research
It has been reported that Goop founder Gwyneth Paltrow now has taken to promoting the weirdest wellness thing she’s ever done: rectal ozone therapy. ‘I have used ozone therapy, rectally. Can I say that?’ she told Dear Media podcast The Art of Being Well. ‘It’s pretty weird. It’s pretty weird, yeah. But it’s been very helpful.’
The benefits of rectal ozone therapy are said to be reduced pain/inflammation, increased energy, improved metabolism/circulation, stimulated immune system, detoxification, anti-aging, and fighting bacterial/viral infections.
But who am I to criticize an authority like Gwyneth?
Therefore, I better look up the evidence! And if you had speculated that there is none, you would have been mistaken. Here are some of the more recent clinical studies listed in Medline:
Objective: Fibromyalgia is a chronic disorder with a very complex symptomatology. Although generalized severe pain is considered to be the cardinal symptom of the disease, many other associated symptoms, especially non-restorative sleep, chronic fatigue, anxiety, and depressive symptoms also play a relevant role in the degree of disability characteristic of the disease. Ozone therapy, which is used to treat a wide range of diseases and seems to be particularly useful in the treatment of many chronic diseases, is thought to act by exerting a mild, transient, and controlled oxidative stress that promotes an up-regulation of the antioxidant system and a modulation of the immune system. According to these mechanisms of action, it was hypothesized that ozone therapy could be useful in fibromyalgia management, where the employed therapies are very often ineffective.
Patients and methods: Sixty-five patients with fibromyalgia, according to the definition of the American College of Rheumatology (Arthritis Rheum 1990; 33: 160-172), were treated at the MEDE Clinic (Sacile, Pordenone, Italy) from February 2016 to October 2018. Females were 55 and males were 10; age ranged from 30 to 72 years, and the time from fibromyalgia diagnosis ranged from 0.5 to 33 years. Treatment was made by autohemotransfusion in 55 patients and by ozone rectal insufflations in 10 patients, according to SIOOT (Scientific Society of Oxygen Ozone Therapy) protocols, twice a week for one month and then twice a month as maintenance therapy.
Results: We found a significative improvement (>50% of symptoms) in 45 patients (70%). No patient reported important side effects. In conclusion, at our knowledge, this is the largest study of patients with fibromyalgia treated with ozone therapy reported in the literature and it demonstrates that the ozone therapy is an effective treatment for fibromyalgia patients without significant side effects.
Conclusions: At the moment, ozone therapy seems a treatment that, also because without any side effect, is possible to be proposed to patients with fibromyalgia that are not obtaining adequate results from other available treatments and it can be considered as complementary/integrative medicine.
No2:
Introduction: The Corona virus disease 19 (COVID-19) has accounted for multiple deaths and economic woes.While the entire medical fraternity and scientists are putting their best feet forward to find a solution to contain this deadly pandemic, there is a growing interest in integrating other known alternative therapies in to standard care. This study is aimed at evaluating the safety and efficacy of ozone therapy (OT), as an adjuvant to the standard of care (SOC).
Methods: In the current randomized control trial, 60 patients with mild to moderate score NEWS score were included in two parallel groups (n = 30/group). The interventional group (OZ) received ozonized rectal insufflation and minor auto haemotherapy, daily along with SOC, while the control group (ST) received SOC alone. The main outcome measures included changes in clinical features, oxygenation index (SpO2), NEWS score, Reverse transcription polymerase chain reaction(RT-PCR), inflammatory markers, requirement of advanced care, and metabolic profiles.
Results: The OZ group has shown clinically significant improvement in the mean values of all the parameters tested compared to ST Group. However, statistical significance were only observed in RT-PCR negative reaction (P = 0.01), changes in clinical symptoms (P < 0.05) and requirement for Intensive care (P < 0.05). No adverse events were reported in OZ group, as against 2 deaths reported in ST group.
Conclusion: OT when integrated with SOC can improve the clinical status and rapidly reduce the viral load compared to SOC alone, which facilitate early recovery and check the need for advanced care and mortality as demonstrated in this study.
Introduction: IgA deficiency is a primary immunodeficiency predominantly due to an antibody defect, for which there is no replacement therapy. Treatment consists of prevention and treatment of infections and other associated conditions. Given the immunomodulatory and regulatory properties of the redox balance of ozone therapy in infectious and inflammatory conditions, evaluation of its effect on IgA deficiency is of interest.
Objective: Assess the benefits and possible adverse effects of ozone treatment in patients with IgA deficiency.
Methods: A monocentric randomized controlled phase 2 clinical trial (RPCEC 00000236) was carried out, after approval by the Institutional Ethics Committee of the Roberto Rodríguez Fernández Provincial General Teaching Hospital in Morón, Ciego de Ávila Province, Cuba. Included were 40 patients aged 5-50 years, distributed in 2 groups of 20, after agreeing to participate and signing informed consent. The experimental group received 2 cycles of ozone by rectal insufflation for 20 days (5 times a week for 4 weeks each cycle) with a 3-month interval between cycles, for a total of 40 doses, with age-adjusted dose ranges. The control group was treated with leukocyte transfer factor (Hebertrans), 1 U per m2 of body surface area subcutaneously, once weekly for 12 weeks. Frequency of appearance and severity of clinical symptoms and signs of associated diseases, serum immunoglobulin concentrations and balance of pro-oxidant and antioxidant biomarkers were recorded at treatment initiation and one month after treatment completion. Therapeutic response was defined as complete, partial, stable disease or progressive disease. Descriptive statistics and significance were calculated to compare groups and assess effect size.
Results: One month after treatment completion, 70% of patients in the experimental group experienced significant increases in IgG(p = 0.000) and IgM (p = 0.033). The experimental group also displayed decreased pro-oxidation biomarkers, glutathione modulation and increased antioxidant enzymes, with reduced oxidative stress; none of these occurred in the control group. Complete therapeutic response was achieved in 85% of patients in the experimental group and only 45% in the control group. Mild, transient adverse events were reported in both groups.
Conclusions: Ozone therapy by rectal insufflation is a suitable therapeutic option for treating IgA deficiency because it produces antioxidant and immunomodulatory effects and is feasible, safe and minimally invasive.
Background: Ozone therapy may stimulate antioxidant systems and protect against free radicals. It has not been used formerly in patients with pulmonary emphysema.
Aim: To assess the effects of rectal ozone therapy in patients with pulmonary emphysema.
Material and methods: Sixty four patients with pulmonary emphysema, aged between 40 and 69 years, were randomly assigned to receive rectal ozone in 20 daily sessions, rectal medicinal oxygen or no treatment. Treatments were repeated three months later in the first two groups. At baseline and at the end of the study, spirometry and a clinical assessment were performed.
Results: fifty patients completed the protocol, 20 receiving ozone therapy, 20 receiving rectal oxygen and 10 not receiving any therapy. At baseline, patients on ozone therapy had significantly lower values of forced expiratory volume in the first second (fEV1) and fEV1/forced vital capacity. At the end of the treatment period, these parameters were similar in the three treatment groups, therefore they only improved significantly in the group on ozone therapy. No differences were observed in other spirometric parameters.
Conclusions: Rectal ozone therapy may be useful in patients with pulmonary emphysema.
Background: Pain secondary to chemotherapy-induced peripheral neuropathy (CIPN) can limit the administration of chemotherapy, cancer-treatment outcomes, and the quality of life of patients. Oxidative stress and inflammation are some of the key mechanisms involved in CIPN. Successful treatments for CIPN are limited. This report shows our preliminary experience using ozone treatment as a modulator of oxidative stress in chronic pain secondary to CIPN. Methods: Ozone treatment, by rectal insufflation, was administered in seven patients suffering from pain secondary to grade II or III CIPN. Pain was assessed by the visual analog scale (VAS). Results: All patients, except one, showed clinically relevant pain improvement. Median pain score according to the VAS was 7 (range: 5-8) before ozone treatment, 4 (range: 2-6) at the end of ozone treatment (p = 0.004), 5.5 (range: 1.8-6.3) 3 months after the end of ozone treatment (p = 0.008), and 6 (range: 2.6-6.6) 6 months after the end of ozone treatment (p = 0.008). The toxicity grade, according to the Common Terminology Criteria for Adverse Events (CTCAE v.5.0), improved in half of the patients. Conclusion: This report shows that most patients obtained clinically relevant and long-lasting improvement in chronic pain secondary to CIPN after treatment with ozone. These observed effects merit further research and support our ongoing randomized clinical trial.
Background: Medical ozone is more bactericidal, fungicidal, and virucidal than any other natural substance. Some studies proved that ozone infused into donated blood samples can kill viruses 100% of the time. Ozone, because of its special biologic properties, has theoretical and practical attributes to make it a potent hepatitis C virus (HCV) inactivator, which suggests an important role in the therapy for hepatitis C.
Aim: The study aim is to evaluate the role of ozone therapy in decreasing HCV ribonucleic acid (HCV RNA) load and its effect on the liver enzymes among patients with chronic hepatitis C.
Methods: This study included 52 patients with chronic hepatitis C (positive polymerase chain reaction [PCR] for HCV RNA and raised serum alanine transaminase [ALT] for more than 6 months). All patients were subjected to meticulous history taking and clinical examination. Complete blood count, liver function tests, and abdominal ultrasonography were requested for all patients. The ozone group included 40 patients who received major autohemotherapy, minor autohemotherapy, and rectal ozone insufflation. The other 12 patients (conventional group) received silymarin and/or multivitamins.
Results: There were significant improvements of most of the presenting symptoms of the patients in the ozone group in comparison to the conventional group. ALT and aspartate transaminase (AST) levels normalized in 57.5% and 60% in the ozone group, respectively, in comparison to 16.7% and 8% in the conventional group, respectively. Polymerase chain reaction (PCR) for HCV RNA was negative among 25% and 44.4% after 30 and 60 sessions of ozone therapy, respectively, in comparison to 8% among the conventional group.
Conclusions: Ozone therapy significantly improves the clinical symptoms associated with chronic hepatitis C and is associated with normalized ALT and AST levels among a significant number of patients. Ozone therapy is associated with disappearance of HCV RNA from the serum (-ve PCR for HCV RNA) in 25%-45% of patients with chronic hepatitis C.
Oxidative stress is suggested to have an important role in the development of complications in diabetes. Because ozone therapy can activate the antioxidant system, influencing the level of glycemia and some markers of endothelial cell damage, the aim of this study was to investigate the therapeutic efficacy of ozone in the treatment of patients with type 2 diabetes and diabetic feet and to compare ozone with antibiotic therapy. A randomized controlled clinical trial was performed with 101 patients divided into two groups: one (n = 52) treated with ozone (local and rectal insufflation of the gas) and the other (n = 49) treated with topical and systemic antibiotics. The efficacy of the treatments was evaluated by comparing the glycemic index, the area and perimeter of the lesions and biochemical markers of oxidative stress and endothelial damage in both groups after 20 days of treatment. Ozone treatment improved glycemic control, prevented oxidative stress, normalized levels of organic peroxides, and activated superoxide dismutase. The pharmacodynamic effect of ozone in the treatment of patients with neuroinfectious diabetic foot can be ascribed to the possibility of it being a superoxide scavenger. Superoxide is considered a link between the four metabolic routes associated with diabetes pathology and its complications. Furthermore, the healing of the lesions improved, resulting in fewer amputations than in control group. There were no side effects. These results show that medical ozone treatment could be an alternative therapy in the treatment of diabetes and its complications.
___________________________
What does that tell us?
That rectal ozone therapy is a panacea?
No, I don’t think so.
In my view, it tells us that strange journals publish a lot of dodgy research from strange research groups that use dodgy methodologies to confirm their odd belief that bogus treatments work for everything.
PS
I wonder which orifice Gwyneth will employ next to get the attention of the public.
Yesterday, it has been reported that Indian scientists found the mode of action of homeopathic remedies. This is the newspaper article:

And this seems to be the abstract of the actual paper:
Homeopathic medicines contain ultra-low concentrations of metal and compounds, and it is challenging to classify homeopathic potencies using modern characterization tools. This work presents a novel experimental tool for classifying various homeopathic medicines under a low-frequency generated electromagnetic (EM) fields. A custom-built primary coil is used for generating EM fields at different excitation frequencies. The potentized test samples were prepared at decimal dilution scale of Ferrum with α‑lactose monohydrate and exhibited significant and distinct induced EM responses in the second sensing coil. The measured responses decrease logarithmically due to reducing Ferrum concentration. The resolution improved in higher potencies from 0.03 µV at 300 Hz to 0.24 µV at 4.8 kHz. Different compounds of homeopathic medicines were also investigated to produce distinct induced EM characteristics. These results were correlated with Raman spectroscopy, impedance analyser, and FT-IR analysis. The experimental investigation confirmed the classification of potencies and the technique developed to detect ultra-low metallic concentrations.
I might be a bit slow on the uptake – but I don’t see how this investigation proves anything. Perhaps someone can explain it to me?
So-called alternative medicine (SCAM) is widely used in Arabia. One of the commonly used methods is camel urine alone or mixed with camel milk. Camel urine is a liquid by-product of camel metabolism. Urine from camels has been used as prophetic medicine for centuries, being a part of ancient Bedouin practices. Camel urine comes out as a concentrated, viscous syrup because the kidneys and intestines of a camel are very efficient at reabsorbing water. 
Camel urine is consumed and used for treating numerous ailments. Some employ it as a treatment for hair loss, for instance. The camel urine from a virgin camel is priced at twenty dollars per liter, with herders saying that it has curative powers.
A recent paper offers more information:
Camel is one of the important livestock species which plays a major role in the pastoral mode of life by fulfilling basic demands of livelihood. Traditionally, camel urine has been used in the treatment of human diseases. With regard to the health benefits of drinking the urine of camels, it has been proven by modern scientific researches. Camel urine has an unusual and unique biochemical composition that contributes to medicinal values. The chemical composition of camel urine showed the presence of purine bases, hypoxanthine, sodium, potassium, creatinine, urea, uric acid, and phosphates. The nano-particles in the camel’s urine can be used to fight cancer. Camel urine has antimicrobial activity against pathogenic bacteria. Its chemical and organic constituents have also inhibitory properties against fungal growth, human platelets, and parasitic diseases mainly fasciollosis in calves. The healthy status of the liver can be restored through ingestion of diet and minerals in camel urine. Camel urine is used by the camel owners and Bedouins as medicine in different ways. The Bedouin in the Arab desert used to mix camel urine with milk. Recently; the WHO has warned against drinking camel urine due to the modern attempt to limit Outbreaks of Respiratory Syndrome (MRS) in the Middle East. There is no scientific dosage for camel urine to be applied as medicine for different diseases and the ways of camel urine formulation and utilization for the care of patients varies from country to country. Therefore, the purposes of the present review describe the biochemical composition of camel urine will be scientifically extracted and formulated as a therapy rather than drinking raw urine and people’s health impact.
Researchers from the Medical Oncology Department, Comprehensive Cancer Center, King Fahad Medical City, Riyadh, Saudi Arabia wanted to determine whether camel urine shows promise in the treatment of cancer. The aim of their study was to observe cancer patients who insisted on using camel urine and to devise some clinically relevant recommendations.
The authors observed 20 cancer patients (15 male, 5 female) from September 2020 to January 2022 who insisted on using camel urine. They documented the demographics of each patient, the method of administering camel urine, the reasons for refusing conventional treatment, the period of follow-up, and the outcome and side effects.
All the patients had radiological investigations before and after finishing treatment with camel urine. All patients used a combination of camel urine and milk, and treatment ranged from a few days up to 6 months. The average amount of urine/milk consumed was 60 ml/day. No clinical benefit was observed and two patients developed brucellosis. Eleven patients changed their minds and eventually accepted conventional antineoplastic treatments but 7 were too weak to receive further treatment and died from their disease.
The authors concluded that camel urine had no clinical benefits in cancer patients, and may even have caused zoonotic infection. The promotion of camel urine as a traditional medicine should be stopped because there is no scientific evidence to support it.
I fear that, yet again, ‘ancient wisdom’ turns out to be just ‘old bullshit’.
I have grumbled about prevalence surveys in so-called alternative medicine (SCAM) before, I know. But, as the problem continues to get on my nerves – I estimate that there are about 10 times more surveys in SCAM than in any other field – allow me to do it again. The subject appeared on my screen in the form of a recent article from a minor, not Medline-listed journal. The paper is entitled:
Investigation of Complementary and Alternative Medicine Use in Turkish Patients with Epilepsy
This type of prevalence survey is typical of its genre and stands for hundreds – thousands even – like it. Its findings reveal a high prevalence of use. From that result, enthusiasts tend to draw stereotypical conclusions, namely that we need more research and that we ought to consider the integration of SCAM into routine care.
WHAT A WASTE OF TIME AND EFFORT!
Who really needs to know how many epilepsy patients in Turkey use SCAM?
Nobody!
You disagree?
Fine, then tell me: why Turkey and why epilepsy? If such information were important (and the methodology of the survey were perfect [which it hardly ever is]), then we surely need it for all diseases. How many different diseases are there? Let’s make it easy and say 1000. This means we need 1000 surveys to obtain a valuable picture of SCAM use in Turkey.
And if this sort of information is relevant in Turkey, we need to have it also for all other major countries. How many major countries exist? Let’s make it simple again and say 500. This means that we need 500 x 1000 or 500 000 surveys to generate a meaningful picture of SCAM use.
Since SCAM use changes quickly, we require these articles to be updated regularly; let’s say every 3 years. That means we require half a million surveys every 3 years.
What for?
What would it tell us?
What would we conclude from this enormous body of research?
Yes, of course, we would conclude that we need more research and we ought to consider the integration of SCAM into routine care!
My point is that if we truly need more research, why not get on with it? Why not finally forget about such useless surveys and do the science? Why not determine which SCAM works for what condition and at what risks? And, in case the findings turn out to be positive [but only then], let’s talk about integration into routine care. To put it even blunter:
The survey mania in SCAM prevents progress.
‘Agoro’ is a German (all texts are my translations from German) website that claims this:
“We specialize in alternative methods of treatment from the field of natural medicine. Our mission is to ensure that the ancient wisdom of our grandparents and ancestors is not forgotten.”
Unsurprisingly, this subject interests me. In particular, I was fascinated by an article entitled
Nux vomica Globuli in der Homöopathie
Nux Vomica in homeopathy
Nux vomica is (after arnica) amongst the most popular remedies in homeopathy. Therefore, we should all be keen to learn all about it.
Here is the translation of this article:
Nux vomica is one of the homeopathic remedies that you can get in all pharmacies. It can help you with various diseases, such as stomach pain. You can also use this homeopathic remedy for nausea and heartburn. You can buy it in the city pharmacies, but you can also make it easy for yourself and use the online pharmacy for globules. Here you will be well advised on the dosage of homeopathic remedies. Similarly, you can also contact the homeopath or naturopath for good advice.
Nux vomica is a remedy derived from the medicinal plant nux vomica. You can use the homeopathic remedy in the potencies D6 and D12. In some cases, it can be recommended to you also in C6, C12, or C30.
You can use the homeopathic remedy in many ways, including for constipation or exhaustion. You will find out which dosage you can take if you consult a professional. In this way, you will be recommended the appropriate potency to experience help from it.
It is crucial that you always seek advice before taking the remedy. As already mentioned, you can use several contact points for this. Whether it is the pharmacy, the naturopath, or the homeopath. In addition, there are many family doctors who now also use homeopathy and could recommend you the appropriate dosage. The consultation is important in any case because the homeopathy must be adapted to your complaints. Otherwise, the remedy will not work or will not work properly.
If you want to use the remedy for yourself, you always need patience. Homeopathic remedies need a little time to work, that is their only disadvantage. How long this always depends on the person and the remedy. Sometimes it takes only a few hours, sometimes a few days or weeks. You can also get advice on this.
Indications for nux vomica
Stomach and intestinal problems
You can use the remedy for you in case of abdominal pain, mild biliousness, and various stomach and intestinal problems. The remedy can also be of great help for nausea, flatulence, nausea, and constipation.
Headaches and migraines
The remedy Nux vomica can help you if you suffer from headaches that are located just above the eye. It can also help you with migraines. Even with a hangover, the remedy could help.
Moods
If you suffer from autumn depression or are often easily frustrated, you can use the remedy.
_______________________
Yes, I do get easily frustrated with texts like this!
But I doubt that nux vomica can help me with this or any other problem.
Some might say that doubting is not good enough, evidence is needed!
I agree but was unable to find sound evidence to show that homeopathic nux vomica was better than a placebo for any condition (in case any of our regular defenders of homeopathy know more, please let me know). On the contrary, I only found studies that suggested its ineffectiveness. Here is an example:
In a monocenter prospective randomized double-blind clinical trial the efficacy of homeopathic treatment was investigated on children with adenoid vegetations justifying an operation. Patients were treated with either homeopathic remedies such as Nux vomica D200, Okoubaka D3, Tuberculinum D200, Barium jodatum D4 and Barium jodatum D6 or with placebo. The duration of the study for each patient was 3 months. Examination of the ears using a microscope, rhinoscopy, stomatoscopy and pharyngoscopy, as well as tympanometry and audiometry were performed after 4, 8 and 12 weeks. Out of a total of 97 children studied between the ages of 4 to 10 years 82 could be analyzed. At the end of the study no operation was required in 70.7% of the placebo-treated children and in 78.1% of the children treated with homeopathic preparations. These results show no statistical significance.
So, where does that leave us in relation to the “ancient wisdom of our grandparents and ancestors“? I fear, that this story shows yet again that, when it comes to homeopathy, the scrutiny of ancient wisdom quickly turns it into old bullshit.
Lower respiratory tract infections (LRTIs) in early childhood are known to influence lung development and lifelong lung health, but their link to premature adult death from respiratory disease is unclear. This analysis aimed to estimate the association between early childhood LRTI and the risk and burden of premature adult mortality from respiratory disease.
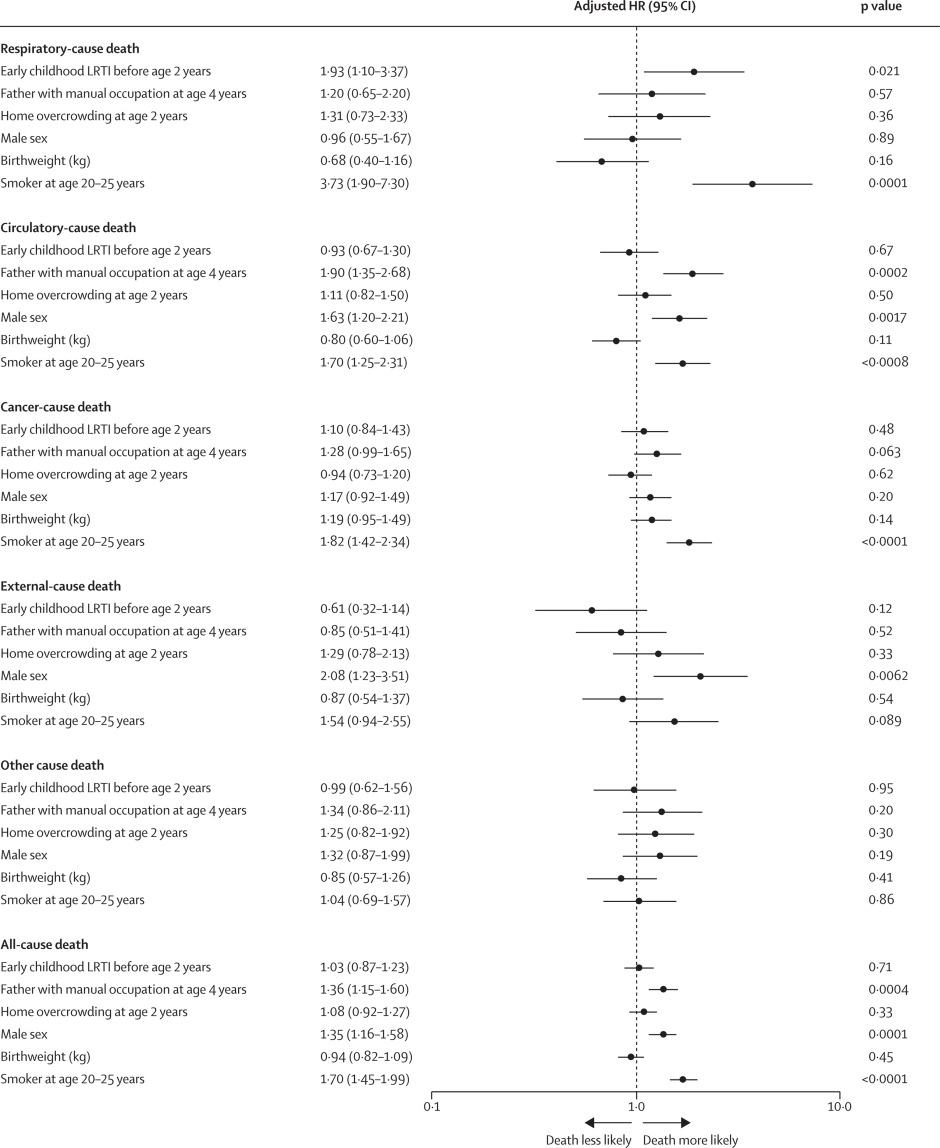
This longitudinal observational cohort study used data collected prospectively by the Medical Research Council National Survey of Health and Development in a nationally representative cohort recruited at birth in March 1946, in England, Scotland, and Wales. It evaluated the association between LRTI during early childhood (age <2 years) and death from respiratory disease from age 26 through 73 years. Early childhood LRTI occurrence was reported by parents or guardians. Cause and date of death were obtained from the National Health Service Central Register. Hazard ratios (HRs) and population attributable risk associated with early childhood LRTI were estimated using competing risks Cox proportional hazards models, adjusted for childhood socioeconomic position, childhood home overcrowding, birthweight, sex, and smoking at age 20–25 years. The researchers compared mortality within the cohort studied with national mortality patterns and estimated corresponding excess deaths occurring nationally during the study period.
5362 participants were enrolled in March, 1946, and 4032 (75%) continued participating in the study at age 20–25 years. 443 participants with incomplete data on early childhood (368 [9%] of 4032), smoking (57 [1%]), or mortality (18 [<1%]) were excluded. 3589 participants aged 26 years (1840 [51%] male and 1749 [49%] female) were included in the survival analyses from 1972 onwards. The maximum follow-up time was 47·9 years. Among 3589 participants, 913 (25%) who had an LRTI during early childhood were at greater risk of dying from respiratory disease by age 73 years than those with no LRTI during early childhood (HR 1·93, 95% CI 1·10–3·37; p=0·021), after adjustment for childhood socioeconomic position, childhood home overcrowding, birthweight, sex, and adult smoking. This finding corresponded to a population attributable risk of 20·4% (95% CI 3·8–29·8) and 179 188 (95% CI 33 806–261 519) excess deaths across England and Wales between 1972 and 2019.
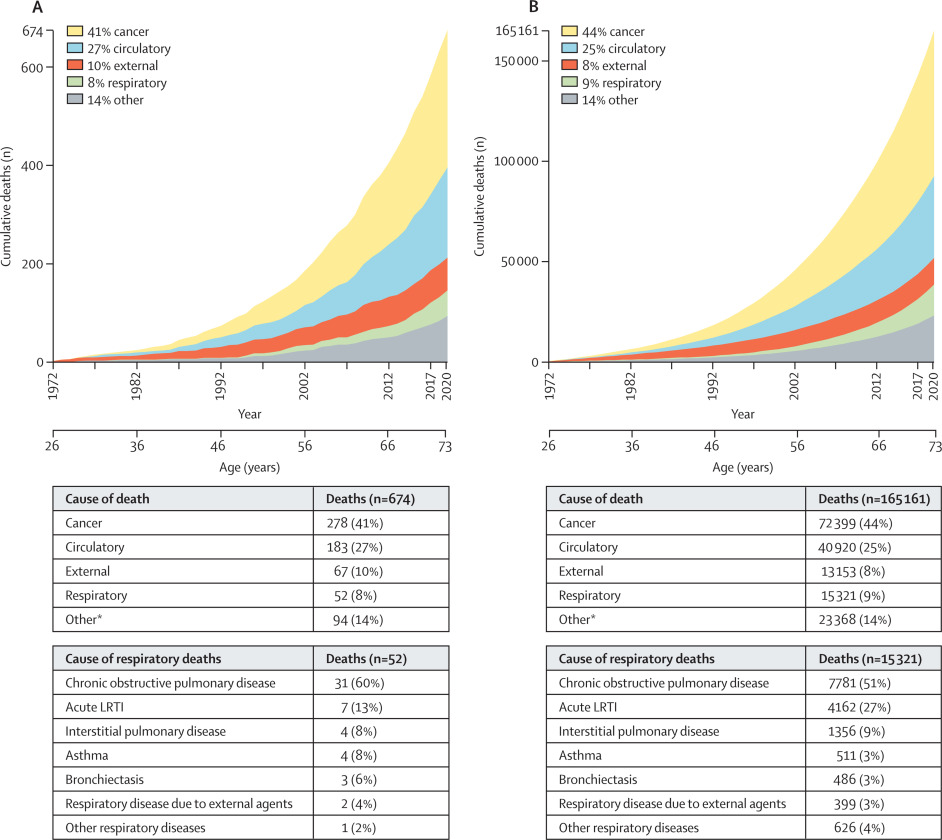
The authors concluded that, in this perspective, life-spanning, nationally representative cohort study, LRTI during early childhood was associated with almost a two times increased risk of premature adult death from respiratory disease, and accounted for one-fifth of these deaths.
What has that got to do with so-called alternative medicine?
Nothing!
Yet, I feel that this study is so remarkable that I need to report on it nonetheless.
What do the findings indicate?
I am not sure. Perhaps they confirm that our genetic makeup is hugely important in determining our health. Thus even the earliest signs of weakness can provide an indication of what might happen in later life.
Whatever the meaning, I find this study fascinating and hope you agree.
I had all but forgotten about these trials until a comment by ‘Mojo’ (thanks Mojo!) reminded me of this article in the JRSM by M.E. Dean. It reviewed these early trials of homeopathy back in 2006. Here are the crucial excerpts:
The homeopath in both trials was a Dr Herrmann, who received a 1-year contract in February 1829 to test homeopathy with the Russian military.3 The first study took place at the Military Hospital in the market town of Tulzyn, in the province of Podolya, Ukraine.4 At the end of 3 months, 164 patients had been admitted, 123 pronounced cured, 18 were convalescing, 18 still sick, and six had died. The homeopathic ward received many gravely ill patients, and the small number of deaths was shown at autopsy to be due to advanced gross pathologies. The results were interesting enough for the Russian government to order Herrmann to the Regional Military Hospital at St Petersburg to take part in a larger trial, supervised by a Dr Gigler. Patients were admitted to an experimental homeopathic ward, for treatment by Herrmann, and comparisons were made with the success rate in the allopathic wards, as happened in Tulzyn. The novelty was Gigler’s inclusion of a ‘no treatment’ ward where patients were not subject to conventional drugging and bleeding, or homeopathic dosing. The untreated patients benefited from baths, tisanes, good nutrition and rest, but also:
‘During this period, the patients were additionally subjects of an innocent deception. In order to deflect the suspicion that they were not being given any medicine, they were prescribed pills made of white breadcrumbs or cocoa, lactose powder or salep infusions, as happened in the homeopathic ward.’3 (page 415)
The ‘no treatment’ patients, in fact, did better than those in both the allopathic and homeopathic wards. The trial had important implications not just for homeopathy but also for the excessive allopathic drugging and bleeding that was prevalent. As a result of the report, homeopathy was banned in Russia for some years, although allopathy was not.
… A well-known opponent of homeopathy, Carl von Seidlitz, witnessed the St Petersburg trial and wrote a hostile report.5 He then conducted a homeopathic drug test in February 1834 at the Naval Hospital in the same city in which healthy nursing staff received homeopathically-prepared vegetable charcoal or placebo in a single-blind cross-over design.6 Within a few months, Armand Trousseau and colleagues were giving placebo pills to their Parisian patients; perhaps in the belief that they were testing homeopathy, and fully aware they were testing a placebo response.7,8 A placebo-controlled homeopathic proving took place in Nuremberg in 1835 and even included a primitive form of random assignment—identical vials of active and placebo treatment were shuffled before distribution.9 Around the same time in England, Sir John Forbes treated a diarrhoea outbreak after dividing his patients into two groups: half received allopathic ‘treatment as usual’ and half got bread pills. He saw no difference in outcome, and when he reported the experiment in 1846 he added that the placebos could just as easily have been homeopathic tablets.10 In 1861, a French doctor gave placebo pills to patients with neurotic symptoms, and his attitude is representative: he called the placebo ‘orthodox homeopathy’, because, as he said, ‘Bread pills or globules of Aconitum 30c or 40c amount to the same thing’.11
References:
Alzheimer’s is a devastating disease against which conventional healthcare has little to offer. No wonder, therefore, that so-called alternative medicine (SCAM) claims to have a wide range of effective treatments. But how good are they really? The present review aimed to explore the role of SCAM in the treatment of Alzheimer’s disease (AD).
Literature searches were conducted using Ovid MEDLINE, CINAHL, Cochrane, and PubMed databases and reference lists up to November 30, 2021. Only randomized clinical trials were included and appraised using the National Institute of Health framework. Data analysis showed that herbs like Gingko Biloba, Melissa Officinalis, Salvia officinalis, Ginseng, and saffron alone or in combination with curcumin, a low-fat diet, NuAD-Trail, and soy lecithin showed significant positive effects on AD. Moreover, the combination of natural and pharmaceuticals has far better effects than only allopathic treatment. The authors concluded that different herbal remedies in combination with FDA approved drugs are effective and more promising in the treatment of AD.
To these findings we need to add a study that is too recent to have been included in the review:
The aim of the randomized clinical trial (RCT) was to investigate the effects of fenugreek seed extract on memory, depression, quality of life, blood pressure, and serum malondialdehyde (MDA) and total antioxidant capacity (TAC) levels in adult AD patients. The study participants included 82 AD patients with mild-to-moderate memory deficits. Patients in the intervention group received 5 cc of fenugreek seed extract for 4 months and subjects in the control group received a placebo. Memory, depression, quality of life, and BP levels, as well as serum MDA and TAC, were assessed before and after the intervention.
There was a significant increase in serum levels of TAC (p < 0.001) and a reduction in serum MDA status (p < 0.001) after 4 months of fenugreek seed extract supplementation. In addition, increasing levels of memory (p < 0.001) and quality of life (p < 0.001), as well as reduction of depression (p = 0.002), systolic BP (p < 0.001), and diastolic BP (p < 0.001) levels were detected in the intervention group compared with baseline.
The authors concluded that Fenugreek seed extract supplementation in AD patients shows promising positive effects on memory, quality of life, BP, and selective oxidative indices levels.
So, there is hope! Some of the evidence is promising but far from convincing. What we need – obviously – is more and better research.
Kourtney Kardashian believes that vaginal health is an important but not sufficiently talked about part of women’s well-being. So, why not make a bit of money on the subject? A recent article explains in more detail:
The reality TV star recently launched a vitamin sweet called Lemme Purr to boost the health of your vagina. On her Instagram channel, she says these gummies use pineapple, vitamin C, and probiotics to target vaginal health and pH levels that “support freshness and taste”.
Kourtney continues with the selling words “Give your vagina the sweet treat it deserves (and turn it into a sweet treat)”. One of the claims she makes is that the vitamin sweet supports a healthy vaginal microflora. As a researcher specialising in the role of vaginal microflora for women’s health, I was curious and wanted to find out which active ingredients this claim is based on.
Lemme Purr contains pineapple extract (probably for its taste), vitamin C (not really needed if you have a balanced diet), and a clinically tested probiotic (Bacillus coagulans). According to the product description, the probiotic has been shown in clinical studies to support vaginal health, freshness, and odour. This surprised me – I should know about these studies and effects as this is my primary research field.
A healthy vaginal microflora is composed of lactobacilli that keep the pH low and protect us from infections. My colleagues and I never identified Bacillus coagulans as being important for the health of vaginas, even though we have analysed thousands of samples during recent years. From other research groups and our own results, we know that Lactobacillus crispatus is the species that is associated with vaginal health and female fertility.
As I may have missed something important, I immediately checked what has been published on that probiotic in scientific journals. I found one systematic review and meta-analysis (a type of analysis where many individual studies are taken together) that mentions Bacillus coagulans. Apparently, it may improve stool frequency and symptoms of constipation, although the authors conclude that more research is needed.
On the topic of women’s vaginal health, I could only find a single study. There, 70 women with vaginal discomfort reported symptom relief after direct vaginal administration of the probiotic. There is nothing published on the oral administration of the probiotic that could support the claims made by Kourtney.
__________________________
I was not entirely sure where women are supposed to put Kourtney’s gummies. So, I watched a video where Kourtney applies one of these items herself. I am very pleased to report that, in the video, she put one in her mouth!
After this relief, I ran a few Medline searches to get an impression of what the evidence tells us. In contrast to the author of the above article, I found plenty of literature on the subject and quite a few clinical trials. So, maybe Kourtney is on to something?
Somehow, I doubt it. I did not find a study with her product. Call me a skeptic, but I do get the feeling after looking at Kourtney’s website that she is much more interested in money than vaginal health.
This review investigated the characteristics, hotspots, and frontiers of global scientific output in acupuncture research for chronic pain over the past decade. the authors retrieved publications on acupuncture for chronic pain published from 2011 to 2022 from the Science Citation Index Expanded (SCI-expanded) of the Web of Science Core Collection (WoSCC). The co-occurrence relationships of journals/countries/institutions/authors/keywords were performed using VOSviewer V6.1.2, and CiteSpace V1.6.18 analyzed the clustering and burst analysis of keywords and co-cited references.

A total of 1616 articles were retrieved. The results showed that:
- the number of annual publications on acupuncture for chronic pain has increased over time;
- the main types of literature are original articles (1091 articles, 67.5 %) and review articles (351 articles, 21.7 %);
- China had the most publications (598 articles, 37 %), with Beijing University of Traditional Chinese Medicine (93 articles, 5.8 %);
- Evidence-based Complementary and Alternative Medicine ranked first (169 articles, 10.45 %) as the most prolific affiliate and journal, respectively;
- Liang FR was the most productive author (43 articles);
- the article published by Vickers Andrew J in 2012 had the highest number of citations (625 citations).

Recently, “acupuncture” and “pain” appeared most frequently. The hot topics in acupuncture for chronic pain based on keywords clustering analysis were experimental design, hot diseases, interventions, and mechanism studies. According to burst analysis, the main research frontiers were functional connectivity (FC), depression, and risk.
The authors concluded that this study provides an in-depth perspective on acupuncture for chronic pain studies, revealing pivotal points, research hotspots, and research trends. Valuable ideas are provided for future research activities.
I might disagree with the authors’ conclusion and would argue that they have demonstrated that:
- the acupuncture literature is dominated by China, which is concerning because we know that 1) these studies are of poor quality, 2) never report negative findings, and 3) are often fabricated;
- the articles tend to be published in journals that are more than a little suspect.
As we have seen recently, the reliable evidence that acupuncture remains effective is wafer-thin. Therefore, I feel that we are currently being misled by a flurry of rubbish publications that have one main aim: to distract from the fact that acupuncture might be nonsense.