pain
In this study, the impact of a multimodal integrative oncology pre- and intraoperative intervention on pain and anxiety among patients undergoing gynecological oncology surgery was explored.
Study participants were randomized into three groups:
- Group A received preoperative touch/relaxation techniques, followed by intraoperative acupuncture, plus standard care;
- Group B received preoperative touch/relaxation only, plus standard care;
- Group C (the control group) received standard care.
Pain and anxiety were scored before and after surgery using the Measure Yourself Concerns and Wellbeing (MYCAW) and Quality of Recovery (QOR-15) questionnaires, using Part B of the QOR to assess pain, anxiety, and other quality-of-life parameters.
A total of 99 patients participated in the study: 45 in Group A, 25 in Group B, and 29 in Group C. The three groups had similar baseline demographic and surgery-related characteristics. Postoperative QOR-Part B scores were significantly higher in the treatment groups (A and B) when compared with controls (p = .005), including for severe pain (p = .011) and anxiety (p = .007). Between-group improvement for severe pain was observed in Group A compared with controls (p = .011). Within-group improvement for QOR depression subscales was observed in only the intervention groups (p <0.0001). Compared with Group B, Group A had better improvement of MYCAW-reported concerns (p = .025).
The authors concluded that a preoperative touch/relaxation intervention may significantly reduce postoperative anxiety, possibly depression, in patients undergoing gynecological oncology surgery. The addition of intraoperative acupuncture significantly reduced severe pain when compared with controls. Further research is needed to confirm these findings and better understand the impact of intraoperative acupuncture on postoperative pain.
Regular readers of my blog know only too well what I am going to say about this study.
Imagine you have a basket full of apples and your friend has the same plus a basket full of pears. Who do you think has more fruit?
Dumb question, you say?
Correct!
Just as dumb, it seems, as this study: therapy A and therapy B will always generate better outcomes than therapy B alone. But that does not mean that therapy A per se is effective. Because therapy A generates a placebo effect, it might just be that it has no effect beyond placebo. And that acupuncture can generate placebo effects has been known for a very long time; to verify this we need no RCT.
As I have so often pointed out, the A+B versus B study design never generates a negative finding.
This is, I fear, precisely the reason why this design is so popular in so-called alternative medicine (SCAM)! It enables promoters of SCAM (who are not as dumb as the studies they conduct) to pretend they are scientists testing their therapies in rigorous RCTs.
The most disappointing thing about all this is perhaps that more and more top journals play along with this scheme to mislead the public!
This meta-analysis of randomized clinical trials (RCTs) was aimed at evaluating the effects of massage therapy in the treatment of postoperative pain.
Three databases (PubMed, Embase, and Cochrane Central Register of Controlled Trials) were searched for RCTs published from database inception through January 26, 2021. The primary outcome was pain relief. The quality of RCTs was appraised with the Cochrane Collaboration risk of bias tool. The random-effect model was used to calculate the effect sizes and standardized mean difference (SMD) with 95% confidential intervals (CIs) as a summary effect. The heterogeneity test was conducted through I2. Subgroup and sensitivity analyses were used to explore the source of heterogeneity. Possible publication bias was assessed using visual inspection of funnel plot asymmetry.
The analysis included 33 RCTs and showed that MT is effective in reducing postoperative pain (SMD, -1.32; 95% CI, −2.01 to −0.63; p = 0.0002; I2 = 98.67%). A similarly positive effect was found for both short (immediate assessment) and long terms (assessment performed 4 to 6 weeks after the MT). Neither the duration per session nor the dose had a significant impact on the effect of MT, and there was no difference in the effects of different MT types. In addition, MT seemed to be more effective for adults. Furthermore, MT had better analgesic effects on cesarean section and heart surgery than orthopedic surgery.
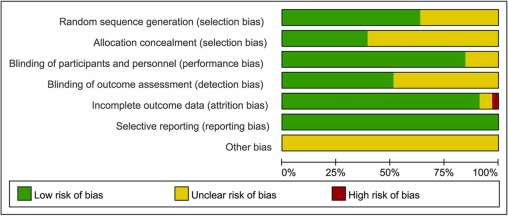
The authors concluded that MT may be effective for postoperative pain relief. We also found a high level of heterogeneity among existing studies, most of which were compromised in the methodological quality. Thus, more high-quality RCTs with a low risk of bias, longer follow-up, and a sufficient sample size are needed to demonstrate the true usefulness of MT.
The authors discuss that publication bias might be possible due to the exclusion of all studies not published in English. Additionally, the included RCTs were extremely heterogeneous. None of the included studies was double-blind (which is, of course, not easy to do for MT). There was evidence of publication bias in the included data. In addition, there is no uniform evaluation standard for the operation level of massage practitioners, which may lead to research implementation bias.
Patients who have just had an operation and are in pain are usually thankful for the attention provided by carers. It might thus not matter whether it is provided by a massage or other therapist. The question is: does it matter? For the patient, it probably doesn’t; However, for making progress, it does, in my view.
In the end, we have to realize that, with clinical trials of certain treatments, scientific rigor can reach its limits. It is not possible to conduct double-blind, placebo-controlled studies of MT. Thus we can only conclude that, for some indications, massage seems to be helpful (and almost free of adverse effects).
This is also the conclusion that has been drawn long ago in some countries. In Germany, for instance, where I trained and practiced in my younger years, Swedish massage therapy has always been an accepted, conventional form of treatment (while exotic or alternative versions of massage therapy had no place in routine care). And in Vienna where I was chair of rehab medicine I employed about 8 massage therapists in my department.
Hypericum perforatum (St John’s wort) is often recommended as a remedy to relieve pain caused by nerve damage. This trial investigated whether homeopathic Hypericum leads to a reduction in postoperative pain and a decrease in pain medication compared with placebo.
The study was designed as a randomized double-blind, monocentric, placebo-controlled clinical trial with inpatients undergoing surgery for lumbar sequestrectomy. Homeopathic treatment was compared to placebo, both in addition to usual pain management. The primary endpoint was pain relief measured with a visual analog scale. Secondary endpoints were the reduction of inpatient postoperative analgesic medication and change in sensory and affective pain perception.
The results show that the change in pain perception between baseline and day 3 did not significantly differ between the study arms. With respect to pain medication, total morphine equivalent doses did not differ significantly. However, a statistical trend and a moderate effect (d = 0.432) in the decrease of pain medication consumption in favor of the Hypericum group was observed.
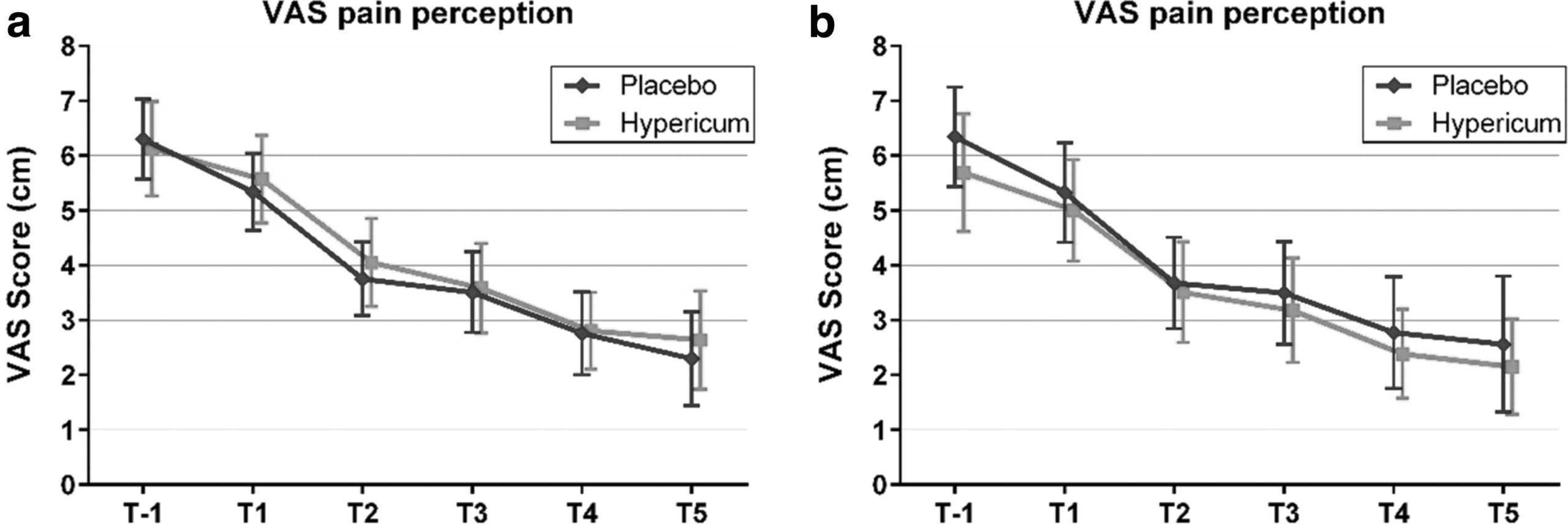
The authors concluded that this is the first trial of homeopathy that evaluated the efficacy of Hypericum C200 after lumbar monosegmental spinal sequestrectomy. Although no significant differences between the groups could be shown, we found that patients who took potentiated Hypericum in addition to usual pain management showed lower consumption of analgesics. Further investigations, especially with regard to pain medication, should follow to better classify the described analgesic reduction.
For a number of reasons, this is a remarkably mysterious and quite hilarious study:
- Hypericum is recommended as an analgesic for neuropathic pain.
- According to the ‘like cures like’ axiom of homeopathy, it therefore must increase pain in such situations.
- Yet, the authors of this trial mounted an RCT to see whether it reduces pain.
- Thus they either do not understand homeopathy or wanted to sabotage it.
- As they are well-known pro-homeopathy researchers affiliated with a university that promotes homeopathy (Witten/Herdecke University, Herdecke, Germany), both explanations are highly implausible.
- The facts that the paper was published in a pro-SCAM journal (J Integr Complement Med), and the study was sponsored by the largest German firm of homeopathics (Deutsche Homoeopathische Union) renders all this even more puzzling.
- However, these biases do explain that the authors do their very best to mislead us by including some unwarranted ‘positive’ findings in their overall conclusions.
In the end, none of this matters, because the results of the study reveal that firstly the homeopathic ‘law of similars’ is nonsense, and secondly one homeopathic placebo (i.e. Hypericum C200) produces exactly the same outcomes as another, non-homeopathic placebo.
Osteopathy is currently regulated in 12 European countries: Cyprus, Denmark, Finland, France, Iceland, Italy, Liechtenstein, Luxembourg, Malta, Portugal, Switzerland, and the UK. Other countries such as Belgium and Norway have not fully regulated it. In Austria, osteopathy is not recognized or regulated. The Osteopathic Practitioners Estimates and RAtes (OPERA) project was developed as a Europe-based survey, whereby an updated profile of osteopaths not only provides new data for Austria but also allows comparisons with other European countries.
A voluntary, online-based, closed-ended survey was distributed across Austria in the period between April and August 2020. The original English OPERA questionnaire, composed of 52 questions in seven sections, was translated into German and adapted to the Austrian situation. Recruitment was performed through social media and an e-based campaign.
The survey was completed by 338 individuals (response rate ~26%), of which 239 (71%) were female. The median age of the responders was 40–49 years. Almost all had preliminary healthcare training, mainly in physiotherapy (72%). The majority of respondents were self-employed (88%) and working as sole practitioners (54%). The median number of consultations per week was 21–25 and the majority of respondents scheduled 46–60 minutes for each consultation (69%).
The most commonly used diagnostic techniques were: palpation of position/structure, palpation of tenderness, and visual inspection. The most commonly used treatment techniques were cranial, visceral, and articulatory/mobilization techniques. The majority of patients estimated by respondents consulted an osteopath for musculoskeletal complaints mainly localized in the lumbar and cervical region. Although the majority of respondents experienced a strong osteopathic identity, only a small proportion (17%) advertise themselves exclusively as osteopaths.
The authors concluded that this study represents the first published document to determine the characteristics of the osteopathic practitioners in Austria using large, national data. It provides new information on where, how, and by whom osteopathic care is delivered. The information provided may contribute to the evidence used by stakeholders and policy makers for the future regulation of the profession in Austria.
This paper reveals several findings that are, I think, noteworthy:
- Visceral osteopathy was used often or very often by 84% of the osteopaths.
- Muscle energy techniques were used often or very often by 53% of the osteopaths.
- Techniques applied to the breasts were used by 59% of the osteopaths.
- Vaginal techniques were used by 49% of the osteopaths.
- Rectal techniques were used by 39% of the osteopaths.
- “Taping/kinesiology tape” was used by 40% of osteopaths.
- Applied kinesiology was used by 17% of osteopaths and was by far the most-used diagnostic approach.
Perhaps the most worrying finding of the entire paper is summarized in this sentence: “Informed consent for oral techniques was requested only by 10.4% of respondents, and for genital and rectal techniques by 21.0% and 18.3% respectively.”
I am lost for words!
I fail to understand what meaningful medical purpose the fingers of an osteopath are supposed to have in a patient’s vagina or rectum. Surely, putting them there is a gross violation of medical ethics.
Considering these points, I find it impossible not to conclude that far too many Austrian osteopaths practice treatments that are implausible, unproven, potentially harmful, unethical, and illegal. If patients had the courage to take action, many of these charlatans would probably spend some time in jail.
Is acupuncture more than a theatrical placebo? Acupuncture fans are convinced that the answer to this question is YES. Perhaps this paper will make them think again.
A new analysis mapped the systematic reviews, conclusions, and certainty or quality of evidence for outcomes of acupuncture as a treatment for adult health conditions. Computerized search of PubMed and 4 other databases from 2013 to 2021. Systematic reviews of acupuncture (whole body, auricular, or electroacupuncture) for adult health conditions that formally rated the certainty, quality, or strength of evidence for conclusions. Studies of acupressure, fire acupuncture, laser acupuncture, or traditional Chinese medicine without mention of acupuncture were excluded. Health condition, number of included studies, type of acupuncture, type of comparison group, conclusions, and certainty or quality of evidence. Reviews with at least 1 conclusion rated as high-certainty evidence, reviews with at least 1 conclusion rated as moderate-certainty evidence and reviews with all conclusions rated as low- or very low-certainty evidence; full list of all conclusions and certainty of evidence.
A total of 434 systematic reviews of acupuncture for adult health conditions were found; of these, 127 reviews used a formal method to rate the certainty or quality of evidence of their conclusions, and 82 reviews were mapped, covering 56 health conditions. Across these, there were 4 conclusions that were rated as high-certainty evidence and 31 conclusions that were rated as moderate-certainty evidence. All remaining conclusions (>60) were rated as low- or very low-certainty evidence. Approximately 10% of conclusions rated as high or moderate-certainty were that acupuncture was no better than the comparator treatment, and approximately 75% of high- or moderate-certainty evidence conclusions were about acupuncture compared with a sham or no treatment.
Three evidence maps (pain, mental conditions, and other conditions) are shown below
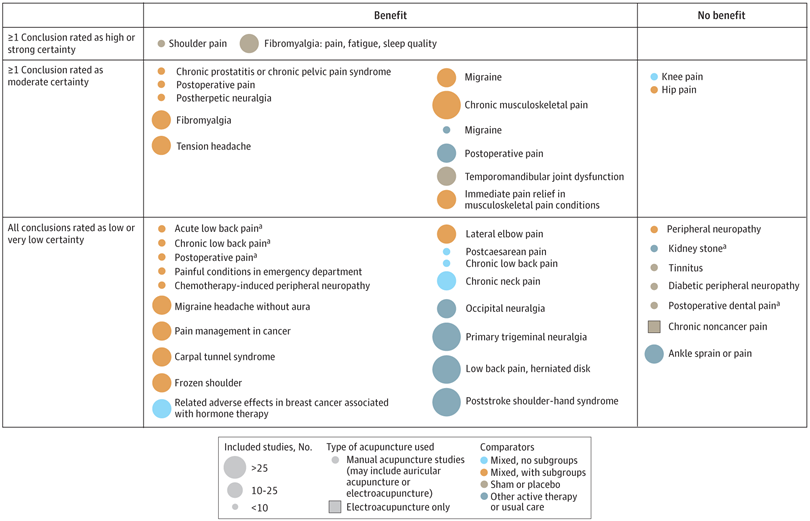
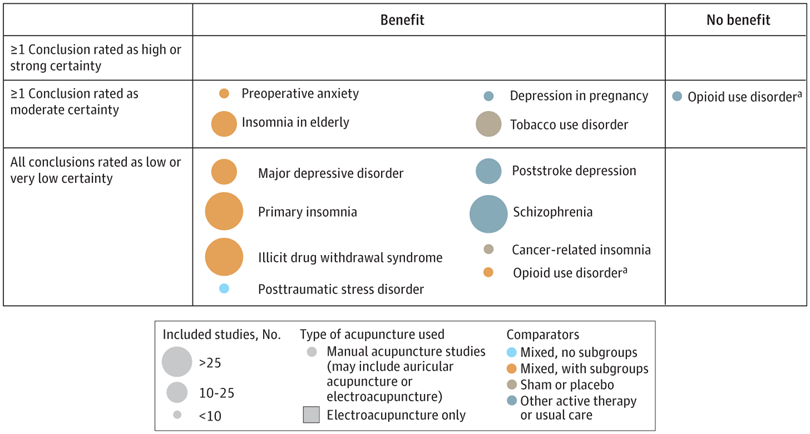

The authors concluded that despite a vast number of randomized trials, systematic reviews of acupuncture for adult health conditions have rated only a minority of conclusions as high- or moderate-certainty evidence, and most of these were about comparisons with sham treatment or had conclusions of no benefit of acupuncture. Conclusions with moderate or high-certainty evidence that acupuncture is superior to other active therapies were rare.
These findings are sobering for those who had hoped that acupuncture might be effective for a range of conditions. Despite the fact that, during recent years, there have been numerous systematic reviews, the evidence remains negative or flimsy. As 34 reviews originate from China, and as we know about the notorious unreliability of Chinese acupuncture research, this overall result is probably even more negative than the authors make it out to be.
Considering such findings, some people (including the authors of this analysis) feel that we now need more and better acupuncture trials. Yet I wonder whether this is the right approach. Would it not be better to call it a day, concede that acupuncture generates no or only relatively minor effects, and focus our efforts on more promising subjects?
The Sunday Times reported yesterday reported that five NHS trusts currently offer moxibustion to women in childbirth for breech babies, i.e. babies presenting upside down. Moxibustion is a form of Traditional Chinese Medicine (TCM) where mugwort is burned close to acupuncture points. The idea is that this procedure would stimulate the acupuncture point similar to the more common way using needle insertion. The fifth toe is viewed as the best traditional acupuncture point for breech presentation, and the treatment is said to turn the baby in the uterus so that it can be delivered more easily.
At least four NHS trusts are offering acupuncture and reflexology with aromatherapy to help women with delayed pregnancies, while 15 NHS trusts offer hypnobirthing classes. Some women are asked to pay fees of up to £140 for it. These treatments are supposed to relax the mother in the hope that this will speed up the process of childbirth.
The Nice guidelines on maternity care say the NHS should not offer acupuncture, acupressure, or hypnosis unless specifically requested by women. The reason for the Nice warning is simple: there is no convincing evidence that these therapies are effective.
Campaigner Catherine Roy who compiled the list of treatments said: “To one degree or another, the Royal College of Midwives, the Care Quality Commission and parts of the NHS support these pseudoscientific treatments.
“They are seen as innocuous but they carry risks, can delay medical help and participate in an anti-medicalisation stance specific to ‘normal birth’ ideology and maternity care. Nice guidelines are clear that they should not be offered by clinicians for treatment. NHS England must ensure that pseudoscience and non-evidence based treatments are removed from NHS maternity care.”
Birte Harlev-Lam, executive director of the Royal College of Midwives (RCM), said: “We want every woman to have as positive an experience during pregnancy, labour, birth and the postnatal period as possible — and, most importantly, we want that experience to be safe. That is why we recommend all maternity services to follow Nice guidance and for midwives to practise in line with the code set out by the Nursing and Midwifery Council.”
A spokeswoman for Nice said it was reviewing its maternity guidelines. NHS national clinical director for maternity and women’s health, Dr Matthew Jolly, said: “All NHS services are expected to offer safe and personalised clinical care and local NHS areas should commission core maternity services using the latest NICE and clinical guidance. NHS trusts are under no obligation to provide complementary or alternative therapies on top of evidence-based clinical care, but where they do in response to the wishes of mothers it is vital that the highest standards of safety are maintained.”
On this blog, we have repeatedly discussed the strange love affair of midwives with so-called alternative medicine (SCAM), for instance, here. In 2012, we published a summary of 19 surveys on the subject. It showed that the prevalence of SCAM use varied but was often close to 100%. Much of it did not seem to be supported by strong evidence for efficacy. We concluded that most midwives seem to use SCAM. As not all SCAMs are without risks, the issue should be debated openly. Today, there is plenty more evidence to show that the advice of midwives regarding SCAM is not just not evidence-based but also often dangerous. This, of course, begs the question: when will the professional organizations of midwifery do something about it?
This double-blind, randomized study assessed the effectiveness of physiotherapy instrument mobilization (PIM) in patients with low back pain (LBP) and compared it with the effectiveness of manual mobilization.
Thirty-two participants with LBP were randomly assigned to one of two groups:
- The PIM group received lumbar mobilization using an activator instrument, stabilization exercises, and education.
- The manual group received lumbar mobilization using a pisiform grip, stabilization exercises, and education.
Both groups had 4 treatment sessions over 2-3 weeks. The following outcomes were measured before the intervention, and after the first and fourth sessions:
- Numeric Pain Rating Scale (NPRS),
- Oswestry Disability Index (ODI) scale,
- Pressure pain threshold (PPT),
- lumbar spine range of motion (ROM),
- lumbar multifidus muscle activation.
There were no differences between the PIM and manual groups in any outcome measures. However, over the period of study, there were improvements in both groups in NPRS (PIM: 3.23, Manual: 3.64 points), ODI (PIM: 17.34%, Manual: 14.23%), PPT (PIM: ⩽ 1.25, Manual: ⩽ 0.85 kg.cm2), lumbar spine ROM (PIM: ⩽ 9.49∘, Manual: ⩽ 0.88∘), and/or lumbar multifidus muscle activation (percentage thickness change: PIM: ⩽ 4.71, Manual: ⩽ 4.74 cm; activation ratio: PIM: ⩽ 1.17, Manual: ⩽ 1.15 cm).
The authors concluded that both methods of lumbar spine mobilization demonstrated comparable improvements in pain and disability in patients with LBP, with neither method exhibiting superiority over the other.
If this conclusion is meant to tell us that both treatments were equally effective, I beg to differ. The improvements documented here are consistent with improvements caused by the natural history of the condition, regression towards the mean, and placebo effects. The data do not prove that they are due to the treatments. On the contrary, they seem to imply that patients get better no matter what therapy is used. Thus, I feel that the results are entirely in keeping with the hypothesis that spinal mobilization is a placebo treatment.
So, allow me to re-phrase the authors’ conclusion as follows:
Lumbar mobilizations do not seem to have specific therapeutic effects and might therefore be considered to be ineffective for LBP.
Acupuncture is emerging as a potential therapy for relieving pain, but the effectiveness of acupuncture for relieving low back and/or pelvic pain (LBPP) during pregnancy remains controversial. This meta-analysis aimed to investigate the effects of acupuncture on pain, functional status, and quality of life for women with LBPP pain during pregnancy.
The authors included all RCTs evaluating the effects of acupuncture on LBPP during pregnancy. Data extraction and study quality assessments were independently performed by three reviewers. The mean differences (MDs) with 95% CIs for pooled data were calculated. The primary outcomes were pain, functional status, and quality of life. The secondary outcomes were overall effects (a questionnaire at a post-treatment visit within a week after the last treatment to determine the number of people who received good or excellent help), analgesic consumption, Apgar scores >7 at 5 min, adverse events, gestational age at birth, induction of labor and mode of birth.
Ten studies, reporting on a total of 1040 women, were included. Overall, acupuncture
- relieved pain during pregnancy (MD=1.70, 95% CI: (0.95 to 2.45), p<0.00001, I2=90%),
- improved functional status (MD=12.44, 95% CI: (3.32 to 21.55), p=0.007, I2=94%),
- improved quality of life (MD=−8.89, 95% CI: (−11.90 to –5.88), p<0.00001, I2 = 57%).
There was a significant difference in overall effects (OR=0.13, 95% CI: (0.07 to 0.23), p<0.00001, I2 = 7%). However, there was no significant difference in analgesic consumption during the study period (OR=2.49, 95% CI: (0.08 to 80.25), p=0.61, I2=61%) and Apgar scores of newborns (OR=1.02, 95% CI: (0.37 to 2.83), p=0.97, I2 = 0%). Preterm birth from acupuncture during the study period was reported in two studies. Although preterm contractions were reported in two studies, all infants were in good health at birth. In terms of gestational age at birth, induction of labor, and mode of birth, only one study reported the gestational age at birth (mean gestation 40 weeks).
The authors concluded that acupuncture significantly improved pain, functional status and quality of life in women with LBPP during the pregnancy. Additionally, acupuncture had no observable severe adverse influences on the newborns. More large-scale and well-designed RCTs are still needed to further confirm these results.
What should we make of this paper? 
In case you are in a hurry: NOT A LOT!
In case you need more, here are a few points:
- many trials were of poor quality;
- there was evidence of publication bias;
- there was considerable heterogeneity within the studies.
The most important issue is one studiously avoided in the paper: the treatment of the control groups. One has to dig deep into this paper to find that the control groups could be treated with “other treatments, no intervention, and placebo acupuncture”. Trials comparing acupuncture combined plus other treatments with other treatments were also considered to be eligible. In other words, the analyses included studies that compared acupuncture to no treatment at all as well as studies that followed the infamous ‘A+Bversus B’ design. Seven studies used no intervention or standard of care in the control group thus not controlling for placebo effects.
Nobody can thus be in the slightest surprised that the overall result of the meta-analysis was positive – false positive, that is! And the worst is that this glaring limitation was not discussed as a feature that prevents firm conclusions.
Dishonest researchers?
Biased reviewers?
Incompetent editors?
Truly unbelievable!!!
In consideration of these points, let me rephrase the conclusions:
The well-documented placebo (and other non-specific) effects of aacupuncture improved pain, functional status and quality of life in women with LBPP during the pregnancy. Unsurprisingly, acupuncture had no observable severe adverse influences on the newborns. More large-scale and well-designed RCTs are not needed to further confirm these results.
PS
I find it exasperating to see that more and more (formerly) reputable journals are misleading us with such rubbish!!!
The aim of this evaluator-blinded randomized clinical trial was to determine if manual therapy added to a therapeutic exercise program produced greater improvements than a sham manual therapy added to the same exercise program in patients with non-specific shoulder pain. 
Forty-five subjects were randomly allocated into one of three groups:
- manual therapy (glenohumeral mobilization technique and rib-cage technique);
- thoracic sham manual therapy (glenohumeral mobilization technique and rib-cage sham technique);
- sham manual therapy (sham glenohumeral mobilization technique and rib-cage sham technique).
All groups also received a therapeutic exercise program. Pain intensity, disability, and pain-free active shoulder range of motion were measured post-treatment and at 4-week and 12-week follow-ups. Mixed-model analyses of variance and post hoc pairwise comparisons with Bonferroni corrections were constructed for the analysis of the outcome measures.
All groups reported improved pain intensity, disability, and pain-free active shoulder range of motion. However, there were no between-group differences in these outcome measures.
The authors concluded that the addition of the manual therapy techniques applied in the present study to a therapeutic exercise protocol did not seem to add benefits to the management of subjects with non-specific shoulder pain.
What does that mean?
I think it means that the improvements observed in this study were due to 1) exercise and 2) a range of non-specific effects, and that they were not due to the manual techniques tested.
I cannot say that I find this enormously surprising. But I would also find it unsurprising if fans of these methods would claim that the results show that the physios applied the techniques not correctly.
In any case, I feel this is an interesting study, not least because of its use of sham therapy. But I somehow doubt that the patients were unable to distinguish sham from verum. If so, the study was not patient-blind which obviously is difficult to achieve with manual treatments.
This systematic review, meta-analysis, and meta-regression investigated the effects of individualized interventions, based on exercise alone or combined with psychological treatment, on pain intensity and disability in patients with chronic non-specific low-back pain.
Databases were searched up to January 31, 2022, to retrieve respective randomized clinical trials of individualized and/or personalized and/or stratified exercise interventions with or without psychological treatment compared to any control.
The findings show:
- Fifty-eight studies (n = 10084) were included. At short-term follow-up (12 weeks), low-certainty evidence for pain intensity (SMD -0.28 [95%CI -0.42 to -0.14]) and very low-certainty evidence for disability (-0.17 [-0.31 to -0.02]) indicates superior effects of individualized versus active exercises, and very low-certainty evidence for pain intensity (-0.40; [-0.58 to -0.22])), but not (low-certainty evidence) for disability (-0.18; [-0.22 to 0.01]) compared to passive controls.
- At long-term follow-up (1 year), moderate-certainty evidence for pain intensity (-0.14 [-0.22 to -0.07]) and disability (-0.20 [-0.30 to -0.10]) indicates effects versus passive controls.
Sensitivity analyses indicate that the effects on pain, but not on disability (always short-term and versus active treatments) were robust. Pain reduction caused by individualized exercise treatments in combination with psychological interventions (in particular behavioral-cognitive therapies) (-0.28 [-0.42 to -0.14], low certainty) is of clinical importance.
The certainty of the evidence was downgraded mainly due to evidence of risk of bias, publication bias, and inconsistency that could not be explained. Individualized exercise can treat pain and disability in chronic non-specific low-back pain. The effects in the short term are of clinical importance (relative differences versus active 38% and versus passive interventions 77%), especially in regard to the little extra effort to individualize exercise. Sub-group analysis suggests a combination of individualized exercise (especially motor-control-based treatments) with behavioral therapy interventions to boost effects.
The authors concluded that the relative benefit of individualized exercise therapy on chronic low back pain compared to other active treatments is approximately 38% which is of clinical importance. Still, sustainability of effects (> 12 months) is doubtable. As individualization in exercise therapies is easy to implement, its use should be considered.
Johannes Fleckenstein, the 1st author from the Goethe-University Frankfurt, Institute of Sports Sciences, Department of Sports Medicine and Exercise Physiology, sees in the study “an urgent health policy appeal” to strengthen combined services in care and remuneration. “Compared to other countries, such as the USA, we are in a relatively good position in Germany. For example, we have a lower prescription of strong narcotics such as opiates. But the rate of unnecessary X-ray examinations, which incidentally can also contribute to the chronicity of pain, or inaccurate surgical indications is still very high.”
Personally, I find the findings of this paper rather unsurprising. As a clinician, many years ago, prescribing exercise therapy for low back pain was my daily bread. None of my team would have ever conceived the idea that exercise does not need to be individualized according to the needs and capabilities of each patient. Therefore, I suggest rephrasing the last sentence of the conclusion: As individualization in exercise therapies is easy to implement, its use should be standard procedure.