chiropractic
Gosh, we in the UK needed that boost of jingoism (at least, if you are white, non-Jewish and equipped with a British passport)! But it’s all very well to rejoice at the news that we have a new little Windsor. With all the joy and celebration, we must not forget that the blue-blooded infant might be in considerable danger!
I am sure that chiropractors know what I am talking about.
KISS (Kinematic Imbalance due to Suboccipital Strain) is a term being used to describe a possible causal relation between imbalance in the upper neck joints in infants and symptoms like postural asymmetry, development of asymmetric motion patterns, hip problems, sleeping and eating disorders. Chiropractors are particularly fond of KISS. It is a problem that chiropractors tend to diagnose in new-borns.
This website explains further:
The kinematic imbalances brought on by the suboccipital strain at birth give rise to a concept in which symptoms and signs associated with the cervical spine manifest themselves into two easily recognizable clinical presentations. The leading characteristic is a fixed lateroflexion [called KISS I] or fixed retroflexion [KISS II]. KISS I may be associated with torticollis, asymmetry of the skull, C–scoliosis of the neck and trunk, asymmetry of the gluteal area and of the limbs, and retardation of the motor development of one side. KISS II, on the other hand, displays hyperextension during sleep, occipital flattening that may be asymmetrical, hunching of the shoulders, fixed supination of the arms, orofacial muscular hypotonia, failure to lift the trunk from a ventral position, and difficulty in breast feeding on one side. [34] The leading trademarks of both KISS I and KISS II are illustrated in Figure 1. [31]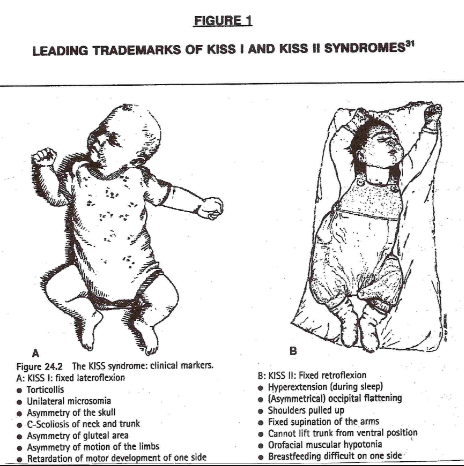
In essence, these birth experiences lay the groundwork for rationalizing the wisdom of providing chiropractic healthcare to the pediatric population…
END OF QUOTE
KISS must, of course, be treated with chiropractic spinal manipulation: the manual adjustment is the most common, followed by an instrument adjustment. This removes the neurological stress, re-balances the muscles and normal head position. Usually a dramatic change can be seen directly after the appropriate adjustment has been given…
Don’t frown! We all know that we can trust our chiropractors.
Evidence?
Do you have to insist on being a spoil-sport?
Alright, alright, the evidence tells a different story. A systematic review concluded that, given the absence of evidence of beneficial effects of spinal manipulation in infants and in view of its potential risks, manual therapy, chiropractic and osteopathy should not be used in infants with the KISS-syndrome, except within the context of randomised double-blind controlled trials.
And this means I now must worry for a slightly different reason: we all know that the new baby was born into a very special family – a family that seems to embrace every quackery available! I can just see the baby’s grandfather recruiting a whole range of anti-vaccinationists, tree-huggers, spoon-benders, homeopaths, faith healers and chiropractors to look after the new-born.
By Jove, one does worry about one’s Royals!
I have often criticised papers published by chiropractors.
Not today!
This article is excellent and I therefore quote extensively from it.
The objective of this systematic review was to investigate, if there is any evidence that spinal manipulations/chiropractic care can be used in primary prevention (PP) and/or early secondary prevention in diseases other than musculoskeletal conditions. The authors conducted extensive literature searches to locate all studies in this area. Of the 13.099 titles scrutinized, 13 articles were included (8 clinical studies and 5 population studies). They dealt with various disorders of public health importance such as diastolic blood pressure, blood test immunological markers, and mortality. Only two clinical studies could be used for data synthesis. None showed any effect of spinal manipulation/chiropractic treatment.
The authors concluded that they found no evidence in the literature of an effect of chiropractic treatment in the scope of PP or early secondary prevention for disease in general. Chiropractors have to assume their role as evidence-based clinicians and the leaders of the profession must accept that it is harmful to the profession to imply a public health importance in relation to the prevention of such diseases through manipulative therapy/chiropractic treatment.
In addition to this courageous conclusion (the paper is authored by a chiropractor and published in a chiro journal), the authors make the following comments:
Beliefs that a spinal subluxation can cause a multitude of diseases and that its removal can prevent them is clearly at odds with present-day concepts, as the aetiology of most diseases today is considered to be multi-causal, rarely mono-causal. It therefore seems naïve when chiropractors attempt to control the combined effects of environmental, social, biological including genetic as well as noxious lifestyle factors through the simple treatment of the spine. In addition, there is presently no obvious emphasis on the spine and the peripheral nervous system as the governing organ in relation to most pathologies of the human body.
The ‘subluxation model’ can be summarized through several concepts, each with its obvious weakness. According to the first three, (i) disturbances in the spine (frequently called ‘subluxations’) exist and (ii) these can cause a multitude of diseases. (iii) These subluxations can be detected in a chiropractic examination, even before symptoms arise. However, to date, the subluxation has been elusive, as there is no proof for its existence. Statements that there is a causal link between subluxations and various diseases should therefore not be made. The fourth and fifth concepts deal with the treatment, namely (iv) that chiropractic adjustments can remove subluxations, (v) resulting in improved health status. However, even if there were an improvement of a condition following treatment, this does not mean that the underlying theory is correct. In other words, any improvement may or may not be caused by the treatment, and even if so, it does not automatically validate the underlying theory that subluxations cause disease…
Although at first look there appears to be a literature on this subject, it is apparent that most authors lack knowledge in research methodology. The two methodologically acceptable studies in our review were found in PubMed, whereas most of the others were identified in the non-indexed literature. We therefore conclude that it may not be worthwhile in the future to search extensively the non-indexed chiropractic literature for high quality research articles.
One misunderstanding requires some explanations; case reports are usually not considered suitable evidence for effect of treatment, even if the cases relate to patients who ‘recovered’ with treatment. The reasons for this are multiple, such as:
- Individual cases, usually picked out on the basis of their uniqueness, do not reflect general patterns.
- Individual successful cases, even if correctly interpreted must be validated in a ‘proper’ research design, which usually means that presumed effect must be tested in a properly powered and designed randomized controlled trial.
- One or two successful cases may reflect a true but very unusual recovery, and such cases are more likely to be written up and published as clinicians do not take the time to marvel over and spend time on writing and publishing all the other unsuccessful treatment attempts.
- Recovery may be co-incidental, caused by some other aspect in the patient’s life or it may simply reflect the natural course of the disease, such as natural remission or the regression towards the mean, which in human physiology means that low values tend to increase and high values decrease over time.
- Cases are usually captured at the end because the results indicate success, meaning that the clinical file has to be reconstructed, because tests were used for clinical reasons and not for research reasons (i.e. recorded by the treating clinician during an ordinary clinical session) and therefore usually not objective and reproducible.
- The presumed results of the treatment of the disease is communicated from the patient to the treating clinician and not to a third, neutral person and obviously this link is not blinded, so the clinician is both biased in favour of his own treatment and aware of which treatment was given, and so is the patient, which may result in overly positive reporting. The patient wants to please the sympathetic clinician and the clinician is proud of his own work and overestimates the results.
- The long-term effects are usually not known.
- Further, and most importantly, there is no control group, so it is impossible to compare the results to an untreated or otherwise treated person or group of persons.
Nevertheless, it is common to see case reports in some research journals and in communities with readers/practitioners without a firmly established research culture it is often considered a good thing to ‘start’ by publishing case reports.
Case reports are useful for other reasons, such as indicating the need for further clinical studies in a specific patient population, describing a clinical presentation or treatment approach, explaining particular procedures, discussing cases, and referring to the evidence behind a clinical process, but they should not be used to make people believe that there is an effect of treatment…
For groups of chiropractors, prevention of disease through chiropractic treatment makes perfect sense, yet the credible literature is void of evidence thereof. Still, the majority of chiropractors practising this way probably believe that there is plenty of evidence in the literature. Clearly, if the chiropractic profession wishes to maintain credibility, it is time seriously to face this issue. Presently, there seems to be no reason why political associations and educational institutions should recommend spinal care to prevent disease in general, unless relevant and acceptable research evidence can be produced to support such activities. In order to be allowed to continue this practice, proper and relevant research is therefore needed…
All chiropractors who want to update their knowledge or to have an evidence-based practice will search new information on the internet. If they are not trained to read the scientific literature, they might trust any article. In this situation, it is logical that the ‘believers’ will choose ‘attractive’ articles and trust the results, without checking the quality of the studies. It is therefore important to educate chiropractors to become relatively competent consumers of research, so they will not assume that every published article is a verity in itself…
END OF QUOTES
YES, YES YES!!!
I am so glad that some experts within the chiropractic community are now publishing statements like these.
This was long overdue.
How was it possible that so many chiropractors so far failed to become competent consumers of research?
Do they and their professional organisations not know that this is deeply unethical?
Actually, I fear they do and did so for a long time.
Why then did they not do anything about it ages ago?
I fear, the answer is as easy as it is disappointing:
If chiropractors systematically trained to become research-competent, the chiropractic profession would cease to exist; they would become a limited version of physiotherapists. There is simply not enough positive evidence to justify chiropractic. In other words, as chiropractic wants to survive, it has little choice other than remaining ignorant of the current best evidence.
This week, I find it hard to decide where to focus; with all the fuzz about ‘Homeopathy Awareness Week’ it is easy to forget that our friends, the chiros are celebrating Chiropractic Awareness Week (9-15 April). On this occasion, the British Chiropractic Association (BCA), for instance, want people to keep moving to make a positive impact on managing and preventing back and neck pain.
Good advice! In a recent post, I even have concluded that people should “walk (slowly and cautiously) to the office of their preferred therapist, have a little rest there (say hello to the staff perhaps) and then walk straight back home.” The reason for my advice is based on the fact that there is precious little evidence that the spinal manipulations of chiropractors make much difference plus some worrying indications that they may cause serious damage.
It seems to me that, by focussing their PR away from spinal manipulations and towards the many other things chiropractors sometimes do – they often call this ‘adjunctive therapies’ – there is a tacit admission here that the hallmark intervention of chiros (spinal manipulation) is of dubious value.
A recent article entitled ‘Spinal Manipulative Therapy and Other Conservative Treatments for Low Back Pain: A Guideline From the Canadian Chiropractic Guideline Initiative’ seems to confirm this impression. Its objective was to develop a clinical practice guideline on the management of acute and chronic low back pain (LBP) in adults. The specific aim was to develop a guideline to provide best practice recommendations on the initial assessment and monitoring of people with low back pain and address the use of spinal manipulation therapy (SMT) compared with other commonly used conservative treatments.
The topic areas were chosen based on an Agency for Healthcare Research and Quality comparative effectiveness review, specific to spinal manipulation as a non-pharmacological intervention. The panel updated the search strategies in Medline and assessed admissible systematic reviews and randomized controlled trials. Evidence profiles were used to summarize judgments of the evidence quality and link recommendations to the supporting evidence. Using the Evidence to Decision Framework, the guideline panel determined the certainty of evidence and strength of the recommendations. Consensus was achieved using a modified Delphi technique. The guideline was peer reviewed by an 8-member multidisciplinary external committee.
For patients with acute (0-3 months) back pain, we suggest offering advice (posture, staying active), reassurance, education and self-management strategies in addition to SMT, usual medical care when deemed beneficial, or a combination of SMT and usual medical care to improve pain and disability. For patients with chronic (>3 months) back pain, we suggest offering advice and education, SMT or SMT as part of a multimodal therapy (exercise, myofascial therapy or usual medical care when deemed beneficial). For patients with chronic back-related leg pain, we suggest offering advice and education along with SMT and home exercise (positioning and stabilization exercises).
The authors concluded that a multimodal approach including SMT, other commonly used active interventions, self-management advice, and exercise is an effective treatment strategy for acute and chronic back pain, with or without leg pain.
I find this paper most interesting and revealing. Considering that it originates from the ‘Canadian Chiropractic Guideline Initiative’, it is remarkably shy about recommending SMT – after all their vision is “To enhance the health of Canadians by fostering excellence in chiropractic care.” They are thus not likely to be overly critical of the treatment chiropractors use most, i. e. SMT.
Perhaps this is also the reason why, in their conclusion, they seem to have rather a large blind spot, namely the risks of SMT. I have commented on this issue more often than I care to remember. Most recently, I posted this:
The reason why my stance, as expressed on this blog and elsewhere, is often critical about certain alternative therapies is thus obvious and transparent. For none of them (except for massage) is the risk/benefit balance positive. And for spinal manipulation, it even turns out to be negative. It goes almost without saying that responsible advice must be to avoid treatments for which the benefits do not demonstrably outweigh the risks.
HAPPY CHIROPRACTIC AWARENESS WEEK EVERYONE!
Did you know that chiropractic is a religion?
Well, not quite but almost.
DD Palmer seriously toyed with the idea of turning chiropractic into a religion.
And rightly so!
In the absence of evidence, belief is everything.
And this is why, to this day, so many chiropractors bank (a most appropriate term in this context!) on belief rather than evidence.
Look, for instance at this lovely advertisement I found on Twitter (there are many more, but this one has to stand for the many).
Seven common benefits of chiropractic care!?!
Beneath the picture of a pathologically straight spine – if that is what chiro does to you, avoid it at all cost! – we see the name of the ‘doctor’ who seems to have designed this impressive picture. ‘Dr’ Schluter is even more versatile than his pretty advertisement implies; he also seems to treat newborn babies! And on his website he also tells us that he is able to treat allergies:
You may be surprised to find that chiropractic can do a great deal to alleviate some allergies. Allergies are very common and we become so used to their effect on us that we tend to ignore their symptoms. And many people are unaware of the gradual decline in health that results. Chiropractic treatment didn’t necessarily set out specifically to provide care for allergies, but due to the nature of the chiropractic care and its effect on the nervous system, it has been shown to help.
If we look at some of the common signs of allergies we find that they include some unexpected examples. Not only do we find the usual ones – asthma, sinus congestion, sneezing, itchy eyes, skin rashes and running nose – but also weight gain, Acne and even fluid retention and heartburn.
Many people approach the problem of allergies as though all allergens affect everyone in the same way; this is not the case. Because we are individuals, different allergens affect each of us in differing ways. Some allergens affect some and not others. Consequently treating the condition must be approached on this basis of individuality.
It may not be the pet fur or dried saliva that is kicked up as your pooch washes and scratches; it may also not be the pollen, grass dust or other one of the many irritants in the air at any one time. It could be that due to a misalignment of the spine (or subluxation), mild though it may be, the nervous system is finding it difficult to help the body adapt to its surroundings and is therefore unable to deal with the necessary adjustments.
As an individual you need to treat your body’s physical and nervous system as such. You could be, without even being aware of it, in a generally stressed condition – this may be through lack of sleep, poor nutrition or any one of a combination of the many other stressors affecting us daily. Suddenly you find that with the first spring pollen dust that comes along you begin to wheeze and sneeze!
You may not have previously connected chiropractors and allergies but, for you or someone you know, the connection could help.
Schluter Chiropractic works on the principle of reducing interference so the nervous system and body can work better. Providing that any symptom or condition (including pain) is occurring as a result of nerve interference from vertebral subluxation, there is a very good chance that it will improve with chiropractic care.
END OF QUOTE
Wise words indeed.
Like most chiros, ‘Dr’ Schulter seems to be a true miracle-worker; and because he can do miracles, he does not need to be rational or concerned about evidence or worried about telling the truth.
For Christ sake, it’s Easter!
We ought to show a bit of belief!!!
Why?
Because without it, the benefits of chiropractic would be just an illusion.
Chiropractic for kids? Yes, many chiropractors advocate (and earn good money with) it, yet it has been pointed out ad nauseam that the claim of being able of treating paediatric conditions is bogus (in fact, the BCA even lost a famous court case over this issue). But evidence does rarely seem to stop a chiro on a mission!
This website shows us how UK chiropractors plan to educate colleagues in ‘paediatric chiropractic’.
START OF QUOTE
INSPIRAL PAEDIATRIC SEMINARS ……..KIDS DYNAMIC DEVELOPMENT
- Join us for an exciting weekend of learning and skills development, in a supportive, enjoyable environment
- Learn the latest in Chiropractic Paediatrics from two world class leaders whose seminars receive rave reviews & letters of gratitude
- Increase your confidence and certainty in working with families in your community
- Fri 7th September 2-6pm, Sat 8th 9-6pm, Sun 9th 9-1pm I
- Investment £649 Earlybird ends August 15th Late fee £679
- Inclusions: Notes, Lunch on Saturday, onsite parking Park Inn Hotel, Bath Rd, Sipson, Heathrow UB7 0DU
NEURODEVELOPMENT
The seminar offers a neurological approach to healthy development in babies & children. It provides clinically relevant assessment, adjusting & clinical decision making. The focus will be on a Chiropractic wellness paradigm with a collaborative approach to promote healthy outcomes across the infant to adolescent years.
SAFE ADJUSTING
This is a hands-on program with a focus on neuro – developmentally appropriate adjusting of the spine and cranial dural system for health. We address some of the leading challenges with infant health and development, and teach exciting home care plans to facilitate optimum development.
YOUR TEACHERS
Genevieve & Rosemary Keating are leaders in Chiropractic paediatric health, learning & development.
Both are experienced Chiropractors, Facilitators, Diplomates of the American Chiropractic Neurology Board and Master Practitioners of Neuro Linguistics.
Rosemary holds a Masters in Chiropractic Paediatrics, and Genevieve is completing her PhD in Early Childhood Development.
END OF QUOTE
The event is hosted and organised by the ‘United Chiropractic Association UK’ (UCA), an organisation with a mission to ensure the public has access to vitalistic chiropractic care, which claims that chiropractors provide care that is safe. Because the techniques used by chiropractors are acquired over years of study and experience, chiropractors have an enviable safety record. In fact, in the words of a classic New Zealand study, chiropractic care is “remarkably safe.” Chiropractors use the latest methods. After years of study, licensing examinations and continuing education seminars, chiropractors in the United Kingdom are at the top of their game, using proven techniques and natural methods to help you get well and stay well.
The UCA is firmly rooted in the gospel of the founding fathers (D D Palmer, B J Palmer etc.): Chiropractic is concerned with the preservation and restoration of health, and focuses particular attention on the subluxation. A subluxation is a complex of functional and/or structural and/or pathological articular changes that compromise neural integrity and may influence organ system function and general health. A subluxation is evaluated, diagnosed, and managed through the use of chiropractic procedures based on the best available rational and empirical evidence. Subluxation is a fundamental axiom of the Chiropractic profession. The World Federation of Chiropractors (WFC) policy statement reaffirms the use of the term vertebral subluxation and it is defined succinctly and accepted by the World Health Organisation (WHO).
Thus, the UCA seems to subscribe to both principles of the Palmers. The first is subluxation and the second is profit.
_________________________________________________________________________________
Now, now, now – I must not be so sarcastic.
Try something constructive, Edzard!
You are absolutely correct, Edzard.
Here it is, my constructive contribution to this event:
I herewith offer the UCA to give two lectures during their course; one about the importance of critical thinking in healthcare, and one reviewing the evidence for and against chiropractic for paediatric conditions.
Chiropractors are fast giving up the vitalistic and obsolete concepts of their founding fathers, we are told over and over again. But are these affirmations true? There are good reasons to be sceptical. Take this recent paper, for instance.
The objective of this survey was to investigate the proportion of Australian chiropractic students who hold non-evidence-based beliefs in the first year of study and to determine the extent to which they may be involved in non-musculoskeletal health conditions.
Students from two Australian chiropractic programs were invited to answer a questionnaire on how often they would give advice on 5 common health conditions in their future practices, as well as to provide their opinion on whether chiropractic spinal adjustments could prevent or help seven health-related conditions.
The response rate of this survey was 53%. Students were highly likely to offer advice on a range of non-musculoskeletal conditions. The proportions were lowest in first year and highest the final year. For instance, 64% of students in year 4/5 believed that spinal adjustments improve the health of infants. Also, high numbers of students held non-evidence-based beliefs about ‘chiropractic spinal adjustments’ which tended to occur in gradually decreasing in numbers in sequential years, except for 5th and final year, when a reversal of the pattern occurred.
The authors concluded that new strategies are required for chiropractic educators if they are to produce graduates who understand and deliver evidence-based health care and able to be part of the mainstream health care system.
This is an interesting survey, but I think its conclusion is wrong!
- Educators do not require ‘new strategies’, I would argue; they simply need to take their duty of educating students seriously – educating in this context does not mean brain-washing, it means teaching facts and evidence-based practice. And this is were any concept of true education would run into problems: it would teach students that chiropractic is built on sand.
- Conclusions need to be based on the data presented. Therefore, the most fitting conclusion, in my view, is that chiropractic students are currently being educated such that, once let loose on the unsuspecting and often all too gullible public, they will be a menace and a serious danger to public health.
You might say that this survey is from Australia and that the findings therefore do not necessarily apply to other countries. Correct! However, I very much fear that elsewhere the situation is similar or perhaps even worse. And my fear does not come out of thin air, it is based on things we have discussed before; see for instance these three posts:
Chiropractic education seems to be a form of religious indoctrination
What are the competencies of a ‘certified paediatric doctor of chiropractic’?
But I would be more than willing to change my mind – provided someone can show me good evidence to the contrary.
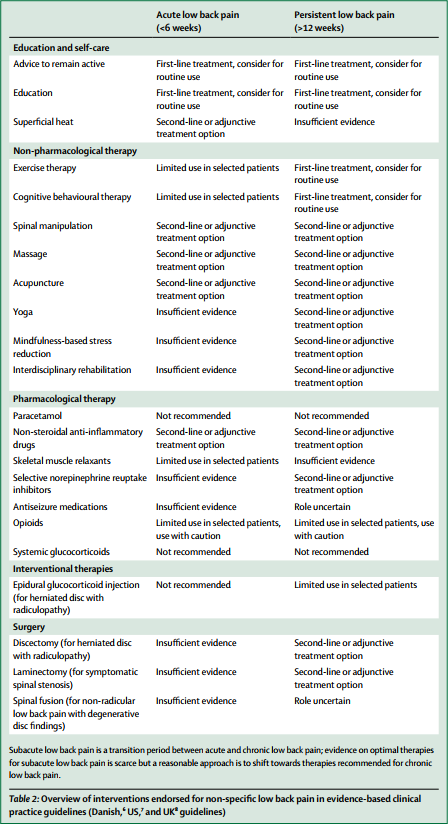
The media have (rightly) paid much attention to the three Lancet-articles on low back pain (LBP) which were published this week. LBP is such a common condition that its prevalence alone renders it an important subject for us all. One of the three papers covers the treatment and prevention of LBP. Specifically, it lists various therapies according to their effectiveness for both acute and persistent LBP. The authors of the article base their judgements mainly on published guidelines from Denmark, UK and the US; as these guidelines differ, they attempt a synthesis of the three.
Several alternative therapist organisations and individuals have consequently jumped on the LBP bandwagon and seem to feel encouraged by the attention given to the Lancet-papers to promote their treatments. Others have claimed that my often critical verdicts of alternative therapies for LBP are out of line with this evidence and asked ‘who should we believe the international team of experts writing in one of the best medical journals, or Edzard Ernst writing on his blog?’ They are trying to create a division where none exists,
The thing is that I am broadly in agreement with the evidence presented in Lancet-paper! But I also know that things are a bit more complex.
Below, I have copied the non-pharmacological, non-operative treatments listed in the Lancet-paper together with the authors’ verdicts regarding their effectiveness for both acute and persistent LBP. I find no glaring contradictions with what I regard as the best current evidence and with my posts on the subject. But I feel compelled to point out that the Lancet-paper merely lists the effectiveness of several therapeutic options, and that the value of a treatment is not only determined by its effectiveness. Crucial further elements are a therapy’s cost and its risks, the latter of which also determines the most important criterion: the risk/benefit balance. In my version of the Lancet table, I have therefore added these three variables for non-pharmacological and non-surgical options:
| EFFECTIVENESS ACUTE LBP | EFFECTIVENESS PERSISTENT LBP | RISKS | COSTS | RISK/BENEFIT BALANCE | |
| Advice to stay active | +, routine | +, routine | None | Low | Positive |
| Education | +, routine | +, routine | None | Low | Positive |
| Superficial heat | +/- | Ie | Very minor | Low to medium | Positive (aLBP) |
| Exercise | Limited | +/-, routine | Very minor | Low | Positive (pLBP) |
| CBT | Limited | +/-, routine | None | Low to medium | Positive (pLBP) |
| Spinal manipulation | +/- | +/- | vfbmae sae |
High | Negative |
| Massage | +/- | +/- | Very minor | High | Positive |
| Acupuncture | +/- | +/- | sae | High | Questionable |
| Yoga | Ie | +/- | Minor | Medium | Questionable |
| Mindfulness | Ie | +/- | Minor | Medium | Questionable |
| Rehab | Ie | +/- | Minor | Medium to high | Questionable |
Routine = consider for routine use
+/- = second line or adjunctive treatment
Ie = insufficient evidence
Limited = limited use in selected patients
vfbmae = very frequent, minor adverse effects
sae = serious adverse effects, including deaths, are on record
aLBP = acute low back pain
The reason why my stance, as expressed on this blog and elsewhere, is often critical about certain alternative therapies is thus obvious and transparent. For none of them (except for massage) is the risk/benefit balance positive. And for spinal manipulation, it even turns out to be negative. It goes almost without saying that responsible advice must be to avoid treatments for which the benefits do not demonstrably outweigh the risks.
I imagine that chiropractors, osteopaths and acupuncturists will strongly disagree with my interpretation of the evidence (they might even feel that their cash-flow is endangered) – and I am looking forward to the discussions around their objections.
We all know that there is a plethora of interventions for and specialists in low back pain (chiropractors, osteopaths, massage therapists, physiotherapists etc., etc.); and, depending whether you are an optimist or a pessimist, each of these therapies is as good or as useless as the next. Today, a widely-publicised series of articles in the Lancet confirms that none of the current options is optimal:
Almost everyone will have low back pain at some point in their lives. It can affect anyone at any age, and it is increasing—disability due to back pain has risen by more than 50% since 1990. Low back pain is becoming more prevalent in low-income and middle-income countries (LMICs) much more rapidly than in high-income countries. The cause is not always clear, apart from in people with, for example, malignant disease, spinal malformations, or spinal injury. Treatment varies widely around the world, from bed rest, mainly in LMICs, to surgery and the use of dangerous drugs such as opioids, usually in high-income countries.
The Lancet publishes three papers on low back pain, by an international group of authors led by Prof Rachelle Buchbinder, Monash University, Melbourne, Australia, which address the issues around the disorder and call for worldwide recognition of the disability associated with the disorder and the removal of harmful practices. In the first paper, Jan Hartvigsen, Mark Hancock, and colleagues draw our attention to the complexity of the condition and the contributors to it, such as psychological, social, and biophysical factors, and especially to the problems faced by LMICs. In the second paper, Nadine Foster, Christopher Maher, and their colleagues outline recommendations for treatment and the scarcity of research into prevention of low back pain. The last paper is a call for action by Rachelle Buchbinder and her colleagues. They say that persistence of disability associated with low back pain needs to be recognised and that it cannot be separated from social and economic factors and personal and cultural beliefs about back pain.
Overview of interventions endorsed for non-specific low back pain in evidence-based clinical practice guidelines (Danish, US, and UK guidelines)
In this situation, it makes sense, I think, to opt for a treatment (amongst similarly effective/ineffective therapies) that is at least safe, cheap and readily available. This automatically rules out chiropractic, osteopathy and many others. Exercise, however, does come to mind – but what type of exercise?
The aim of this meta-analysis of randomized controlled trials was to gain insight into the effectiveness of walking intervention on pain, disability, and quality of life in patients with chronic low back pain (LBP) at post intervention and follow ups.
Six electronic databases (PubMed, Science Direct, Web of Science, Scopus, PEDro and The Cochrane library) were searched from 1980 to October 2017. Randomized controlled trials (RCTs) in patients with chronic LBP were included, if they compared the effects of walking intervention to non-pharmacological interventions. Pain, disability, and quality of life were the primary health outcomes.
Nine RCTs were suitable for meta-analysis. Data was analysed according to the duration of follow-up (short-term, < 3 months; intermediate-term, between 3 and 12 months; long-term, > 12 months). Low- to moderate-quality evidence suggests that walking intervention in patients with chronic LBP was as effective as other non-pharmacological interventions on pain and disability reduction in both short- and intermediate-term follow ups.
The authors concluded that, unless supplementary high-quality studies provide different evidence, walking, which is easy to perform and highly accessible, can be recommended in the management of chronic LBP to reduce pain and disability.
I know – this will hardly please the legions of therapists who earn their daily bread with pretending their therapy is the best for LBP. But healthcare is clearly not about the welfare of the therapists, it is/should be about patients. And patients should surely welcome this evidence. I know, walking is not always easy for people with severe LBP, but it seems effective and it is safe, free and available to everyone.
My advice to patients is therefore to walk (slowly and cautiously) to the office of their preferred therapist, have a little rest there (say hello to the staff perhaps) and then walk straight back home.
On this blog, we had many chiropractors commenting that their profession is changing fast and the old ‘philosophy’ is a thing of the past. But are these assertions really true? This survey might provide an answer. A questionnaire was sent to chiropractic students in all chiropractic programs in Australia and New Zealand. It explored student viewpoints about the identity, role/scope, setting, and future of chiropractic practice as it relates to chiropractic education and health promotion. Associations between the number of years in the program, highest degree preceding chiropractic education, institution, and opinion summary scores were evaluated by multivariate analysis of variance tests.
A total of 347 chiropractic students participated. For identity, most students (51.3%) hold strongly to the traditional chiropractic theory but also agree (94.5%) it is important that chiropractors are educated in evidence-based practice. The main predictor of student viewpoints was a student’s chiropractic institution. Chiropractic institution explained over 50% of the variance around student opinions about role/scope of practice and approximately 25% for identity and future practice.
The authors concluded that chiropractic students in Australia and New Zealand seem to hold both traditional and mainstream viewpoints toward chiropractic practice. However, students from different chiropractic institutions have divergent opinions about the identity, role, setting, and future of chiropractic practice, which is most strongly predicted by the institution. Chiropractic education may be a potential determinant of chiropractic professional identity, raising concerns about heterogeneity between chiropractic schools.
Traditional chiropractic theory is, of course, all the palmereque nonsense about ‘95% of all diseases are caused by subluxations of the spine’ etc. And evidence-based practice means knowing that subluxations are a figment of the chiropractic imagination.
Imagine a physician who believes in evidence and, at the same time, in the theory of the 4 humours determining our health.
Imagine a geologist thinking that the earth is flat and also spherical.
Imagine a biologist subscribing to both creationism and evolution.
Imagine a surgeon earning his livelihood with blood-letting and key-hole surgery.
Imagine a doctor believing in vital energy after having been taught physiology.
Imagine an airline pilot considering the use of flying carpets.
Imagine a chemist engaging in alchemy.
Imagine a Brexiteer who is convinced of doing the best for the UK.
Imagine a homeopath who thinks he practices evidence-based medicine.
Imagine a plumber with a divining rod.
Imagine an expert in infectious diseases believing is the miasma theory.
Imagine a psychic hoping to use her skills for winning a fortune on the stock market.
————————————————————————————————————————————-
Once you have imagined all of these situations, I fear, you might know (almost) all worth knowing about chiropractic.
Do chiropractors even know the difference between promotion and research?
Probably a rhetorical question.
Personally, I have seen them doing so much pseudo-research that I doubt they recognise the real thing, even if they fell over it.
Here is a recent example that stands for many, many more such ‘research’ projects (some of which have been discussed on this blog).
But first a few sentences on the background of this new ‘study’.
The UD chiropractic profession is currently on the ‘opioid over-use bandwagon’ hoping that this move might promote their trade. Most chiropractors have always been against using (any type of) pharmaceutical treatment and advise their patients accordingly. D D Palmer, the founder of chiropractic, was adamant that drugs are to be avoided; he stated for instance that Drugs are delusive; they do not adjust anything. And “as the Founder intended, chiropractic has existed as a drug-free healthcare profession for better than 120 years.” To this day, chiropractors are educated and trained to argue against non-drug treatments and regularly claim that chiropractic is a drug-free alternative to traditional medicine.
Considering this background, this new piece of (pseudo) research is baffling, in my view.
The objective of this investigation was to evaluate the association between utilization of chiropractic services and the use of prescription opioid medications. The authors used a retrospective cohort design to analyse health insurance claims data. The data source was the all payer claims database administered by the State of New Hampshire. The authors chose New Hampshire because health claims data were readily available for research, and in 2015, New Hampshire had the second-highest age-adjusted rate of drug overdose deaths in the United States.
The study population comprised New Hampshire residents aged 18-99 years, enrolled in a health plan, and with at least two clinical office visits within 90 days for a primary diagnosis of low-back pain. The authors excluded subjects with a diagnosis of cancer. They measured likelihood of opioid prescription fill among recipients of services delivered by chiropractors compared with a control group of patients not consulting a chiropractor. They also compared the cohorts with regard to rates of prescription fills for opioids and associated charges.
The adjusted likelihood of filling a prescription for an opioid analgesic was 55% lower among chiropractic compared to non-chiropractic patients. Average charges per person for opioid prescriptions were also significantly lower among the former group.
The authors concluded that among New Hampshire adults with office visits for noncancer low-back pain, the likelihood of filling a prescription for an opioid analgesic was significantly lower for recipients of services delivered by doctors of chiropractic compared with nonrecipients. The underlying cause of this correlation remains unknown, indicating the need for further investigation.
The underlying cause remains unknown???
Really?
Let me speculate, or even better, let me extrapolate by drawing an analogy:
Employees by a large Hamburger chain set out to study the association between utilization of Hamburger restaurant services and vegetarianism. The authors used a retrospective cohort design. The study population comprised New Hampshire residents aged 18-99 years, who had entered the premises of a Hamburger restaurant within 90 days for a primary purpose of eating. The authors excluded subjects with a diagnosis of cancer. They measured the likelihood of vegetarianism among recipients of services delivered by Hamburger restaurants compared with a control group of individuals not using meat-dispensing facilities. They also compared the cohorts with regard to the money spent in Hamburger restaurants.
The adjusted likelihood of being a vegetarian was 55% lower among the experimental group compared to controls. The average money spent per person in Hamburger restaurants were also significantly lower among the Hamburger group.
The authors concluded that among New Hampshire adults visiting Hamburger restaurants, the likelihood of vegetarianism was significantly lower for consumers frequenting Hamburger restaurants compared with those who failed to frequent such places. The underlying cause of this correlation remains unknown, indicating the need for further investigation.
Daaaahhhhhhh!