critical thinking
This shocking paper presents 5 cases of patients with moderate to severe COVID-19 infections, 2 of them hospitalized in the intensive care unit, who were successfully treated with homeopathy. All 5 patients responded to homeopathic treatment in an unexpectedly short time span (in fact, it took up to 8 days), improving both physically and mentally.
The authors concluded that the present case series emphasizes the rapidity of response among moderate to severely ill patients to homeopathic treatment, when conventional medical options have been unable to relieve or shorten the disease. The observations described should encourage use of homeopathy in treating patients with COVID-19 during the acute phase of the disease.
If I hear about patients suffering from a cold, or tennis elbow, or otitis, or back pain, or allergy who responded to homeopathic treatment in an unexpectedly short time span, I tend to giggle and usually consider it a waste of time to explain that the observed outcome most likely is not a RESPONSE to homeopathic treatment but a non-causally related by-product. Correlation is not causation! What caused the outcome was, in fact, the natural history of the condition which would have improved even without homeopathy. To make this even clearer, I sometimes ask the homeopath: HOW DO YOU KNOW THAT THE PATIENT WOULD NOT HAVE IMPROVED EVEN FASTER IF YOU HAD NOT GIVEN HIM THE HOMEOPATHIC REMEDY? This question sometimes (sadly not always) leads to the realization that homeopathy may not have caused the outcome.
But when, in the middle of a pandemic during which millions of people died and continue to die, someone writes in a medical journal that 5 COVID patients responded to homeopathic treatment in an unexpectedly short time span, I feel compelled to disclose the statement as pure, unethical, irresponsible, and dangerous quackery.
The 5 patients with COVID-19 were hospitalized at a tertiary medical center in Jerusalem for moderate to severe
COVID-19-related symptoms. Each of them requested homeopathic treatment in addition to conventional therapy from the hospital’s ‘Center for Integrative Complementary Medicine’. All 5 patients were over 18 years old and had confirmed COVID-19 infection at the time of admission. They received their homeopathic medications as small round pills (globules); no further information about the homeopathic treatment was provided. Similarly, we also do not learn whether some patients who did not receive homeopathy recovered just as quickly (I am sure that worldwide thousands did), or whether some patients who did get homeopathic remedies failed to recover.
To make matters worse, the authors of this paper state this:
Several conclusions are evident from the cases presented:
1 homeopathy’s effect may be expected within minutes or, at most, hours;
2 contrary to classical homeopathic consultations, which may extend over an hour, correct medications for patients with acute COVID-19 symptoms may be determined in minutes;
3 there were no observable adverse effects to homeopathic treatment of COVID-19;
4 therapy can be administered via telehealth services, increasing safety of treating patients with active infection;
5 patient satisfaction was high; scoring their experience of homeopathic therapy on a 7-point scale, ranging
from “It greatly improved my condition” to “It greatly aggravated my condition,” all 5 patients indicated it
had greatly improved their condition.
The possibility that the outcomes are not causally related to the homeopathic treatment seems to have escaped the authors. The harm that can be done by such an article seems obvious: fans of homeopathy might be misled into assuming that homeopathy is an effective therapy for COVID infections and other serious conditions. It is not hard to imagine that this error would cost many lives.
The authors state in their article that, to the best of their knowledge, this is the first time that a tertiary medical center has permitted homeopathic therapy of patients under treatment for COVID-19-related illness.
I sincerely hope that it is also the last time!
Kneipp therapy goes back to Sebastian Kneipp (1821-1897), a catholic priest who was convinced to have cured himself of tuberculosis by using various hydrotherapies. Kneipp is often considered by many to be ‘the father of naturopathy’. Kneipp therapy consists of hydrotherapy, exercise therapy, nutritional therapy, phototherapy, and ‘order’ therapy (or balance). Kneipp therapy remains popular in Germany where whole spa towns live off this concept.
The obvious question is: does Kneipp therapy work? A team of German investigators has tried to answer it. For this purpose, they conducted a systematic review to evaluate the available evidence on the effect of Kneipp therapy.
A total of 25 sources, including 14 controlled studies (13 of which were randomized), were included. The authors considered almost any type of study, regardless of whether it was a published or unpublished, a controlled or uncontrolled trial. According to EPHPP-QAT, 3 studies were rated as “strong,” 13 as “moderate” and 9 as “weak.” Nine (64%) of the controlled studies reported significant improvements after Kneipp therapy in a between-group comparison in the following conditions:
- chronic venous insufficiency,
- hypertension,
- mild heart failure,
- menopausal complaints,
- sleep disorders in different patient collectives,
- as well as improved immune parameters in healthy subjects.
No significant effects were found in:
- depression and anxiety in breast cancer patients with climacteric complaints,
- quality of life in post-polio syndrome,
- disease-related polyneuropathic complaints,
- the incidence of cold episodes in children.
Eleven uncontrolled studies reported improvements in allergic symptoms, dyspepsia, quality of life, heart rate variability, infections, hypertension, well-being, pain, and polyneuropathic complaints.
The authors concluded that Kneipp therapy seems to be beneficial for numerous symptoms in different patient groups. Future studies should pay even more attention to methodologically careful study planning (control groups, randomisation, adequate case numbers, blinding) to counteract bias.
On the one hand, I applaud the authors. Considering the popularity of Kneipp therapy in Germany, such a review was long overdue. On the other hand, I am somewhat concerned about their conclusions. In my view, they are far too positive:
- almost all studies had significant flaws which means their findings are less than reliable;
- for most indications, there are only one or two studies, and it seems unwarranted to claim that Kneipp therapy is beneficial for numerous symptoms on the basis of such scarce evidence.
My conclusion would therefore be quite different:
Despite its long history and considerable popularity, Kneipp therapy is not supported by enough sound evidence for issuing positive recommendations for its use in any health condition.
They say, one has to try everything at least once – except line-dancing and incest. So, when I was invited to co-organize a petition, I considered it and thought: WHY NOT?
Here is the text (as translated by myself) of our petition to the German Medical Association:
Dear President Dr Reinhardt,
Dear Ms Lundershausen,
Mrs Held,
Dear Ms Johna,
We, the undersigned doctors, would like to draw your attention to the insistence of individual state medical associations on preserving “homeopathy” as a component of continuing medical education. We hope that you, by virtue of your office, will ensure a nationwide regulation so that this form of sham treatment [1], as has already happened in other European countries, can no longer call itself part of medicine.
We justify our request by the following facts:
- After the landmark vote in Bremen in September 2019 to remove “homeopathy” from the medical training regulations, 10 other state medical associations have so far followed Bremen’s example. For reasons of credibility and transparency, it would be desirable if the main features of the training content taught were not coordinated locally in the future, but centrally and uniformly across the country so that there is no “training tourism”. Because changes to a state’s own regulations of postgraduate training are only binding for the examination committee of the respective state, this does not affect national regulations but is reduced to only a symbolic character without sufficient effects on the portfolio of medical education nationwide.
- Medicine always works through the combination of a specifically effective part and non-specific placebo effects. By insisting on a pseudo-medical methodology – as is “homeopathy” represents in our opinion – patients are deprived of the specific effective part and often unnecessarily deprived of therapy appropriate to the indication. Tragically, it happens again and again that the “therapeutic window of opportunity” for an appropriate therapy is missed, tumors can grow to inoperable size, etc.
- Due to the insistence of individual state medical associations on the “homeopathic doctrine of healing” as part of the medical profession, we are increasingly exposed to the blanket accusation that, by tolerating this doctrine, we are supporting and promoting ways of thinking and world views that are detached from science. This is a dangerous situation, which in times of a pandemic manifests itself in misguided aggression reflected not just in vaccination skepticism and vaccination refusal, but also in unacceptable personal attacks and assaults on vaccinating colleagues in private practice.
Responsible:
Dr. med. Dent. Hans-Werner Bertelsen
Prof. Dr. med. Edzard Ernst
George A. Rausche
You can sign the petition here:
Static or motion manual palpation tests of the spine are commonly used by chiropractors and osteopaths to assess pain location and reproduction in low back pain (LBP) patients. But how reliable are they?
The purpose of this review was to evaluate the reliability and validity of manual palpation used for the assessment of LBP in adults. The authors systematically searched five databases from 2000 to 2019 and critically appraised the internal validity of studies using QAREL and QUADAS-2 instruments.
A total of 2023 eligible articles were identified, of which 14 were at low risk of bias. Evidence suggests that reliability of soft tissue structures palpation is inconsistent, and reliability of bony structures and joint mobility palpation is poor. Preliminary evidence was found to suggest that gluteal muscle palpation for tenderness may be valid in differentiating LBP patients with and without radiculopathy.
The authors concluded that the reliability of manual palpation tests in the assessment of LBP patients varies greatly. This is problematic because these tests are commonly used by manual therapists and clinicians. Little is known about the validity of these tests; therefore, their clinical utility is uncertain. High quality validity studies are needed to inform the clinical use of manual palpation tests.
I have repeatedly drawn attention to the fact that the diagnostic methods used by chiropractors and osteopaths are of uncertain or disproven validity (see for instance here, or here). Why is that important?
Imagine you consult a chiropractor or osteopath. Simply put, this is what is likely to happen:
- They listen to your complaint.
- They do a few tests which are of dubious validity.
- They give you a diagnosis that is meaningless.
- They treat you with manual therapies that are neither effective nor safe.
- You pay.
- They persuade you that you need many more sessions.
- You pay regularly.
- When eventually your pain has gone away, they persuade you to have useless maintenance treatment.
- You pay regularly.
In a nutshell, they have very little to offer … which explains why they attack everyone who dares to disclose this.
It has recently been reported that a Canadian naturopath claims he can treat autism with fecal transplants at a clinic in Mexico. The College of Naturopathic Physicians of B.C. has thus barred him stating that it has taken “extraordinary action” against Jason Klop in response to a complaint from a whistle-blowing former employee, who alleges that he manufactured these products in a “household lab” in B.C. without standard procedures or quality control.
While the complaint is under investigation, Klop cannot manufacture, advertise or sell fecal microbiota transplants (FMT). He’ll also be subject to random on-site audits to make sure he’s not violating his conditions.
This is the first public sign of concrete action by the college since CBC News reported on Klop’s business in January 2020 — nearly 20 months ago. Klop has been charging about $15,000 US for autistic children as young as two years old to have FMT treatment at a clinic near Tijuana. The process isn’t approved as a treatment of autism and carries serious risks of infection.
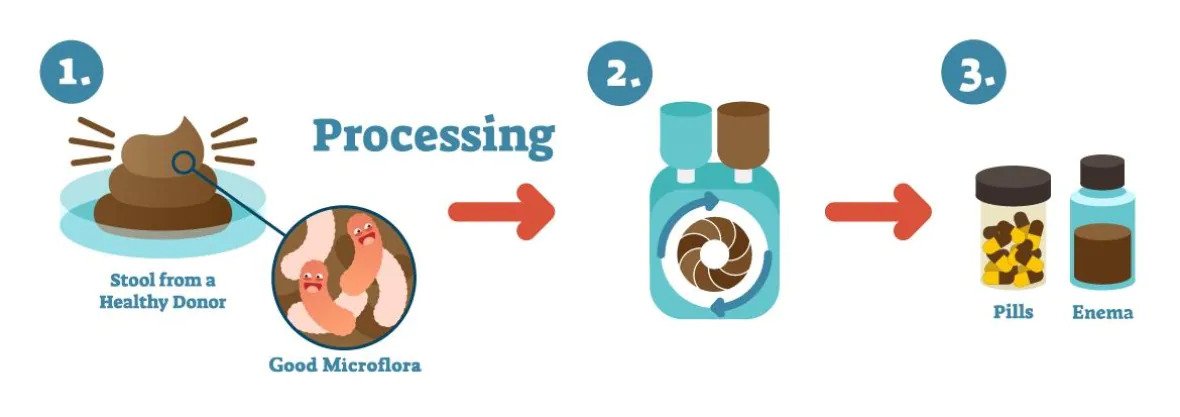
An illustration shows how fecal microbiota transplants are produced. (Vancouver Island Health Authority)
In a promotional video posted in January, Klop says he believes that “precision manipulation of the gut microbiome will solve every single chronic disease.” He also issued an affidavit boasting that he has a new lab that “produces the best and safest FMT materials in the world” and described the former employee who complained as “manifestly unreliable.” Klop argued that “lives are at stake” if he were to stop what he’s doing and described his therapy as a “life-saving measure.”
_____________________
Is there any evidence at all for FMT as a treatment of autism? A recent systematic review drew this conclusion: evidence from human studies suggesting beneficial effects of probiotic, prebiotic, and combination thereof, as well as fecal transplants in autism spectrum disorder, is limited and inconclusive.
I was alerted to this announcement by the Faculty of Homeopathy:
Faculty of Homeopathy Accredited Education
The role of Dentistry in Integrative Medicine and Homeopathy
Dentistry appears to be the Cinderella of healthcare and the importance of good oral health is hugely underestimated. The mouth is the portal into the rest of our bodies. There is increasing evidence proving that health of the oral cavity has strong links with the health of the rest of the body especially increasing risk of heart disease, low birth weight babies and type 2 diabetes. The aim of this webinar is to highlight the vital importance of dentistry and oral health in integrative medicine and why healthcare professionals need to work closely with dentists. It will also cover how, as homeopaths, we can appreciate symptoms in the mouth as indications of general health or disease and manage dental conditions.
THE TICKETS FOR THIS WEBINAR ARE LIMITED THEREFORE, PLEASE REGISTER NOW TO ENSURE ACCESS.
Some splendid platitudes there:
- the Cinderella of healthcare
- The mouth is the portal into the rest of our bodies
- health of the oral cavity has strong links with the health of the rest of the body…
But what about the importance of dentistry in integrative medicine? The importance of dentistry in medicine is fairly clear to me. However, what is the importance of dentistry in integrative medicine?
Even more puzzling seems the ‘role of dentistry in homeopathy’? What on earth do they mean by that? Perhaps they meant the ‘role of homeopathy in dentistry’?
And what is the role of homeopathy in dentistry? The British Homeopathic Dental Association should know, shouldn’t they? On their website, they explain that they are a group of dentists and dental care professionals that have an interest in using homeopathy alongside our dentistry.
On the basis of what evidence, you ask? They kindly provide an answer to that question:
In dentistry there is limited research though studies have shown improved bone healing around implants with Symphytum and reduced discomfort and improved healing time with ulcers and beneficial in oral lichen planus. These studies have small numbers and are not generally acepted as stong evidence.
Are they trying to tell us that there is no good evidence? Looks like it, doesn’t it? In this case, the above Webinar seems rather superfluous.
For those of you who want to save the money for the tickets, here is a full and evidence-based summary of all the conditions where homeopathy might be helpful in dentistry:
–
–
–
–
–
–
–
–
–
–
–
–
–
–
–
–
THE END
Cannabis seems often to be an emotional subject where more heat than light is generated. Does it work for chronic pain? This cannot be such a difficult question to answer definitively. Yet, systematic reviews have provided conflicting results due, in part, to limitations of analytical approaches and interpretation of findings.
A new systematic review is therefore both necessary and welcome. It aimed at determining the benefits and harms of medical cannabis and cannabinoids for chronic pain. Included were all randomised clinical trials of medical cannabis or cannabinoids versus any non-cannabis control for chronic pain at ≥1-month follow-up.
A total of 32 trials with 5174 adult patients were included, 29 of which compared medical cannabis or cannabinoids with placebo. Medical cannabis was administered orally (n=30) or topically (n=2). Clinical populations included chronic non-cancer pain (n=28) and cancer-related pain (n=4). Length of follow-up ranged from 1 to 5.5 months.
Compared with placebo, non-inhaled medical cannabis probably results in a small increase in the proportion of patients experiencing at least the minimally important difference (MID) of 1 cm (on a 10 cm visual analogue scale (VAS)) in pain relief (modelled risk difference (RD) of 10% (95% confidence interval 5% to 15%), based on a weighted mean difference (WMD) of −0.50 cm (95% CI −0.75 to −0.25 cm, moderate certainty)). Medical cannabis taken orally results in a very small improvement in physical functioning (4% modelled RD (0.1% to 8%) for achieving at least the MID of 10 points on the 100-point SF-36 physical functioning scale, WMD of 1.67 points (0.03 to 3.31, high certainty)), and a small improvement in sleep quality (6% modelled RD (2% to 9%) for achieving at least the MID of 1 cm on a 10 cm VAS, WMD of −0.35 cm (−0.55 to −0.14 cm, high certainty)). Medical cannabis taken orally does not improve emotional, role, or social functioning (high certainty). Moderate certainty evidence shows that medical cannabis taken orally probably results in a small increased risk of transient cognitive impairment (RD 2% (0.1% to 6%)), vomiting (RD 3% (0.4% to 6%)), drowsiness (RD 5% (2% to 8%)), impaired attention (RD 3% (1% to 8%)), and nausea (RD 5% (2% to 8%)), but not diarrhoea; while high certainty evidence shows greater increased risk of dizziness (RD 9% (5% to 14%)) for trials with <3 months follow-up versus RD 28% (18% to 43%) for trials with ≥3 months follow-up; interaction test P=0.003; moderate credibility of subgroup effect).
The authors concluded that moderate to high certainty evidence shows that non-inhaled medical cannabis or cannabinoids results in a small to very small improvement in pain relief, physical functioning, and sleep quality among patients with chronic pain, along with several transient adverse side effects, compared with placebo.
This is a high-quality review. Its findings will disappoint the many advocates of cannabis as a therapy for chronic pain management. The bottom line, I think, seems to be that cannabis works but the effect is not very powerful, while we have treatments for managing chronic pain that are both more effective and arguably less risky. So, its place in clinical routine is debatable.
PS
Cannabis is, of course, a herbal remedy and therefore belongs to so-called alternative medicine (SCAM). Yet, I am aware that the medical cannabis preparations used in most studies are based on single cannabinoids which makes them conventional medicines.
Diabetic polyneuropathy is a prevalent, potentially disabling condition. Evidence-based treatments include specific anticonvulsants and antidepressants for pain management. All current guidelines advise a personalized approach with a low-dose start that is tailored to the maximum response having the least side effects or adverse events. Homeopathy has not been shown to be effective, but it is nevertheless promoted by many homeopaths as an effective therapy.
This study assessed the efficacy of individualized homeopathic medicines in the management of diabetic polyneuropathy. A multi-centric double-blind, placebo-controlled, randomized clinical trial was conducted by the Indian Central Council for Research in Homoeopathy at six centers with a sample size of 84. Based on earlier observational studies and repertorial anamnesis of DDSP symptoms 15 homeopathic medicines were shortlisted and validated scales were used for evaluating the outcomes post-intervention. The primary outcome measure was a change in Neuropathy Total Symptom Score-6 (NTSS-6) from baseline to 12 months. Secondary outcomes included changes in peripheral nerve conduction study (NCS), World Health Organization Quality of Life BREF (WHOQOL-BREF) and Diabetic Neuropathy Examination (DNE) score at 12 months.
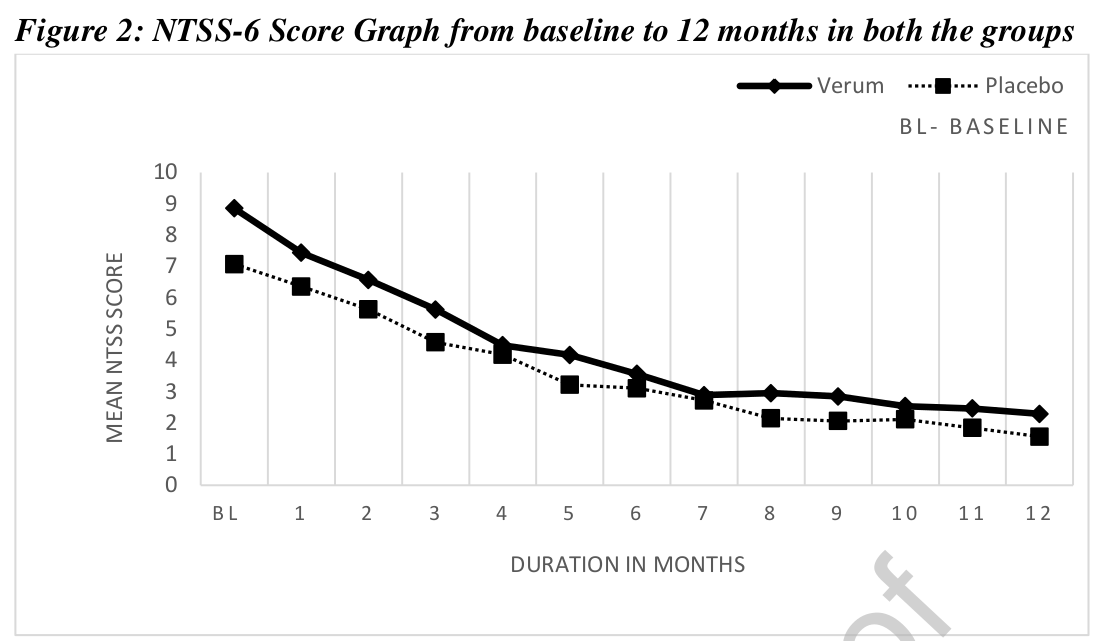
Data of 68 enrolled cases were considered for data analysis. A statistically significant difference (p<0.014) was found in NTSS-6 post-intervention in the Verum group. A positive trend was noted for the Verum group as per the graph plotted for DNE score and assessment done for NCS. No significant difference was found between the groups for WHOQOL-Bref. Out of 15 pre-identified homeopathic medicines, 11 medicines were prescribed in potencies in ascending order from 6C to 1M.
The authors refrain from drawing conclusions about the efficacy of their homeopathic treatment (which is more than a little odd, as their stated aim was to assess the efficacy of individualized homeopathic medicines in the management of diabetic polyneuropathy). So, please allow me to do it for them:
The findings of this study confirm that homeopathy is a useless treatment.
The General Chiropractic Council (GCC) regulates chiropractors in the UK, Isle of Man, and Gibraltar to ensure the safety of patients undergoing chiropractic treatment. The GCC sets the standards of chiropractic practice and professional conduct that all chiropractors must meet.

By providing a lengthy ruling in the case of the late John Lawler and his chiropractor, Arlene Scholten, the GCC has recently established new standards for chiropractors working in the UK, Isle of Man, and Gibraltar (see also today’s article in The Daily Mail). If I interpret the GCC’s ruling correctly, a UK chiropractor is henceforth allowed to do all of the following things without fearing to get reprimanded, as long as he or she produces evidence that the deeds were done not with malicious intentions but in a state of confusion and panic:
- Treat a patient with treatments that are contraindicated.
- Fail to obtain informed consent.
- Pose as a real doctor without informing the patient that the practitioner is just a chiropractor who has never been near a medical school.
- Cause the death of a patient by treatment to the neck.
- Administer first aid in a way that makes matters worse.
- Tell lies to the ambulance men who consequently failed to employ a method of transport that would save the patient’s life.
- Keep inaccurate patient records that conceal what treatments were administered.
In previous years, the job of a chiropractor had turned out to be demanding, difficult, and stressful. This was due not least to the GCC’s professional standards which UK chiropractors were obliged to observe. The code of the GCC stated prominently that “our overall purpose is to protect the public.”
All this is now a thing of the past.
The new ruling changed everything. Now, UK chiropractors can relax and can happily pursue their true devotion, namely to keep their bank manager happy, while not worrying too much about the welfare and health of their patients.
In the name of all UK chiropractors, I herewith express my thanks to the GCC for unashamedly protecting first and foremost the interests of their members, while tacitly discarding medical ethics and evidently not protecting the public.
MAKE CHIROPRACTIC GREAT AGAIN!
Homeopaths believe that their remedies work for every condition imaginable and that naturally includes irritable bowel syndrome (IBS). But what does the evidence show?
The aim of this pilot study was to evaluate the efficacy of individualized homeopathic treatment in patients with IBS. The study was carried out at the National Homeopathic Hospital of the Secretary of Health, Mexico City, Mexico and included 41 patients: 3 men and 38 women, mean age 54 ± 14.89 years, diagnosed with IBS as defined by the Rome IV Diagnostic criteria. Single individualized homeopathics were prescribed for each patient, taking into account all presenting symptoms, clinical history, and personality via repertorization using RADAR Homeopathic Software. The homeopathic remedies were used at the fifty-millesimal (LM) potency per the Mexican Homeopathic Pharmacopoeia starting with 0/1 and increasing every month (0/2, 0/3, 0/6). Severity scales were applied at the beginning of treatment and every month for 4 months of treatment. The evaluation was based on comparing symptom severity scales during treatment.
The results demonstrated that 100% of patients showed some improvement and 63% showed major improvement or were cured. The study showed a significant decrease in the severity of symptom scores 3 months after the treatment, with the pain score showing a decrease already one month after treatment.
The authors state that the results highlight the importance of individualized medicine regimens using LM potency, although the early decrease in pain observed could also be due to the fact that Lycopodium clavatum and Nux vomica were the main homeopathic medicine prescribed, and these medicines contain many types of alkaloids, which have shown significant analgesic effects on pain caused by physical and chemical stimulation.
The authors concluded that this pilot study suggests that individualized homeopathic treatment using LM potencies benefits patients with IBS.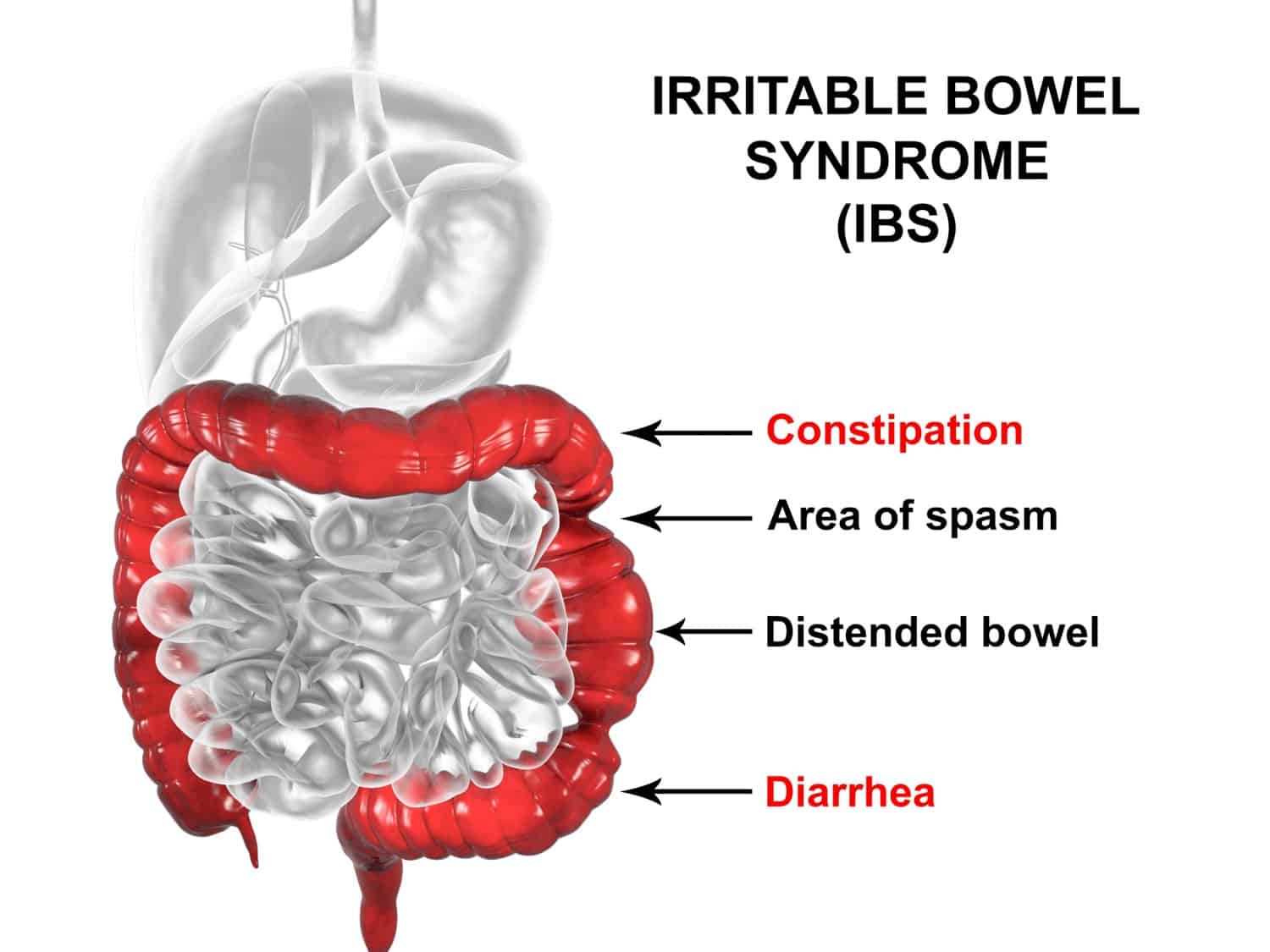
Where to begin?
Let me mention just a few rather obvious points:
- A pilot study is not for evaluating the efficacy, but for testing the feasibility of a definitive trial.
- The study has no control group, therefore the outcome cannot be attributed to the treatment but is most likely due to a mixture of placebo effects, regression towards the mean, and natural history of IBS.
- The conclusions are not warranted.
- The paper was published in the infamous Altern Ther Health Med.
Just to make sure that nobody is fooled into believing that homeopathy might nonetheless be effective for IBS. Here is what the Cochrane review on this subject tells us: no firm conclusions regarding the effectiveness and safety of homeopathy for the treatment of IBS can be drawn. Further high quality, adequately powered RCTs are required to assess the efficacy and safety of clinical and individualised homeopathy for IBS compared to placebo or usual care.
In my view, even the conclusion of the Cochrane review is odd and slightly misleading. The correct conclusion would have been something more to the point:
THE CURRENT TRIAL EVIDENCE FAILS TO INDICATE THAT HOMEOPATHY IS AN EFFECTIVE TREATMENT FOR IBS.