pseudo-science
Guest post by Björn Geir
I have tried to find a form or type of quackery that can be confirmed to have died out and is no longer practised. Once I thought I had found one, but it turns out that phrenology is still “a thing” and is being practised by a few eccentrics.
I am almost convinced by now that any quackery or SCAM, as Professor Ernst has proposed to call it, never dies. Once someone has invented a SCAM, it will live on forever, like the proverbial zombie, neither dead nor properly alive and useful. Even bloodletting, the archetypical reject from the practice of medicine, is still being practised in some corners of this world. Google “Wet cupping” or “Hijama” if you don’t believe me.
The world will have to live with health-related scam and swindle but its popularity can and should be suppressed and held to an acceptable low. If truth and science are promoted and SCAM is vigilantly and constantly opposed, then public trust in it can be held back and even reversed as now has been shown in Norway.
My somewhat abridged translation of an article published on June 30th on the Norwegian state broadcasting services website.
————
Norwegians have become much more sceptical towards natural medicine
Fifteen years ago, most Norwegians had faith in natural medicine. Not anymore.
– This is dramatic. A total reversal of opinion, says John Spilling of Ipsos, a company that performs an annual survey of public opinion in Norway. About 3500 people have been interviewed every year since 1985.
The survey, called Norwegian Monitor, has shown that the alternative industry had its heyday in the 80´s and 90´s, at least according to the Norwegian population’s confidence in natural medicine.
On average, eight out of ten thought this kind of therapy and naturopaths could help when ordinary doctors had given up.
But after the turn of the millennium, something started to happen.
The confidence plummeted.

A screenshot from the article showing the representation of the annual Norwegian Monitor survey results for the statement: Naturopaths and natural medicine can often help when ordinary doctors and medicine fall short.
The results are represented as follows:
Black – Impossible to answer
Grey – No answer
Dark red – Totally disagree
Light red – Partially disagree
Dark blue – Partially agree
Light blue – Totally agree
The graph in the article is interactive so you can find the individual rates by hovering over the bars in the article online.
This year only three out of ten fully or partially agree that natural medicine and naturopaths can help. Mr. Spilling is surprised by the magnitude of change, which also has been steadily declining instead of the usual ups and downs seen in so many other areas.
– I see almost no parallels, he says.
The patients stopped coming
The article interviews Ms. Hilde Moldestad. A homeopath since many decades, now retired and leads the Norwegian Homeopathic Patient Association.
Ms. Moldestad marked the decline already while practising.
– The patients stopped coming, because the trends were such that no one was to believe that there was anything good about homeopathy.
She also noted a strongly declining interest within the patient association.
– There are less and less members. People are not so interested in being team members anymore, they want it free online.
Ms. Moldestad is determined that homeopathy works.
– The irony is that the more research that shows that homeopathy works, the stronger the opposition to using the method.
The [Norwegian] National Research Center for Alternative Medicine writes that there is no solid evidence that homeopathic medicines have an effect. And both the Norwegian Medicines Agency and the Norwegian Pharmacists’ Association believe that in practice the pills only contain water and sugar.
– But we are up in a paradigm shift. The damage that has been inflicted on humanity during the period in which school medicine has been allowed to dominate, can no longer be undermined, says Ms. Moldestad in the patient association.The article then interviews Mr. Gunnar Tjomlid, an active Norwegian sceptic who talks about some local background stories of local interest and speculates that perhaps this change correlates with the introduction and distribution of internet access in Norway.
Less use
It is not only the Norwegian Monitor survey that shows a decline for the alternative industry. Every two years, the National Research Center for Alternative Medicine (Nafkam) conducts a survey on, among other things, how often Norwegians visit alternative therapists.
– In 2012, you had just under 40 percent who had been to an alternative therapist. And in December 2020, it was 22 percent. So, there has been a declining trend, says Mr. Ola Lillenes, information director at Nafkam.
At the same time, self-treatment, especially with self-help techniques, has increased.
– Healing and homeopathy are probably among those who have fallen the most through these years.
Education and emotions
Jarle Botnen runs the Bø Institute of Natural Medicine in Telemark. In addition, he is part of the steering group in the association of alternative treatment organizations. Over 1000 therapists are affiliated with this organisation which is named Saborg.
– There is a noticeable decline, that is exactly correct, says Botnen.
He has several theories as to why Norwegians have become more sceptical of natural medicine.
Norwegians have received more education and have less trust in their own feelings.
People are used to simple solutions, such as over-the-counter painkillers. They do not treat the cause of the ailments, which takes more time.
It is difficult to distinguish charlatans from the serious [alternative practitioners]. The industry has also not managed to cooperate well enough, according to Botnen.
The pharmaceutical industry has been lobbying to get more of the market for alternative medicine.
The attitude in the media has changed from being positive to natural medicine to often the opposite.
Small brown glass bottles with homeopathic pills lie in a drawer in a pharmacy.
Sales of homeopathic medicines have declined at the same time as Norwegians have become more sceptical of natural medicine.
– We often hear remarks such as “we trust the authorities”, “the authorities have approved the preparation or treatment”. This is reflected in the consumption of chemical and synthetic medicine, which has increased somewhat formidably during this period, Botnen believes.
John Spilling in Ipsos says it is true that people have great confidence in the public sector. Confidence in hospitals and elderly care has also increased, while the alternative industry has had the opposite development.
– Most of Norway’s population does not trust this type of product. I can only understand that the situation of this industry is very different than in 2001.
End of article————-
These are indeed positive and convincing results. I suspect a similar trend has been happening in most other populations? It would be very interesting to know if a similar trend has been observed elsewhere.
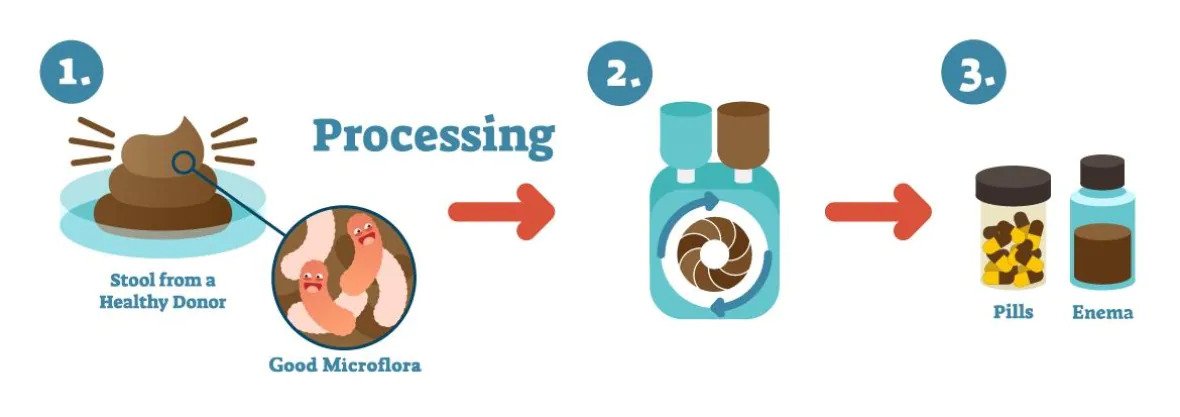
I have previously reported that a Canadian naturopath, Jason Klop, is under investigation for selling fecal Microbiota transplants to treat autistic children. Now, there is a new twist in this story.

On Twitter, J.N. Stea summarized it nicely:
This naturopath is fighting a judge so that he can charge parents about $15,000 to give his nephew’s poop to children as a treatment for autism. His lawyer argues that he should be allowed to since naturopathy isn’t scientific anyway.
Klop’s lawyer defends the naturopath against an investigation into his business of selling fecal microbiota transplants to families of autistic children. The College of Naturopathic Physicians (CoN) had banned Klop for selling, advertising, and manufacturing pills made from human feces claiming that Klop has been engaging in conduct not acceptable for a naturopathic physician. Klop’s lawyer, Jason Gratl, argued this was difficult to prove in a field that has a few restrictions and some ambiguous boundaries.
“What does it take to be a naturopath and do something that is not appropriate in a field so wide-ranging and open to interpretation?” the lawyer, Gratl, asked the court suggesting that the lack of scientific evidence supporting the use of fecal Microbiota Transplants (FMT) to treat autism is not necessarily relevant in this instance.
“Naturopaths can rely on science in certain aspects, but they are not bound to science,” Gratl said. He explained that naturopathic practices could be based on anecdotes and historical knowledge. Later, he pointed out that the field also includes homeopathy, which, some believe, involves magical thinking. It is definitely not scientific in its core.” After describing the case as a “tragedy”, Gratl called the allegations against his client “entirely unverfounded and scurrilous.”
I suspect it is nothing new to most readers, yet I find it gratifying to hear from a lawyer that naturopathy
- is not science,
- relies on anecdote instead of evidence,
- and involves magical thinking.
I do think, however, that despite all this, naturopaths should not be allowed to do any odd nonsense that comes to their minds and fills their bank accounts quickly.
Guest post by Ken McLeod
Believe it or not, there are practitioners of a health system with little or no evidence of efficacy and safety who are registered with the Australian Health Practitioner Registration Agency. That is, so-called Traditional Chinese Medicine, whose practitioners are registered alongside evidence-based practitioners such as doctors, nurses, pharmacists, and dentists.
Governments who framed the relevant legislation evidently hoped that registration would enable the public to have confidence that they would be treated with evidence-based medicine. Such confidence is misplaced, as has been shown in The Skeptic and elsewhere many times.
Here’s another example of the failure of the health practitioner registration system.
Jamie Lloyd Allan is registered with AHPRA with the Chinese Medical Registration Number CMR0002096457, with no endorsements. He practices at his clinic in eastern Sydney. He advertises at his website meridianremedies.com.au.
And some of his claims are deeply worrying. Allan claims that he uses “Chinese Herbal medicine & Acupuncture in conjunction with testing and removal of accumulated toxins and heavy metals, developing comprehensive individualised herbal antimicrobial and detoxification protocols.”
He claims that “toxins and heavy metals … enter our bodies, disrupt normal healthy cell behaviour, impair our immune system, often contribute and sometimes cause many different types of illnesses and health conditions.”
His claims are designed to generate unfounded worries in people, offering a smorgasbord of claims how he can help people learn [the words and spelling are his]:
• how mercury from common amalgam fillings can be passed from mother to child to grandchild and why preconception detoxification is important;
• how to assess a dentist to know your [sic] getting the best and safest care during amalgam removal;
• about mercury/autism connection, heavy metal accumulation and neurological diseases such as Alzheimer’s, Parkinson’s and Dementia;
• more about mercury, aluminium, cadmium and lead toxicity;
• how heavy metal accumulation acts as an antenna for electromagnetic radiation from devices such as wifi, cell phone, cordless phones, thus focusing the frequencies on the areas where the metals are stored, causing changes in the proteins and even DNA;
• the science behind electromagnetic radiation and how it affects human cells;
• Glyphosate toxicity, and how many of us have it and how it affects our health, and lots more.
Allan goes into the alleged toxicity of mercury amalgam fillings further at his blog. I should not have to say it, but his claims are baseless and have been debunked many times. The US Food and Drug Administration has said that existing evidence shows that dental amalgam is not harmful to the general population (tinyurl.com/589mbrr6). And as Scientific American said “Mercury and Autism: Enough Already! The science shows that they have nothing to do with each other and never have.” (tinyurl.com/mwwdxxak)
Allan also writes extensively on “EMF Sensitivity Wi-Fi and Cell Phone radiation – Heavy Metals and EMF Sensitivity and Autism” – he claims “Autism rates double every 5 years and the only thing that parallels that in our environment is the increase of man made Electro magnetic Radiation and fields largely in the high frequencies from cell phone Wi-Fi, smart meters and other Electro magnetic devices.’ This is unconscionable; scaring potential clients with this, while conveniently forgetting that correlation does not mean causation.
Allan also offers the following techniques as a “Detox for autism”:
• Sauna or heat therapy (far infrared is best) Cold shower straight after to close pores and wash of toxins
• Clay plasters, Clay on scars, then shower
• Ionic Foot Cleanses, Detox baths, Takara foot Pads, or raw white potato strapped on soles of feet
• Fibre + Enemas or colonics, slippery elm, keep bowls [sic] moving
• Liver gall bladder flush with lemon oil
• Exercise, dry skin brush
• Chi Machine for lymph drainage and movement to parasympathetic dominance
• Olive or other healthy oils for swish and spit
• Genetic, vitamin, mineral testing to guide your diet and supplements
• Western and Chinese Herbs to detox bowls [sic], liver, kidney, lymph
• Homeopathic drops & plenty of water orally
• Laser Energetic detox
• Ozonized bath, Epson salt bath
• Enema for detox reactions in kids
• Stronger detox agents DMPS, DMSA, EDTA can be used in case of high-level toxicity. For children, the use of the above mention techniques over DMPS, DMSA and EDTA is preferred first.
“Raw white potato strapped on soles of feet”!! Come on! This is lunacy. And enemas for children? And what qualifications does Allan hold to diagnose and administer these dangerous pharmaceuticals?
Luckily, Allan offers the perfect scanner to diagnose what’s wrong with you, the Oligoscan.
As described, “This a [sic] spectrographic-based test. Every element on the periodic table has its own unique absorption spectra, meaning that different elements absorb certain wavelengths of light, and reflect others. The spectra of lead will be different from that of mercury, or calcium, or any other element. The Oligoscan shines a laser on different points on the hand, and based off of [sic] which wavelengths of light are absorbed or reflected back, the levels of different metals and minerals in the cells of your hand can be determined. This is similar to how astronomers can analyze the wavelengths of light emitted by distant stars to determine their chemical make-up.
“The Oligoscan has the advantage of testing the levels of metals that are actually in your cells, not what you are able to excrete. It tests the heavy metal load of the tissues. This is important because heavy metals have a affinity [sic] for tissues and are often store [sic] there and not in the blood. It can also measure aluminium, which most other tests will miss. Oligoscan results tend to correlate with other accurate tests.”
A search of the TGA’s register of therapeutic goods did not find the Oligoscan listed.
Clearly, Allan is engaged in a process of scaring potential clients with misinformation, then offering diagnostic and treatment processes that are deceptive, ineffective and dangerous, and not listed with the TGA; for all of which he is not qualified.
COMPLAINT PROCESS
A complaint was sent to the NSW Health Care Complaints Commission describing the above issues. (In NSW and Queensland, complaints concerning health care practitioners, registered and unregistered, are lodged with the relevant State authorities, the HCCC and OHO respectively.) We added that “This should not be treated as merely a case of misleading advertising; Allan is clearly endangering the public, so I recommend a thorough audit of his practice, and when my allegations are found to be proven, suitable disciplinary action taken and entered on the AHPRA register.”
The HCCC responded saying “Following consultation with the Chinese Medicine Council of New South Wales, it was decided to refer this matter to the Australian Health Practitioner
Regulation Agency (AHPRA) as AHPRA is the designated agency to manage concerns about advertising. We did not identify any other issues that would require further action by the Commission.” (We approached the Chinese Medicine Council of NSW – their response is quoted in the sidebar.)
The HCCC continued: “The Commission obtained a written response from Mr Allan. In his response to the Commission, Mr Allan stated that he had no record of providing any care and treatment to you.
“Mr Allan acknowledged that his website may have created a misunderstanding about what actual treatments are offered at his clinic, and what was on his website for educational purposes only.
“Mr Allan noted that he has never owned an Oligoscan or used it at his clinic, he has therefore removed that information from his website.
“Mr Allan confirmed that he does not offer the techniques under the heading ‘detox for autism’ at his clinic, the information was for educational purposes only, and he has now removed this information from his website.
“Further, Mr Allan has confirmed that he has removed the information on his website about Glyphosate Toxicity, Toxicity of Mercury Amalgam fillings, Nutrition for Autism, and all avenues of receiving mercury toxicity.
“Mr Allan also stated that he has since edited the information on EMF Sensitivity Wi-Fi and Cell Phone radiation – Heavy Metals and EMF Sensitivity Autism, as well as editing the information contained on the home and about pages of his website.
“Mr Allan stated that he has left the resources section with all the raw studies, and some information contained in other sections, as he feels that they are of use for anybody wanting to learn more about this specialised area.”
So, in spite of the detailed evidence and a call for a thorough audit of his practice, this was treated as merely a case of misleading advertising. This is standard operating procedure; the regulatory authorities cannot get over the divide between advertising and clinical practice. This has been shown in the hundreds of complaints sent to regulators; misleading advertising of dangerous practices and misinformation is simply treated as an advertising issue. The regulators cannot accept that if a practitioner advertises a therapy then they are more than likely using those therapies and, when those therapies have been found to be ineffective, they are engaging in practice in their clinics that deserves more than the dismissive response we received.
The public deserve much better than that.
Note: All of the quotes above were from Allan’s website until he removed them. The relevant pages have, nonetheless, can be accessed via the WayBack Machine, and can be supplied if required.
The Chinese Medicine Council’s position
The Chinese Medical Council were referred to the issues in the main article and were asked the following questions:
• Is the advice and those therapies [offered by Allan] of any concern to the Council?
• Should the complaint to the NSW Health Care Complaints Commission have led to an audit of his practice and when the allegations are proven, should there have been disciplinary action?
A spokesperson for the Chinese Medicine Council of NSW replied: “The Chinese Medicine Council of NSW (the Council) works in collaboration with the NSW Health Care Complaints Commission (HCCC) to receive and manage complaints about registered practitioners in
NSW. Our paramount legal obligation is to protect the public. We deal with practitioners whose conduct, performance or health may represent a risk to the public or is not in the public interest.
“We do this by assessing complaints, promoting compliance with professional standards and delivering programs to ensure practitioners provide safe care to the public and their patients. We do not have the legal power to discipline a NSW practitioner or to deregister them.
“By law, the Council cannot provide information about an individual practitioner. Only information that is publicly available can be disclosed, such as information recorded on the national register of practitioners which is maintained by the Australian Health Practitioner Regulation Agency (AHPRA), or publication of the outcomes of NCAT [New South Wales Civil and Administrative Tribunal] proceedings.
“Changes to a registered health practitioner’s registration status, such as the imposition of conditions or suspension, are published on the AHPRA online public register.
“The Council will not be making any further public comments at this time.
So, the Chinese Medicine Council have taken no action to protect the public and made no real comment. At least they have promised “Only information that is publicly available can be disclosed”, a statement of breathless inanity.
*‘first published in the Australian Skeptic magazine of June 2022.
I only now learned of the death of one of the most bizarre proponents that the cult of homeopathy has ever produced in its 200-year history. From his official obituary, one would not suspect much weirdness:
John R. Benneth passed away Nov. 9, 2021 in Chico, Calif., after a long battle with Parkinson’s disease.

John shepherded the Pixieland Theatre in Lincoln City for many years, writing, directing, and acting in plays that kept audiences coming back. He appeared often on stage in Portland and became a familiar face in local and national commercials. In the mid-1980s he was the host, writer, and creative force behind The Portland Underground, a weekly, live, late-night local access show. He gave many local actors a chance to stretch their improv talents on that and his earlier show, Mysterious Planet. His was the voice of both Portland Talk Radio’s controversial Jack Hammer, and Kandu the Mystic. He later performed regularly as Mark Twain in Virginia City, Nev., and on cruises on Lake Tahoe. John started working as a private investigator in Portland in 1978, and in 1982, he founded the National Missing Children’s Locate Center, helping parents to find their children across the U.S. He later became internationally known for his research into and advocacy for Homeopathic Medicine and was invited to present a treatise on the subject at London’s Oxford University in 2010.
John was a member of both Hawthorne and Washington Masonic lodges and the Scottish Rite of Portland.
He was preceded in death by his parents, John and Bettiana Benneth; and by his wife, Catherine Benneth. He is survived by his brother, David; and his four sons, Horatio, Merlin, Cyrano and Evan.
The ‘Bolen report’ offers a little more, albeit weirdly unreliable information:
John Benneth, PG Hom.- London (Hons) is the renowned discoverer of the link between Homeopathy and Conventional Ionic Chemistry.
The first to accept a notorious challenge to Homeopathy, he forced the James Randi Educational Foundation (JREF), in 1999, to back down from a spurious offer to award $1,000,000 for a test identifying homeopathic solutes from their liquid aqueous vehicles.
In 2010, by invitation of Nobel laureate physicist Brian Josephson at Cambridge’s Cavendish Laboratory, he presented the Supramolecular Chemistry of the Homeopathic Remedy revealing structural changes and the physics of hydrolysis and molecular self assembling chain reactions.
He is the author of Ebola Prophylaxis and Cure detailing the use of FDA approved homeopathic pharmaceuticals in the treatment of hemorrhagic fevers, presented in advance of the reported successful use of homeopathic remedies to cure Ebola.
He is a proponent for the use of homeopathic pharmaceuticals to cure sepsis and other dire conditions for conventional use in hospital emergency and intensive care, and the Ionic Vaccine for the safe and effective non-molecular prevention of epidemic diseases.
To estimate the true extent of Benneth’s eccentricity, we need to read some of the posts by John himself johnbenneth.wordpress.com. Alternatively, we might access some of his appearances on youtube, quackometer, or even just a post I published several years ago.
I am sad that John is gone. I always thought he was mad like a hatter, but he had me in stitches whenever our paths crossed.
It seems that no ancient treatment is daft enough for some researchers of so-called alternative medicine (SCAM) to not pick it up. Even bloodletting is back, it seems!
The aim of this study was to investigate the effects of therapeutic phlebotomy on ambulatory blood pressure in patients with grade 1 hypertension. In this randomized-controlled intervention study, patients with unmedicated hypertension grade 1 were randomized into an intervention group (phlebotomy group; 500 mL bloodletting at baseline and after 6 weeks) and a control group (waiting list) and followed up for 8 weeks. The primary endpoint was the 24-h ambulatory mean arterial pressure between the intervention and control groups after 8 weeks. Secondary outcome parameters included ambulatory/resting systolic/diastolic blood pressure, heart rate, and selected laboratory parameters (e.g., hemoglobin, hematocrit, erythrocytes, and ferritin). Resting systolic/diastolic blood pressure/heart rate and blood count were also assessed at 6 weeks before the second phlebotomy to ensure safety. A per-protocol analysis was performed.
Fifty-three hypertension participants (56.7 ± 10.5 years) were included in the analysis (n = 25 intervention group, n = 28 control group). The ambulatory measured mean arterial pressure decreased by -1.12 ± 5.16 mmHg in the intervention group and increased by 0.43 ± 3.82 mmHg in the control group (between-group difference: -1.55 ± 4.46, p = 0.22). Hemoglobin, hematocrit, erythrocytes, and ferritin showed more pronounced reductions in the intervention group in comparison with the control group, with significant between-group differences. Subgroup analysis showed trends regarding the effects on different groups classified by serum ferritin concentration, body mass index, age, and sex. Two adverse events (AEs) (anemia and dizziness) occurred in association with the phlebotomy, but no serious AEs.
The authors concluded that therapeutic phlebotomy resulted in only minimal reductions of 24-h ambulatory blood pressure measurement values in patients with unmedicated grade 1 hypertension. Further high-quality clinical studies are warranted, as this finding contradicts the results of other studies.
This paper requires a few short comments:
- The effect on blood pressure was not ‘minimal’, as the authors pretend, it was non-existent (i.e. not significant and due to chance only).
- This lack of effect had to be expected considering human physiology.
- The fact that hemoglobin, hematocrit, erythrocytes, and ferritin all change after bloodletting is equally expected.
- Mild adverse effects are also no surprise.
- What is a surprise, however, that such a trial was ever conducted and passed by an ethics committee. Any medic who has not slept through his/her cardiovascular physiology lectures could have predicted the results quite accurately. And running a trial where the result is well-known before the study has started can hardly be called ethical.
Nausea and vomiting are common symptoms of patients with advanced cancer. While there is some evidence for acupuncture point stimulation in the treatment of these symptoms for patients having anticancer treatment, there is little for when they are not related to such treatment.
This study aimed to determine whether acupressure at the pericardium 6 sites can help treat nausea and vomiting suffered by palliative care patients with advanced cancer. The researchers conducted a double-blind randomized controlled trial-active versus placebo acupressure wristbands. In-patients with advanced cancer in two specialist palliative care units who fitted either or both of the following criteria were approached: nausea that was at least of moderate severity; vomiting daily on average for the prior 3 days.
A total of 57 patients were randomized to have either active or placebo acupressure wristbands. There was no difference in any of the outcome measures between the two groups:
- change from the baseline number of vomits;
- Visual Analogue Scale for ‘did acupressure wristbands help you to feel better?’;
- the total number of doses of antiemetic medication;
- the need for escalation of antiemetics.
The authors concluded that, in contrast to a previously published feasibility study, active acupressure wristbands were no better than placebo for specialist palliative care in patients with advanced cancer and nausea and vomiting.
When the research into acupuncture for nausea and vomiting began some 20 years ago, the evidence turned out to be encouraging. Later, as the studies became more and more rigorous, many trials failed to confirm the initial findings. Today, the totality of the evidence is far less convincing than it seemed years ago.
This is a phenomenon that can be observed not just in acupuncture research but in many types of treatment:
- Initially, over-enthusiastic researchers become victims of their own optimism.
- These investigators are less into testing hypotheses than into confirming their own wishful thinking.
- Thus, several positive trials emerge.
- These, however, turn out to be methodologically flawed.
- Eventually, the subject might be picked up by real scientists who truly test hypotheses.
- More and more negative studies thus emerge.
- Depending on how many flawed studies were initially published and how critical the authors of systematic reviews are, it can take years until the totality of the evidence depicts the true picture which discloses the initial findings as false-positive.
The message is, I think, clear: poor quality studies have the potential to mislead us for many years. Eventually, however, the self-cleansing ability of science should generate the truth about the value of any treatment. In other words:
poor-quality science is not just useless, it causes long-term harm
and
critical thinking prevents harm
As promised, I would like to correct the errors in my previous assessment of this paper. To remind everyone:
This systematic review evaluated individualized homeopathy as a treatment for children with attention deficit and hyperactivity disorder (ADHD) when compared to placebo or usual care alone.
Thirty-seven online sources were searched up to March 2021. Studies investigating the effects of individualized homeopathy against any control in ADHD were eligible. Data were extracted to a predefined excel sheet independently by two reviewers.
Six studies were analyzed:
- 5 were RCTs
- 2 were controlled against standard treatments;
- 4 were placebo-controlled and double-blinded.
The meta-analysis revealed a significant effect size across studies of Hedges’ g = 0.542 (95% CI 0.311-0.772; z = 4,61; p < 0.001) against any control and of g = 0.605 (95% CI 0.05-1.16; z = 2.16, p = 0.03) against placebo. The effect estimations are based on studies with an average sample size of 52 participants.
The authors concluded that individualized homeopathy showed a clinically relevant and statistically robust effect in the treatment of ADHD.
_______________________________
Now that I was able to access the full papers, I would like to offer a thorough analysis.
To get included in the review, primary studies had to be:
- Published after 1980,
- Investigating an individualized homeopathic intervention in childhood ADHD,
- Comparing the intervention to a control condition (placebo, standard care or treatment as usual, both of which are referred to as “active control”) in a randomized or non-randomized parallel-group study
design with one or more arms.
Six studies were included:
- Fibert, P., Peasgood, T. & Relton, C. Rethinking ADHD intervention trials: feasibility testing of two treatments and a methodology. Eur. J. Pediatr. 178, 983–993 (2019). – DOI
- Fibert, P., Relton, C., Heirs, M. & Bowden, D. A comparative consecutive case series of 20 children with a diagnosis of ADHD receiving homeopathic treatment, compared with 10 children receiving usual care. Homeopathy 105, 194–201 (2016). – DOI
- Jacobs, J., Williams, A. L., Girard, C., Njike, V. Y. & Katz, D. Homeopathy for attention-deficit/hyperactivity disorder: a pilot randomized-controlled trial. J. Altern. Complement. Med. 11, 799–806 (2005). – DOI
- Jones, M. The efficacy of homoeopathic simillimum in the treatment of attention-deficit/hyperactivity disorder (AD/HD) in schoolgoing children aged 6-11 years. https://openscholar.dut.ac.za/bitstream/10321/534/1/Jones_2009.pdf (2009).
- Frei, H. et al. Homeopathic treatment of children with attention deficit hyperactivity disorder: a randomised, double blind, placebo controlled crossover trial. Eur. J. Pediatr. 164, 758–767 (2005). – DOI
- Oberai, P. et al. Homoeopathic management of attention deficit hyperactivity disorder: a randomised placebo-controlled pilot trial. Indian J. Res. Homoeopathy 7, 158–167 (2013).
Exclusion criteria were:
- Homeopathic intervention not individualized,
- Serious methodological flaws, such as incidental unblinding, failure to report important data, or insufficient data for meta-analysis.
One study was excluded:
- Lamont, J. Homoeopathic treatment of attention deficit hyperactivity disorder. Br. Homeopathic J. 86, 196–200 (1997). – DOI
I will first make several points about Walach’s systematic review itself and then have a look at the primary studies that it included. Finally, I will try to draw some conclusions.
The review authors state in their introduction that “beneficial effects of this intervention [homeopathy] have been shown for various kinds of medical conditions, including child diarrhea, supportive care in cancer, fibromyalgia, or ADHD.” In other words, already in the introduction, they disclose their strong pro-homeopathy bias; it would, of course, not be difficult to find investigations that contradict their optimism.
Despite the stated inclusion/exclusion criteria, the authors did include the Frei-study that did not follow a parallel-group design (see also below).
The authors included two active-controlled studies both of which did not report the type of treatment received by the control group. In other words, these trials failed to report important data which was a stated exclusion criterium (see below).
In their discussion section, the authors state that “all included studies employed individualized homeopathy and were of comparable, solid quality, hence a lack of methodological rigor is unlikely the reason for the difference between homeopathy and controls…” This, I think, is grossly misleading; even according to the authors’ own assessments, one study was deemed to have a high risk of bias and in two studies the risk of bias was “unclear”.
The overall positive effect of homeopathy demonstrated by the review was determined almost exclusively by the study of Oberai et al (p-value = 0.000). In fact, the studies by Jones and by Jacobs were negative, and the one by Frei was borderline positive with a p-value of 0.46. The authors address this crucial issue repeatedly and claim that excluding Oberai et al would still generate an overall positive meta-analytic result. Yet, they do not mention that the overall result would no longer be clinically relevant.
Looking at the included primary studies, I should make the following points:
- The two Filbert studies, as mentioned, failed to report important data and should, according to the stated exclusion criteria, not have been included.
- The study by Jacobs was a pilot study and generated negative findings.
- The study by Jones is a non-peer-reviewed thesis. In my view, it should never have been included.
- The study by Frei was a cross-over trial. According to the exclusion/inclusion criteria of the authors, it should not have been included.
- The study by Oberai et al is the trial that has by far the largest effect size and thus is the driver of the overall result of the review. It is therefore important to have a closer look at it.
Here is the abstract:
Objective: To evaluate the usefulness of individualised homoeopathic medicines in treatment of Attention Deficit Hyperactivity Disorder (ADHD).
Design: Randomised placebo-controlled single-blind pilot trial.
Setting: Central Research Institute (Homoeopathy), Kottayam, Kerala, India from June 2009 to November 2011.
Participants: Children aged 6-15 years meeting the Diagnostic Statistical Manual of mental disorders (DSM-IV) criteria for ADHD.
Interventions: A total of 61 patients (Homoeopathy = 30, placebo = 31) were randomised to receive either individualised homoeopathic medicine in fifty millesimal (LM) potency or placebo for a period of one year.
Outcome measures: Conner’s Parent Rating Scale-Revised: Short (CPRS-R (S)), Clinical Global Impression-Severity Scale (CGI-SS), Clinical Global Impression- Improvement Scale (CGI-IS) and Academic performance.
Results: A total of 54 patients (homoeopathy = 27, placebo = 27) were analysed under modified intention to treat (ITT). All patients in homoeopathy group showed better outcome in baseline adjusted General Linear Model (GLM) repeated measures ANCOVA for oppositional, cognition problems, hyperactivity and ADHD Index (domains of CPRS-R (S)) and CGI-IS at T3, T6, T9 and T12 (P = 0.0001). The mean baseline-adjusted treatment difference between groups at month 12 from baseline for all individual outcome measures favoured homoeopathy group; Oppositional (−16.4, 95% CI – 20.5 to − 12.2, P = 0.0001), Cognition problems (−15.5, 95% CI − 19.2 to − 11.8, P = 0.0001), Hyperactivity (−20.6, 95% CI − 25.6 to − 15.4, P = 0.0001), ADHD I (−15.6, 95% CI − 19.5 to − 11.6, P = 0.0001), Academic performance 14.4%, 95% CI 8.3 to 20.5, P = 0.0001), CGISS (−1.6, 95% CI − 1.9 to − 1.2, P = 0.0001), CGIIS (−1.6, 95% CI − 2.3 to -0.9, P = 0.0001).
Conclusion: This pilot study provides evidence to support the therapeutic effects of individualised homoeopathic medicines in ADHD children. However, the results need to be validated in multi-center randomised double-blind placebo-controlled clinical trial.
Here are a few points of concern related to the Oberai et al:
- The trial was a mere pilot study.
- Despite the fact that it is now 9 years old, the authors never published a definitive trial.
- The study was published in an obscure journal that is not Medline-listed.
- The study is very poorly reported.
- It is unclear how the diagnosis of ADHD for including the patients was verified.
- The control patients were treated for one year with a placebo and no other therapies. In my view, this is not ethical.
- The method of randomization is unclear.
- The authors state that acute symptoms were treated throughout the study period with homeopathy, even in the control group. This seems odd and defies the principle of a placebo-controlled trial.
- The authors state that only the patients were blind, not the investigators. This opens the door wide for all sorts of biases. It is, for example, likely that it also de-blinded the patients (the verum could be adjusted and changed, while the placebo remained constant).
All in all, this paper is of poor quality, Its findings are far from trustworthy and were not meant to be definitive. According to the following exclusion criteria, it should have been excluded:
- It had several serious methodological flaws.
- It did not blind the investigators.
- It is likely that patients were de-blinded.
- It failed to report important data.
So, why did Walach and his co-authors include it?
Could it be because, without the Oberai-study, the overall findings of the review would at best have turned out to be borderline significant and not clinically relevant?
In a previous post, I reported about the ‘biggest ever’, ‘history-making’ conference on integrative medicine. It turns out that it was opened by none other than Prince Charles. Here is what the EXPRESS reported about his opening speech:
Opening the conference, Charles said:
“I know a few people have seen this integrated approach as being in some way opposed to modern medicine. It isn’t. But we need to combine this with a personal approach that also takes account of our beliefs, hopes, culture and history. It builds upon the abilities of our minds and bodies to heal, and to live healthy lives by improving diet and lifestyle.”
Dr. Michael Dixon, Chair of the College of Medicine, said:
“Medicine, as we know it, is no longer affordable or sustainable. Nor is it able to curb the increase in obesity, mental health problems and most long-term diseases. A new medical mindset is needed, which goes to the heart of true healthcare. The advantages and possibilities of social prescription are limitless. An adjustment to the system now will provide a long-term, sustainable solution for the NHS to meet the ever-increasing demand for funding and healthcare professionals.”
_______________________
Charles very kindly acknowledges that not everyone is convinced about his concept of integrated/integrative medicine. Good point your royal highness! But I fear Charles did not quite understand our objections. In a nutshell: it is not possible to cure the many ills of conventional medicine by adding unproven and disproven therapies to it. In fact, it distracts from our duty to constantly improve conventional medicine. And pretending it is all about diet and lifestyle is simply not true (see below). Moreover, it is disingenuous to pretend that diet and lifestyle do not belong to conventional healthcare.
Dr. Dixon’s concern about the affordability of medicine is, of course, justified. But the notion that “the advantages and possibilities of social prescription are limitless” is a case of severe proctophasia, and so is Dixon’s platitude about ‘adjusting the system’. His promotion of treatments like Acupuncture, Alexander Technique, Aromatherapy, Herbal Medicine, Homeopathy, Hypnotherapy, Massage, Naturopathy, Reflexology, Reiki, Tai Chi, Yoga Therapy will not adjust anything, it will only make healthcare less efficient.
I do not doubt for a minute that doctors are prescribing too many drugs and that we could save huge amounts by reminding patients that they are responsible for their own health while teaching them how to improve it without pills. This is what we learn in medical school! All we need to do is remind everyone concerned. In fact, Charles and his advisor, Michael, could be most helpful in achieving this – but not by promoting a weird branch of healthcare (integrative/integrated medicine or whatever other names they choose to give it) that can only distract from the important task at hand.
Alan Gaby, the assistant editor of the journal Integr Med has written an interesting commentary about widespread fraud in natural health products research. Here is an excerpt of his article:
During the past 49 years, I have reviewed and analyzed more than 50 000 papers from the biomedical literature, most of which were related to the field of nutritional medicine. Doing this work has given me some understanding of how to assess the reliability of a study. Over the past 10 to 15 years, an uncomfortably large and growing number of published papers related to my area of expertise have left me wondering whether the research was fabricated; that is, whether people were writing papers about research that had not actually been conducted. If the studies were not actually conducted, the publishing of this research is an affront to all who value integrity in science, and it has the potential to harm practitioners and patients who rely on its findings.
The studies that have raised concerns have come primarily from Iran and to a lesser extent from Egypt, China, India, Japan, and a few other countries. Characteristics of these concerning studies typically include one or more of the following:
- The study comes from an investigator or research group that has published an enormous number of randomized clinical trials in a relatively short period of time.
- The number of participants in the trial is unusually large, when considering the resources that appear to be available to the researchers.
- The recruitment period for the trial is unusually short.
- The paper is submitted to a journal unusually rapidly after the study is completed, or in some cases before it would have been possible to have completed the trial.
- A randomized double-blind trial is conducted before there is any preliminary evidence of efficacy in humans (such as case reports or uncontrolled trials). Because double-blind trials are expensive to conduct, such trials are generally reserved for treatments for which there is some evidence of efficacy.
- The magnitude of the reported improvement is much larger than is typically seen in trials using just one or two nutrients.
- No funding source is listed or the study is listed as self-funded. This is of particular concern when the sample size or study design suggests that the study was expensive.
- The design of the study raises ethical issues, such as participants not being permitted to use treatments that are known to be effective.
- One or more baseline characteristics of the study group appear to be implausible.
- The research was conducted by a student as part of a graduate school thesis, and the magnitude of the project seems to have been beyond the capabilities and resources of a student.
__________________________________
What Gaby alludes to is a problem indeed. I have previously posted about the Chinese aspect of this story. What Gaby does not mention is the fact that even many studies of so-called alternative medicine (SCAM) which seem to be not overtly fraudulent are nevertheless highly suspect. I am referring to trials that are fatally flawed and/or studies that draw unwarranted conclusions. These are, of course, the types of studies that are the main target of this blog. Because they are so numerous, I feel that the damage they do is much bigger than that of the more overtly fraudulent papers.
This systematic review evaluated individualized homeopathy as a treatment for children with attention deficit and hyperactivity disorder (ADHD) when compared to placebo or usual care alone.
Thirty-seven online sources were searched up to March 2021. Studies investigating the effects of individualized homeopathy against any control in ADHD were eligible. Data were extracted to a predefined excel sheet independently by two reviewers.
Six studies were analyzed:
- 5 were RCTs
- 2 were controlled against standard treatments;
- 4 were placebo-controlled and double-blinded.
The meta-analysis revealed a significant effect size across studies of Hedges’ g = 0.542 (95% CI 0.311-0.772; z = 4,61; p < 0.001) against any control and of g = 0.605 (95% CI 0.05-1.16; z = 2.16, p = 0.03) against placebo. The effect estimations are based on studies with an average sample size of 52 participants.
The authors concluded that individualized homeopathy showed a clinically relevant and statistically robust effect in the treatment of ADHD.
This is a counter-intuitive result (to put it mildly), and it is, therefore, wise to have a look at the 6 included studies:
1.Frei, H. et al. Homeopathic treatment of children with attention deficit hyperactivity disorder: a randomised, double blind, placebo controlled crossover trial. Eur. J. Pediatr. 164, 758–767 (2005).
This was a trial with just 62 patients who had previously responded to homeopathy. The study was conducted by known proponents of homeopathy and had a highly unusual design. The results suggested that homeopathy was better than placebo.
2. Oberai, P. et al. Homoeopathic management of attention deficit hyperactivity disorder: a randomised placebo-controlled pilot trial. Indian J. Res. Homoeopathy 7, 158–167 (2013).
This one was published in an obscure journal that I could not access.
3. Jacobs, J., Williams, A. L., Girard, C., Njike, V. Y. & Katz, D. Homeopathy for attention-deficit/hyperactivity disorder: a pilot randomized-controlled trial. J. Altern. Complement. Med. 11, 799–806 (2005)
This study showed that there were no statistically significant differences between homeopathic remedy and placebo groups on the primary or secondary outcome variables.
4. Jones, M. The efficacy of homoeopathic simillimum in the treatment of attention-deficit/hyperactivity disorder (AD/HD) in schoolgoing children aged 6-11 years (2009).
This was a small unpublished (and not peer-reviewed) thesis. Its results showed no statistically significant effect of treatment.
5. Lamont, J. Homoeopathic treatment of attention deficit hyperactivity disorder. Br. Homeopathic J. 86, 196–200 (1997)
This was a small (n=46) trial with an unusual design. Its results suggested that homeopathy was better than placebo.
6. von Ammon, K. et al. Homeopathic RCT embedded in a long-term observational study of children with ADHD—a successful model of whole systems CAM research. Eur. J. Integr. Med. 1, 27 (2008).
Even though the journal is Medline-listed, I was unable to find this paper. I did, however, find a paper by the same authors with the same title. It turned out to be a duplication of the paper by Frei et al listed above.
_________________________
All in all, this brief analysis of the available abstracts (most full papers are behind paywalls) leaves many questions as to the trustworthiness of this systematic review unanswered. The fact that H. Walach (and other apologists of homeopathy) is its senior author does not inspire me with overwhelming confidence. In any case, I very much doubt that the authors’ conclusion is correct. I therefore would encourage someone with access to all full papers to initiate a more thorough analysis; the abstracts obviously leave many questions unanswered. For instance, it would be crucial to know how many of the trials followed an A+B versus B design (I suspect most studies did, and this would completely invalidate the review’s conclusion). I am more than happy to co-operate with such an evaluation.