pregnancy
This study evaluated the effect of ear acupressure (auriculotherapy) on the weight-gaining pattern of overweight women during pregnancy. It was a single-blinded randomized clinical trial conducted between January and September 2022 and took place in health centers of Qom University of Medical Sciences in Iran.
One-hundred thirty overweight pregnant women were selected by a purposeful sampling method and then divided into two groups by block randomization method. In the intervention group, two seeds were placed in the left ear on the metabolism and stomach points, while two seeds were placed in the right ear on the mouth and appetite points. Participants in the intervention group were instructed to press the seeds six times a day, 20 minutes before a meal for five weeks. For the placebo group, the Vaccaria seedless label was placed at the same points as the intervention group.
A digital scale with an accuracy of 0.1 kg was used to weigh the pregnant women during each visit. Descriptive statistics, independent T-test, chi-square, and repeated measure ANOVA (analysis of variance) test were used to check the research objectives.
There was a statistically significant difference between the auriculotherapy and placebo groups immediately after completing the study (1120.68 ± 425.83 vs. 2704.09 ± 344.96 (g); = 0.018), respectively. Also, there was a substantial difference in the weight gain of women two weeks (793.10 ± 278.38 vs. 1090.32 ± 330.31 (g); < 0.001) and four weeks after the intervention (729.31 ± 241.52 vs. 964.51 ± 348.35 (g); < 0.001) between the auriculotherapy and placebo groups.
The authors concluded that the results of the present study indicated the effectiveness of auriculotherapy in controlling the weight gain of overweight pregnant women. This treatment could be used as a safe method, with easy access, and low cost in low-risk pregnancies.
In order to understand these findings, it is worth reading the methods section of the paper. It explains what actually happened with the two groups:
After providing explanations to familiarize the participants with the working method and answering their questions, the participants were requested to be comfortable. The first author who has an auriculotherapy certificate did the intervention. The intervention began by disinfecting both ears with a 70% alcohol solution. After determining the location of metabolism and stomach points in the left ear and mouth and appetite points in the right ear related to weight and appetite control, the researcher placed the seeds on the desired points… The intervention lasted for a total of 5 weeks. The seeds were changed twice a week (once every three days) by the researcher. The participants in the intervention group were taught to press the seeds 6 times a day for one minute each time. The pressure method was to use moderate stimulation with continuous pressure. In the first session, the researcher fully taught the participants the amount of pressure and the duration of it in a practical way and asked them to do this once in her presence to ensure that it was correct. Participants were recommended to do this preferably 20 minutes before eating. The researcher reminded the participants in the intervention group of their daily interventions by phone or text message. Each night, they were asked to check if they had followed the instructions and completed the daily registration checklist. In each seed replacement session, which was performed every three days, the checklist of the previous session was viewed and checked, and a checklist was received every week at the same time as the participants were weighed. Subjects were also emphasized in case of any symptoms of allergies or infections and pain as soon as possible through the contact number provided to them to discuss the issue with the researcher to remove the seeds.
In the placebo group, instead of real seeds, a label without Vaccaria seed (waterproof fabric adhesive) was placed by the researcher at the desired points in both ears, and the participants did not receive training to compress the points. They also did not receive the list of daily pressing points. All follow-ups and replacement of labels were performed in the same way as the intervention group in the placebo group. Finally, all participants were requested to notify the researcher if any seeds or labels were removed for any reason. It should be noted that pregnant mothers were unaware of the nature of the group to which they belonged.
It seems clear, therefore, that the patients were NOT blinded and that the verum patients received different care and more attention/encouragement than the placebo group. This means firstly that the trial was NOT single-blind, as the authors claim. Secondly, it means that the outcomes were most likely NOT due to ear acupressure at all – they were caused by the non-specific effects of expectation, extra attention, etc. which, in turn, motivated the women to better control their weight. Consequently, the conclusions of this study should be re-phrased:
The results of the present study fail to indicate the effectiveness of auriculotherapy in controlling the weight gain of overweight pregnant women.
In addition, I feel that the researchers, supervisors, peer-reviewers, editors should all bow their heads in shame for trying to mislead us.
The increasing demand for fertility treatments has led to the rise of private clinics offering so-called alternative medicine (SCAM) treatments. Even King Charles has recently joined in with this situalion. One of the most frequently offered SCAM infertility treatment is acupuncture. However, there is no good evidence to support the effectiveness of acupuncture in treating infertility.
This study evaluated the scope of information provided by SCAM fertility clinics in the UK. A content analysis was conducted on 200 websites of SCAM fertility clinics in the UK that offer acupuncture as a treatment for infertility. Of the 48 clinics that met the eligibility criteria, the majority of the websites did not provide sufficient information on: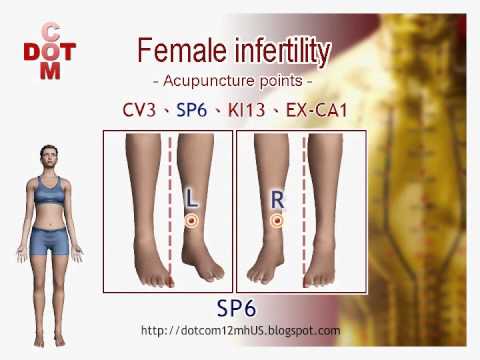
- the efficacy,
- the risks,
- the success rates
of acupuncture for infertility.
The authors concluded that this situation has the potential to infringe on patient autonomy, provide false hope and reduce the chances of pregnancy ever being achieved as fertility declines during the time course of ineffective acupuncture treatment.
The authors are keen to point out that their investigation has certain limitations. The study only analysed the information provided on the clinics’ websites and did not assess the quality of the treatment provided by the clinics.
Therefore, the study’s fndings cannot be generalized to the quality of the acupuncture treatment provided by the clinics.
Nonetheless the paper touches on very important issues: far too many health clinics that offer SCAM for this or that indication operate way outside the ethically (and legally) acceptable norm. They advertise their services without making it clear that they are neither effective nor safe. Desperate consumers thus fall for their promises. In the case of infertility, this might result merely in frustration and loss of (often substantial amounts of) money. In the case of serious disease, such as cancer, this often results in premature death.
It is time, I think, that this entire sector is regualted in a way that it does not endanger the well-being, health, or life of consumers.
Charles has a well-documented weakness for so-called alternative medicine (SCAM) – not just any SCAM but predominantly the type of SCAM that is both implausible and ineffective. Therefore, nobody can be all that surprised to read in THE TIMES that he has decided to use SCAM for helping women who have difficulties getting pregnant.

If one really wanted to employ SCAM for this aim one is spoilt for choice. In fact, there are only few SCAMs that don’t claim to be useful for this purpose.
A recent review, for instance, suggested that some supplements might be helpful. Other authors advocate SCAMs such as acupuncture, moxibustion, Chinese herbal medicine, psychological intervention, biosimilar electrical stimulation, homeopathy, or hyperbaric oxygen therapy.
Yes, I know! The evidence for these treatments is lousy, and I would never issue a recommendation based on such flimsy evidence.
Yet, the SCAM project at Dumfries House, the Scottish stately home Charles restored in 2007, offers acupuncture, reflexology, massage, yoga, and hypnotherapy for infertile women.
REFLEXOLOGY for female infertility?
Reflexology, also called zone therapy, is a manual treatment where pressure is applied usually to the sole of the patient’s foot and sometimes also to other areas such as the hands or ears. According to its proponents, foot reflexology is more than a simple foot massage that makes no therapeutic claims beyond relaxation. It is based on the idea that the human body is divided into 10 zones each of which is represented on the sole of the foot. Reflexologists employ maps of the sole of the foot where the body’s organs are depicted. By massaging specific zones which are assumed to be connected to specific organs, reflexologists believe to positively influence the function of these organs. While reflexology is mostly used as a therapy, some therapists also claim they can diagnose health problems through feeling tender or gritty areas on the sole of the foot which, they claim, correspond to specific organs.
Reflexology is not merely implausible as a treatment for infertility, it also boasts of some fairly rigorous trial evidence. A clinical trial (perhaps even the most rigorous of all the trials of SCAM for female fertility problems) testing whether foot reflexology might have a positive effect on the induction of ovulation stated that “the results suggest that any effect on ovulation would not be clinically relevant”.
So, as so often before in the realm of SCAM, Charles has demonstrated that his lack of critical thinking leads him to the least promising options.
Well done, Your Majesty!
Semen retention is a so-called alternative medicine (SCAM) that involves intentionally avoiding ejaculating. A person can do this by abstaining from any sexual activity, stopping before the point of ejaculation, or teaching themselves to orgasm without ejaculating.
Although this practice may seem new, this is likely only due to recent internet popularity. In fact, semen retention is an ancient practice, believed to boost male physical and spiritual energy.
Some other names for semen retention include:
- coitus reservatus
- seminal conservation
- sexual continence
It is also known as or included in practices called:
- karezza (Italian)
- maithuna (Hindu Tantra)
- sahaja (Hindu Yoga)
- tantra (Hinduism and Buddhism)
- cai Yin pu Yang and cai Yang pu Yin (Taoist)
Semen retention is said to be good for a range of things:
Mental health
- increased motivation
- improved energy and focus
- more self-confidence
- reduced anxiety
- better memory
- improved concentration
Physical health
- clearer skin
- increased testosterone
- more weight loss
- increased muscle mass
- physical rejuvenation
- a deeper voice
Spiritual health
- a greater sense of purpose
- stronger or deeper emotional bonds in relationships
- a stronger sense of overall harmony
________________________
Yes, I agree, this sounds weird!
But is there any evidence?
Yes, e.g.:
Males of some species use mate retention behavior and investment in ejaculate quality as anti-cuckoldry tactics concurrently while others do so in a compensatory fashion. Leivers, Rhodes, and Simmons (2014) reported that men who performed mate retention less frequently produced higher-quality ejaculates, suggesting that humans use these tactics compensatorily. We conducted a conceptual replication of this research in a sample of 41 men (18-33 years; M = 23.33; SD = 3.60). By self-report, participants had not had a vasectomy and had never sought infertility treatment. We controlled for several covariates known to affect ejaculate quality (e.g., abstinence duration before providing an ejaculate) and found no statistically significant relationships between mate retention behavior and four components of ejaculate quality: sperm velocity, sperm concentration, slow motility, and ejaculate volume. The present results provide little support for the hypothesis that human males deploy mate retention behavior and ejaculate quality investment compensatorily. We discuss the limitations of this study and highlight the need for research to address questions about the nature of anti-cuckoldry tactic deployment in humans, especially concerning investment in ejaculate quality.
In species where females mate with multiple males, the sperm from these males must compete to fertilise available ova. Sexual selection from sperm competition is expected to favor opposing adaptations in males that function either in the avoidance of sperm competition (by guarding females from rival males) or in the engagement in sperm competition (by increased expenditure on the ejaculate). The extent to which males may adjust the relative use of these opposing tactics has been relatively neglected. Where males can successfully avoid sperm competition from rivals, one might expect a decrease in their expenditure on tactics for the engagement in sperm competition and vice versa. In this study, we examine the relationship between mate guarding and ejaculate quality using humans as an empirical model. We found that men who performed fewer mate guarding behaviors produced higher quality ejaculates, having a greater concentration of sperm, a higher percentage of motile sperm and sperm that swam faster and less erratically. These effects were found independent of lifestyle factors or factors related to male quality. Our findings suggest that male expenditure on mate guarding and on the ejaculate may represent alternative routes to paternity assurance in humans.
The uncritical application of western psychiatric concepts in non-western societies resulting in culturally invalid psychiatric syndromes, have been extensively documented. Such instances are considered ‘category errors’. In contrast, ‘reverse category errors’ although theoretically postulated, have never been empirically demonstrated. Diagnostic criteria of an established South Asian culture specific neurosis, Dhāt syndrome, were deployed by a psychiatrist of South Asian origin, amongst 47 white Britons in London, UK, presenting for the first time with a clinic diagnosis of ICD-9 Depressive Neurosis (Dysthymic Disroder, ICD-11). The proceedure yielded a new disorder, Semen Retention Syndrome. Based on narrative accounts and quantitative scores on the Hamilton Depression Rating Scale, the evidence suggests that a significant subset of white British subjects diagnosed with Dysthymic Disorder, may in fact be expressing a psychological variation of a previously unknown local White British somatisation phenomena labelled Semen Retention Syndrome. Anxiety and depressive symptoms presented by this subset of subjects were primarily attributed to a core irrational belief and a cognitive error centered around misunderstood concepts of semen physiology. Consequently, the undue focus on mood idioms by both white British patients and their health professionals, leads to a mistaken diagnosis of Mood Disorder, and results in incorrect treatment. The implications of this ethnocentric mode of reasoning raises concerns about existing concepts in psychiatric phenomenology and for official international diagnostic classificatory systems. The paper concludes by arguing that category errors in both directions are instances of cultural iatrogenesis, and underscore the importance of a culturally valid psychiatry.
_________________________
I was unable to find support for any of the above-listed effects of semen retention. So, claims like “Semen Retention is life-changing, especially for men. Not only, it help you turn into a real alpha male but also offers great health benefits” need to be taken with a pinch of salt. Yet, it did occur to me that semen retention might have one positive outcome:
It reduces the chances of stupid people multiplying!
The Sunday Times reported yesterday reported that five NHS trusts currently offer moxibustion to women in childbirth for breech babies, i.e. babies presenting upside down. Moxibustion is a form of Traditional Chinese Medicine (TCM) where mugwort is burned close to acupuncture points. The idea is that this procedure would stimulate the acupuncture point similar to the more common way using needle insertion. The fifth toe is viewed as the best traditional acupuncture point for breech presentation, and the treatment is said to turn the baby in the uterus so that it can be delivered more easily.
At least four NHS trusts are offering acupuncture and reflexology with aromatherapy to help women with delayed pregnancies, while 15 NHS trusts offer hypnobirthing classes. Some women are asked to pay fees of up to £140 for it. These treatments are supposed to relax the mother in the hope that this will speed up the process of childbirth.
The Nice guidelines on maternity care say the NHS should not offer acupuncture, acupressure, or hypnosis unless specifically requested by women. The reason for the Nice warning is simple: there is no convincing evidence that these therapies are effective.
Campaigner Catherine Roy who compiled the list of treatments said: “To one degree or another, the Royal College of Midwives, the Care Quality Commission and parts of the NHS support these pseudoscientific treatments.
“They are seen as innocuous but they carry risks, can delay medical help and participate in an anti-medicalisation stance specific to ‘normal birth’ ideology and maternity care. Nice guidelines are clear that they should not be offered by clinicians for treatment. NHS England must ensure that pseudoscience and non-evidence based treatments are removed from NHS maternity care.”
Birte Harlev-Lam, executive director of the Royal College of Midwives (RCM), said: “We want every woman to have as positive an experience during pregnancy, labour, birth and the postnatal period as possible — and, most importantly, we want that experience to be safe. That is why we recommend all maternity services to follow Nice guidance and for midwives to practise in line with the code set out by the Nursing and Midwifery Council.”
A spokeswoman for Nice said it was reviewing its maternity guidelines. NHS national clinical director for maternity and women’s health, Dr Matthew Jolly, said: “All NHS services are expected to offer safe and personalised clinical care and local NHS areas should commission core maternity services using the latest NICE and clinical guidance. NHS trusts are under no obligation to provide complementary or alternative therapies on top of evidence-based clinical care, but where they do in response to the wishes of mothers it is vital that the highest standards of safety are maintained.”
On this blog, we have repeatedly discussed the strange love affair of midwives with so-called alternative medicine (SCAM), for instance, here. In 2012, we published a summary of 19 surveys on the subject. It showed that the prevalence of SCAM use varied but was often close to 100%. Much of it did not seem to be supported by strong evidence for efficacy. We concluded that most midwives seem to use SCAM. As not all SCAMs are without risks, the issue should be debated openly. Today, there is plenty more evidence to show that the advice of midwives regarding SCAM is not just not evidence-based but also often dangerous. This, of course, begs the question: when will the professional organizations of midwifery do something about it?
Acupuncture is emerging as a potential therapy for relieving pain, but the effectiveness of acupuncture for relieving low back and/or pelvic pain (LBPP) during pregnancy remains controversial. This meta-analysis aimed to investigate the effects of acupuncture on pain, functional status, and quality of life for women with LBPP pain during pregnancy.
The authors included all RCTs evaluating the effects of acupuncture on LBPP during pregnancy. Data extraction and study quality assessments were independently performed by three reviewers. The mean differences (MDs) with 95% CIs for pooled data were calculated. The primary outcomes were pain, functional status, and quality of life. The secondary outcomes were overall effects (a questionnaire at a post-treatment visit within a week after the last treatment to determine the number of people who received good or excellent help), analgesic consumption, Apgar scores >7 at 5 min, adverse events, gestational age at birth, induction of labor and mode of birth.
Ten studies, reporting on a total of 1040 women, were included. Overall, acupuncture
- relieved pain during pregnancy (MD=1.70, 95% CI: (0.95 to 2.45), p<0.00001, I2=90%),
- improved functional status (MD=12.44, 95% CI: (3.32 to 21.55), p=0.007, I2=94%),
- improved quality of life (MD=−8.89, 95% CI: (−11.90 to –5.88), p<0.00001, I2 = 57%).
There was a significant difference in overall effects (OR=0.13, 95% CI: (0.07 to 0.23), p<0.00001, I2 = 7%). However, there was no significant difference in analgesic consumption during the study period (OR=2.49, 95% CI: (0.08 to 80.25), p=0.61, I2=61%) and Apgar scores of newborns (OR=1.02, 95% CI: (0.37 to 2.83), p=0.97, I2 = 0%). Preterm birth from acupuncture during the study period was reported in two studies. Although preterm contractions were reported in two studies, all infants were in good health at birth. In terms of gestational age at birth, induction of labor, and mode of birth, only one study reported the gestational age at birth (mean gestation 40 weeks).
The authors concluded that acupuncture significantly improved pain, functional status and quality of life in women with LBPP during the pregnancy. Additionally, acupuncture had no observable severe adverse influences on the newborns. More large-scale and well-designed RCTs are still needed to further confirm these results.
What should we make of this paper? 
In case you are in a hurry: NOT A LOT!
In case you need more, here are a few points:
- many trials were of poor quality;
- there was evidence of publication bias;
- there was considerable heterogeneity within the studies.
The most important issue is one studiously avoided in the paper: the treatment of the control groups. One has to dig deep into this paper to find that the control groups could be treated with “other treatments, no intervention, and placebo acupuncture”. Trials comparing acupuncture combined plus other treatments with other treatments were also considered to be eligible. In other words, the analyses included studies that compared acupuncture to no treatment at all as well as studies that followed the infamous ‘A+Bversus B’ design. Seven studies used no intervention or standard of care in the control group thus not controlling for placebo effects.
Nobody can thus be in the slightest surprised that the overall result of the meta-analysis was positive – false positive, that is! And the worst is that this glaring limitation was not discussed as a feature that prevents firm conclusions.
Dishonest researchers?
Biased reviewers?
Incompetent editors?
Truly unbelievable!!!
In consideration of these points, let me rephrase the conclusions:
The well-documented placebo (and other non-specific) effects of aacupuncture improved pain, functional status and quality of life in women with LBPP during the pregnancy. Unsurprisingly, acupuncture had no observable severe adverse influences on the newborns. More large-scale and well-designed RCTs are not needed to further confirm these results.
PS
I find it exasperating to see that more and more (formerly) reputable journals are misleading us with such rubbish!!!
Earlier this year, I started the ‘WORST PAPER OF 2022 COMPETITION’. As a competition without a prize is no fun, I am offering the winner (that is the lead author of the winning paper) one of my books that best fits his/her subject. I am sure this will overjoy him or her.
And how do we identify the winner? I will continue blogging about nominated papers (I hope to identify about 10 in total), and towards the end of the year, I let my readers decide democratically.
In this spirit of democratic voting, let me suggest to you ENTRY No 8 (it is so impressive that I must show you the unadulterated abstract):
Introduction
Female sexual dysfunction (FSD) seriously affects the quality of life of women. However, most women do not have access to effective treatment.
Aim
This study aimed to determine the feasibility and effectiveness of the use of acupuncture in FSD treatment based on existing clear acupuncture protocol and experience-supported face-to-face therapy.
Methods
A retrospective analysis was performed on 24 patients with FSD who received acupuncture from October 2018 to February 2022. The Chinese version of the female sexual function index , subjective sensation, sexual desire, sexual arousal, vaginal lubrication, orgasm, sexual satisfaction, and dyspareunia scores were compared before and after the treatment in all 24 patients.
Main Outcome Measure
A specific female sexual function index questionnaire was used to assess changes in female sexual function before and after the acupuncture treatment.
Results
In this study, the overall treatment improvement rate of FSD was 100%. The Chinese version of the female sexual function index total score, sexual desire score, sexual arousal score, vaginal lubrication score, orgasm score, sexual satisfaction score, and dyspareunia score during intercourse were significantly different before and after the treatment (P < .05). Consequently, participants reported high levels of satisfaction with acupuncture. This study indicates that acupuncture could be a new and effective technique for treating FSD. The main advantages of this study are its design and efficacy in treating FSD. To the best of our knowledge, this is the first study to evaluate the efficacy of acupuncture in the treatment of FSD using the female sexual function index scale from 6 dimensions. The second advantage is that the method used (ie, the nonpharmacological method) is simple, readily available, highly safe with few side effects, and relatively inexpensive with high patient satisfaction. However, limitations include small sample size and lack of further detailed grouping, pre and post control study of patients, blank control group, and pre and post control study of sex hormones.
Conclusion
Acupuncture can effectively treat FSD from all dimensions with high safety, good satisfaction, and definite curative effect, and thus, it is worthy of promotion and application.
My conclusion is very different: acupuncture can effectively kill any ability for critical thinking.
I hardly need to list the flaws of this paper – they are all too obvious, e.g.:
- there is no control group; the results might therefore be due to a host of factors that are unrelated to acupuncture,
- the trial was too small to allow far-reaching conclusions,
- the study does not tell us anything about the safety of acupuncture.
The authors call their investigation a ‘pilot study’. Does that excuse the flimsiness of their effort? No! A pilot study cannot draw conclusions such as the above.
What’s the harm? you might ask; nobody will ever read such rubbish and nobody will have the bizarre idea to use acupuncture for treating FSD. I’m afraid you would be wrong to argue in this way. The paper already got picked up by THE DAILY MAIL in an article entitled “Flailing libido? Acupuncture could help boost sex drive, scientists say” which was as devoid of critical thinking as the original study. Thus we can expect that hundreds of desperate women are already getting needled and ripped off as we speak. And in any case, offensively poor science is always harmful; it undermines public trust in research (and it renders acupuncture research the laughing stock of serious scientists).
I have often called out unreliable or fraudulent research in the realm of Traditional Chinese Medicine (TCM). I think it is important to do so because the abundance of scientific misconduct is such that it has become a danger to public health. Today, I present yet another example:
This recent review claimed to summarize the evidence on TCM in treating MI, the clinical evaluations of TCM in treating male infertility (MI), and the molecular mechanisms of TCM effects. I was alerted to the fact that the authors cite a paper on acupuncture that I had co-authored. Here is the section in question from the review:
Acupuncture is one of the therapeutic techniques that are part of TCM. Acupuncture is a non-invasive technique and is regarded as free of risk if performed by trained personnel [35]. One of the advantages of acupuncture was that the incidence of adverse effects was substantially lower than that of many drugs or other accepted [35]. Acupuncture has been used in the treatment of male and female infertility and in assisted reproductive technology treatments for many years. A total of 100 patients with MI who met the diagnostic criteria were randomly divided into two groups [7]. Half of the patients received acupuncture treatment, and the other half received placebo acupuncture. After 10 weeks treatment, acupuncture successfully improved the indicators of the semen, including the spermatozoa survival rate, b-level activity rate, sperm density, sperm activity rate. A total of 28 infertile patients with severe oligoasthenozoospermia received acupuncture according to the principles of acupuncture and 29 infertile patients received placebo acupuncture. A significantly higher percentage of motile sperm (World Health Organization categories A-C), but no effect on sperm concentration, was found after acupuncture compared with placebo acupuncture [36]. Of the 279 cases of male sterility treated by the combination of acupuncture, pilose antler essence injection to acupoints and oral administration of Chinese materia medica, 142 cases (47.8%) were cured, 81 cases (27.3%) markedly effective, 53 cases (17.8%) effective and 21 cases (7.1%) ineffective [37]. The therapeutic effect of the combination of these three treatments was satisfactory.
Ref 7
Emerging evidence has shown that cell-cell interactions between testicular cells, in particular at the Sertoli cell-cell and Sertoli-germ cell interface, are crucial to support spermatogenesis. The unique ultrastructures that support cell-cell interactions in the testis are the basal ES (ectoplasmic specialization) and the apical ES. The basal ES is found between adjacent Sertoli cells near the basement membrane that also constitute the blood-testis barrier (BTB). The apical ES is restrictively expressed at the Sertoli-spermatid contact site in the apical (adluminal) compartment of the seminiferous epithelium. These ultrastructures are present in both rodent and human testes, but the majority of studies found in the literature were done in rodent testes. As such, our discussion herein, unless otherwise specified, is focused on studies in testes of adult rats. Studies have shown that the testicular cell-cell interactions crucial to support spermatogenesis are mediated through distinctive signaling proteins and pathways, most notably involving FAK, Akt1/2 and Cdc42 GTPase. Thus, manipulation of some of these signaling proteins, such as FAK, through the use of phosphomimetic mutants for overexpression in Sertoli cell epithelium in vitro or in the testis in vivo, making FAK either constitutively active or inactive, we can modify the outcome of spermatogenesis. For instance, using the toxicant-induced Sertoli cell or testis injury in rats as study models, we can either block or rescue toxicant-induced infertility through overexpression of p-FAK-Y397 or p-FAK-Y407 (and their mutants), including the use of specific activator(s) of the involved signaling proteins against pAkt1/2. These findings thus illustrate that a potential therapeutic approach can be developed to manage toxicant-induced male reproductive dysfunction. In this review, we critically evaluate these recent findings, highlighting the direction for future investigations by bringing the laboratory-based research through a translation path to clinical investigations.
This paper does not relate to the statement it is meant to support by the review authors.
Ref 35
The review by Qin et al (1) includes 5 trials none of which should have been included in a quality metaanalysis as the methodology was unconvincing: In the trial by Alraek et al., patients were randomised to receive either acupuncture or no treatment. This means that no attempt was made to control for the effects of placebo or extra attention. Therefore, this study does not demonstrate an effect of acupuncture as the outcome could be due to non-specific effects unrelated with this therapy. By contrast, the trial by Aune et al. did attempt to control for placebo effects by using a sham control group. Sham acupuncture was given using six needles superficially inserted in the calves, thighs or abdomen outside known acupuncture points or meridians. Needles were not manipulated in the sham group. Sham or placebo controls have the purpose of rendering patients unaware of whether they receive the real or the sham treatment. The method used here cannot achieve this aim; patients would be easily able to tell which intervention they received. In other words, this study also did not adequately control for placebo effects. The remaining three trials are all not Medline-listed, authored by Chinese investigators and published in inaccessible journals. This should disqualify them from inclusion as they were unverifiable by the peer review process. According to the published table, they were equivalence trials of acupuncture versus antibiotics with a sample size around 30. This means they are grossly underpowered and thus unable to generate reliable results. Unless BJOG peer reviewers could see the primary articles, or be provided with translations from Chinese, the systematic review should not have been accepted. The “many eyes of science” requires transparency, testing, challenge and verification. Although in the past, inconclusive results of acupuncture have not been thought to be due to Chinese influence (2), it has been noted that virtually all recent published acupuncture trials are “positive” (3), raising questions of publication and other biases. Our colleagues are under tremendous pressure to publish, but we do them no favours by effectively lowering the standard of scientific peer review. Elite journals too have an obligation to train and reiterate about publication ethics and sound scientific writing (4). As none of the primary studies convincingly demonstrated that acupuncture is an effective therapy for recurrent urinary tract infections, no positive conclusion was warranted. Although Qin et al. did state that the risk of bias of the included trials was generally high or unclear (1), the BJOG nevertheless allowed them to turn massive uncertainty into relatively firm, positive conclusions in the abstract (“Acupuncture appeared to be beneficial for treatment and prophylaxis of rUTIs”) and tweetable abstract (“This review found that acupuncture may improve treatment and prevent recurrence of urinary tract infection in women”), thus leading to excited media headlines that inevitably mislead the public. ‘May’ is a weasel word which should be avoided as it is unfalsifiable (for example, pigs do not fly but they ‘may’ fly in the future). The definite, straightforward conclusion must be “There is no good evidence to support the use of acupuncture for the treatment and prophylaxis of recurrent UTIs”. It is not acceptable to give international credibility to an implausible modality that no objective, independent high-quality review has found effective beyond placebo (5). The dampening accompanying mini-commentary (6) does not undo the damage.
The review should be withdrawn while the primary papers are translated for peer reviewers to examine, the above limitations discussed in the text, and the positive ‘spin’ in conclusions corrected. These improvements would consolidate the researchers’ probity and justify the accolade of BJOG publication.
Our letter to the editor does not bear any relation to the statement it is meant to support by the review authors.
Ref 36
In this first prospective, randomized, single-blind, placebo-controlled study, 28 infertile patients with severe oligoasthenozoospermia received acupuncture according to the principles of traditional Chinese medicine (TCM) and 29 infertile patients received placebo acupuncture. A significantly higher percentage of motile sperm (World Health Organization categories A–C), but no effect on sperm concentration, was found after acupuncture compared with placebo acupuncture.
This small study is far from convincing and does not lend itself to far-reaching conclusions
Ref 37
Of the 279 cases of male sterility treated by the combination of acupuncture, pilose antler
essence injection to acupoints and oral administration of Chinese materia medica, 142
cases (47.8%) were cured, 81 cases (27.3%) markedly effective, 53 cases (17.8%) effective
and 21 cases (7.1%) ineffective. The therapeutic effect of the combination of these three
treatments was satisfactory.
This study had no control group and used two different therapies. Therefore, it does not allow any conclusion about the effectiveness of acupuncture.
____________________
Perhaps you feel that these errors are trivial. But I would disagree. The review authors’ praise of acupuncture for MI is misplaced and will mislead the public. There are plenty of reviews on the subject, and those that are not overtly biased arrive at conclusions like these:
- The current evidence on acupuncture for oligoasthenozoospermia is inadequate to draw a solid conclusion due to the poor methodological quality. Rigorous full-scale RCTs are needed to validate the therapeutic efficacy and safety of acupuncture in treating oligoasthenozoospermia.
- The current evidence showing that acupuncture might improve poor semen quality is insufficient because of the small number of studies, inadequacy of procedures and/or insufficient information for semen analysis, high levels of heterogeneity, high risk of bias, and poor quality of reporting. Further large, well-designed RCTs are required.
So, how did this sloppy review come about?
Its authors are affiliated to the TCM Regulating Metabolic Diseases Key Laboratory of Sichuan Province, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu 610072, China, and the Tea Research Institute, Sichuan Academy of Agricultural Sciences, Chengdu 610066, China. A footnote tells us that their review was supported by the National Natural Science Foundation of China [No. 81973647] and the Xinglin scholar discipline promotion talent program of Chengdu University of traditional Chinese medicine [No. BSH2021018]. This sounds respectable enough.
The journal that published the review is ‘Pharmacological Research – Modern Chinese Medicine‘. Its stated aims are as follows: The journal publishes articles reporting on advances in our comprehension of mechanism and safety in experimental pharmacology and clinical efficacy and safety of pharmacologically active substances, including compound prescriptions, utilized in Traditional Chinese Medicine applying modern scientific research methods. Studies reporting also on the mechanisms of actions of the active substance(s) investigated are encouraged.
The editors in chief of the journal are Guan-Hua Du, PhD, China Academy of Chinese Medical Sciences Institute of Chinese Materia Medica, Beijing, China and Emilio Clementi, M.Mus, MD, PhD, University of Milan, Milan, Italy. No doubt, these are respectable scientists. And because they are, they should make sure that what they publish is correct – a criterion this recent review clearly does not meet.
Many chiropractors seem to view the present pandemic as a business opportunity and make no end of false claims to attract customers. This has now been outlawed in the US. Medscape reported that a US district court will decide whether a chiropractor who is charged with 10 counts of making false marketing claims related to COVID-19 will be the first person convicted under a new federal law.
On his website, chiropractor ‘Dr.’ Eric Neptune advertises his services as follows:
Have you ever been told by your medical doctor that you or a member of your family had a specific disease, syndrome, or sickness? Did your doctor then recommend a drug or surgery to fix the issue, or tell you that you would have to live with it for the rest of your life? If so, you are not alone!
Nepute Wellness Center is unlike any medical clinic you may have been to. The clinic team is focused on finding and fixing the CAUSE of your problem vs. seeking out and treating only the SYMPTOMS. Nepute Wellness Center is equipped with state-of-the-art diagnostic equipment and testing, as well as medical doctors, nurses, and chiropractors who have been uniquely trained to treat your whole body, regardless of age, and return your body to a healthy balance so that it can heal itself the way God intended.
If you are tired of trying to treat your symptoms using prescription and over-the-counter pills, or even considering surgery, then Nepute Wellness Center may be right for you! Or like many, you want to be proactive with your health and prevent sickness and disease before you begin to suffer any symptoms, allowing you to live the full life you deserve, then make Nepute Wellness Center your partner in health!
Already over a year ago, Eric Nepute, the owner of Quickwork, based in St. Louis, Missouri, managed to make headlines. He had recorded a video that racked up more than 21 million views and suggested that drinking tonic water would prevent COVID-19 infections. Now, Mr. Neptune is the first person charged by the Federal Trade Commission (FTC) under the new COVID- 19 Consumer Protection Act. His company which has several locations in St. Louis County advertised its vitamin D and zinc products on social media and the internet as drugs that could treat or prevent COVID-19 claiming that their products are “more effective than the available COVID-19 vaccines”.
The FTC warned Nepute’s company in May 2020 about making unsubstantiated claims for other products regarding efficacy against COVID-19 and advised him to immediately stop making claims that were not supported by scientific evidence. However, Nepute seemed undeterred.
The FTC is seeking to fine Nepute and Quickwork up to US$43,792 for each violation of the COVID-19 Consumer Protection Act. In addition, the FTC seeks to bar the company from making health claims unless they are true and can be substantiated by scientific evidence.
Through his attorney, Neptune told the local NBC TV news affiliate, “I feel that I have not done anything wrong. I encourage everyone to live a healthy lifestyle during this unprecedented time. My attorneys are reviewing the complaint and I have no further comments at this time.”
I have become used to lamentably poor research in the realm of SCAM, particularly homeopathy. Thus, there is little that can amaze me these days; at least this is what I had thought. But this paper is an exception. The new trial is entitled ‘ETHICAL CLINICAL TRIAL OF LESSER KNOWN HOMEOPATHIC REMEDIES IN INFERTILITY IN FEMALES’, and it is truly outstanding. Here is the abstract:
Background & Objective: Homoeopathy with time honoured results, has a great number of cured cases of infertility, but without much evidence. So, it is imperative to show scientifically the scope of homoeopathy in treating infertility cases. Materials and Methodology: 7 lesser known medicines (Alteris farinosa, Janosia Ashoka, Viburnum opulus, Euphonium, Ustilago, Bacillus sycocuss, Bacillus morgan) were prescribed to the sample size (n=23), at the project site O.P.D/I.P.D. of Homoeopathy university, Saipura, Jaipur and Dr Madan Pratap Khunteta Homoeopathic Medical College, Hospital & Research Centre, Station Road, Jaipur & its extension O.P.D.’s. for study within 12 months. Result-In the present study 7 (30.43%) patients were prescribed Janosia Ashoka amongst whom 2(28.57%) showed marked improvement, while 5(71.43%) remained in the state of status quo. Conclusion- Study has shown encouraging and effective treatment in infertility in females.
It does not tell us much; therefore, let me copy several crucial passages from the paper itself:
Objectives of the study-
- To study the efficacy of homoeopathic medicines in the treatment of infertility in females.
- To enhance the knowledge of materia medica in cases of infertility in females.
Material and Methodology-
The study was conducted at O.P.D./I.P.D.of Homoeopathy University, Saipura, Sanganer and Dr M.P.K. Homoeopathic Medical College &Research Centre, Station Road, Jaipur from 2010 to 2013 for a total period of 3 Years. A sample size of n=23 and 7 lesser known remedies were selected for the studies.
Result-
Inferences- Based on clinical symptoms and pathological investigations. It was inferred that out of 23 patients taken for study, 2 (8.69%) patients showed marked improvement, while 21 (91.31%) patients remained in the state of status quo.
_________________________________________________
No, I am not kidding you. There is no further relevant information about the trial methodology nor about the results. Therefore, I feel unable to even criticise this study; it is even too awful for a critique.
As I said: outstanding!
And all this could be quite funny – except, of course, some nutter will undoubtedly use this paper for claiming that there is evidence for homeopathy to efficiently treat female infertility.
You have to be a homeopath to call this an ethical trial!