osteopathy
Osteopathic manipulative treatment (OMT) is advocated not merely for spinal or musculoskeletal problems, as many consumers seem to think, osteopaths also claim it to be effective for (almost) every condition. Some osteopaths who believe in the gospel of Andrew Still, the founder of osteopathy, recommend it even to facilitate breastfeeding.
But is it effective?
A double-blind randomised controlled trial to answer this question was conducted between July 2013 and March 2016. Breastfed term infants were eligible if one of the following criteria was met: suboptimal breastfeeding behaviour, maternal cracked nipples or maternal pain. The infants were randomly assigned to the intervention or the control group. The intervention consisted of two sessions of early OMT, while in the control group, the manipulations were performed on a doll behind a screen. The primary outcome was the exclusive breastfeeding rate at 1 month, which was assessed in an intention-to-treat analysis. Randomisation was computer generated and only accessible to the osteopath practitioner. The parents, research assistants and paediatricians were masked to group assignment.
One hundred twenty-eight mother-infant dyads were randomised, with 64 assigned to each group. In each group, five infants were lost to follow-up. In the intervention group, 31 of 59 (53%) of infants were still exclusively breastfed at 1 month vs 39 of 59 (66%) in the control group, (OR 0.55, 95% CI 0.26 to 1.17; p=0.12). After adjustment for suboptimal breastfeeding behaviour, caesarean section, use of supplements and breast shields, the adjusted OR was 0.44 (95% CI 0.17 to 1.11; p=0.08). No adverse effects were reported in either group.
The authors concluded succinctly that OMT did not improve exclusive breastfeeding at 1 month.
Surprised?
Suppose not!
The only question that I can think of is this: why did osteopaths ever think that OMT might facilitate breastfeeding?
Neck pain affects a vast number of people and leads to reduced quality of life and high costs. Clinically, it is a difficult condition to manage, and the effect sizes of the currently available treatments are moderate at best. Activity and manual therapy are first-line treatment options in several guidelines. But how effective are they really?
This study investigated the combination of home stretching exercises and spinal manipulative therapy in a multicentre randomized controlled clinical trial, carried out in a multidiscipline range of primary care clinics.
The treatment modalities utilized were spinal manipulative therapy combined with home stretching exercises compared to home stretching exercises alone. Both groups received 4 treatments for 2 weeks. The primary outcome was pain, where the subjective pain experience was investigated by assessing pain intensity (NRS – 11) and the quality of pain (McGill Pain Questionnaire). Neck disability and health status were secondary outcomes, measured using the Neck Disability Indexthe EQ-5D, respectively.
One hundred thirty-one adult subjects were randomized to one of the two treatment groups. All subjects had experienced persistent or recurrent neck pain the previous 6 months and were blinded to the other group intervention. The clinicians provided treatment for subjects in both groups and could not be blinded. The researchers collecting data were blinded to treatment allocation, as was the statistician performing data analyses. An intention-to-treat analysis was used.
Sixty-six subjects were randomized to the intervention group, and 65 to the control group. For NRS – 11, a B-coefficient of – 0,01 was seen, indication a 0,01 improvement for the intervention group in relation to the control group at each time point with a p-value of 0,305. There were no statistically significant differences between groups for any of the outcome measures.
Four intense adverse events were reported in the study, three in the intervention group, and one in the control group. More adverse incidents were reported in the intervention group, with a mean pain intensity (NRS-11) of 2,75 compared to 1,22 in the control group. There were no statistically significant differences between the two groups.
The authors concluded that there is no additional treatment effect from adding spinal manipulative therapy to neck stretching exercises over 2 weeks for patients with persistent or recurrent neck pain.
This is a rigorous and well-reported study. It suggests that adjuvant manipulations are not just ineffective for neck pain, but also cause some adverse effects. This seems to confirm many previously discussed investigations concluding that chiropractors do not generate more good than harm for patients suffering from neck pain.
The effectiveness of manipulation versus mobilization for the management of spinal conditions, including cervicogenic headache, is conflicting, and a pragmatic approach comparing manipulation to mobilization has not been examined in a patient population with cervicogenic headache.
This study evaluated the effectiveness of manipulation compared to mobilization applied in a pragmatic fashion for patients with cervicogenic headache.
Forty-five (26 females) patients with cervicogenic headache were randomly assigned to receive either pragmatically selected manipulation or mobilization. Outcomes were measured at baseline, the second visit, discharge, and 1-month follow-up. The endpoints of the study included the Neck Disability Index (NDI), Numeric Pain Rating Scale (NPRS), the Headache Impact Test (HIT-6), the Global Rating of Change (GRC), the Patient Acceptable Symptoms Scale (PASS). The primary outcome measures were the effects of treatment on disability and pain. They were examined with a mixed-model analysis of variance (ANOVA), with treatment group (manipulation versus mobilization) as the between-subjects variable and time (baseline, 48 hours, discharge, and follow-up) as the within-subjects variable.
The interaction for the mixed model ANOVA was not statistically significant for NDI (p = 0.91), NPRS (p = 0.81), or HIT (p = 0.89). There was no significant difference between groups for the GRC or PASS.
The authors concluded that manipulation has similar effects on disability, pain, GRC, and cervical range of motion as mobilization when applied in a pragmatic fashion for patients with cervicogenic headaches.
Essentially, this study is an equivalence trial comparing one treatment to another. As such it would need a much larger sample size than the 45 patients enrolled by the investigators. If, however, we ignored this major flaw and assumed the results are valid, they would be consistent with both manipulation and mobilization being pure placebos.
I can imagine that many chiropractors find this conclusion unacceptable. Therefore, let me offer an alternative: both approaches were equally effective. Therefore, mobilization, which is associated with far fewer risks, is preferable. This means that patients suffering from cervicogenic headache should see an osteopath who is less likely to use manipulation than a chiropractor.
And again, I can imagine that many chiropractors find this conclusion unacceptable.
In a recently published study, the willingness to be vaccinated of parents of underage children and persons without underage children was examined. The study was based on a random sample (telephone survey, n = 2014, survey between 12.11.2020 and 10.12.2020).
The results revealed that parents consistently show a lower propensity to vaccinate with a COVID-19 vaccine than respondents without minor children (54.1% vs. 71.1%). Fathers showed a more pronounced own willingness to vaccinate than mothers. Furthermore, men were more willing than women to have their own child vaccinated with a COVID-19 vaccine.
The overall sample also showed that a rejection of so-called alternative medicine (SCAM) was associated with a significantly higher willingness to be vaccinated. There was also a significant correlation between the attitude towards homeopathy and one’s own willingness to be vaccinated. If homeopathy was supported, the willingness to vaccinate was lower. This correlation between the attitude towards homeopathy and willingness to vaccinate was also evident in the sub-sample of parents. Among the parents, it was again the women who significantly more often had a positive attitude towards homeopathy than men, who more often do not think anything of it.
This new evidence ties in neatly with many of my previous posts on the subject of SCAM and vaccination, for instance:
- More information on homeopaths’ and anthroposophic doctors’ attitude towards vaccinations
- The anti-vaccination movement is financed by the dietary supplement industry
- The UK Society of Homeopaths, a hub of anti-vaccination activists?
- HOMEOPATHY = “the complete alternative to vaccination” ?!?!
- Are anthroposophy-enthusiasts for or against vaccinations?
- Far too many chiropractors believe that vaccinations do not have a positive effect on public health
- Andrew Wakefield, Donald Trump, SCAM, and the anti-vaccination cult
- Naturopaths’ counselling against vaccinations could be criminally negligent
- HOMEOPATHS AGAINST VACCINATION: “The decision to vaccinate and how you implement that decision is yours and yours alone”
- Use of alternative medicine is associated with low vaccination rates
- Integrative medicine physicians tend to harbour anti-vaccination views
- Vaccination: chiropractors “espouse views which aren’t evidence based”
- Faith-healing as an alternative to vaccination?
- Learning about homeopathy the hard way: the story of Aaron Rodgers
- Patients consulting chiropractors, homeopaths, or naturopaths are less likely to agree to the flu jab
- Parents’ Willingness to Vaccinate with a COVID-19 Vaccine: strongly influenced by homeopathy
- “The uncensored truth” about COVID-19 vaccines” … as told by some chiro loons
- Beliefs and behaviors of US chiropractors
- Many naturopaths, homeopaths, and chiropractors are a risk to public health
- Homeopaths (and other SCAM practitioners) are peddling dangerous myths
- Misinformation and fraudulent claims about boosting immunity during the pandemic
Collectively, this evidence tells us that:
- the effect has been shown in many different ways,
- it can therefore be assumed to be real,
- it is not confined to COVID vaccinations,
- it is not confined to one particular branch of SCAM,
- it even affects MDs (who surely should know better) dabbling in SCAM,
- it has a long history,
- it is prevalent in many, if not most countries,
- it does real harm.
So, the next time someone tells you that SCAM and SCAM practitioners have a positive influence on public health, tell them to think again.
As we have discussed ad nauseam on this blog, spinal manipulation therapy (SMT) can cause serious adverse events, including spinal epidural hematoma (SEH), an emergency that can cause severe neurological dysfunction. Chinese surgeons have reported three cases of SEH after SMT.
- The first case was a 30-year-old woman who experienced neck pain and numbness in both upper limbs immediately after SMT. Her symptoms persisted after 3 d of conservative treatment, and she was admitted to our hospital. Magnetic resonance imaging (MRI) demonstrated an SEH, extending from C6 to C7.
- The second case was a 55-year-old man with sudden back pain 1 d after SMT, numbness in both lower limbs, an inability to stand or walk, and difficulty urinating. MRI revealed an SEH, extending from T1 to T3.
- The third case was a 28-year-old man who suddenly developed symptoms of numbness in both lower limbs 4 h after SMT. He was unable to stand or walk and experienced mild back pain. MRI revealed an SEH, extending from T1 to T2.
All three patients underwent surgery after failed conservative treatment. Blood clots were found during the operation in case 1 and case 2, and the postoperative pathology confirmed a hematoma. In case three, a vein ruptured during the operation, causing massive bleeding. The three patients recovered to ASIA grade E on day 5, 1 wk, and day 10 after surgery, respectively. All patients returned to normal after 3 mo of follow-up.
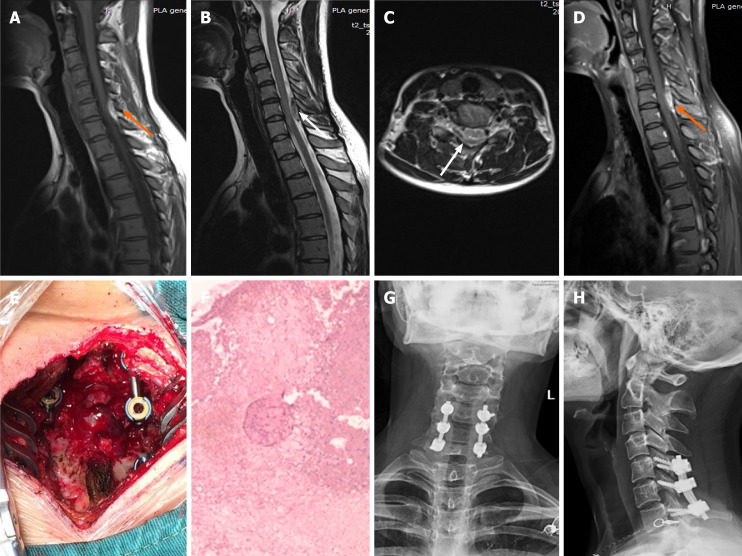
Imaging examinations of case 1. A: T1-weighted preoperative magnetic resonance imaging (MRI) image shows high signal intensity (orange arrow); B and C: Preoperative T2-weighted image shows low signal intensity, and an axial T2-weighted image demonstrates that the hematoma occurred in the posterior region (white arrow); D: Preoperative enhanced MRI suggests an enhanced hematoma signal (orange arrow); E: Intraoperative photograph shows that spinal cord compression has recovered; F: Postoperative pathology suggested a hematoma; G and H: X-ray at the 3-mo follow-up indicated intact internal fixation.
The authors concluded that before proceeding with SMT, each patient should be evaluated in detail and checked for risk factors. In cases where the physical condition changes rapidly, physicians should be alert to the danger and send the patient to the emergency department for a complete MRI examination. We recommend surgery if neurological symptoms appear.
In their paper, the authors also review 15 further cases of SEH that have been previously published. They stress several times in their article that this complication is rare. In my view, this begs the question: how do they know? As there is no post-marketing surveillance of chiropractors or other clinicians doing SMT, I would insist that nobody can be sure about the true incidence of SEH or any other complication after SMT.
Static or motion manual palpation tests of the spine are commonly used by chiropractors and osteopaths to assess pain location and reproduction in low back pain (LBP) patients. But how reliable are they?
The purpose of this review was to evaluate the reliability and validity of manual palpation used for the assessment of LBP in adults. The authors systematically searched five databases from 2000 to 2019 and critically appraised the internal validity of studies using QAREL and QUADAS-2 instruments.
A total of 2023 eligible articles were identified, of which 14 were at low risk of bias. Evidence suggests that reliability of soft tissue structures palpation is inconsistent, and reliability of bony structures and joint mobility palpation is poor. Preliminary evidence was found to suggest that gluteal muscle palpation for tenderness may be valid in differentiating LBP patients with and without radiculopathy.
The authors concluded that the reliability of manual palpation tests in the assessment of LBP patients varies greatly. This is problematic because these tests are commonly used by manual therapists and clinicians. Little is known about the validity of these tests; therefore, their clinical utility is uncertain. High quality validity studies are needed to inform the clinical use of manual palpation tests.
I have repeatedly drawn attention to the fact that the diagnostic methods used by chiropractors and osteopaths are of uncertain or disproven validity (see for instance here, or here). Why is that important?
Imagine you consult a chiropractor or osteopath. Simply put, this is what is likely to happen:
- They listen to your complaint.
- They do a few tests which are of dubious validity.
- They give you a diagnosis that is meaningless.
- They treat you with manual therapies that are neither effective nor safe.
- You pay.
- They persuade you that you need many more sessions.
- You pay regularly.
- When eventually your pain has gone away, they persuade you to have useless maintenance treatment.
- You pay regularly.
In a nutshell, they have very little to offer … which explains why they attack everyone who dares to disclose this.
In their 2019 systematic review of spinal manipulative therapy (SMT) for chronic back pain, Rubinstein et al included 7 studies comparing the effect of SMT with sham SMT.
They defined SMT as any hands-on treatment of the spine, including both mobilization and manipulation. Mobilizations use low-grade velocity, small or large amplitude passive movement techniques within the patient’s range of motion and control. Manipulation uses a high-velocity impulse or thrust applied to a synovial joint over a short amplitude near or at the end of the passive or physiological range of motion. Even though there is overlap, it seems fair to say that mobilization is the domain of osteopaths, while manipulation is that of chiropractors.
The researchers found:
- low-quality evidence suggesting that SMT does not result in a statistically better effect than sham SMT at one month,
- very low-quality evidence suggesting that SMT does not result in a statistically better effect than sham SMT at six and 12 months.
- low-quality evidence suggesting that, in terms of function, SMT results in a moderate to strong statistically significant and clinically better effect than sham SMT at one month. Exclusion of an extreme outlier accounted for a large percentage of the statistical heterogeneity for this outcome at this time interval (SMD −0.27, 95% confidence interval −0.52 to −0.02; participants=698; studies=7; I2=39%), resulting in a small, clinically better effect in favor of SMT.
- very low-quality evidence suggesting that, in terms of function, SMT does not result in a statistically significant better effect than sham SMT at six and 12 months.
This means that SMT has effects that are very similar to placebo (the uncertain effects on function could be interpreted as the result of residual de-blinding due to a lack of an optimal placebo or sham intervention). In turn, this means that the effects patients experience are largely or completely due to a placebo response and that SMT has no or only a negligibly small specific effect on back pain. Considering the facts that SMT is by no means risk-free and that less risky treatments exist, the inescapable conclusion is that SMT cannot be recommended as a treatment of chronic back pain.
This systematic review assessed the effect of spinal manipulative therapy (SMT), the hallmark therapy of chiropractors, on pain and function for chronic low back pain (LBP) using individual participant data (IPD) meta-analyses.
Of the 42 RCTs fulfilling the inclusion criteria, the authors obtained IPD from 21 (n=4223). Most trials (s=12, n=2249) compared SMT to recommended interventions. The analyses showed moderate-quality evidence that SMT vs recommended interventions resulted in similar outcomes on
- pain (MD -3.0, 95%CI: -6.9 to 0.9, 10 trials, 1922 participants)
- and functional status at one month (SMD: -0.2, 95% CI -0.4 to 0.0, 10 trials, 1939 participants).
Effects at other follow-up measurements were similar. Results for other comparisons (SMT vs non-recommended interventions; SMT as adjuvant therapy; mobilization vs manipulation) showed similar findings. SMT vs sham SMT analysis was not performed, because data from only one study were available. Sensitivity analyses confirmed these findings.
The authors concluded that sufficient evidence suggest that SMT provides similar outcomes to recommended interventions, for pain relief and improvement of functional status. SMT would appear to be a good option for the treatment of chronic LBP.
In 2019, this team of authors published a conventional meta-analysis of almost the same data. At this stage, they concluded as follows: SMT produces similar effects to recommended therapies for chronic low back pain, whereas SMT seems to be better than non-recommended interventions for improvement in function in the short term. Clinicians should inform their patients of the potential risks of adverse events associated with SMT.
Why was the warning about risks dropped in the new paper?
I have no idea.
But the risks are crucial here. If we are told that SMT is as good or as bad as recommended therapies, such as exercise, responsible clinicians need to decide which treatment they should recommend to their patients. If effectiveness is equal, other criteria come into play:
- cost,
- risk,
- availability.
Can any reasonable person seriously assume that SMT would do better than exercise when accounting for costs and risks?
I very much doubt it!
The objective of this systematic review was to assess the effects and reliability of sham procedures in manual therapy (MT) trials in the treatment of back pain (BP) in order to provide methodological guidance for clinical trial development. Different databases were screened up to 20 August 2020. Randomised clinical trials involving adults affected by BP (cervical and lumbar), acute or chronic, were included. Hand contact sham treatment (ST) was compared with different MT (physiotherapy, chiropractic, osteopathy, massage, kinesiology, and reflexology) and to no treatment. Primary outcomes were BP improvement, the success of blinding, and adverse effect (AE). Secondary outcomes were the number of drop-outs. Dichotomous outcomes were analysed using risk ratio (RR), continuous using mean difference (MD), 95% CIs. The minimal clinically important difference was 30 mm changes in pain score.
A total of 24 trials were included involving 2019 participants. Different manual treatments were provided:
- SM/chiropractic (7 studies, 567 participants).
- Osteopathy (5 trials, 645 participants).
- Kinesiology (1 trial, 58 participants).
- Articular mobilisations (6 trials, 445 participants).
- Muscular release (5 trials, 304 participants).
Very low evidence quality suggests clinically insignificant pain improvement in favour of MT compared with ST (MD 3.86, 95% CI 3.29 to 4.43) and no differences between ST and no treatment (MD -5.84, 95% CI -20.46 to 8.78).ST reliability shows a high percentage of correct detection by participants (ranged from 46.7% to 83.5%), spinal manipulation being the most recognised technique. Low quality of evidence suggests that AE and drop-out rates were similar between ST and MT (RR AE=0.84, 95% CI 0.55 to 1.28, RR drop-outs=0.98, 95% CI 0.77 to 1.25). A similar drop-out rate was reported for no treatment (RR=0.82, 95% 0.43 to 1.55).

Forest plot of comparison ST versus MT in back pain outcome at short term. MT, manual therapy; ST, sham treatment.
The authors concluded that MT does not seem to have clinically relevant effect compared with ST. Similar effects were found with no treatment. The heterogeneousness of sham MT studies and the very low quality of evidence render uncertain these review findings. Future trials should develop reliable kinds of ST, similar to active treatment, to ensure participant blinding and to guarantee a proper sample size for the reliable detection of clinically meaningful treatment effects.
Essentially these findings suggest that the effects patients experience after MT are not due to MT per see but to placebo effects. The review could be criticised because of the somewhat odd mix of MTs lumped together in one analysis. Yet, I think it is fair to point out that most of the studies were of chiropractic and osteopathy. Thus, this review implies that chiropractic and osteopathy are essentially placebo treatments.
The authors of the review also provide this further comment:
Similar findings were found in other reviews conducted on LBP. Ruddock et al included studies where SM was compared with what authors called ‘an effective ST’, namely a credible sham manipulation that physically mimics the SM. Pooled data from four trials showed a very small and not clinically meaningful effect in favour of MT.52
Rubinstein et al 53 compared SM and mobilisation techniques to recommended, non-recommended therapies and to ST. Their findings showed that 5/47 studies included attempted to blind patients to the assigned intervention by providing an ST. Of these five trials, two were judged at unclear risk of participants blinding. The authors also questioned the need for additional studies on this argument, as during the update of their review they found recent small pragmatic studies with high risk of bias. We agree with Rubinstein et al that recent studies included in this review did not show a higher quality of evidence. The development of RCT with similar characteristic will probably not add any proof of evidence on MT and ST effectiveness.53
If we agree that chiropractic and osteopathy are placebo therapies, we might ask whether they should have a place in the management of BP. Considering the considerable risks associated with them, I feel that the answer is obvious and simple:
NO!
Multiple sclerosis (MS) causes a range of different symptoms. Patients with MS have looked for alternative therapies to control their MS progress and treat their symptoms. Non-invasive therapeutic approaches such as massage can have benefits to mitigate some of these symptoms. However, there is no rigorous review of massage effectiveness for patients suffering from MS.
The present systematic review was aimed at examining the effectiveness of different massage approaches on common MS symptoms, including fatigue, pain, anxiety, depression, and spasticity.
A total of 12 studies met the inclusion criteria. The authors rated 5 studies as being of fair and 7 studies of good methodological quality. Fatigue was improved by different massage styles, such as reflexology, nonspecific therapeutic massage, and Swedish massage. Pain, anxiety, and depression were effectively improved by reflexology techniques. Spasticity was reduced by Swedish massage and reflexology techniques.
The authors concluded that different massage approaches effectively improved MS symptoms such as fatigue, pain, anxiety, depression, and spasticity.
Clinical trials of massage therapy face formidable obstacles including:
- difficulties in obtaining funding,
- difficulties in finding expert researchers who are interested in the subject,
- difficulties to control for placebo effects,
- difficulties in blinding patients,
- impossibility of blinding therapists,
- confusion about the plethora of different massage techniques.
Thus, the evidence is often less convincing than one would hope. This, however, does not mean that massage therapy does not have considerable potential for a range of indications. One could easily argue that this situation is similar to spinal manipulation. Yet, there are at least three important differences:
- massage therapy is not as heavily burdened with frequent adverse effects and potentially life-threatening complications,
- massage therapy has a rational basis,
- the existing evidence is more uniformly encouraging.
Consequently, massage therapy (particularly, classic or Swedish massage) is more readily being accepted even in the absence of solid evidence. In fact, in some countries, e.g. Germany and Austria, massage therapy is considered to be a conventional treatment.