study design
Radix Salviae Miltiorrhizae (Danshen) is a herbal remedy that is part of many TCM herbal mixtures. Allegedly, Danshen has been used in clinical practice for over 2000 years.
But is it effective?
The aim of this systematic review was to evaluate the current available evidence of Danshen for the treatment of cancer. English and Chinese electronic databases were searched from PubMed, the Cochrane Library, EMBASE, and the China National Knowledge Infrastructure (CNKI), VIP database, Wanfang database until September 2018. The methodological quality of the included studies was evaluated by using the method of Cochrane system.
Thirteen RCTs with 1045 participants were identified. The studies investigated the lung cancer (n = 5), leukemia (n = 3), liver cancer (n = 3), breast or colon cancer (n = 1), and gastric cancer (n = 1). A total of 83 traditional Chinese medicines were used in all prescriptions and there were three different dosage forms. The meta-analysis suggested that Danshen formulae had a significant effect on RR (response rate) (OR 2.38, 95% CI 1.66-3.42), 1-year survival (OR 1.70 95% CI 1.22-2.36), 3-year survival (OR 2.78, 95% CI 1.62-4.78), and 5-year survival (OR 8.45, 95% CI 2.53-28.27).
The authors concluded that the current research results showed that Danshen formulae combined with chemotherapy for cancer treatment was better than conventional drug treatment plan alone.

I am getting a little tired of discussing systematic reviews of so-called alternative medicine (SCAM) that are little more than promotion, free of good science. But, because such articles do seriously endanger the life of many patients, I do nevertheless succumb occasionally. So here are a few points to explain why the conclusions of the Chinese authors are nonsense:
- Even though the authors claim the trials included in their review were of high quality, most were, in fact, flimsy.
- The trials used no less than 83 different herbal mixtures of dubious quality containing Danshen. It is therefore not possible to define which mixture worked and which did not.
- There is no detailed discussion of the adverse effects and no mention of possible herb-drug interactions.
- There seemed to be a sizable publication bias hidden in the data.
- All the eligible studies were conducted in China, and we know that such trials are unreliable to say the least.
- Only four articles were published in English which means those of us who cannot read Chinese are unable to check the correctness of the data extraction of the review authors.
I know it sounds terribly chauvinistic, but I do truly believe that we should simply ignore Chinese articles, if they have defects that set our alarm bells ringing – if not, we are likely to do a significant disservice to healthcare and progress.
Chiropractic spinal manipulative therapy (CSMT) for migraine?
Why?
There is no good evidence that it works!
On the contrary, there is good evidence that it does NOT work!
A recent and rigorous study (conducted by chiropractors!) tested the efficacy of chiropractic CSMT for migraine. It was designed as a three-armed, single-blinded, placebo -controlled RCT of 17 months duration including 104 migraineurs with at least one migraine attack per month. Active treatment consisted of CSMT (group 1) and the placebo was a sham push manoeuvre of the lateral edge of the scapula and/or the gluteal region (group 2). The control group continued their usual pharmacological management (group 3). The results show that migraine days were significantly reduced within all three groups from baseline to post-treatment. The effect continued in the CSMT and placebo groups at all follow-up time points (groups 1 and 2), whereas the control group (group 3) returned to baseline. The reduction in migraine days was not significantly different between the groups. Migraine duration and headache index were reduced significantly more in the CSMT than in group 3 towards the end of follow-up. Adverse events were few, mild and transient. Blinding was sustained throughout the RCT. The authors concluded that the effect of CSMT observed in our study is probably due to a placebo response.
One can understand that, for chiropractors, this finding is upsetting. After all, they earn a good part of their living by treating migraineurs. They don’t want to lose patients and, at the same time, they need to claim to practise evidence-based medicine.
What is the way out of this dilemma?
Simple!
They only need to publish a review in which they dilute the irritatingly negative result of the above trial by including all previous low-quality trials with false-positive results and thus generate a new overall finding that alleges CSMT to be evidence-based.
This new systematic review of randomized clinical trials (RCTs) evaluated the evidence regarding spinal manipulation as an alternative or integrative therapy in reducing migraine pain and disability.
The searches identified 6 RCTs eligible for meta-analysis. Intervention duration ranged from 2 to 6 months; outcomes included measures of migraine days (primary outcome), migraine pain/intensity, and migraine disability. Methodological quality varied across the studies. The results showed that spinal manipulation reduced migraine days with an overall small effect size as well as migraine pain/intensity.
The authors concluded that spinal manipulation may be an effective therapeutic technique to reduce migraine days and pain/intensity. However, given the limitations to studies included in this meta-analysis, we consider these results to be preliminary. Methodologically rigorous, large-scale RCTs are warranted to better inform the evidence base for spinal manipulation as a treatment for migraine.
Bob’s your uncle!
Perhaps not perfect, but at least the chiropractic profession can now continue to claim they practice something akin to evidence-based medicine, while happily cashing in on selling their unproven treatments to migraineurs!
But that’s not very fair; research is not for promotion, research is for finding the truth; this white-wash is not in the best interest of patients! I hear you say.
Who cares about fairness, truth or conflicts of interest?
Christine Goertz, one of the review-authors, has received funding from the NCMIC Foundation and served as the Director of the Inter‐Institutional Network for Chiropractic Research (IINCR). Peter M. Wayne, another author, has received funding from the NCMIC Foundation and served as the co‐Director of the Inter‐Institutional Network for Chiropractic Research (IINCR)
And who the Dickens are the NCMIC and the IINCR?
At NCMIC, they believe that supporting the chiropractic profession, including chiropractic research programs and projects, is an important part of our heritage. They also offer business training and malpractice risk management seminars and resources to D.C.s as a complement to the education provided by the chiropractic colleges.
The IINCR is a collaborative effort between PCCR, Yale Center for Medical Informatics and the Osher Center for Integrative Medicine at Brigham and Women’s Hospital and Harvard Medical School. They aim at creating a chiropractic research portfolio that’s truly translational. Vice Chancellor for Research and Health Policy at Palmer College of Chiropractic Christine Goertz, DC, PhD (PCCR) is the network director. Peter Wayne, PhD (Osher Center for Integrative Medicine at Brigham and Women’s Hospital and Harvard Medical School) will join Anthony J. Lisi, DC (Yale Center for Medical Informatics and VA Connecticut Healthcare System) as a co-director. These investigators will form a robust foundation to advance chiropractic science, practice and policy. “Our collective efforts provide an unprecedented opportunity to conduct clinical and basic research that advances chiropractic research and evidence-based clinical practice, ultimately benefiting the patients we serve,” said Christine Goertz.
Really: benefiting the patients?
You could have fooled me!
The aim of this new systematic review was to evaluate the controlled trials of homeopathy in bronchial asthma. Relevant trials published between Jan 1, 1981, and Dec 31, 2016, were considered. Substantive research articles, conference proceedings, and master and doctoral theses were eligible. Methodology was assessed by Jadad’s scoring, internal validity by the Coch-rane tool, model validity by Mathie’s criteria, and quality of individualization by Saha’s criteria.
Sixteen trials were eligible. The majority were positive, especially those testing complex formulations. Methodological quality was diverse; 8 trials had “high” risk of bias. Model validity and individualization quality were compromised. Due to both qualitative and quantitative inadequacies, proofs supporting individualized homeopathy remained inconclusive. The trials were positive (evidence level A), but inconsistent, and suffered from methodological heterogeneity, “high” to “uncertain” risk of bias, incomplete study reporting, inadequacy of independent replications, and small sample sizes.
The authors of this review come from:
- the Department of Homeopathy, District Joint Hospital, Government of Bihar, Darbhanga, India;
- the Department of Organon of Medicine and Homoeopathic Philosophy, Sri Sai Nath Postgraduate Institute of Homoeopathy, Allahabad, India;
- the Homoeopathy University Jaipur, Jaipur, India;
- the Central Council of Homeopathy, Hooghly,
- the Central Council of Homeopathy, Howrah, India
They state that they have no conflicts of interest.
The review is puzzling on so many accounts that I had to read it several times to understand it. Here are just some of its many oddities:
- According to its authors, the review adhered to the PRISMA-P guideline; as a co-author of this guideline, I can confirm that this is incorrect.
- The authors claim to have included all ‘controlled trials (randomized, non-randomized, or observational) of any form of homeopathy in patients suffering from persistent and chronic bronchial asthma’. In fact, they also included uncontrolled studies (16 controlled trials and 12 uncontrolled observational studies, to be precise).
- The authors included papers published between Jan 1, 1981, and Dec 31, 2016. It is unacceptable, in my view, to limit a systematic review in this way. It also means that the review was seriously out of date already on the day it was published.
- The authors tell us that they applied no language restrictions. Yet they do not inform us how they handled papers in foreign languages.
- Studies of homeopathy as a stand alone therapy were included together with studies of homeopathy as an adjunct. Yet the authors fail to point out which studies belonged to which category.
- Several of the included studies are not of homeopathy but of isopathy.
- The authors fail to detail their results and instead refer to an ‘online results table’ which I cannot access even though I have the on-line paper.
- Instead, they report that 28 studies were included and ‘thus, the level of evidence was graded as A.’
- No direction of outcome was provided in the results section. All we do learn from the paper’s discussion section is that ‘the majority of the studies were positive, and the level of evidence could be graded as A (strong scientific evidence)’.
- Despite the high risk of bias in most of the included studies, the authors suggest a ‘definite role of homeopathy beyond placebo in the treatment of bronchial asthma’.
- The current Cochrane review (also authored by a pro-homeopathy team) concluded that there is not enough evidence to reliably assess the possible role of homeopathy in asthma. Yet the authors of this new review do not even attempt to explain the contradiction.
Confusion?
Incompetence?
Scientific misconduct?
Fraud?
YOU DECIDE!
The aim of this systematic review was to determine the efficacy of conventional treatments plus acupuncture versus conventional treatments alone for asthma, using a meta-analysis of all published randomized clinical trials (RCTs).
The researchers included all RCTs in which adult and adolescent patients with asthma (age ≥12 years) were divided into conventional treatments plus acupuncture (A+B) and conventional treatments (B). Nine studies were included. The results showed that A+B could improve the symptom response rate and significantly decrease interleukin-6. However, indices of pulmonary function, including the forced expiratory volume in one second (FEV1) and FEV1/forced vital capacity (FVC) failed to be improved with A+B.
The authors concluded that conventional treatments plus acupuncture are associated with significant benefits for adult and adolescent patients with asthma. Therefore, we suggest the use of conventional treatments plus acupuncture for asthma patients.
I am thankful to the authors for confirming my finding that A+B must always be more/better than B alone (the 2nd sentence of their conclusion is, of course, utter nonsense, but I will leave this aside for today). Here is the short abstract of my 2008 article:
In this article, we test the hypothesis that randomized clinical trials of acupuncture for pain with certain design features (A + B versus B) are likely to generate false positive results. Based on electronic searches in six databases, 13 studies were found that met our inclusion criteria. They all suggested that acupuncture is effective (one only showing a positive trend, all others had significant results). We conclude that the ‘A + B versus B’ design is prone to false positive results and discuss the design features that might prevent or exacerbate this problem.
Even though our paper was on acupuncture for pain, it firmly established the principle that A+B is always more than B. Think of it in monetary terms: let’s say we both have $100; now someone gives me $10 more. Who has more cash? Not difficult, is it?
But why do SCAM-fans not get it?
Why do we see trial after trial and review after review ignoring this simple and obvious fact?
I suspect I know why: it is because the ‘A+B vs B’ study-design never generates a negative result!
But that’s cheating!
And isn’t cheating unethical?
My answer is YES!
(If you want to read a more detailed answer, please read our in-depth analysis here)
The present trial evaluated the efficacy of homeopathic medicines of Melissa officinalis (MO), Phytolacca decandra (PD), and the combination of both in the treatment of possible sleep bruxism (SB) in children (grinding teeth during sleep).
Patients (n = 52) (6.62 ± 1.79 years old) were selected based on the parents report of SB. The study comprised a crossover design that included 4 phases of 30-day treatments (Placebo; MO 12c; PD 12c; and MO 12c + PD 12c), with a wash-out period of 15 days between treatments.
At baseline and after each phase, the Visual Analogic Scale (VAS) was used as the primary outcome measure to evaluate the influence of treatments on the reduction of SB. The following additional outcome measures were used: a children’s sleep diary with parent’s/guardian’s perceptions of their children’s sleep quality, the trait of anxiety scale (TAS) to identify changes in children’s anxiety profile, and side effects reports. Data were analyzed by ANOVA with repeated measures followed by Post Hoc LSD test.
Significant reduction of SB was observed in VAS after the use of Placebo (-1.72 ± 0.29), MO (-2.36 ± 0.36), PD (-1.44 ± 0.28) and MO + PD (-2.21 ± 0.30) compared to baseline (4.91 ± 1.87). MO showed better results compared to PD (p = 0.018) and Placebo (p = 0.050), and similar result compared to MO+PD (p = 0.724). The sleep diary results and TAS results were not influenced by any of the treatments. No side effects were observed after treatments.
The authors concluded that MO showed promising results in the treatment of possible sleep bruxism in children, while the association of PD did not improve MO results.
Even if one fully subscribed to the principles of homeopathy, this trial raises several questions:
- Why was it submitted and then published in the journal ‘Phytotherapy’. All the remedies were given as C12 potencies. This has nothing to do with phytomedicine.
- Why was a cross-over design chosen? According to homeopathic theory, a homeopathic treatment has fundamental, long-term effects which last much longer than the wash-out periods between treatment phases. This effectively rules out such a design as a means of testing homeopathy.
- MO is used in phytomedicine to induce sleep and reduce anxiety. According to the homeopathic ‘like cures like’ assumption, this would mean it ought to be used homeopathically to treat sleepiness or for keeping patients awake or for making them anxious. How can it be used for sleep bruxism?
Considering all this, I ask myself: should we trust this study and its findings?
What do you think?
Dengue is a viral infection spread by mosquitoes; it is common in many parts of the world. The symptoms include fever, headache, muscle/joint pain and a red rash. The infection is usually mild and lasts about a week. In rare cases it can be more serious and even life threatening. There’s no specific treatment – except for homeopathy; at least this is what many homeopaths want us to believe.
This article reports the clinical outcomes of integrative homeopathic care in a hospital setting during a severe outbreak of dengue in New Delhi, India, during the period September to December 2015.
Based on preference, 138 patients received a homeopathic medicine along with usual care (H+UC), and 145 patients received usual care (UC) alone. Assessment of thrombocytopenia (platelet count < 100,000/mm3) was the main outcome measure. Kaplan-Meier analysis enabled comparison of the time taken to reach a platelet count of 100,000/mm3.
The results show a statistically significantly greater rise in platelet count on day 1 of follow-up in the H+UC group compared with UC alone. This trend persisted until day 5. The time taken to reach a platelet count of 100,000/mm3 was nearly 2 days earlier in the H+UC group compared with UC alone.
The authors concluded that these results suggest a positive role of adjuvant homeopathy in thrombocytopenia due to dengue. Randomized controlled trials may be conducted to obtain more insight into the comparative effectiveness of this integrative approach.
The design of the study is not able to control for placebo effects. Therefore, the question raised by this study is the following: can an objective parameter like the platelet count be influenced by placebo? The answer is clearly YES.
Why do researchers go to the trouble of conducting such a trial, while omitting both randomisation as well as placebo control? Without such design features the study lacks rigour and its results become meaningless? Why can researchers of Dengue fever run a trial without reporting symptomatic improvements? Could the answer to these questions perhaps be found in the fact that the authors are affiliated to the ‘Central Council for Research in Homoeopathy, New Delhi?
One could argue that this trial – yet another one published in the journal ‘Homeopathy’ – is a waste of resources and patients’ co-operation. Therefore, one might even argue, such a study might be seen as unethical. In any case, I would argue that this study is irrelevant nonsense that should have never seen the light of day.
Power Point therapy (PPT) is not what you might think it is; it is not related to a presentation using power point. Power According to the authors of the so far only study of PPT, it is based on the theories of classic acupuncture, neuromuscular reflexology, and systems theoretical approaches like biocybernetics. It has been developed after four decades of experience by Mr. Gerhard Egger, an Austrian therapist. Hundreds of massage and physiotherapists in Europe were trained to use it, and apply it currently in their practice. The treatment can be easily learned. It is taught by professional PPT therapists to students and patients for self-application in weekend courses, followed by advanced courses for specialists.
The core hypothesis of the PPT system is that various pain syndromes have its origin, among others, in a functional pelvic obliquity. This in turn leads to a static imbalance in the posture of the body. This may result in mechanical strain and possible spinal nerve irritation that may radiate and thus affect dermatomes, myotomes, enterotomes, sclerotomes, and neurotomes of one or more vertebra segments. Therefore, treating reflex zones for the pelvis would reduce and possibly resolve the functional obliquity, improve the statics, and thus cure the pain through improved function. In addition, reflex therapy might be beneficial also in patients with unknown causes of back pain. PPT uses blunt needle tips to apply pressure to specific reflex points on the nose, hand, and feet. PPT has been used for more than 10 years in treating patients with musculoskeletal problems, especially lower back pain.
Sounds more than a little weird?
Yes, I agree.
Perhaps we need some real evidence.
The aim of this RCT was to compare 10 units of PPT of 10 min each, with 10 units of standard physiotherapy of 30 min each. Outcomes were functional scores (Roland Morris Disability, Oswestry, McGill Pain Questionnaire, Linton-Halldén – primary outcome) and health-related quality of life (SF-36), as well as blinded assessments by clinicians (secondary outcome).
Eighty patients consented and were randomized, 41 to PPT, 39 to physiotherapy. Measurements were taken at baseline, after the first and after the last treatment (approximately 5 weeks after enrolment). Multivariate linear models of covariance showed significant effects of time and group and for the quality of life variables also a significant interaction of time by group. Clinician-documented variables showed significant differences at follow-up.
The authors concluded that both physiotherapy and PPT improve subacute low back pain significantly. PPT is likely more effective and should be studied further.
I was tempted to say ‘there is nothing fundamentally wrong with this study’. But then I hesitated and, on second thought, found a few things that do concern me:
- The theory on which PPT is based is not plausible (to put it mildly).
- It would have been easy to conduct a placebo-controlled trial of PPT. The authors justify their odd study design stating this: This was the very first randomized controlled trial of PPT. Therefore, the study has to be considered a pilot. For a pivotal study, a clearly defined primary outcome would have been essential. This was not possible, as no previous experience was able to suggest which outcome would be the best. In my view, this is utter nonsense. Defining the primary outcome of a back pain study is not rocket science; there are plenty of validated measures of pain.
- The study was funded by the Foundation of Natural Sciences and Technical Research in Vaduz, Liechtenstein. I cannot find such an organisation on the Internet.
- The senior author of this study is Prof H Walach who won the prestigious award for pseudoscientist of the year 2012.
- Walach provides no less than three affiliations, including the ‘Change Health Science Institute, Berlin, Germany’. I cannot find such an organisation on the Internet.
- The trial was published in a less than prestigious SCAM journal, ‘Forschende Komplementarmedizin‘ – its editor in-chief: Harald Walach.
So, in view of these concerns, I think PPT might not be nearly as promising as this study implies. Personally, I will wait for an independent replication of Walach’s findings.
An impressive 17% of US chiropractic patients are 17 years of age or younger. This figure increases to 39% among US chiropractors who have specialized in paediatrics. Data for other countries can be assumed to be similar. But is chiropractic effective for children? All previous reviews concluded that there is a paucity of evidence for the effectiveness of manual therapy for conditions within paediatric populations.
This systematic review is an attempt to shed more light on the issue by evaluating the use of manual therapy for clinical conditions in the paediatric population, assessing the methodological quality of the studies found, and synthesizing findings based on health condition.
Of the 3563 articles identified through various literature searches, 165 full articles were screened, and 50 studies (32 RCTs and 18 observational studies) met the inclusion criteria. Only 18 studies were judged to be of high quality. Conditions evaluated were:
- attention deficit hyperactivity disorder (ADHD),
- autism,
- asthma,
- cerebral palsy,
- clubfoot,
- constipation,
- cranial asymmetry,
- cuboid syndrome,
- headache,
- infantile colic,
- low back pain,
- obstructive apnoea,
- otitis media,
- paediatric dysfunctional voiding,
- paediatric nocturnal enuresis,
- postural asymmetry,
- preterm infants,
- pulled elbow,
- suboptimal infant breastfeeding,
- scoliosis,
- suboptimal infant breastfeeding,
- temporomandibular dysfunction,
- torticollis,
- upper cervical dysfunction.
Musculoskeletal conditions, including low back pain and headache, were evaluated in seven studies. Only 20 studies reported adverse events.
The authors concluded that fifty studies investigated the clinical effects of manual therapies for a wide variety of pediatric conditions. Moderate-positive overall assessment was found for 3 conditions: low back pain, pulled elbow, and premature infants. Inconclusive unfavorable outcomes were found for 2 conditions: scoliosis (OMT) and torticollis (MT). All other condition’s overall assessments were either inconclusive favorable or unclear. Adverse events were uncommonly reported. More robust clinical trials in this area of healthcare are needed.
There are many things that I find remarkable about this review:
- The list of indications for which studies have been published confirms the notion that manual therapists – especially chiropractors – regard their approach as a panacea.
- A systematic review evaluating the effectiveness of a therapy that includes observational studies without a control group is, in my view, highly suspect.
- Many of the RCTs included in the review are meaningless; for instance, if a trial compares the effectiveness of two different manual therapies none of which has been shown to work, it cannot generate a meaningful result.
- Again, we find that the majority of trialists fail to report adverse effects. This is unethical to a degree that I lose faith in such studies altogether.
- Only three conditions are, according to the authors, based on evidence. This is hardly enough to sustain an entire speciality of paediatric chiropractors.
Allow me to have a closer look at these three conditions.
- Low back pain: the verdict ‘moderate positive’ is based on two RCTs and two observational studies. The latter are irrelevant for evaluating the effectiveness of a therapy. One of the two RCTs should have been excluded because the age of the patients exceeded the age range named by the authors as an inclusion criterion. This leaves us with one single ‘medium quality’ RCT that included a mere 35 patients. In my view, it would be foolish to base a positive verdict on such evidence.
- Pulled elbow: here the verdict is based on one RCT that compared two different approaches of unknown value. In my view, it would be foolish to base a positive verdict on such evidence.
- Preterm: Here we have 4 RCTs; one was a mere pilot study of craniosacral therapy following the infamous A+B vs B design. The other three RCTs were all from the same Italian research group; their findings have never been independently replicated. In my view, it would be foolish to base a positive verdict on such evidence.
So, what can be concluded from this?
I would say that there is no good evidence for chiropractic, osteopathic or other manual treatments for children suffering from any condition.
And why do the authors of this new review arrive at such dramatically different conclusion? I am not sure. Could it perhaps have something to do with their affiliations?
- Palmer College of Chiropractic,
- Canadian Memorial Chiropractic College,
- Performance Chiropractic.
What do you think?
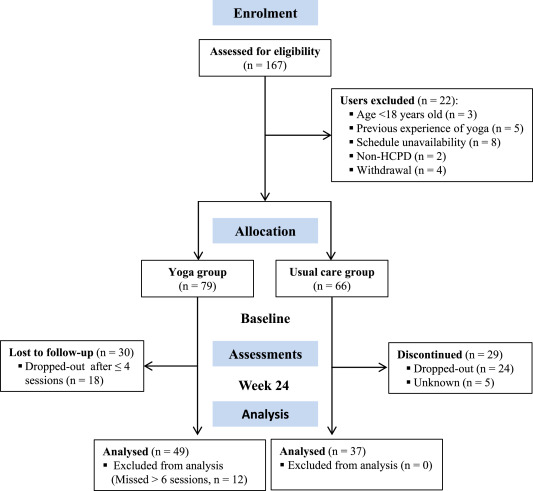
A recent blog-post pointed out that the usefulness of yoga in primary care is doubtful. Now we have new data to shed some light on this issue.
The new paper reports a ‘prospective, longitudinal, quasi-experimental study‘. Yoga group (n= 49) underwent 24-weeks program of one-hour yoga sessions. The control group had no yoga.
Participation was voluntary and the enrolment strategy was based on invitations by health professionals and advertising in the community (e.g., local newspaper, health unit website and posters). Users willing to participate were invited to complete a registration form to verify eligibility criteria.
The endpoints of the study were:
- quality of life,
- psychological distress,
- satisfaction level,
- adherence rate.
The yoga routine consisted of breathing exercises, progressive articular and myofascial warming-up, followed by surya namascar (sun salutation sequence; adapted to the physical condition of each participant), alignment exercises, and postural awareness. Practice also included soft twists of the spine, reversed and balance postures, as well as concentration exercises. During the sessions, the instructor discussed some ethical guidelines of yoga, as for example, non-violence (ahimsa) and truthfulness (satya), to allow the participant to have a safer and integrated practice. In addition, the participants were encouraged to develop their awareness of the present moment and their body sensations, through a continuous process of self-consciousness, keeping a distance between body sensations and the emotional experience. The instructor emphasized the connection between breathing and movement. Each session ended with a guided deep relaxation (yoga nidra; 5–10 min), followed by a meditation practice (5–10 min).
The results of the study showed that the patients in the yoga group experienced a significant improvement in all domains of quality of life and a reduction of psychological distress. Linear regression analysis showed that yoga significantly improved psychological quality of life.
The authors concluded that yoga in primary care is feasible, safe and has a satisfactory adherence, as well as a positive effect on psychological quality of life of participants.
Are the authors’ conclusions correct?
I think not!
Here are some reasons for my judgement:
- The study was far to small to justify far-reaching conclusions about the safety and effectiveness of yoga.
- There were relatively high numbers of drop-outs, as seen in the graph above. Despite this fact, no intention to treat analysis was used.
- There was no randomisation, and therefore the two groups were probably not comparable.
- Participants of the experimental group chose to have yoga; their expectations thus influenced the outcomes.
- There was no attempt to control for placebo effects.
- The conclusion that yoga is safe would require a sample size that is several dimensions larger than 49.
In conclusion, this study fails to show that yoga has any value in primary care.
PS
Oh, I almost forgot: and yoga is also satanic, of course (just like reading Harry Potter!).
Excellent journals always publish excellent science!
If this is what you believe, you might want to read a study of chiropractic just published in the highly respected SCIENTIFIC REPORTS.
The objective of this study was to investigate whether a single session of chiropractic care could increase strength in weak plantar flexor muscles in chronic stroke patients. Maximum voluntary contractions (strength) of the plantar flexors, soleus evoked V-waves (cortical drive), and H-reflexes were recorded in 12 chronic stroke patients, with plantar flexor muscle weakness, using a randomized controlled crossover design. Outcomes were assessed pre and post a chiropractic care intervention and a passive movement control. Repeated measures ANOVA was used to asses within and between group differences. Significance was set at p < 0.05. Following the chiropractic care intervention there was a significant increase in strength (F (1,11) = 14.49, p = 0.002; avg 64.2 ± 77.7%) and V-wave/Mmax ratio (F(1,11) = 9.67, p = 0.009; avg 54.0 ± 65.2%) compared to the control intervention. There was a significant strength decrease of 26.4 ± 15.5% (p = 0.001) after the control intervention. There were no other significant differences. Plantar flexor muscle strength increased in chronic stroke patients after a single session of chiropractic care. An increase in V-wave amplitude combined with no significant changes in H-reflex parameters suggests this increased strength is likely modulated at a supraspinal level. Further research is required to investigate the longer term and potential functional effects of chiropractic care in stroke recovery.
In the article we find the following further statements (quotes in bold, followed by my comments in normal print):
- Data were collected by a team of researchers from the Centre for Chiropractic Research at the New Zealand College of Chiropractic. These researchers can be assumed to be highly motivated in generating a positive finding.
- The entire spine and both sacroiliac joints were assessed for vertebral subluxations, and chiropractic adjustments were given where deemed necessary, by a New Zealand registered chiropractor. As there is now near-general agreement that such subluxations are a myth, the researchers treated a non-existing entity.
- The chiropractor did not contact on a segment deemed to be subluxated during the control set-up and no adjustive thrusts were applied during any control intervention. The patients therefore were clearly able to tell the difference between real and control treatments. Participants were not checked for blinding success.
- Maximum isometric plantarflexion force was measured using an isometric strain gauge. Such measurements crucially depend on the motivation of the patient.
- The grant proposal for this study was reviewed by the Australian Spinal Research Foundation to support facilitation of funding from the United Chiropractic Association. Does this not mean the researchers had a conflict of interest?
- The authors declare no competing interests. Really? They were ardent subluxationists supported by the United Chiropractic Association, an organisation stating that chiropractic is concerned with the preservation and restoration of health, and focuses particular attention on the subluxation, and subscribes to to the obsolete concept of vitalism: we ascribe to the idea that all living organisms are sustained by an innate intelligence, which is both different from and greater than physical and chemical forces. Further, we believe innate intelligence is an expression of universal intelligence.
So, in essence, what we have here is an under-powered study sponsored by vitalists and conducted by subluxationists treating a mythical entity with dubious interventions without controlling for patients’ expectation pretending their false-positive findings are meaningful.
I cannot help wondering what possessed the SCIENTIFIC REPORTS to publish such poor science.