risk/benefit
There are of course 2 types of osteopaths: the US osteopaths who are very close to real doctors, and the osteopaths from all other countries who are practitioners of so-called alternative medicine. This post, as all my posts on this subject, is about the latter category.
I was alerted to a paper entitled ‘Osteopathy under scrutiny’. It goes without saying that I thought it relevant; after all, scrutinising so-called altermative medicine (SCAM), such as osteopathy is one of the aims of this blog. The article itself is in German, but it has an English abstract:
Osteopathic medicine is a medical specialty that enjoys a high level of recognition and increasing popularity among patients. High-quality education and training are essential to ensure good and safe patient treatment. At a superficial glance, osteopathy could be misunderstood as a myth; accurately considered, osteopathic medicine is grounded in medical and scientific knowledge and solid theoretical and practical training. Scientific advances increasingly confirm the empirical experience of osteopathy. Although more studies on its efficacy could be conducted, there is sufficient evidence for a reasonable application of osteopathy. Current scientific studies show how a manually executed osteopathic intervention can induce tissue and even cellular reactions. Because the body actively responds to environmental stimuli, osteopathic treatment is considered an active therapy. Osteopathic treatment is individually applied and patients are seen as an integrated entity. Because of its typical systemic view and scientific interpretation, osteopathic medicine is excellently suited for interdisciplinary cooperation. Further work on external evidence of osteopathy is being conducted, but there is enough knowledge from the other pillars of evidence-based medicine (EBM) to support the application of osteopathic treatment. Implementing careful, manual osteopathic examination and treatment has the potential to cut healthcare costs. To ensure quality, osteopathic societies should be intimately involved and integrated in the regulation of the education, training, and practice of osteopathic medicine.
This does not sound as though the authors know what scutiny is. In fact, the abstract reads like a white-wash of quackery. Why might this be so? To answer this question, we need to look no further than to the ‘conflicts of interest’ where the authors state (my translation): K. Dräger and R. Heller state that, in addition to their activities as further education officers/lecturers for osteopathy (Deutsche Ärztegesellschaft für Osteopathie e. V. (DÄGO) and the German Society for Osteopathic Medicine e. V. (DGOM)) there are no conflicts of interest.
But, to tell you the truth, the article itself is worse, much worse that the abstract. Allow me to show you a few quotes (all my [sometimes free] translations).
- Osteopathic medicine is a therapeutic method based on the scientific findings from medical research.
- [The osteopath makes] diagnostic and therapeutic movements with the hands for evaluating limitations of movement. Thereby, a blocked joint as well as a reduced hydrodynamic or vessel perfusion can be identified.
- The indications of osteopathy are comparable to those of general medicine. Osteopathy can be employed from the birth of a baby up to the palliative care of a dying patient.
- Biostatisticians have recognised the weaknesses of RCTs and meta-analyses, as they merely compare mean values of therapeutic effects, and experts advocate a further evidence level in which statictical correlation is abandonnened in favour of individual causality and definition of cause.
- In ostopathy, the weight of our clinical experience is more important that external evidence.
- Research of osteopathic medicine … the classic cause/effect evaluation cannot apply (in support of this statement, the authors cite a ‘letter to the editor‘ from 1904; I looked it up and found that it does in no way substantiate this claim)
- Findings from anatomy, embryology, physiology, biochemistry and biomechanics which, as natural sciences, have an inherent evidence, strengthen in many ways the plausibility of osteopathy.
- Even if the statistical proof of the effectiveness of neurocranial techniques has so far been delivered only in part, basic research demonstrates that the effects of traction or compression of bogily tissue causes cellular reactions and regulatory processes.
What to make of such statements? And what to think of the fact that nowhere in the entire paper even a hint of ‘scrutiny’ can be detected? I don’t know about you, but for me this paper reflects very badly on both the authors and on osteopathy as a whole. If you ask me, it is an odd mixture of cherry-picking the evidence, misunderstanding science, wishful thinking and pure, unadulterated bullshit.
You urgently need to book into a course of critical thinking, guys!
The authors of this review wanted to determine similarities and differences in the reasons for using or not using so-called alternative medicine (SCAM) amongst general and condition-specific populations, and amongst populations in each region of the globe.
Quantitative or qualitative original articles in English, published between 2003 and 2018 were reviewed. Conference proceedings, pilot studies, protocols, letters, and reviews were excluded. Papers were appraised using valid tools and a ‘risk of bias’ assessment was also performed. Thematic analysis was conducted. Reasons were coded in each paper, then codes were grouped into categories. If several categories reported similar reasons, these were combined into a theme. Themes were then analysed using χ2 tests to identify the main factors related to reasons for CAM usage.
A total of 231 publications were included. Reasons for SCAM use amongst general and condition-specific populations were similar. The top three reasons were:
- (1) having an expectation of benefits of SCAM (84% of publications),
- (2) dissatisfaction with conventional medicine (37%),
- (3) the perceived safety of SCAM (37%).
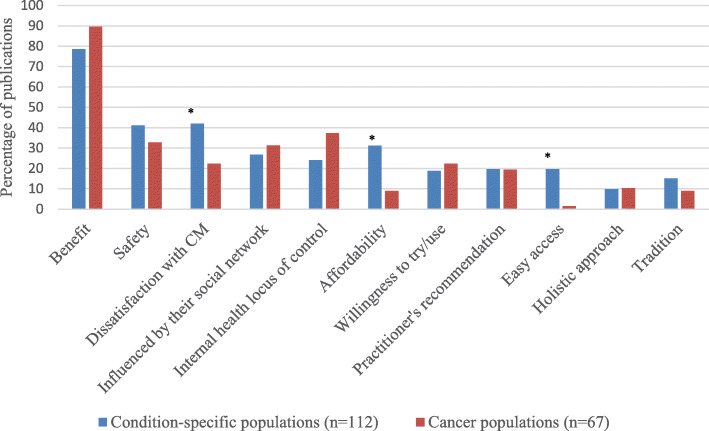
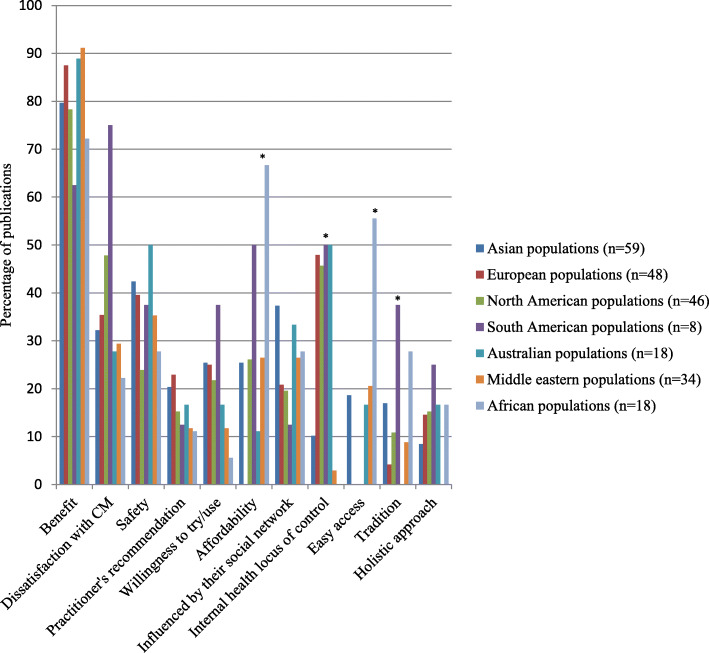
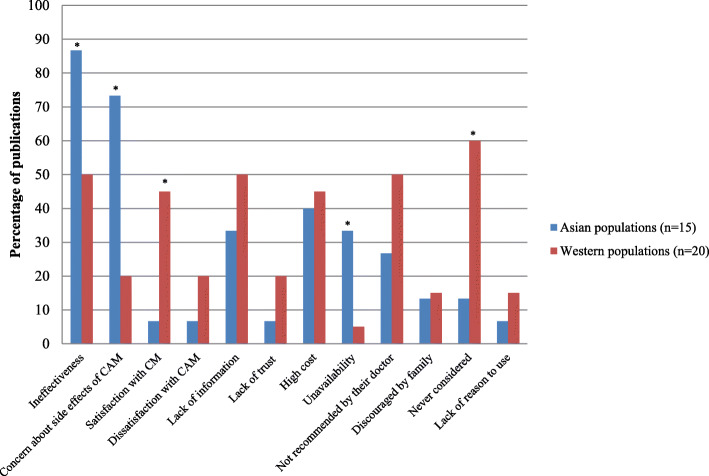
Internal health locus of control as an influencing factor was more likely to be reported in Western populations, whereas the social networks was a common factor amongst Asian populations (p < 0.05). Affordability, easy access to SCAM and tradition were significant factors amongst African populations (p < 0.05). Negative attitudes towards SCAM and satisfaction with conventional medicine were the main reasons for non-use (p < 0.05).
The authors concluded that dissatisfaction with conventional medicine and positive attitudes toward SCAM, motivate people to use SCAM. In contrast, satisfaction with conventional medicine and negative attitudes towards SCAM are the main reasons for non-use.
At this point, I thought: so what? This is all very obvious and does not necessitate an extensive review of the published literature. What it actually shows is that the realm of SCAM is obsessed with conducting largely useless surveys, a phenomenon, I once called ‘survey mania‘. But a closer look at the review does reveal some potentially interesting findings.
In less developed parts of the world, like Africa, SCAM use seems to be determined by affordability, accessibility and tradition. This makes sense and ties in with my impression that consumers in such countries would give up SCAM as soon as they can afford proper medicine.

This notion seems to be further supported by the reasons for not using SCAM. Asian consumers claim overwhelmingly that this is because they consider SCAM ineffective and unsafe.
In our review of 2011 (not cited in the new review), we looked at some of the issues from a slightly different angle and evaluated the expectations of SCAM users. Seventy-three articles met our inclusion criteria of our review. A wide range of expectations emerged. In order of prevalence, they included:
- the hope to influence the natural history of the disease;
- the desire to prevent disease and promote health/general well-being;
- the hope of fewer side effects;
- the wish to be in control over one’s health;
- the hope for symptom relief;
- the ambition to boost the immune system;
- the hope to receive emotional support;
- the wish to receive holistic care;
- the hope to improve quality of life;
- the expectation to relief of side effects of conventional medicine;
- the desire for a good therapeutic relationship;
- the hope to obtain information;
- the hope of coping better with illness;
- the expectation of supporting the natural healing process;
- the availability of SCAM.
All of these aspects, issues and notions might be interesting, even fascinating to some, but we should not forget three important caveats:
- Firstly, SCAM is such a diverse area that any of the above generalisations are highly problematic; the reasons and expectations of someone trying acupuncture may be entirely different from those of someone using homeopathy, for instance.
- Secondly (and more importantly), the ‘survey mania’ of SCAM researchers has not generated the most reliable data; in fact, most of the papers are hardly worth the paper they were printed on.
- Thirdly (and even more importantly, in my view), why should any of this matter? We have known about some of these issues for at least 3 decades. Has this line of research changed anything? Has it prevented consumers getting exploited by scrupulous SCAM entrepreneurs? Has it made consumers, politicians or anyone else more aware of the risks associated with SCAM? Has it saved many lives? I doubt it!
This systematic review and meta-analysis was aimed at investigating the effect and safety of acupuncture for the treatment of chronic spinal pain.
The authors included 22 randomized controlled trials (RCTs) involving patients with chronic spinal pain treated by acupuncture versus sham acupuncture, no treatment, or another treatment were included. Chronic spinal pain was defined as:
- chronic neck pain,
- chronic low back pain,
- or sciatica for more than 3 months.
Fourteen studies had a high risk of bias, 5 studies had a low risk of bias, and 5 studies had an unclear risk of bias. Pooled analysis revealed that:
- acupuncture can reduce chronic spinal pain compared to sham acupuncture (weighted mean difference [WMD] -12.05, 95% confidence interval [CI] -15.86 to -8.24),
- acupuncture can reduce chronic spinal pain compared to mediation control (WMD -18.27, 95% CI -28.18 to -8.37),
- acupuncture can reduce chronic spinal pain compared to usual care control (WMD -9.57, 95% CI -13.48 to -9.44),
- acupuncture can reduce chronic spinal pain compared to no treatment control (WMD -17.10, 95% CI -24.83 to -9.37).
In terms of functional disability, acupuncture can improve physical function at
- immediate-term follow-up (standardized mean difference [SMD] -1.74, 95% CI -2.04 to -1.44),
- short-term follow-up (SMD -0.89, 95% CI -1.15 to -0.62),
- long-term follow-up (SMD -1.25, 95% CI -1.48 to -1.03).

Trials assessed as having a high risk of bias (WMD −13.45, 95% CI −17.23 to −9.66, I 2 96.2%, moderate-quality evidence, including 14 studies and 1379 patients) found greater effects of acupuncture treatment than trials assessed as having a low risk of bias (WMD −11.99, 95% CI −13.94 to −10.03, I 2 44.6%, high-quality evidence, including 4 studies and 432 patients), but smaller effects than trials assessed as having an unclear risk of bias (WMD −14.51, 95% CI −17.25 to −11.78, I 2 0%, high-quality evidence, including 3 studies and 190 patients).
Only 6 trials provided information on adverse events. No trial reported data on serious adverse events during acupuncture treatment. The most frequent adverse events were temporarily worsened pain and needle pain at the acupuncture site, which can decrease quickly after a short period of rest.
The authors concluded that compared to no treatment, sham acupuncture, or conventional therapy such as medication, massage, and physical exercise, acupuncture has a significantly superior effect on the reduction in chronic spinal pain and function improvement. Acupuncture might be an effective treatment for patients with chronic spinal pain and it is a safe therapy.
I think this is a thorough review which produced interesting findings. I agree with most of what the authors report, except with their conclusions which I find too optimistic. In view of the facts that
- only 5 RCTs had a low risk of bias,
- collectively, the rigorous trials reported smaller effect sizes,
- the majority of trials failed to mention adverse effects which, in my view, casts considerable doubt on their quality and ethical standard,
I would have phrased the conclusion differently: compared to no treatment, sham acupuncture, or conventional therapies, acupuncture seems to have a significantly superior effect on pain and function. Due to the lack rigour of most studies, these effects are less certain than one would have wished. Many trials fail to report adverse effects which reflects poorly on their quality and ethics and prevents conclusions about the safety of acupuncture. In essence, this means that the effectiveness and safety of acupuncture as a treatment of chronic spinal pain remains uncertain.
I very rarely discuss animal experiments on this blog. Their applicability to clinical situations in human patients is almost invariably doubtful. Of course, this does not mean that they cannot be important; on the contrary, they may point the way towards relevant research and help formulate hypotheses.
This study might be exceptionally relevant in this way. To investigate the safety and efficacy of megadose sodium ascorbate in sepsis, sheep were instrumented with pulmonary and renal artery flow-probes, and laser-Doppler and oxygen-sensing probes in the kidney. Conscious sheep received an infusion of live Escherichia coli for 31 hours. At 23.5 hours of sepsis, sheep received fluid resuscitation (30 mL/kg, Hartmann solution) and were randomized to IV sodium ascorbate (0.5 g/kg over 0.5 hr + 0.5 g/kg/hr for 6.5 hr; n = 5) or vehicle (n = 5). Norepinephrine was titrated to restore mean arterial pressure to baseline values (~80 mm Hg).
Sepsis-induced fever (41.4 ± 0.2°C; mean ± SE), tachycardia (141 ± 2 beats/min), and a marked deterioration in clinical condition in all cases. Mean arterial pressure (86 ± 1 to 67 ± 2 mm Hg), arterial PO2 (102.1 ± 3.3 to 80.5 ± 3.4 mm Hg), and renal medullary tissue PO2 (41 ± 5 to 24 ± 2 mm Hg) decreased, and plasma creatinine doubled (71 ± 2 to 144 ± 15 µmol/L) (all p < 0.01).
Direct observation indicated that in all animals, sodium ascorbate dramatically improved the clinical state, from malaise and lethargy to a responsive, alert state within 3 hours. Body temperature (39.3 ± 0.3°C), heart rate (99.7 ± 3 beats/min), and plasma creatinine (32.6 ± 5.8 µmol/L) all decreased. Arterial (96.5 ± 2.5 mm Hg) and renal medullary PO2 (48 ± 5 mm Hg) increased. The norepinephrine dose was decreased, to zero in four of five sheep, whereas mean arterial pressure increased (to 83 ± 2 mm Hg).
These physiologic findings were subsequently confirmed in a coronavirus patient with shock by compassionate use of 60 g of sodium ascorbate over 7 hours.
The authors concluded that IV megadose sodium ascorbate reversed the pathophysiological and behavioral responses to Gram-negative sepsis without adverse side effects. Clinical studies are required to determine if such a dose has similar benefits in septic patients.
As always with animal experiments, it is difficult to extrapolate to clinical situations in human patients. However, the fact that the authors did try their approach on one COVID-19 patient is encouraging. I agree with their conclusion that careful human studies are now required.
Melatonin is an indolamine hormone which is secreted from the human pineal gland during night-time acting as physiological regulator. In many countries, dietary supplements containing synthetically produced melatonin are available. Melatonin is being promoted as a treatment of a range of conditions, including virtually all types of cancer.
One website, for instance, states that the anti-cancer benefits of melatonin aren’t just indirect; this miracle molecule is also classified as a directly cytotoxic hormone and anti-cancer agent. Studies have referred to melatonin as a “full-service anti-cancer agent” due to its ability to inhibit the initiation of cell mutation and cancer growth, and to halt the progression and metastasis of cancer cell colonies.
Such statements sound far too good to be true. So, let’s have a look and find out what the evidence tells us. Test-tube experiments suggest that melatonin has anti-cancer effects.[1] Its actions include the advancement of apoptosis, the arrest of the cell cycle, inhibition of metastasis, and antioxidant activity.[2]
A review of 21 clinical trials of melatonin for cancer found positive effects for complete response, partial response, and stable disease. In trials combining melatonin with chemotherapy, adjuvant melatonin therapy decreased 1-year mortality and improved outcomes of complete response, partial response, and stable disease. In these studies, melatonin also significantly reduced asthenia, leukopenia, nausea and vomiting, hypotension, and thrombocytopenia. The authors concluded that melatonin may benefit cancer patients who are also receiving chemotherapy, radiotherapy, supportive therapy, or palliative therapy by improving survival and ameliorating the side effects of chemotherapy.[3]
A further systematic review of RCTs of melatonin in solid tumour cancer patients evaluated its effect on one-year survival. Ten trials were included of melatonin as either sole treatment or as adjunct treatment. Melatonin reduced the risk of death at 1 year. Effects were consistent across melatonin dose, and type of cancer. No severe adverse events were reported.[4]
A 2012 systematic review confirmed these findings by concluding that Melatonin as an adjuvant therapy for cancer led to substantial improvements in tumor remission, 1-year survival, and alleviation of radiochemotherapy-related side effects.[5]
Finally, a 2020 review concluded that melatonin in combination with anticancer agents may improve the efficacy of routine medicine and survival rate of patients with cancer. [6] Apart from its direct anticancer potential, melatonin also seems to reduce chemotherapy toxicity, while improving its therapeutic efficacy.[7]
So, is this evidence compelling? While all this does indeed sound encouraging, it is necessary to mention several important caveats:
- The primary studies of melatonin suffer from several methodological shortcomings.
- Their vast majority originate from one single research group.
- In recent years, there have been no further clinical studies trying to replicate the initial findings.
This means that definitive trials are still missing, and it would seem wise to interpret the existing evidence with great caution.
References
[1] Kong X, Gao R, Wang Z, Wang X, Fang Y, Gao J, Reiter RJ, Wang J. Melatonin: A Potential Therapeutic Option for Breast Cancer. Trends Endocrinol Metab. 2020 Sep 3:S1043-2760(20)30155-7. doi: 10.1016/j.tem.2020.08.001. Epub ahead of print. PMID: 32893084.
[2] Samanta S. Melatonin: an endogenous miraculous indolamine, fights against cancer progression. J Cancer Res Clin Oncol. 2020 Aug;146(8):1893-1922. doi: 10.1007/s00432-020-03292-w. Epub 2020 Jun 24. PMID: 32583237.
[3] Seely D, Wu P, Fritz H, Kennedy DA, Tsui T, Seely AJ, Mills E. Melatonin as adjuvant cancer care with and without chemotherapy: a systematic review and meta-analysis of randomized trials. Integr Cancer Ther. 2012 Dec;11(4):293-303. doi: 10.1177/1534735411425484. Epub 2011 Oct 21. PMID: 22019490.
[4] Mills E, Wu P, Seely D, Guyatt G. Melatonin in the treatment of cancer: a systematic review of randomized controlled trials and meta-analysis. J Pineal Res. 2005 Nov;39(4):360-6. doi: 10.1111/j.1600-079X.2005.00258.x. PMID: 16207291.
[5] Wang YM, Jin BZ, Ai F, Duan CH, Lu YZ, Dong TF, Fu QL. The efficacy and safety of melatonin in concurrent chemotherapy or radiotherapy for solid tumors: a meta-analysis of randomized controlled trials. Cancer Chemother Pharmacol. 2012 May;69(5):1213-20. doi: 10.1007/s00280-012-1828-8. Epub 2012 Jan 24. PMID: 22271210.
[6] Pourhanifeh MH, Mehrzadi S, Kamali M, Hosseinzadeh A. Melatonin and gastrointestinal cancers: Current evidence based on underlying signaling pathways. Eur J Pharmacol. 2020 Nov 5;886:173471. doi: 10.1016/j.ejphar.2020.173471. Epub 2020 Aug 30. PMID: 32877658.
[7] Iravani S, Eslami P, Dooghaie Moghadam A, Moazzami B, Mehrvar A, Hashemi MR, Mansour-Ghanaei F, Mansour-Ghanaei A, Majidzadeh-A K. The Role of Melatonin in Colorectal Cancer. J Gastrointest Cancer. 2020 Sep;51(3):748-753. doi: 10.1007/s12029-019-00336-4. PMID: 31792737.
- the chiro suggests a manipulation of the neck;
- this often involves forcing a spinal joint beyond its physiological range of motion;
- the treatment will be short but needs repeating several times during the coming weeks;
- the expected benefits are a reduction of pain and improvement of motion;
- the total cost of the treatment series will be xy;
- there are many other treatment options for neck pain;
- most of these have a better risk/benefit profile than neck manipulation;
- having no treatment for neck pain at all is likely to lead to full resolution of the problem over time.
Apart from any doubts that chiropractors would actually comply with these requirements, the question remains: is the listed information sufficient? Does it outline a truly a fully informed consent? I think that essential aspects of informed consent are missing.
- The code does not explicidly require an explanation about the possible harms of spinal manipulation (i.e. 50% of all patients will suffer mild to moderate adverse effects lasting 2-3 days, and occasionally patients will have a stroke of which some have died).
- Moreover, the code mentions EXPECTED benefits, but not benefits supported by evidence. Chiros may well EXPECT their treatment to work, but what does the evidence show? As often discussed on this blog, the evidence is negative or very week, depending how you want to interpret it. The code does not require a chiro to inform his patients about this fact.
So, the way I see it, the code does not expressedly demand the chiro to explain his patient that the treatment he is being asked to consent to is
- not supported by sound evidence for effectiveness,
- nor that the treatment is burdened with significant risks.
And what about the other questions listed above? An Australian chiropractor who will remain anonymous gave me the following answers:
_____________________________________
Yet, Australian chiropractors claim that they abide by the ethical imperative of informed consent. Are they taking the Mickey?
Perhaps not. Perhaps they are merely trying to make sure they do not lose the majority of their clientele. As I already pointed out in my previous post, fully informed consent would make most chiropractic patients turn round and run a mile.
I was alerted to an outstanding article by an unusual author, a law firm, on the subject of chiropractic. Allow me to quote a few passages from it (without changing a word or adding a comment):
When Katie May passed away suddenly from a stroke at just 34 years old, it was initially ruled an accident. After further investigation, a coroner determined the stroke that claimed the model and single mother’s life was caused by injuries sustained during neck manipulation by a chiropractor. And Ms. May is not the first to be affected by this seemingly harmless procedure…
What health issues can be caused by chiropractic manipulation?
Chiropractors typically use their hands to apply pressure to joints, aiming to help alleviate pain and improve body function. This is referred to as a chiropractic adjustment.
Adjustments are commonly performed for neck and/or back pain. Although the Mayo Clinic says the risk of a serious complication is relatively small, these complications can include:
- A herniated disk, or worsening of an existing herniated disk
- Compression of nerves in the lower spinal column
- Stroke, which can result in paralysis or death
The last item on this list is particularly concerning.
Patients who receive neck manipulation are at risk for a stroke caused by vertebral artery dissection. Located in the neck, the vertebral arteries supply blood to the brain and can be torn by stretching and sudden force applied during a neck adjustment.
Studies have shown that vertebral artery dissection occurs in approximately 1 in 100,000 people and can be caused by something as simple as cracking your neck.
How could a chiropractor be responsible for a patient’s injury?
Although the risk of being seriously injured by a chiropractor is low, tragic accidents can and do happen. If you or a loved one believe you have been the victim of medical malpractice, please contact an experienced personal injury attorney.
Explaining how an injury or medical error occurred will help your attorney determine the potential liability of a chiropractor and any other involved parties. A chiropractor’s liability could fall into a legal category such as:
- Failure to Diagnose a Medical Condition – The chiropractor breaches a duty of care to their patients by failing to diagnose an underlying medical condition. This could occur when a patient reveals or exhibits symptoms of a severe issue, such as a stroke, and is not referred for appropriate medical attention.
- Lack of Informed Consent – A patient is treated without being properly informed of the potential risks or side effects, and experiences an injury from that treatment.
- Negligent Manipulation – The patient’s body is adjusted by the chiropractor in such a way that it causes a new injury or worsens an existing injury. This could also include manipulation of a patient who is pregnant and goes into premature labor.
- Chiropractic Induced Injury – A patient suffers injury, permanent irreversible damage such as paralysis or wrongful death as the direct result of a chiropractic manipulation.
To find out whether or not you may have a case, please discuss your concerns with a qualified personal injury attorney.
What should I do if I think I have been injured by chiropractic manipulation?
A personal injury attorney can help recover compensation for victims of medical malpractice, including those who have experienced a chiropractic injury. Surviving loved ones can also pursue their case after a family member’s wrongful death.
An attorney will help you collect documents, photos and other items pertaining to your case – but staying organized early in the process will be helpful. Try to preserve important documents, such as:
- Photographs before and after treatment
- Medical records and medical bills
- Receipts, appointment confirmations and other paperwork from your chiropractor
There is a time limit to file a medical malpractice lawsuit, referred to as a statute of limitations…
The issue of informed consent has made regular appearances on this blog. It is important and has many intriguing aspects, particularly for so-called alternative medicine (SCAM). On the one hand, it is a ‘conditio sine qua non’ for any form of healthcare, while, on the other hand, it is a near impossibility in SCAM practice.
In this new article published in a chiro-journal, the authors review the origins of informed consent and trace the duty of disclosure and materiality through landmark medical consent cases in four common law (case law) jurisdictions. The duty of disclosure has evolved from a patriarchal exercise to one in which patient autonomy in clinical decision making is paramount. Passing time has seen the duty of disclosure evolve to include non-medical aspects that may influence the delivery of care. The authors argue that a patient cannot provide valid informed consent for the removal of vertebral subluxation. Further, vertebral subluxation care cannot meet code of conduct standards because it lacks an evidence base and is practitioner-centered.
The uptake of the expanded duty of disclosure has been slow and incomplete by practitioners and regulators. The expanded duty of disclosure has implications, both educative and punitive for regulators, chiropractic educators and professional associations. The authors discuss how practitioners and regulators can be informed by other sources such as consumer law. For regulators, reviewing and updating informed consent requirements is required. For practitioners it may necessitate disclosure of health status, conflict of interest when recommending “inhouse” products, recency of training after attending continuing professional development, practice patterns, personal interests and disciplinary findings.
The authors conclude that, ultimately such matters are informed by the deliberations of the courts. It is our opinion that the duty of a mature profession to critically self-evaluate and respond in the best interests of the patient before these matters arrive in court.
In their paper, the authors also provide a standard list of items required for ‘informed’ consent:
(1) emphasizing the patient’s role in shared decision-making
(2) disclosure of information
a. explaining the patient’s medical status including diagnosis and prognosis
b. describing the proposed diagnostic and therapeutic intervention, including the likelihood and effect of associated risks and benefits of the proposed action, including material risks
c. discussing alternatives to the proposed intervention, including doing nothing
(3) prompting and answering patient questions related to the proposed course of action (NB. this involves probing for understanding, not simply asking ‘do you have any questions’), and
(4) eliciting the patient’s preference (usually by signature). (NB. A signed form is not consent. The conversation between the clinician and the patient or carer is the true process of obtaining informed consent. The signature on the consent form is proof that the conversation took place and that the patient understood and agreed.)
The authors of this article – I do commend it to all chiropractors – take a mostly judicial view of informed consent (for an ethical perspective on the subject, I recommend our book). They do not discuss, whether chiropractors do, in fact, adhere to the ethical imperative of informed consent. As I have stated before, there is not much research on this issue. But the little that does exist fails to show that chiropractors care much about it.
But why?
If it’s an ethical imerative, why do chiropractors not abide by it?
The answer to this question is not difficult to find. Just imagine a conversation between a chiropractor (C) and a patient with neck pain (P):
- P: What’s your diagnisis?
- C: You are suffering from acute neck pain.
- P: Thanks, that much was clear to me. What do you suggest I do?
- C: I will perform a manipulation of your neck, if you agree.
- P: Why would this help?
- C: It can realign the vertebrae that are out of place, simply put.
- P: And my pain will disappear?
- C: Sometimes it does, yes.
- P: But will it disappear quicker than without manipulation.
- C: Some of the evidence says so.
- P: Ok, but what does the most reliable evidence say?
- C: It is not entirely clear cut.
- P: Hmm, that does not sound too good.
- P: So, tell me, are there any risks?
- C: About 50% of patients suffer from minor to moderate pain for 2-3 days afterwards.
- P: That’s a lot!
- P: Anything else?
- C: In some cases, neck manipulation was followed by a stroke.
- P: Gee that’s bad; how often has this happened?
- C: We know of about 500 such cases.
- P: Heavens!
- C: Now, do you want the treatment or not?
- P: How much will you charge?
- C: Only 60 Euros per session.
- P: You mean I have to come back for more, each time risking a stroke?
- C: Well… You don’t have to.
- P: Thanks for the info; I am off. Cherio!
I rest my case.
I know of one patient who turned to the Gerson Therapy having been told that she was suffering from terminal cancer and would not survive another course of chemotherapy. Happily, seven years later she is alive and well. So therefore it is vital that, rather than dismissing such experiences, we should further investigate the beneficial nature of these treatments.
HRH The Prince of Wales (2004)
I was reminded of this embarrassing (because displaying profound ignorance) quote when I looked at the website of the ‘GERSON SUPPORT GROUP UK‘ where it is prominently cited. Under the heading ‘SCIENCE & CLINICAL RATIONAL’ the site offers a long article about the Gerson therapy (GT). Allow me to show you a few quotes from it:
Dr Max Gerson’s therapy is based on the belief that insufficient nutrients within the cells and an accumulation of toxins in the tissues lead to a breakdown in healthy cellular function which, if left unchecked, can trigger cancer.
That is interesting, I find, because the statement clearly admits that the GT is not an evidence-based therapy but a belief-based treatment.
The therapy that he developed uses a restrictive, plant-based diet and specific supplements to boost healthy cellular function; and various detoxification procedures, including coffee enemas, to eliminate waste products.
The claims hidden in this sentence remain unproven. There is no evidence that cellular fuction is boosted, nor that the procedures eliminate toxins.
… we only need to look at communities across the globe which exist in a pre-industrialised state to see that, whilst they might be more likely to die from pneumonia or tuberculosis, rates of degenerative illness are a fraction of those in the ‘developed‘ world. The age-adjusted death rate from breast cancer is less than 2 per 100,000 of the population in Thailand, Sri Lanka and El Salvador and around 33 per 100,000 in the UK, US, The Netherlands and numerous other affluent, Western countries.
Correlation is not causation! Pre-industrial societies also watch less TV, eat less ice-cream, read less fashion magazines, etc., etc. Are these habits also the cause of cancer?
… migrant studies show that within two generations the cancer rates of migrants increase rapidly towards Western rates, again underlining the assertion that cancer is caused primarily by diet and lifestyle rather than ‘faulty’ genes.
In no way is this an argument for eating raw vegetable and taking your coffee via the rectum.
In the German scientific golden age of the 1920s and 30s…
Golden age for what, for fascists?
Gerson had used a restricted diet to cure himself of migraines. He then helped another patient to reverse tuberculosis, and many others to reverse a variety of degenerative illnesses, all by similar means. He later developed his therapy to the point where he was able to help individuals reverse cancer.
In this case, Max Gerson was ignorant of the fact that experience and evidence are two fundamentally different things.
Max Gerson developed his therapy in an iterative way, starting with a restrictive plant-based diet, adding vitamins, minerals and enzymes to encourage the oxygenation of the cells and then introducing the coffee enemas to aid detoxification of waste products. What is fascinating is that science has subsequently explained the mechanism of action behind some of his theories. (See Biochemical Basis to the Therapy).
Science has not explained the mechanism of action, not least because the action has never been verified. There are no robust clinical trials of Gerson’s therapy. Evidently, 100 years were not enough to conduct any – or perhaps the proponents know only too well that they would not generate the results they hoped?
Equally interesting is that in 2012 Dr Thomas Seyfried published the results of many years research in Cancer as a Metabolic Disease.
Really? On Medline, I find only two cancer-related papers for Seyfried T. 2012:
Dietary restriction promotes vessel maturation in a mouse astrocytoma.
Thus, nearly a century after their original proposition that the fundamental cause of cancer was faulty cellular metabolism, it seems that doctors Otto Warburg and Max Gerson might be vindicated.
No, to ‘vindicate’ a therapeutic suggestion one needs several rigorous clinical trials. And for the GT, they remain absent.
_______________________________
So, what does the GT amount to?
- proponents had ~100 years to produce evidence;
- they failed to do so;
- thus the therapy is at best unproven;
- it is also biologically implausible;
- moreover, it is expensive;
- crucially it is not free of serious adverse effects;
- it is promoted only by those who seem to make money from it.
The only controlled clinical trial of a Gerson-like therapy that I know of is this one (rarely cited by Gerson fans):
Conventional medicine has had little to offer patients with inoperable pancreatic adenocarcinoma; thus, many patients seek alternative treatments. The National Cancer Institute, in 1998, sponsored a randomized, phase III, controlled trial of proteolytic enzyme therapy versus chemotherapy. Because most eligible patients refused random assignment, the trial was changed in 2001 to a controlled, observational study.
METHODS
All patients were seen by one of the investigators at Columbia University, and patients who received enzyme therapy were seen by the participating alternative practitioner. Of 55 patients who had inoperable pancreatic cancer, 23 elected gemcitabine-based chemotherapy, and 32 elected enzyme treatment, which included pancreatic enzymes, nutritional supplements, detoxification, and an organic diet. Primary and secondary outcomes were overall survival and quality of life, respectively.
RESULTS
At enrollment, the treatment groups had no statistically significant differences in patient characteristics, pathology, quality of life, or clinically meaningful laboratory values. Kaplan-Meier analysis found a 9.7-month difference in median survival between the chemotherapy group (median survival, 14 months) and enzyme treatment groups (median survival, 4.3 months) and found an adjusted-mortality hazard ratio of the enzyme group compared with the chemotherapy group of 6.96 (P < .001). At 1 year, 56% of chemotherapy-group patients were alive, and 16% of enzyme-therapy patients were alive. The quality of life ratings were better in the chemotherapy group than in the enzyme-treated group (P < .01).
CONCLUSION
Among patients who have pancreatic cancer, those who chose gemcitabine-based chemotherapy survived more than three times as long (14.0 v 4.3 months) and had better quality of life than those who chose proteolytic enzyme treatment.
Considering all this, I believe, it would be hard to name a cancer quackery that is less credible than the GT.
THE FIRST WORLDWIDE MANIFESTO AGAINST PSEUDOSCIENCE
2750 signatories from 44 countries have signed it [I was number 11] and today is its official launch. I am delighted to present to you the full text of the English version:
Let’s be clear: pseudoscience kills. And they are being used with total impunity thanks to European
laws that protect them.
They kill thousands of people, with names and families. People such as Francesco Bonifaz, a 7-yearold boy whose doctor prescribed homeopathy instead of antibiotics. He died in Italy [1]. People like Mario Rodríguez, who was 21 years old and was told to use vitamins to treat his cancer. He died in Spain [2]. People like Jacqueline Alderslade, a 55-year-old woman whose homeopath told her to stop taking her asthma medication. She died in Ireland [3]. People like Cameron Ayres, a 6-month-old baby, whose parents did not want to give their child “scientific medicine”. He died in England [4]. People like Victoria Waymouth, a 57-year-old woman who was prescribed a homeopathic medication to treat her heart problem. She died in France [5]. People like Sofia Balyaykina, a 25-year-old woman, who had a cancer that was curable with chemotherapy but was recommended an “alternative treatment”, a mosquito bite treatment. She died in Russia [6]. People like Erling Møllehave, a 71-year-old man whose acupuncturist pierced and damaged his lung with a needle. He died in Denmark [7]. People like Michaela Jakubczyk-Eckert, a 40-year-old-woman whose therapist recommended the German NewMedicine to treat her breast cancer. She died in Germany [8]. People like Sylvia Millecam, a 45-year-old woman whose New Age healer promised to cure her cancer. She died in the Netherlands [9].
European directive 2001/83/CE has made –and still makes— possible the daily deception of thousands of hundreds of European citizens [10]. Influential lobbyists have been given the opportunity to redefine what a medicine is, and now they are selling sugar to sick people and making them believe it can cure them or improve their health. This has caused deaths and will continue to do so until Europe admits an undeniable truth: scientific knowledge cannot yield to economic interests, especially when it means deceiving patients and violating their rights.
Europe is facing very serious problems regarding public health. Overmedication, multi-resistant bacteria and the financial issues of the public systems are already grave enough, without the additional problem of gurus, fake doctors or even qualified doctors claiming they can cure any disease by manipulating chakras, making people eat sugar or using “quantic frequencies”. Europe must not only stop the promotion of homeopathy but also actively fight to eradicate public health scams. More than 150 pseudo-therapies have been identified as being in use throughout Europe. Thousands of citizens lives depend on this being prevented. In fact, according to a recent research, 25.9 % of Europeans have used pseudo-therapies last year. In other words, 192 million patients have been deceived [11].
Some believe there is a conflict between freedom of choice for a treatment and the removal of pseudo-therapies, but this is not true. According to article 25 of the Universal Declaration of Human Rights, every person has a right to medical care. Lying to patients in order to sell them useless products that could kill them breaks their right to correct information about their health. This way, even if a citizen has a right to refuse medical treatment when he or she is properly informed, it is also true that nobody has the right to lie to obtain profit at the expense of someone else’s life. Only in a world in which lying to a sick person would be considered ethical, could homeopathy —or any other pseudo-therapy— be allowed to continue to be sold to citizens.
Effective treatments being replaced by false ones is not the only danger of pseudo-therapies. Obvious delays in therapeutic care occur when a person gets false products instead of medication at the early stages of a disease. Many times, it is then too late by the time they get treated with proper medicine. Moreover, several of these practices have serious effects on their own and may cause damage or even death because of their side effects.
Many pseudo-therapists argue that “the other medicine” comes with side effects as well, which is indeed true. However, the difference resides in that pseudo-therapies cannot cure a disease or improve your health, and because of that patients assume risks in exchange of promises that are a scam, according to the full weight of the scientific evidence available. Lying to a sick person is not another type of medicine, it is simply lying to a sick person.
Every country has to face the pseudo-therapies issue in its own ways. Yet it is not acceptable that European laws protect the distortion of scientific facts so that thousands of citizens can be deceived or even lead to their deaths.
We, the signatories of this manifest, therefore declare that:
1. Scientific knowledge is incompatible with what pseudo-therapies postulate, as in the case
of homeopathy.
2. European laws that protect homeopathy are not acceptable in a scientific and technological
society that respects the right of the patients not to be deceived.
3. Homeopathy is the best known pseudo-therapy, but it is not the only one nor the most
dangerous one. Others, such as acupuncture, reiki, German New Medicine, iridology,
biomagnetism, orthomolecular therapy and many more, are gaining ground and causing
victims.
4. Measures must be taken to stop pseudo-therapies, since they are harmful and result in
thousands of people being adversely affected.
5. Europe needs to work towards creating legislation that will help stop this problem.
Europe being concerned about the misinformation phenomena but at the same time protecting one the most dangerous types of it, health misinformation, is just not coherent. This is why the people signing this manifesto urge the governments of European countries to end a problem in which the name of science is being used falsely and which has already cost too many lives.
[1] Homeopathy boy died of encephalitis. Redazione ANSA, 2017.
http://www.ansa.it/english/news/general_news/2017/05/29/homeopathy-boy-died-of-encephalitis-3_13e02493-
4e62-4787-9162-12d831121ef6.html
[2] Grieving dad sues over ‘cure cancer with vitamins’ therapy, The local. Emma Anderson, 2016.
https://www.thelocal.es/20160412/grieving-father-sues-naturopath-over-son-cure-cancer-vitamins-leukaemia
[3] Asthmatic ‘told to give up drugs’. The Irish News, 2001.
https://www.independent.ie/irish-news/asthmatic-told-to-give-up-drugs-26063764.html
[4] Homeopaths warn of further tragèdies. BBC News, 2000.
http://news.bbc.co.uk/2/hi/health/702699.stm
[5] Alternative cure doctor suspended. BBC News, 2007.
http://news.bbc.co.uk/2/hi/uk_news/england/london/6255356.stm
[6] Футболист рассказал трагичную историю жены. Она умерла от рака в 25 лет. Sport24, 2018.
https://sport24.ru/news/football/2018-08-28-futbolist-rasskazal-tragichnuyu-istoriyu-zheny-ona-umerla-ot-raka-v-25-let
[7] Mand døde efter akupunktur – enke vil nu lægge sag an mod behandleren, TV2, 2018.
http://nyheder.tv2.dk/samfund/2018-01-23-mand-doede-efter-akupunktur-enke-vil-nu-laegge-sag-an-modbehandleren [8] The price of refusing science-based medical and surgical therapy in breast càncer, Science Blogs, 2012.
https://scienceblogs.com/insolence/2012/08/30/the-price-of-refusing-science-based-medical-and-surgical-therapy-inbreast-cancer
[9] Psychic ‘misled actress to hopeless cancer death’. Expatica. 2004.
http://web.archive.org/web/20070208144309/http://www.expatica.com/actual/article.asp?subchannel_i
d=19&story_id=4821
[10] Directive 2001/83/EC of the European Parliament and of the Council of 6 November 2001.
https://ec.europa.eu/health/sites/health/files/files/eudralex/vol1/dir_2001_83_consol_2012/dir_2001_83_cons_2012_en.pdf
[11] Use of complementary and alternative medicine in Europe: Health-related and sociodemographic
determinants. Scandinavian Journal of Public Health. Laura M. Kemppainen et al. 2018.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5989251/
FOUR QUESTIONS TO DC + CRITICAL CHIRO (CC):
1) what does the law say about informed consent for Australian chiros?
2) what info exactly do you have to provide?
3) who monitors it?
4) what published evidence do we have about compliance?
CC then posted this reply:
Here we go again you demand evidence while providing little if any for your own assumptions (poor case studies do not count. The pleural of anecdote does not equal evidence whether it’s from chiro’s or you).
We have been over this many times over many years, I cite research/provide links yet you still find it challenging to take it onboard. It is human nature to feel obligated once making a public statement to defend it no matter how much evidence is sent your way. So not surprising.
“1) what does the law say about informed consent for Australian chiros?”
It is all freely available on the national regulators website (as you know and as I have referenced in the past):
https://www.chiropracticboard.gov.au/Codes-guidelines/Code-of-conduct.aspx
https://www.chiropracticboard.gov.au/Search.aspx?q=Informed+consent
Some research by chiropractors on this topic (cited many times in the past):
Risk Management for Chiropractors and Osteopaths. Informed consent
A Common Law Requirement (2004):
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2051308/
Quick advanced PubMed with filters set to “Chiropractic” AND “Informed consent”.
https://www.ncbi.nlm.nih.gov/pmc/?term=(Chiropractic)+AND+Informed+consent
Not rocket science
Latest paper that you wrote an ill informed blog on and the comments were not going as you expected (So I expected you to double down like Donald Trump with a new blog within days. Your getting predictable).
https://chiromt.biomedcentral.com/articles/10.1186/s12998-020-00342-5
This paper questions the legal implications of vertebral subluxations with high powered legal input and is a broadside by evidence based chiropractors against vitalistic chiropractors. You respond a snide fantasy informed consent dialogue when you should be supporting the authors:
https://edzardernst.com/2020/11/informed-consent-why-chiropractors-dont-like-it/
“2) what info exactly do you have to provide?”
“4) what published evidence do we have about compliance?”
We have discussed this as well. It is a common law requirement for every profession and is checked upon re-registration by AHPRA every year and by the professional indemnity insurers every year. No informed consent, no registration and no professional indemnity insurance.
Checked AHPRA’s panel decisions and went back 5 YEARS and found ONE decision relating to informed consent:
https://www.ahpra.gov.au/Publications/Panel-decisions.aspx
“3) who monitors it?”
Another of your tired old arguments that we have discussed many times over the years.
In the UK there is the “‘Chiropractic Reporting and Learning System’ (CRLS)” but this is set up by the association representing chiropractors and not the registration board that advocates for patients. Right idea and step in the right direction, wrong organization.
Here years ago there was a trial of an adverse event reporting system in a Melbourne emergency department systematically collected relevant AE information on all professions which was sent to the relevant board for investigation.
It was supported by doctors and chiropractors while physio’s were not involved. A doctor involved told me it was killed off by ER doctors who “snivelled” about the extra paperwork.
There is no AE reporting system for physio’s, chiro’s, osteo’s, GP’s in private practice etc.
Over the years you have harped on and on about this topic as if it is a failing purely of the chiropractic profession when we have supported initiatives for its implementation.
You have also kept up with the research even commenting on an chiropractic researcher on AE’s Charlotte Leboeuf-Yde (who you highly regard) yet ignored until you could take issue with two sentences written in a blog then you wrote this hatchet blog:
https://edzardernst.com/2017/04/we-have-an-ethical-legal-and-moral-duty-to-discourage-chiropractic-neck-manipulations/
So you are asking for evidence yet willfully ignore an author who “I have always thought highly of Charlotte’s work”.
Stop the cynical cherry picked blogs and start supporting the researchers and reformers otherwise you are just someone standing on the sidelines blindly throwing grenades. You do not care who you hit or the damage you do to the chiropractors leading the reform you demand yet consistently fail to support.
____________________________________
I thought the tone of this response was oddly aggressive and found that CC had failed to understand some of my questions. Yet the link to the chiro’s code of conduct https://www.chiropracticboard.gov.au/Codes-guidelines/Code-of-conduct.aspx was useful. This is what it says about informed consent: