemic reactions accounted for only 1.27%. Although the included studies showed that AEs were very commonly encountered (11.09%), only 5 cases of severe AEs reported from 2013 to 2017 (0.1%) by using catgut thread, which is rarely employed nowadays with new absorbable surgical suture being more popular. All of the patients with severe AEs were recovered after symptomatic treatment with no sequelae.
The authors concluded that the evidence showed that TEAT is a relatively safe and convenient therapy especially since application of new absorbable surgical suture. Improving practitioner skills, regulating operations, and paying attention to the patients’ conditions may reduce the incidence of AEs and improve safety of TEAT.
TEAT was initially used in China only but recently it has become popular elsewhere as well. Therefore the question about its risks has become relevant. The present paper is interesting in that it demonstrates that AEs do occur with some regularity. The authors’ conclusion that TEAT is “relatively safe” is, however, not justified because:
- the total sample size was not large enough for a generalizable conclusion;
- only RCTs and case reports were included, whereas case series and case-control studies (which would provide more relevant data) were excluded or might not even exist;
- RCTs of acupuncture often fail to mention or under-report AEs;
- acupuncture papers from China are notoriously unreliable.
So, all we can conclude from the evidence presented here is that AEs after TEAT do occur and do not seem to be all that rare. As the efficacy of TEAT has not been shown beyond doubt, this must inevitably lead to the conclusion that the risk-benefit balance of TEAT is not positive. In turn, that means that TEAT cannot be recommended as a treatment for any condition.