herbal medicine
“I don’t take chemicals,
I prefer natural herbal remedies!”
How often have we heard such statements? They are usually pronounced with an air of smug superiority and condescending pity towards those poor consumers who swallow paracetamol, ibuprofen, or other chemicals when having a headache or other health problem.
But the air of superiority seems misplaced because these ‘herbivores’ actually consume many more chemicals than the ‘chemivores’. What those who swear by ‘non-chemical’ medicines ignore is the fact that herbal remedies are packed with many different chemicals.
Below I have listed the main active chemical compound of some very well-known herbal remedies:
- Calendula (Calendula officinalis L.): flavonoids, triterpene alcohols, triterpene saponins, carotenoids, polysaccharides, essential oil
- Chamomile (Matricaria recutita L.): essential oil, sesquiterpenes, dicycloethern
- Echinacea (Echinacea purpurea): polysaccharides, caffeic acid derivatives, alkamides, polyacetylenes, essential oil.
- Eucalyptus (Eucalyptus globulus Labill.): cineole, euglobales, macrocarpales
- Garlic (Allium sativum L.): alliin [(+)- S-allyl-L-cystein sulfoxide], allicin (allyl 2- thiosulphate propane)
- Hops (Humulus lupulus L.): phloroglucinol derivates, essential oil
- Lavender (Lavandula angustifolia Mill.): linalyl acetate and linalool, tannins
- Liquorice (Glycyrrhiza glabra L.): triterpenoid, flavonoids, isoflavones, polysaccharides
- Peppermint (Mentha x piperita L.): menthol, menthone, menthyl acetate, tannins, flavonoids
- Valerian (Valeriana officinalis L.): essential oil, sesquiterpene acids, iridoids, lignans, caffeic acid derivatives, alkaloids
Whenever I explain this to a ‘herbivore’ (here defined as a person who prefers herbal to conventional medicine), she is initially taken aback but, as soon as she has recovered from the shock, she regains their superior attitude and says: “Ah yes, but these are natural chemicals; they cannot do any harm, you know.”
“No, I don’t know!” I then reply, “There are two errors in what you just said: firstly, many chemicals that plants produce are highly poisonous – in fact, some of the most potent toxins we know come from plants – and secondly there is no difference between a chemical XY produced by a plant and the same chemical produced in a factory.”
At this stage, we usually change the subject or part our ways.
Post-traumatic stress disorder (PTSD), previously known as battle fatigue syndrome or shell shock, is a condition that can be triggered by the experience of some frightening event. PTSD can be debilitating leading to the production of feelings of helplessness, intense fear, and horror. Numerous treatments of PTSD exist but few have been shown to be truly effective. A team of Canadian researchers explored the effects of cannabis on PTSD symptoms, quality of life (QOL), and return to work (RTW). Their systematic review also investigated harms such as adverse effects and dropouts due to adverse effects, inefficacy, and all-cause dropout rates.
Their electronic searches located one RCT and 10 observational studies (n = 4672). Risk of bias (RoB) was assessed with the Cochrane risk of bias tool and ROBINS-I. Evidence from the included studies was mainly based on studies with no comparators. Results from unpooled, high RoB studies suggested that cannabis was associated with a reduction in overall PTSD symptoms and improved QOL. Dry mouth, headaches, and psychoactive effects such as agitation and euphoria were the most commonly reported adverse effects. In most studies, cannabis was well tolerated. A small proportion of patients experienced a worsening of PTSD symptoms.
The authors concluded that the evidence in the current study primarily stems from low quality and high RoB observational studies. Further RCTs investigating cannabis effects on PTSD treatment should be conducted with larger sample sizes and explore a broader range of patient-important outcomes.
Various drugs are currently used for the treatment of PTSD including selective serotonin reuptake inhibitors; tricyclic antidepressants (amitriptyline and isocarboxazid); mood stabilizers (Divalproex and lamotrigine); atypical antipsychotics (aripiprazole and quetiapine) but their effectiveness has not been proven. A recent systematic review included 30 RCTs of a range of heterogeneous non-psychological and non-pharmacological interventions. There was emerging evidence for 6 different approaches:
- acupuncture,
- neurofeedback,
- saikokeishikankyoto (a herbal preparation),
- somatic experiencing,
- transcranial magnetic stimulation,
- yoga.
This list makes me wonder: are these treatments, including cannabis, truly promising, or is PTSD one of those conditions for which nearly every treatment works a little because of its placebo effect?
Due to polypharmacy and the rising popularity of so-called alternative medicines (SCAM), oncology patients are particularly at risk of drug-drug interactions (DDI) or herb-drug interactions (HDI). The aims of this study were to assess DDI and HDI in outpatients taking oral anticancer drugs.
All prescribed and non-prescribed medications, including SCAMs, were prospectively collected by hospital pharmacists during a structured interview with the patient. DDI and HDI were analyzed using four interaction software programs: Thériaque®, Drugs.com®, Hédrine, and Memorial Sloan Kettering Cancer Center (MSKCC) database. All detected interactions were characterized by severity, risk, and action mechanism. The need for pharmaceutical intervention to modify drug use was determined on a case-by-case basis.
A total of 294 patients were included, with a mean age of 67 years [55-79]. The median number of chronic drugs per patient was 8 [1-29] and 55% of patients used at least one SCAM. At least 1 interaction was found for 267 patients (90.8%): 263 (89.4%) with DDI, 68 (23.1%) with HDI, and 64 (21.7%) with both DDI and HDI. Only 13% of the DDI were found in Thériaque® and Drugs.com® databases, and 125 (2.5%) were reported with a similar level of risk on both databases. 104 HDI were identified with only 9.5% of the interactions found in both databases. 103 pharmaceutical interventions were performed, involving 61 patients (20.7%).
The authors concluded that potentially clinically relevant drug interactions were frequently identified in this study, showing that several databases and structured screening are required to detect more interactions and optimize medication safety.
These data imply that DDIs are more frequent than HDIs. This does, however, not tell us which are more important. One crucial difference between DDIs and HDIs is that the former are usually known to the oncology team who should thus be able to prevent them or deal with them appropriately; in contrast, HDIs are often not known to the oncology team because many patients fail to disclose the fact that they take herbal remedies. Some forget, some do not think of herbals as medicine, others may be worried about their physician’s reaction.
It follows that firstly, conventional healthcare practitioners should always ask about the usage of herbal remedies, and secondly, they need to be informed about which herbal remedy might interact with which drug. The first can easily be implemented into routine history-taking; the second is more problematic, not least because our knowledge about HDIs is still woefully incomplete. In view of this, it might often be wise to tell patients to stop taking herbal remedies while they are on prescription drugs.
This amazing announcement reached me via Twitter. It seems that the people in the AYUSH ministry are highly delusional. According to Wikipedia, the Ministry of Ayurveda, Yoga, Naturopathy, Unani, Siddha, Sowa-Rigpa and Homoeopathy (abbreviated as AYUSH) is purposed with developing education, research and propagation of indigenous alternative medicine systems in India. As per a recent notification published in the Gazette of India on 13 April 2021, the Ministry of AYUSH (Ayurveda, Yoga & Naturopathy, Unani, Siddha and Homoeopathy), will now be known as the Ministry of Ayush.
India is suffering from a very severe health crisis, and the ministry should stop its propaganda for useless solutions.
- Ayurveda,
- Homeopathy (considered to be indigenous in India),
- Yoga,
- Naturopathy,
- Unani,
- Sidda,
- Sowa-Rigpa (the traditional medicine of Tibet)
have in common that they can offer very little help to patients infected by COVID-19. In view of this fact, the announcement is ununderstandable and irresponsible, in my view.
Epidemiological studies on the association between coffee intake, arguably a herbal remedy, and cancer risk have yielded inconsistent results. To summarize and appraise the quality of the current evidence, researchers conducted an umbrella review of existing findings from meta-analyses of observational studies.
They searched PubMed, Embase, Web of Science and the Cochrane database to obtain systematic reviews and meta-analyses of associations between coffee intake and cancer incidence. For each association, they estimated the summary effect size using the fixed- and random-effects model, the 95% confidence interval, and the 95% prediction interval. We also assessed heterogeneity, evidence of small-study effects, and excess significance bias.
Twenty-eight individual meta-analyses including 36 summary associations for 26 cancer sites were retrieved for this umbrella review. A total of 17 meta-analyses were significant at P ≤ 0.05 in the random-effects model. For the highest versus lowest categories, 4 of 26 associations had a more stringent P value (P ≤ 10− 6). Associations for five cancers were significant in dose-response analyses. Most studies (69%) showed low heterogeneity (I2 ≤ 50%). Three and six associations had evidence of excessive significance bias and publication bias, respectively. Coffee intake was inversely related to the risk of liver cancer and endometrial cancer and was characterized by dose-response relationships. There were no substantial changes when the researchers restricted analyses to a meta-analysis of cohort studies.
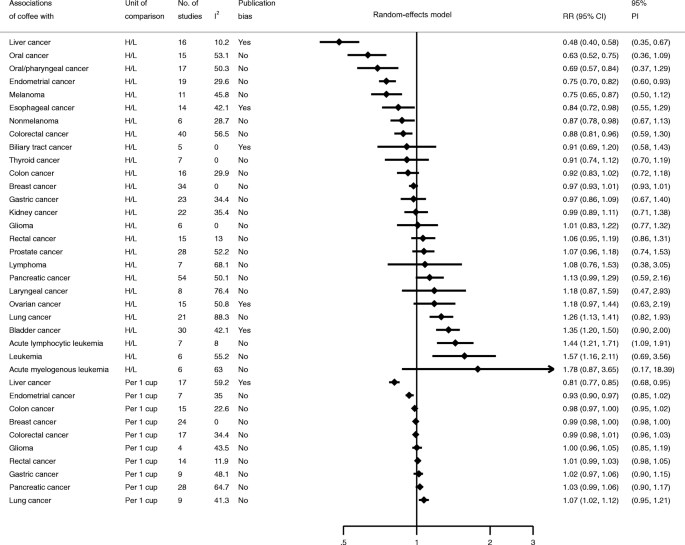
The authors concluded that there is highly suggestive evidence for an inverse association between coffee intake and risk of liver and endometrial cancer. Further research is needed to provide more robust evidence for cancer at other sites.
This is an interesting analysis that begs many questions. Let me just make four brief points:
- Correlation is not causation! Epidemiological studies throw up all sorts of associations that are too often mistaken as causal relationships. The question of whether coffee causes a decrease in the risk of certain cancers is as yet unanswered. The authors mention dose relationships which would, of course, increase the likelihood of a causal effect. Yet, they do not prove it.
- Another argument that would strengthen the possibility of a causal effect would be a plausible mechanism of action. However, the biological mechanism of how coffee might affect the risk remains unclear. Coffee contains a range of biologically active chemicals, including caffeine and phenolic compounds. In so-called alternative medicine (SCAM), coffee is also claimed to be a ‘detox‘ remedy. Yet it is unclear how exactly they might reduce the risk.
- The studies were all about the oral consumption of coffee. None considered anal application, like in Gerson therapy.
- The only way to find out whether coffee does, in fact, reduce the risk of certain cancers is to conduct prospective controlled clinical trials. Such studies are, however, not easy to conduct, particularly if designed such that their findings are truly reliable.
So, the answer to the question DOES COFFEE CONSUMPTION PREVENT CANCER? will remain unanswered for some time, I am afraid. Meanwhile, I suggest we enjoy our coffee per oral (and avoid it per anal).
The use of so-called alternative medicine (SCAM) is common among breast cancer patients, but less is known about whether SCAM influences breast cancer survival. The primary aim of this recent study from Tunesia was to determine the impact of self-use of herbs on the overall survival of women with breast cancer.
The researchers conducted a prospective study including 110 patients with breast cancer. All patients were questioned about their usage of herbal remedies. The demographic data and the overall survival of the patients were then analyzed.
The average age was 51 years (30-80 years old). In total, 37 had metastatic disease (33.6%), and 48 patients had taken plant-based treatments (43.6%). Of those women, 19 patients consumed Graviola (39.6%) and 29 Alenda (60.4%). Overall survival rates at 3 years and at 5 years were 96.2% and 82.4% in the absence of herbal medicine usage versus 78.5% and 78.5% in the presence of herbal medicine use (p = 0.015).
The authors concluded that self-medication with Graviola or Alenda may be associated with an increase of death risk in patients with breast cancer. Further studies are needed to confirm these results.
This is only a small and not very rigorous case-control study. In itself, it would be far from conclusive. What renders it relevant, however, is the fact that its findings do by no means stand alone. We have seen several times on this blog that SCAM use can shorten the life of cancer patients, e.g.:
- More evidence that SCAM-use is associated with shorter survival of cancer patients
- Patients who received CM were more likely to refuse additional CCT, and had a higher risk of death. The results suggest that mortality risk associated with CM was mediated by the refusal of CCT.
- The use of CAM had significantly associated with delay in presentation and resolution of diagnosis.
- CAM did not provide any definite survival benefit, CAM users reported clinically significant worse health-related quality of life.
So, perhaps it is true? Perhaps using SCAM is not such a good idea, if you are suffering from cancer!
The mechanisms of such detrimental effects are not difficult to imagine. They might include direct effects on the cancer, interactions with prescribed drugs, delay of cancer diagnosis, or less strict adherence to the anti-cancer treatments.
The Chinese have made several attempts to persuade us that their traditional remedies are effective for COVID-19 infections. Here is yet another one. This review summarised the evidence of the therapeutic effects and safety of Chinese herbal medicine (CHM) used with or without conventional western therapy for COVID-19. All clinical studies of the therapeutic effects and safety of CHM for COVID-19 were included. The authors
- summarized the general characteristics of included studies,
- evaluated the methodological quality of the randomized controlled trials (RCTs) using the Cochrane risk of bias tool,
- analyzed the use of CHM,
- used Revman 5.4 software to present the risk ratio (RR) or mean difference (MD) and their 95% confidence interval (CI) to estimate the therapeutic effects and safety of CHM.
A total of 58 clinical studies were identified including;
- 10 RCTs,
- 1 non-randomized controlled trials,
- 11 retrospective studies with a control group,
- 12 case-series,
- 24 case-reports.
All of the studies had been performed in China. No RCTs of high methodological quality were identified. The most frequently tested oral Chinese patent medicine, Chinese herbal medicine injection, or prescribed herbal decoction were:
- Lianhua Qingwen granule/capsule,
- Xuebijing injection,
- Maxing Shigan Tang.
The pooled analyses showed that there were statistical differences between the intervention group and the comparator group (RR 0.42, 95% CI 0.21 to 0.82, six RCTs; RR 0.38, 95% CI 0.23 to 0.64, five retrospective studies with a control group), indicating that CHM plus conventional western therapy appeared to be better than conventional western therapy alone in reducing aggravation rate.
In addition, compared with conventional western therapy, CHM plus conventional western therapy had the potential advantages in increasing the recovery rate and shortening the duration of fever, cough, and fatigue, improving the negative conversion rate of nucleic acid test, and increasing the improvement rate of chest CT manifestations and shortening the time from receiving the treatment to the beginning of chest CT manifestations improvement.
For adverse events, the pooled data showed that there were no statistical differences between the CHM and the control groups.
The authors concluded that current low certainty evidence suggests that there maybe a tendency that CHM plus conventional western therapy is superior to conventional western therapy alone. The use of CHM did not increase the risk of adverse events.
One of the principles to remember here is this: RUBBISH IN, RUBBISH OUT. If you meta-analyze primary data that are rubbish, your findings can only be rubbish as well.
All one needs to know about the primary data entered into the present analysis is that there were no rigorous RCTs… not one! That means the evidence is, as the authors rightly but modestly conclude of LOW CERTAINTY. My conclusions would have been a little different:
- In terms of safety, the dataset is too small and unreliable to make any judgment.
- In terms of efficacy, there is no sound data that CHM has a positive effect.
As I don’t live in the UK at present, I miss much of what the British papers report about so-called alternative medicine (SCAM). Therefore, I am a bit late to stumble over an article on the business activities of our Royals. It brought back into memory a little tiff I had with Prince Charles.
The article in the Express includes the following passage:

The UK’s first professor of complementary medicine, Edzard Ernst, dubbed the Duchy Originals detox tincture — which was being sold on the market at the time — “outright quackery”.
The product, called Duchy Herbals’ Detox Tincture, was advertised as a “natural aid to digestion and supports the body’s elimination processes” and a “food supplement to help eliminate toxins and aid digestion”.
The artichoke and dandelion mix cost £10 for a 50ml bottle.
Yet, Professor Ernst said Charles and his advisers seemed to be ignoring the science in favour of relying on “make-believe” and “superstition”, and said the suggestion that such products could remove bodily toxins was “implausible, unproven and dangerous”.
He noted: “Prince Charles thus financially exploits a gullible public in a time of financial hardship.”
This passage describes things accurately but not completely. What actually happened was this:
Unbeknown to me and with the help of some herbalists, Duchy Originals had developed the ‘detox tincture’ during a time when I was researching the evidence about ‘detox’. Eventually, my research was published as a review of the detox concept:
Background: The concept that alternative therapies can eliminate toxins and toxicants from the body, i.e. ‘alternative detox’ (AD) is popular.
Sources of data: Selected textbooks and articles on the subject of AD.
Areas of agreement: The principles of AD make no sense from a scientific perspective and there is no clinical evidence to support them.
Areas of controversy: The promotion of AD treatments provides income for some entrepreneurs but has the potential to cause harm to patients and consumers.
Growing points: In alternative medicine, simplistic but incorrect concepts such as AD abound. AREAS TIMELY FOR RESEARCH: All therapeutic claims should be scientifically tested before being advertised-and AD cannot be an exception.
When I was asked by a journalist what I thought about Charles’ new ‘detox tincture’, I told her that it was not supported by evidence which clearly makes it quackery. I also joked that Duchy Originals could thus be called ‘Dodgy Originals’. The result was this newspaper article and a subsequent media storm in the proverbial teacup.
At Exeter University, I had just fallen out of favor because of the ‘Smallwood Report’ and the complaint my involvement in it prompted by Charles’ first private secretary (full story in my memoir). After the ‘Dodgy Originals story’ had hit the papers, I was summoned ominously to my dean, Prof John Tooke, who probably had intended to give me a dressing down of major proportions. By the time we were able to meet, a few weeks later, the MHRA had already reprimanded Duchy Originals for misleading advertising which took most of the wind out of Tooke’s sail. The dressing down thus turned into something like “do you have to be so undiplomatic all the time?”.
Several months later, I was invited by the Science Media Centre, London, to give a lecture on the occasion of my retirement (Fiona Fox, the head of the SMC, had felt that, since my own University does not have the politeness to run a valedictory lecture for me, she will organize one for journalists). In that short lecture, I tried to summarize 19 years of research which inevitably meant briefly mentioning Charles and his foray into detox.
When I had finished, there were many questions from the journalists. Jenny Hope from the Daily Mail asked, “You mentioned snake-oil salesmen in your talk, and you also mentioned Prince Charles and his tinctures. Do you think that Prince Charles is a snake-oil salesman?” My answer was brief and to the point: “Yes“. The next day, this was all over the press. The Mail’s article was entitled ‘Charles? He’s just a snake-oil salesman: Professor attacks prince on ‘dodgy’ alternative remedies‘.
The advice of Tooke (who by then had left Exeter) to be more diplomatic had evidently not borne fruits (but the tinctures were discreetly taken off the market).
Diplomatic or honest?
This has been a question that I had to ask myself regularly during my 19 years at Exeter. For about 10 years, I had tried my best to walk the ‘diplomatic route’. When I realised that, in alternative medicine, the truth is much more important than diplomacy, I gradually changed … and despite all the hassle and hardship it brought me, I do not regret the decision.
In March 2020, ITV reported that a faith healer has been accused of “exploiting” people’s anxiety about the coronavirus crisis by selling a “plague protection kit” for £91. Bishop Climate Wiseman, head of the Kingdom Church in Camberwell, south London, has promised his followers the small bottle of oil and piece of red yarn will protect them from Covid-19. In a blog post, Bishop Wiseman claimed his concoction of cedar wood, hyssop and scarlet yarn acts as “an invisible barrier to the powers of darkness”. He wrote: “It is by faith that you can be saved from the coronavirus pandemic by covering yourself with the divine plague protection oil and wearing the scarlet yarn on your body. That is why I want to encourage you, if you haven’t done so already, to get your divine plague protection kit today!”
He claimed that the remedy was based on a passage from chapter 14 of the Old Testament Book of Leviticus. It reads: “Then he is to take the cedar wood, the hyssop, the scarlet yarn, and the live bird, dip them into the blood of the dead bird and the fresh water, and sprinkle the house seven times. In this way, he will make atonement for the house, and it will be clean.”
Bishop Wiseman told the PA news agency the church had sold more than 1,000 of the kits. “This is based on the Bible – I’m a Christian and there is a way that the Bible says to protect us from plagues.” One can also buy miracle money house blessing oil and anointed oil for court cases. On the Kingdom Church’s website, it claims thousands of people have been healed from “all sorts” of sickness and disease since it was founded in 2005.
Now, the Charity Commission has appointed an interim manager to the church following concerns raised by the National Secular Society about ‘plague protection kits’ sold by its bishop. England and Wales’s charity regulator announced that it appointed an interim manager to The Kingdom Church GB in February, who will “consider the charity’s future operation and viability”.
Elsewhere, the oil is advertised as follows:
Plagues Divine Protection Anointing Oil Have you been battling with countless amount of fear due to an economical wide spread of plaques and viruses? Then this Anointing Oil is for you.
The Plagues Divine Protection Anointing Oil was created by Master Prophet, Prophet Climate Wiseman through divine guidance and instruction from the Holy Spirit. This oil contains two biblical integrant which is biblically proven to remove plagues of all kind. These two Integrants are Hyssop and Cedar wood. The Bible clearly tells us in the book of Leviticus 14:51-53 “Then he is to take the cedar wood, the hyssop, the scarlet yarn and the live bird, dip them into the blood of the dead bird and the fresh water, and sprinkle the house seven times. He shall purify the house with the bird’s blood, the fresh water, the live bird, the cedar wood, the hyssop and the scarlet yarn. Then he is to release the live bird in the open fields outside the town. In this way he will make atonement for anointedoils
The commission said it had “serious ongoing concerns” about the charity’s administration and the financial relationship with its two subsidiary companies. It found the charity does not have a bank account and charity funds have instead been deposited into the charity’s subsidiaries’ bank accounts. It is investigating the legality of this relationship. The commission only appoints interim managers to charities “after very careful consideration” if there is misconduct or mismanagement in the administration of a charity, or if it is necessary or desirable to protect the charity’s property.
The post originally included claims that “every coronavirus and any other deadly thing” would “pass over” those using the oil and yarn. It was later edited to remove some specific references to coronavirus, but continued to claim people could “be saved from every pandemic” by using the oil and string.
On 20 February 2021, I published on my blog a comment on a new study of an Ayurvedic remedy for COVID-19. The study was in my view suspect, and I expressed this as follows:
I have the following concerns or questions about this trial:
- Why do the authors call it a pilot study? A pilot study is merely for testing the feasibility of a trial design and is not meant to yield definitive efficacy results.
- The authors state that the patients were asymptomatic yet in the discussion they claim they were asymptomatic or mildly symptomatic.
- Some of the effect sizes reported here are extraordinary and seem almost too good to be true.
- The claim of no adverse effect is implausible; even placebos would cause perceived adverse effects in a percentage of patients.
- If the study is solid and withstands the scrutiny of the raw data, it is of huge relevance for public health. So, why did the authors publish it in PHYTOMEDICINE, a relatively minor and little-known journal?
An article in The Economic Times’ reported this:
Patanjali Ayurved released what it called the first “evidence-based” medicine for Covid-19 on Friday. It claimed it has been “recognised by the WHO (World Health Organization) as an ayurvedic medicine for corona”. Patanjali promoter, yoga guru Baba Ramdev, released a scientific research paper in this regard at the launch, presided over by Union health minister Harsh Vardhan and transport minister Nitin Gadkari. The Ayurveda products maker said it has received a certification from the Ayush ministry. “Coronil has received the Certificate of Pharmaceutical Product (CoPP) from the Ayush section of Central Drugs Standard Control Organisation (CDSCO) as per the WHO certification scheme,” it said in a statement. Under the CoPP, Coronil can be exported to 158 countries, the company said, adding that based on the presented data, the ministry has recognised Coronil as medicine for “supporting measure in Covid-19”.
Am I the only one who fears that something is not entirely kosher about the study? (This is an honest question, and I would be pleased to receive answers from my readers)
What happened next is most puzzling. After putting it on Facebook several times, I got banned for 72 hours from posting this article or anything else on Facebook. When this period had elapsed, I put the article in question again on Facebook. Subsequently, I was banned again but this time for 7 days. Facebook gave the following explanation:
You can’t post or comment for 7 days
This is because your previous posts didn’t follow our Community Standards.
No one else can see these posts.
1 Mar
Your post goes against our Community Standards on misinformation that could cause physical harm
We usually offer the chance to request a review, and follow up if we’ve gotten decisions wrong.
We have fewer reviewers available at the moment because of the coronavirus (COVID-19) outbreak. We’re trying hard to prioritise reviewing content with the most potential for harm.
This means that we may not be able to follow up with you, though your feedback helps us do better in the future.
Thank you for understanding.
On Twitter, the hype had begun even before its text was available. Priti Gandhi, for instance, tweeted:
Yet another feather in India’s cap!! 1st evidence-based, CoPP-WHO GMP certified medicine for Covid-19 released today. Congratulations to @yogrishiramdev ji, @Ach_Balkrishna ji & the team of scie…
EDZARDERNST.COM An RCT on the efficacy of ayurvedic treatment on asymptomatic COVID-19 patients
________________________________
As I did not feel I had broken any rules, I protested against the bans each time. When the 2nd ban was over, I posted my article yet again and, sure enough, yesterday I got banned again, this time for 30 days. Here is how they let me know:
You can’t post or comment for 30 days
This is because you previously posted something that didn’t follow our Community Standards.
This post goes against our standards on misinformation that could cause physical harm, so only you can see it.
Learn more about updates to our standards. On Twitter, the hype had begun even before its text was available. Priti Gandhi, for instance, tweeted: Yet another feather in India’s cap!! 1st evidence-based, CoPP-WHO GMP certified medicine for Covid-19 released today. Congratulations to @yogrishiramdev ji, @Ach_Balkrishna ji & the team of scie…
EDZARDERNST.COM An RCT on the efficacy of ayurvedic treatment on asymptomatic COVID-19 patients
As the reason for the ban always seems to be the Ayurvedic study, I suspect that some party interested in the product is behind the complaints that lead to the bans. I find it extraordinary that I can be banned repeatedly without having done anything wrong and without my objections ever being considered.