spinal manipulation
This is a fascinating new review of upper neck manipulation. It raises many concerns that we, on this blog, have been struggling with for years. I take the liberty of quoting a few passages which I feel are important and encourage everyone to study the report in full:
The Minister of Health, Seniors and Active Living gave direction to the Health Professions Advisory Council (“the Council”) to undertake a review related to high neck manipulation.
Specifically, the Minister directed the Council to undertake:
1) A review of the status of the reserved act in other Canadian jurisdictions,
2) A literature review related to the benefits to patients and risks to patient safety associated with the procedure, and
3) A jurisprudence review or a review into the legal issues that have arisen in Canada with respect to the performance of the procedure that touch upon the risk of harm to a patient.
In addition, the Minister requested the Council to seek written input on the issue from:
- Manitoba Chiropractic Stroke Survivors
- Manitoba Chiropractic Association
- College of Physiotherapists of Manitoba
- Manitoba Naturopathic Association
- College of Physicians and Surgeons of Manitoba
- other relevant interested parties as determined by the Council
… The review indicated that further research is required to:
- strengthen evidence for the efficacy of cervical spinal manipulations (CSM) as a treatment for neck pain and headache, “as well as for other indications where evidence currently does not exist (i.e., upper back and should/arm pain, high blood pressure, etc.)”
- establish safety and efficacy of CSM in infants and children
- assess the risk versus benefit in consideration of using HVLA cervical spine manipulation, which also involve cost-benefit analyses that compare CSM to other standard treatments.
… the performance of “high neck manipulation” or cervical spine manipulation does present a risk of harm to patients. This risk of harm must be understood by both the patient and the practitioner.
Both the jurisprudence review and the research literature review point to the need for the following actions to mitigate the risk of harm associated with the performance of cervical spine manipulation:
- Action One: Ensure that the patient provides written informed consent prior to initiating treatment which includes a discussion about the risk associated with cervical spine manipulation.
- Action Two: Provide patients with information to assist in the early recognition of a serious adverse event.
This is too wonderful (I found it on Twitter where it was posted by ‘Doctors Leonard and Michael Valentine’, chiropractors at Valentine Chiropractic in Fountain Valley, CA.) – I have to show it to you.

This could almost pass without a comment. But for what it’s worth, here are my 7 points:
- platitude,
- platitude,
- no, they do not easily move out of alignment, and if they do, you are severely ill and need urgent treatment but not chiropractic,
- subluxations as dreamt up by chiropractors are a myth; they simply do not exist,
- it is vital that we don’t disclose this BS, if not chiros need to find new jobs,
- chiros pretend to find subluxations because this is their livelihood,
- pathetic platitude.

During Voltaire’s time, this famous quote was largely correct. But today, things are very different, and I often think this ‘bon mot’ ought to be re-phrased into ‘The art of alternative medicine consists in amusing the patient, while medics cure the disease’.
To illustrate this point, I shall schematically outline the story of a patient seeking care from a range of clinicians. The story is invented but nevertheless based on many real experiences of a similar nature.
Tom is in his mid 50s, happily married, mildly over-weight and under plenty of stress. In addition to holding a demanding job, he has recently moved home and, as a consequence of lots of heavy lifting, his whole body aches. He had previous episodes of back trouble and re-starts the exercises a physio once taught him. A few days later, the back-pain has improved and most other pains have subsided as well. Yet a dull and nagging pain around his left shoulder and arm persists.
He is tempted to see his GP, but his wife is fiercely alternative. She was also the one who dissuaded Tom from taking Statins for his high cholesterol and put him on Garlic pills instead. Now she gives Tom a bottle of her Rescue Remedy, but after a week of taking it Tom’s condition is unchanged. His wife therefore persuades him to consult alternative practitioners for his ‘shoulder problem’. Thus he sees a succession of her favourite clinicians.
THE CHIROPRACTOR examines Tom’s spine and diagnoses subluxations to be the root cause of his problem. Tom thus receives a series of spinal manipulations and feels a little improved each time. But he is disappointed that the pain in the left shoulder and arm returns. His wife therefore makes another appointment for him.
THE ENERGY HEALER diagnoses a problem with Tom’s vital energy as the root cause of his persistent pain. Tom thus receives a series of healing sessions and feels a little improved each time. But he is disappointed that the pain in the left shoulder and arm returns. His wife therefore makes another appointment for him.
THE REFLEXOLOGIST examines Tom’s foot and diagnoses knots on the sole of his foot to cause energy blockages which are the root cause of his problem. Tom thus receives a series of most agreeable foot massages and feels a little improved each time. But he is disappointed that the pain in the left shoulder and arm returns. His wife therefore makes another appointment for him.
THE ACUPUNCTURIST examines Tom’s pulse and tongue and diagnoses a chi deficiency to be the root cause of his problem. Tom thus receives a series of acupuncture treatments and feels a little improved each time. But he is disappointed that the pain in the left shoulder and arm returns. His wife therefore makes another appointment for him.
THE NATUROPATH examines Tom and diagnoses some form of auto-intoxication as the root cause of his problem. Tom thus receives a full program of detox and feels a little improved each time. But he is disappointed that the pain in the left shoulder and arm returns. His wife therefore makes another appointment for him.
THE HOMEOPATH takes a long and detailed history and diagnoses a problem with Tom’s vital force to be the root cause of his pain. Tom thus receives a homeopathic remedy tailor-made for his needs and feels a little improved after taking it for a few days. But he is disappointed that the pain in the left shoulder and arm returns. His wife therefore tries to make another appointment for him.
But this time, Tom had enough. His pain has not really improved and he is increasingly feeling unwell.
 At the risk of a marital dispute, he consults his GP. The doctor looks up Tom’s history, asks a few questions, conducts a brief physical examination, and arranges for Tom to see a specialist. A cardiologist diagnoses Tom to suffer from coronary heart disease due to a stenosis in one of his coronary arteries. She explains that Tom’s dull pain in the left shoulder and arm is a rather typical symptom of this condition.
At the risk of a marital dispute, he consults his GP. The doctor looks up Tom’s history, asks a few questions, conducts a brief physical examination, and arranges for Tom to see a specialist. A cardiologist diagnoses Tom to suffer from coronary heart disease due to a stenosis in one of his coronary arteries. She explains that Tom’s dull pain in the left shoulder and arm is a rather typical symptom of this condition.
Tom has to have a stent put into the affected coronary artery, receives several medications to lower his cholesterol and blood pressure, and is told to take up regular exercise, lose weight and make several other changes to his stressful life-style. Tom’s wife is told in no uncertain terms to stop dissuading her husband from taking his prescribed medicines, and the couple are both sent to see a dietician who offers advice and recommends a course on healthy cooking. Nobody leaves any doubt that not following this complex (holistic!) package of treatments and advice would be a serious risk to Tom’s life.
It has taken a while, but finally Tom is pain-free. More importantly, his prognosis has dramatically improved. The team who now look after him have no doubt that a major heart attack had been imminent, and Tom could easily have died had he continued to listen to the advice of multiple non-medically trained clinicians.
The root cause of his condition was misdiagnosed by all of them. In fact, the root cause was the atherosclerotic degeneration in his arteries. This may not be fully reversible, but even if the atherosclerotic process cannot be halted completely, it can be significantly slowed down such that he can live a full life.
My advice based on this invented and many real stories of a very similar nature is this:
- alternative practitioners are often good at pampering their patients;
- this may contribute to some perceived clinical improvements;
- in turn, this perceived benefit can motivate patients to continue their treatment despite residual symptoms;
- alternative practitioner’s claims about ‘root causes’ and holistic care are usually pure nonsense;
- their pampering may be agreeable, but it can undoubtedly cost lives.
The British press recently reported that a retired bank manager (John Lawler, aged 80) died after visiting a chiropractor in York. This tragic case was published in multiple articles, most recently in THE SUN. Personally, I find this regrettable – not the fact that the press warns consumers of chiropractic, but the tone and content of the articles.
Let me explain this by citing the one in THE SUN of today. Here is the critical bit that concerns me:
Ezvard Ernst, Emeritus Professor of Complementary Medicine at Exeter University, published a study showing at least 26 people had died as a result. He said: “The evidence is not in favour of chiropractic treatments. Nobody knows how many have suffered severe complications or died.” Edvard Ernst, Professor of Complementary Medicine, says many have suffered complications or died from chiropractors treatments… A study from Exeter University shows at least 26 people have died as a result of treatment.
And what is wrong with this?
The answer is lots:
- My first name is consistently misspelled (a triviality, I agree).
- I am once named as Emeritus Professor and once as Professor of Complementary Medicine. The latter is wrong (another triviality, perhaps, but some of my more demented critics have regularly accused me of carrying wrong titles)
- The mention of 26 deaths after chiropractic treatments is problematic and arguably misleading (see below).
- Our ‘study’ was not a study but a systematic review (another triviality?).
Now you probably think I am being pedantic, but I feel that the article is regrettable not so much by what it says but by what it fails to say. To understand this better, I will below copy my emails to the journalist who asked for help in researching this article.
- My email of 17/10 answering all 7 of the journalist’s specific questions:
- 1. Why are you sceptical of chiropractic?
- I have researched the subject for more than 2 decades, and I know that the evidence is not in favour of chiropractic
- 2. How many people do you believe have died in Britain as a result of being treated by a chiropractor? If it’s not possible to say, can you estimate?
- nobody knows how many patients have suffered severe complications or deaths. there is no system to monitor such events that is comparable to the post-marketing surveillance of conventional medicine. we did some research and found that the under-reporting of cases of severe complications was close to 100% in the UK.
- 3. What is so dangerous about chiropractic? Is there a particular physical treatment than endangers life?
- manipulations that involve rotation and over-extension of the upper spine can lead to a vertebral artery breaking up. this causes a stroke which sometimes is fatal.
- 4. Is the industry well regulated?
- UK chiropractors are regulated by the General Chiropractic Council. it is debatable whether they are fit for purpose (see here:http://edzardernst.com/2015/02/the-uk-general-chiropractic-council-fit-for-purpose/)
- 5. Should we be suspicious of claims that chiropractic can cure things like IBS and autism?
- such claims are not based on good evidence and therefore misleading and unethical. sadly, however, they are prevalent.
- 6. Who trains chiropractors?
- there are numerous colleges that specialise in that activity.
- 7. Is it true Prince Charles is to blame for the rise in popularity/prominence of chiropractic?
- I am not sure. certainly he has been promoting all sorts of unproven treatments for decades.
- My email of 18/10 answering 3 further specific questions
- 1. Would you actively discourage anyone from being treated by a chiropractor?
yes, anyone I feel responsible for
2. Are older people particularly at risk or could one wrong move affect anyone?
older people are at higher risk of bone fractures and might also have more brittle arteries prone to dissection
3. If someone has, say, a bad back or stiff neck what treatment would you recommend instead of chiropractic?
I realise every case is different, but you are sceptical of all complementary treatments (as I understand it) so what would you suggest instead?
I would normally consider therapeutic exercises and recommend seeing a good physio. - 3. My email of 23/10 replying to his request for specific UK cases
- the only thing I can offer is this 2001 paper
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1297923/
- where we discovered 35 cases seen by UK neurologists within the preceding year. the truly amazing finding here was that NONE of them had been reported anywhere before. this means under-reporting was exactly 100%.
END OF QUOTES
I think that makes it quite obvious that much relevant information never made it into the final article. I also know that several other experts provided even more information than I did which never appeared.
The most important issues, I think, are firstly the lack of a monitoring system for adverse events, secondly the level of under-reporting and thirdly the 50% rate of mild to moderate adverse-effects. Without making these issues amply clear, lay readers cannot possibly make any sense of the 26 deaths. More importantly, chiropractors will now be able to respond by claiming: 26 deaths compare very favourably with the millions of fatalities caused by conventional medicine. In the end, the message that will remain in the heads of many consumers is this: CONVENTIONAL MEDICINE IS MUCH MORE DANGEROUS THAN CHIROPRACTIC!!! (The 1st comment making this erroneous point has already been published: Don’t be stupid Andy. You wanna discuss how many deaths occur due to medication side effects and drug interactions? There is a reason chiros have the lowest malpractice rates.)
Don’t get me wrong, I am not accusing the author of the SUN-article. For all I know, he has filed a very thoughtful and complete piece. It might have been shortened by the editor who may also have been the one adding the picture of the US starlet with her silicone boobs. But I am accusing THE SUN of missing a chance to publish something that might have had the chance of being a meaningful contribution to public health.
Perhaps you still think this is all quite trivial. Yet, after having experienced this sort of thing dozens, if not hundreds of times, I disagree.
This is the question asked by the American Chiropractic Association. And this is their answer [the numbers in square brackets were inserted by me and refer to my comments below]:
Chiropractic is widely recognized [1] as one of the safest drug-free, non-invasive therapies available for the treatment of neuromusculoskeletal complaints [2]. Although chiropractic has an excellent safety record [3], no health treatment is completely free of potential adverse effects. The risks associated with chiropractic, however, are very small [4]. Many patients feel immediate relief following chiropractic treatment [5], but some may experience mild soreness, stiffness or aching, just as they do after some forms of exercise [6]. Current research shows that minor discomfort or soreness following spinal manipulation typically fades within 24 hours [7]…
Some reports have associated high-velocity upper neck manipulation with a certain rare kind of stroke, or vertebral artery dissection [8]. However, evidence suggests that this type of arterial injury often takes place spontaneously in patients who have pre-existing arterial disease [9]. These dissections have been associated with everyday activities such as turning the head while driving, swimming, or having a shampoo in a hair salon [10]. Patients with this condition may experience neck pain and headache that leads them to seek professional care—often at the office of a doctor of chiropractic or family physician—but that care is not the cause of the injury. The best evidence indicates that the incidence of artery injuries associated with high-velocity upper neck manipulation is extremely rare—about one to three cases in 100,000 patients who get treated with a course of care [11]. This is similar to the incidence of this type of stroke among the general population [12]…
When discussing the risks of any health care procedure, it is important to look at that risk in comparison to other treatments available for the same condition [13]. In this regard, the risks of serious complications from spinal manipulation for conditions such as neck pain and headache compare very favorably with even the most conservative care options. For example, the risks associated with some of the most common treatments for musculoskeletal pain—over-the-counter or prescription nonsteroidal anti-inflammatory drugs (NSAIDS) and prescription painkillers—are significantly greater than those of chiropractic manipulation [14]…
Doctors of chiropractic are well trained professionals who provide patients with safe, effective care for a variety of common conditions. Their extensive education has prepared them to identify patients who have special risk factors [15] and to get those patients the most appropriate care, even if that requires referral to a medical specialist [16].
END OF QUOTE
- Appeal to tradition = fallacy
- …and every other condition that brings in cash.
- Not true.
- Probably not true.
- The plural of anecdote is anecdotes, not evidence.
- Not true, the adverse effects of spinal manipulation are different and more severe.
- Not true, they last 1-3 days.
- Not just ‘some reports’ but a few hundred.
- Which does not mean that spinal manipulation cannot provoke such events.
- True, but this does not mean that spinal manipulation cannot provoke such events.
- There are other estimates that gives much higher figures; without a proper monitoring system, nobody can provide an accurate incidence figure.
- Not true, see above.
- ‘Available’ is meaningless – ‘effective’ is what we need here.
- The difference between different treatments is not merely their safety but also their effectiveness; in the end it is the risk/benefit balance that determines their value.
- Not true, there are no good predictors to identify at-risk populations.
- Chiropractors are notoriously bad at referring to other healthcare professionals; they have a huge conflict of interest in keeping up their cash-flow.
So, is chiropractic a safe treatment?
My advice here is not to ask chiropractors but independent experts.
I recently came across this article; essentially it claims that, in 1918, chiropractic proved itself to be the method of choice for treating the flu!
Unbelievable?
Here is a short quote from it:
Chiropractors got fantastic results from influenza patients while those under medical care died like flies all around. Statistics reflect a most amazing, almost miraculous state of affairs. The medical profession was practically helpless with the flu victims but chiropractors seemed able to do no wrong.”
“In Davenport, Iowa, 50 medical doctors treated 4,953 cases, with 274 deaths. In the same city, 150 chiropractors including students and faculty of the Palmer School of Chiropractic, treated 1,635 cases with only one death.”
“In the state of Iowa, medical doctors treated 93,590 patients, with 6,116 deaths – a loss of one patient out of every 15. In the same state, excluding Davenport, 4,735 patients were treated by chiropractors with a loss of only 6 cases – a loss of one patient out of every 789.
“National figures show that 1,142 chiropractors treated 46,394 patients for influenza during 1918, with a loss of 54 patients – one out of every 886.”
“Reports show that in New York City, during the influenza epidemic of 1918, out of every 10,000 cases medically treated, 950 died; and in every 10,000 pneumonia cases medically treated 6,400 died. These figures are exact, for in that city these are reportable diseases.”
“In the same epidemic, under drugless methods, only 25 patients died of influenza out of every 10,000 cases; and only 100 patients died of pneumonia out of every 10,000 cases…”
“In the same epidemic reports show that chiropractors in Oklahoma treated 3,490 cases of influenza with only 7 deaths. But the best part of this is, in Oklahoma there is a clear record showing that chiropractors were called in 233 cases where medical doctors had cared for the patients, and finally gave them up as lost. The chiropractors saved all these lost cases but 25.”
END OF QUOTE
So what does that sort of ‘evidence’ really show?
Does it prove that chiropractic is effective against influenza?
No!
Does it even suggest that chiropractic is effective against influenza?
No!
What then?
I think it shows that some chiropractors (like many homeopaths) are deluded to a point where they are unable to differentiate pseudoscience from science, anecdote from evidence, cause from effect, etc.
In the case you need more explanations, let me re-phrase this section from a previous post:
In the typical epidemiological case/control study, one large group of patients [A] is retrospectively compared to another group [B]. By large, I mean with a sample size of thousands of patients. In our case, group A has been treated by chiropractors, while group B received the treatments available at the time. It is true that several of such reports seemed to suggest that chiropractic works. But this does by no means prove anything; the result might have been due to a range of circumstances, for instance:
- group A might have been less ill than group B,
- group A might have been richer and therefore better nourished,
- group A might have benefitted from better hygiene,
- group A might have received better care, e. g. hydration,
- group B might have received treatments that made the situation not better but worse.
Because these are RETROSPECTIVE studies, there is no way to account for these and many other factors that might have influenced the outcome. This means that epidemiological studies of this nature can generate interesting results which, in turn, need testing in properly controlled studies where these confounding factors are adequately controlled for. Without such tests, they are next to worthless.
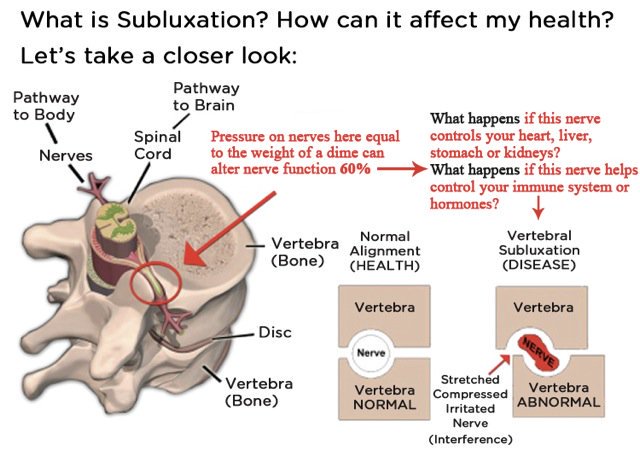
How often have we heard that chiropractic has moved on and has given up the concept of subluxation/malalignment? For sure there is no evidence for such nonsense, and it would be high time to give it up! But, as has been argued here and elsewhere, if chiros give it up, what is there left? What then would differentiate them from physios ? The answer is not a lot.
In any case, chiros have by no means given up subluxation. One can argue this point ad nauseam; yet, most chiros remain in denial.
For this post, I have chosen a different approach to make my point. I simply went on twitter and had a look what messages chiros tweet. The impression I got is that the majority of chiros are totally immersed in subluxation. To provide some proof, I have copied a few images – if chiros do not listen to words, perhaps they understand pictures, I thought.
So, here we go – enjoy!
[please click to see them full size]



On this blog, we have often discussed the risks of spinal manipulation. As I see it, the information we have at present suggests that
- mild to moderate adverse effects are extremely frequent and occur in about half of all patients;
- serious adverse effects are being reported regularly;
- the occur usually with chiropractic manipulations of the neck (which are not of proven efficacy for any condition) and often relate to vascular accidents;
- the consequences can be permanent neurological deficits and even deaths;
- under-reporting of such cases might be considerable and therefore precise incidence figures are not available;
- there is no system to accurately monitor the risks;
- chiropractors are in denial of these problems.
Considering the seriousness of these issues, it is important to do more rigorous research. Therefore, any new paper published on this subject is welcome. A recent article might shed new light on the topic.
The objective of this systematic review was to identify characteristics of 1) patients, 2) practitioners, 3) treatment process and 4) adverse events (AE) occurring after cervical spinal manipulation (CSM) or cervical mobilization. A systematic searches were performed in 6 electronic databases up to December 2014. Of the initial 1043 articles thus located, 144 were included, containing 227 cases. 117 cases described male patients with a mean age of 45 and a mean age of 39 for females. Most patients were treated by chiropractors (66%). Manipulation was reported in 95% of the cases, and neck pain was the most frequent indication for the treatment. Cervical arterial dissection (CAD) was reported in 57% of the cases and 45.8% had immediate onset symptoms. The overall distribution of gender for CAD was 55% for female. Patient characteristics were described poorly. No clear patient profile, related to the risk of AE after CSM, could be extracted, except that women seemed more at risk for CAD. The authors of this review concluded that there seems to be under-reporting of cases. Further research should focus on a more uniform and complete registration of AE using standardized terminology.
This article provides little new information; but it does confirm what I have been saying since many years: NECK MANIPULATIONS ARE ASSOCIATED WITH SERIOUS RISKS AND SHOULD THEREFORE BE AVOIDED.
Systematic reviews are aimed at summarising and critically evaluating the evidence on a specific research question. They are the highest level of evidence and are more reliable than anything else we have. Therefore, they represent a most useful tool for both clinicians and researchers.
But there are, of course, exceptions. Take, for instance, this recent systematic review by researchers from the
- Texas Chiropractic College, Pasadena, the Palmer Center for Chiropractic Research, Palmer College of Chiropractic, Davenport,
- Department of Planning, Policy and Design, University of California, Irvine,
- VA Puget Sound Health Care System, Tacoma,
- New York Chiropractic College, Seneca Falls,
- Logan University College of Chiropractic, Chesterfield,
- University of Western States, Portland.
How often have I pointed out that most studies of chiropractic (and other alternative therapies) are overtly unethical because they fail to report adverse events? And if you think this is merely my opinion, you are mistaken. This new analysis by a team of chiropractors aimed to describe the extent of adverse events reporting in published RCTs of Spinal Manipulative Therapy (SMT), and to determine whether the quality of reporting has improved since publication of the 2010 Consolidated Standards Of Reporting Trials (CONSORT) statement.
The Physiotherapy Evidence Database and the Cochrane Central Register of Controlled Trials were searched for RCTs involving SMT. Domains of interest included classifications of adverse events, completeness of adverse events reporting, nomenclature used to describe the events, methodological quality of the study, and details of the publishing journal. Data were analysed using descriptive statistics. Frequencies and proportions of trials reporting on each of the specified domains above were calculated. Differences in proportions between pre- and post-CONSORT trials were calculated with 95% confidence intervals using standard methods, and statistical comparisons were analysed using tests for equality of proportions with continuity correction.
Of 7,398 records identified in the electronic searches, 368 articles were eligible for inclusion in this review. Adverse events were reported in 140 (38.0%) articles. There was a significant increase in the reporting of adverse events post-CONSORT (p=.001). There were two major adverse events reported (0.3%). Only 22 articles (15.7%) reported on adverse events in the abstract. There were no differences in reporting of adverse events post-CONSORT for any of the chosen parameters.
The authors concluded that although there has been an increase in reporting adverse events since the introduction of the 2010 CONSORT guidelines, the current level should be seen as inadequate and unacceptable. We recommend that authors adhere to the CONSORT statement when reporting adverse events associated with RCTs that involve SMT.
We conducted a very similar analysis back in 2012. Specifically, we evaluated all 60 RCTs of chiropractic SMT published between 2000 and 2011 and found that 29 of them did not mention adverse effects at all. Sixteen RCTs reported that no adverse effects had occurred (which I find hard to believe since reliable data show that about 50% of patients experience adverse effects after consulting a chiropractor). Complete information on incidence, severity, duration, frequency and method of reporting of adverse effects was included in only one RCT. Conflicts of interests were not mentioned by the majority of authors. Our conclusion was that adverse effects are poorly reported in recent RCTs of chiropractic manipulations.
The new paper suggests that the situation has improved a little, yet it is still wholly unacceptable. To conduct a clinical trial and fail to mention adverse effects is not, as the authors of the new article suggest, against current guidelines; it is a clear and flagrant violation of medical ethics. I blame the authors of such papers, the reviewers and the journal editors for behaving dishonourably and urge them to get their act together.
The effects of such non-reporting are obvious: anyone looking at the evidence (for instance via systematic reviews) will get a false-positive impression of the safety of SMT. Consequently, chiropractors are able to claim that very few adverse effects have been reported in the literature, therefore our hallmark therapy SMT is demonstrably safe. Those who claim otherwise are quite simply alarmist.