chiropractic
In a paper discussed in a previous blog, Ioannidis et al published a comprehensive database of a large number of scientists across science. They used Scopus data to compile a database of the 100,000 most-cited authors across all scientific fields based on their ranking of a composite indicator that considers six citation metrics (total citations; Hirsch h-index; coauthorship-adjusted Schreiber hm-index; number of citations to papers as single author; number of citations to papers as single or first author; and number of citations to papers as single, first, or last author). The authors also added this caution:
Citation analyses for individuals are used for various single-person or comparative assessments in the complex reward and incentive system of science. Misuse of citation metrics in hiring, promotion or tenure decision, or other situations involving rewards (e.g., funding or awards) takes many forms, including but not limited to the use of metrics that are not very informative for scientists and their work (e.g., journal impact factors); focus on single citation metrics (e.g., h-index); and use of calculations that are not standardized, use different frames, and do not account for field. The availability of the data sets that we provide should help mitigate many of these problems. The database can also be used to perform evaluations of groups of individuals, e.g., at the level of scientific fields, institutions, countries, or memberships in diversely defined groups that may be of interest to users.
It seems thus obvious and relevant to employ the new metrics for defining the most ‘influential’ (most frequently cited) researchers in so-called alternative medicine (SCAM). Doing this creates not one but two non-overlapping tables (because ‘complementary&alternative medicine’ is listed both as a primary and a secondary field (not sure about the difference)). Below, I have copied a small part of these tables; the first three columns are self-explanatory; the 4th relates to the number of published articles, the 4th to the year of the author’s first publication, the 5th to the last, the 6th column is the rank amongst 100 000 scientists of all fields who have published more than a couple of papers.
TABLE 1
| Ernst, E. | University of Exeter | gbr | 2253 | 1975 | 2018 | 104 |
| Davidson, Jonathan R. T. | Duke University | usa | 426 | 1972 | 2017 | 1394 |
| Kaptchuk, Ted J. | Harvard University | usa | 245 | 1993 | 2018 | 6545 |
| Eisenberg, David M. | Harvard University | usa | 127 | 1991 | 2018 | 8641 |
| Lundeberg, Thomas | 340 | 1983 | 2016 | 17199 | ||
| Linde, Klaus | Technische Universitat Munchen | deu | 276 | 1993 | 2018 | 19488 |
| Schwartz, Gary E. | University of Arizona | usa | 264 | 1967 | 2018 | 21893 |
| Eloff, J.N. | University of Pretoria | zaf | 204 | 1997 | 2018 | 23830 |
| Birch, Stephen | McMaster University | can | 244 | 1985 | 2018 | 31925 |
| Wilson, Kenneth H. | Duke University | usa | 76 | 1976 | 2017 | 40760 |
| Kemper, Kathi J. | Ohio State University | usa | 181 | 1988 | 2017 | 45193 |
| Oken, Barry S. | Oregon Health and Science University | usa | 121 | 1974 | 2018 | 51325 |
| Pittler, M.H. | 155 | 1997 | 2016 | 53183 | ||
| Postuma, Ronald B. | McGill University | can | 159 | 1998 | 2018 | 61018 |
| Patwardhan, Bhushan | University of Pune | ind | 144 | 1989 | 2018 | 64465 |
| Krucoff, Mitchell W. | Duke University | usa | 261 | 1986 | 2016 | 66028 |
| Chiesa, Alberto | 87 | 1973 | 2017 | 82390 | ||
| Baliga, Manjeshwar Shrinath | 142 | 2002 | 2018 | 83030 | ||
| Mischoulon, David | Harvard University | usa | 194 | 1992 | 2018 | 91705 |
| Büssing, Arndt | University of Witten/Herdecke | deu | 207 | 1980 | 2018 | 95907 |
| Langevin, Helene M. | Harvard University | usa | 67 | 1999 | 2018 | 98290 |
| Creath, Katherine | 84 | 1984 | 2017 | 99709 | ||
| Kuete, Victor | University of Dschang | cmr | 239 | 2005 | 2018 | 128347 |
TABLE 2
| White, Adrian | University of Plymouth | gbr | 294 | 1990 | 2016 | 16714 |
| Astin, John A. | California Pacific Medical Center | usa | 50 | 1994 | 2014 | 21379 |
| Kelly, Gregory S. | 37 | 1985 | 2011 | 31037 | ||
| Walach, Harald | University of Medical Sciences Poznan | pol | 246 | 1996 | 2018 | 31716 |
| Berman, Brian M. | University of Maryland School of Medicine | usa | 211 | 1986 | 2018 | 34022 |
| Lewith, George | University of Southampton | gbr | 380 | 1980 | 2018 | 34830 |
| Kidd, Parris M. | University of California at Berkeley | usa | 38 | 1976 | 2011 | 36571 |
| Jonas, Wayne B. | 187 | 1992 | 2018 | 42445 | ||
| MacPherson, Hugh | University of York | gbr | 143 | 1996 | 2018 | 49923 |
| Bell, Iris R. | University of Arizona | usa | 142 | 1984 | 2015 | 51016 |
| Patrick, Lyn | 21 | 1999 | 2018 | 57086 | ||
| Ritenbaugh, Cheryl | University of Arizona | usa | 172 | 1981 | 2018 | 63248 |
| Boon, Heather | University of Toronto | can | 188 | 1988 | 2017 | 69066 |
| Aickin, Mikel | University of Arizona | usa | 149 | 1996 | 2014 | 72040 |
| Lee, Myeong Soo | 430 | 1996 | 2018 | 72358 | ||
| Lao, Lixing | University of Hong Kong | hkg | 247 | 1990 | 2018 | 74896 |
| Witt, Claudia M. | Charite – Universitatsmedizin Berlin | deu | 238 | 2001 | 2018 | 78849 |
| Sherman, Karen J. | 136 | 1984 | 2017 | 82542 | ||
| Verhoef, Marja J. | University of Calgary | can | 190 | 1989 | 2016 | 84314 |
| Smith, Caroline A. | University of Western Sydney | aus | 135 | 1979 | 2018 | 94130 |
| Miller, Alan L. | 30 | 1980 | 2016 | 94421 | ||
| Paterson, Charlotte | University of Bristol | gbr | 71 | 1995 | 2017 | 95130 |
| Milgrom, Lionel R. | London Metropolitan University | gbr | 107 | 1979 | 2017 | 112943 |
| Adams, Jon | University of Technology NSW | aus | 294 | 1999 | 2018 | 128486 |
| Litscher, Gerhard | Medical University of Graz | aut | 245 | 1986 | 2018 | 133122 |
| Chen, Calvin Yu-Chian | China Medical University Taichung | chn | 130 | 2007 | 2016 | 164522 |
No other researchers are listed in the ‘Complementary&Alternative Medicine’ categories and made it into the list of the 100 000 most-cited scientists.
To make this easier to read, I have ordered all SCAM researchers according to their rank in one single list and, where known to me, added the respective focus in SCAM research (ma = most areas of SCAM):
- ERNST EDZARD (ma)
- DONALDSON JONATHAN
- KAPTCHUK TED (acupuncture)
- EISENBERG DAVID (TCM)
- WHITE ADRIAN (acupuncture)
- LUNDEBERG THOMAS (acupuncture)
- LINDE KLAUS (homeopathy)
- ASTIN JOHN (mind/body)
- SCHWARTZ GARRY (healing)
- ELOFF JN
- KELLY GREGORY
- WALLACH HARALD (homeopathy)
- BIRCH STEVEN (acupuncture)
- BERMAN BRIAN (acupuncture)
- LEWITH GEORGE (acupuncture)
- KIDD PARRIS
- WILSON KENNETH
- JONAS WAYNE (homeopathy)
- KEMPER KATHIE (ma)
- MACPHERSON HUGH (acupuncture)
- BELL IRIS (homeopathy)
- OKEN BARRY (dietary supplements)
- PITTLER MAX (ma)
- PATRICK LYN
- RITENBAUGH CHERYL (ma)
- POSTUMA RONALD
- PATWARDHAN BHUSHAN
- KRUCOFF MICHELL
- BOON HEATHER
- AICKIN MIKEL (ma)
- LEE MYEONG SOO (TCM)
- LAO LIXING (acupuncture)
- WITT CLAUDIA (ma)
- CHIESA ALBERTO
- SHERMAN KAREN (acupuncture)
- BALIGA MANJESHWAR
- VERHOEF MARIA (ma)
- MISCHOULON DAVID
- SMITH CAROLINE (acupuncture)
- MILLER ALAN
- PATERSON CHARLOTTE (ma)
- BUESSING ARNDT (anthroposophical medicine)
- LANGEVIN HELENE (ma)
- CREATH KATHERINE
- MILGROM LIONEL (homeopathy)
- KUETE VICTOR
- ADAMS JON (ma)
- LITSCHER GERHARD
- CHEN CALVIN
The list is interesting in several regards. Principally, it offers individual SCAM researchers for the first time the opportunity to check their international standing relative to their colleagues. But, as the original analysis in Ioannidis’s paper contains much more data than depicted above, there is much further information to be gleaned from it.
For instance, I looked at the rate of self-citation (not least because I have sometimes been accused of overdoing this myself). It turns out that, with 7%, I am relative modest and well below average in that regard. Most of my colleagues are well above that figure. Researchers who have exceptionally high self-citation rates include Buessing (30%), Kuete (43%), Adams (36%), Litscher (45%), and Chen (53%).
The list also opens the possibility to see which countries dominate SCAM research. The dominance of the US seems fairly obvious and would have been expected due to the size of this country and the funds the US put into SCAM research. Considering the lack of funds in the UK, my country ranks surprisingly high, I find. No other country is well-represented in this list. In particular Germany does not appear often (even if we would classify Wallach as German); considering the large amounts of money Germany has invested in SCAM research, this is remarkable and perhaps even a bit shameful, in my view.
Looking at the areas of research, acupuncture and homeopathy seem to stand out. Remarkably, many of the major SCAMs are not or not well represented at all. This is in particular true for herbal medicine, chiropractic and osteopathy.
The list also confirms my former team as the leaders in SCAM research. (Yes, I know: in the country of the blind, the one-eyed man is king.) Pittler, White and Lee were, of course, all former co-workers of mine.
Perhaps the most intriguing finding, I think, relates to the many SCAM researchers who did not make it into the list. Here are a few notable absentees:
- Behnke J – GERMANY (homeopathy)
- Bensoussan A – AUSTRALIA (acupuncture)
- Brinkhaus B – GERMANY (acupuncture)
- Bronfort G – US (chiropractic)
- Chopra D – US (mind/body)
- Cummings M – UK (acupuncture)
- Dixon M – UK (ma)
- Dobos G – GERMANY (ma)
- Fisher P – UK (homeopathy)
- Fonnebo V – NORWAY (ma)
- Frass M – AUSTRIA (homeopathy)
- Goertz C – US (chiropractic)
- Hawk C -US (chiropractic)
- Horneber M – GERMANY (ma)
- Jacobs J – US (homeopathy)
- Jobst K – UK (homeopathy)
- Kraft K – GERMANY (naturopathy)
- Lawrence D – US (chiropractic)
- Long CR – US (chiropractic)
- Meeker WC – US (chiropractic)
- Mathie R – UK (homeopathy)
- Melchart – GERMANY (ma)
- Michalsen A – GERMANY (ma)
- Mills S – UK (herbal medicine)
- Peters D – UK (ma)
- Reilly D -US (homeopathy)
- Reily D – UK (homeopathy)
- Robinson N – UK (ma)
- Streitberger K – GERMANY (acupuncture)
- Tuchin PJ – US (chiropractic)
- Uehleke – GERMANY (naturopathy)
- Ullman D – US (homeopathy)
- Weil A – US (ma)
I leave it to you to interpret this list and invite you to add more SCAM researchers to it.
(thanks to Paul Posadski for helping with the tables)
A chiro, a arms dealer and a Brexit donor meet in a bar.
The arms dealer: my job is so secret, I cannot tell my neighbour what I do.
The Brexit donor: I have to keep things so close to my chest that not even my wife knows what I am doing.
The chiro: that’s nothing; my work is so secret that not even I know what I am doing.
CHILDISH, I KNOW!
But I am yet again intrigued by a survey aimed at finding out what chiropractors are up to. One might have thought that, after 120 years, they know what they are doing.
This survey described the profiles of chiropractors’ practice and the reasons, nature of the care provided to their patients and extent of interprofessional collaborations in Ontario, Canada. The researchers randomly recruited chiropractors from a list of registered chiropractors (n=3978) in active practice in 2015. Of the 135 randomly selected chiropractors, 120 were eligible, 43 participated and 42 completed the study.
Each chiropractor recorded information for up to 100 consecutive patient encounters, documenting patient health profiles, reasons for encounter, diagnoses and care provided. Descriptive statistics summarised chiropractor, patient and encounter characteristics, with analyses accounting for clustering and design effects. Thus data on 3523 chiropractor-patient encounters became available. More than 65% of participating chiropractors were male, mean age 44 years and had practised on average 15 years. The typical patient was female (59% of encounters), between 45 and 64 years (43%) and retired (21%) or employed in business and administration (13%). Most (39.4%) referrals were from other patients, with 6.8% from physicians. Approximately 68% of patients paid out of pocket or claimed extended health insurance for care. Most common diagnoses were back (49%, 95% CI 44 to 56) and neck (15%, 95% CI 13 to 18) problems, with few encounters related to maintenance/preventive care (0.86%, 95% CI 0.2 to 3.9) and non-musculoskeletal problems (1.3%, 95% CI 0.7 to 2.3). The most common treatments included spinal manipulation (72%), soft tissue therapy (70%) and mobilisation (35%).
The authors concluded that this is the most comprehensive profile to date of chiropractic practice in Canada. People who present to Ontario chiropractors are mostly adults with a musculoskeletal condition. Our results can be used by stakeholders to make informed decisions about workforce development, education and healthcare policy related to chiropractic care.
I am so sorry to have mocked this paper. I shouldn’t have, because it actually does reveal a few interesting snippets:
- Only 7% of referrals come from real doctors.
- The vast majority of all patients receive spinal manipulations.
- About 6% of them are under 14 years of age.
- Chiropractors seem to dislike surveys; only 35% of those asked complied.
- 23% of all consultations were for general or unspecified problems,
- 8% for neurologically related problems,
- 5% for non-musculoskeletal problems (eg, digestive, ear, eye, respiratory, skin, urology, circulatory, endocrine and metabolic, psychological).
- Chiropractors rarely refer patients to other clinicians; this only happened in less than 3% of encounters.
- Apart from manipulation, chiropractors employ all sorts of other dubious therapies (ultrasound 3%, acupuncture 3%, , traction 1%, interferential therapy 3%, soft laser therapy 3%).
- 68% of patients pay out of their own pocket…
… NO WONDER, THEY DO NOT SEEM TO BE IN NEED OF ANY TYPE OF TREATMENT: 54% of all patients reported being in “excellent/very good overall health”!
I have written about this more often than I care to remember, and today I do it again.
Why?
Because it is important!
Chiropractic is not effective for kids, and chiropractic is not harmless for kids – what more do we need to conclude that chiropractors should not be allowed anywhere near them?
And most experts now agree with this conclusion; except, of course, the chiropractors themselves. This recent article in THE CHRONICLE OF CHIROPRACTIC is most illuminating in this context:
It was only a matter of time before the attack on the chiropractic care of children spread to the United States from Australia and Canada and its also no surprise that insurance companies would jump on the bandwagon first. According to Blue Cross and Blue Shield Children under the age of 5 years should not receive chiropractic care (spinal manipulation) ” . . . because the skeletal system is not mature at this time.”
The Blues further contend that:
“Serious adverse events may be associated with pediatric spinal manipulation in children under the age of 5 years due to the risks of these procedures in children this age.”
The Blues claims that their determination is based on standards of care – though they do not state which ones.
“This determination was based on standards of care in pediatric medicine as well as current medical evidence.”
This is not the first time Blue Cross attacked the chiropractic care of children. In 2005 CareFirst Blue Cross claimed that:
“Spinal manipulation services to treat children 12 years of age and younger, for any condition, is considered experimental and investigational.”
The ridiculous and false claims by Blue Cross come on the heels of a ban placed on spinal manipulation of infants by the Chiropractic Board of Australia (see related story) and attacks on chiropractors who care for children in Canada by chiropractic regulatory boards there.
There is in fact plenty of evidence to support the chiropractic care of infants and children and there are practice guidelines (the highest level on the research hierarchy pyramid) that support such care.
The real issue is not whether or not evidence exists to support the chiropractic care of children – the real issue is power and the lack of any necessity for evidence for those with the power.
__________________________________________________________________
END OF QUOTE
What can we learn from this outburst?
- Chiropractors often take much-needed critique as an ‘attack’. My explanation for this phenomenon is that they sense how wrong they truly are, get defensive, and fear for their cash-flow.
- When criticised, they do not bother to address the arguments. This, I believe, is again because they know they are in the wrong.
- Chiropractors are in denial as to what they can and cannot achieve with their manipulations. My explanation for this is that they might need to be in denial – because otherwise they would have to stop practising.
- They often insult criticism as ridiculous and false without providing any evidence. The likely explanation is that they have no reasonable evidence to offer.
- All they do instead is stating things like ‘there is plenty of evidence’. They don’t like to present the ‘evidence’ because they seem to know that it is worthless.
- Lastly, in true style, they resort to conspiracy theories.
To any critical thinker their behaviour thus makes one conclusion virtually inescapable: DON’T LET A CHIROPRACTOR NEAR YOUR KIDS!
The World Federation of Chiropractic, Strategic Plan 2019-2022 has just been published. It is an odd document that holds many surprises. Sadly, none of them are positive.
As the efficacy and safety of chiropractic spinal manipulations, the hallmark treatment that close to 100% of all chiropractic patients receive, are more than a little doubtful, one would expect that such a strategy would focus on the promotion of rigorous clinical research to create more certainty in these two important areas. If you are like me and were hoping for a firm commitment to such activities, you will be harshly disappointed.
Already in the introduction, the WFC sets an entirely different agenda:
We believe that everyone deserves access to chiropractic. We believe in chiropractors being accessible throughout the world. We believe that societies can thrive where chiropractors are available as a part of people’s health care teams.
If you are not put off by such self-serving, nauseous nonsense and read on, you find what the WFC call the ‘FOUR STRATEGIC PILLARS’
- SUPPORT
- EMPOWERMENT
- PROMOTION
- ADVANCEMENT
The text supporting the first three pillars consists of insufferable platitudes, and I will therefore not burden you with it. But the title of No4 did raise my hopes of finding something along the lines of an advancement of the evidence-base of chiropractic. Sadly, this turned out to be over-optimistic. Here is the 4th pillar in its full beauty:
Advancing the chiropractic profession together under the banner of evidence-based, people-centered, interprofessional and collaborative care.
Around the world health is delivered according to prevailing societal, cultural and political factors. These social determinants mean that chiropractors must adapt to the environment in which they practice.
As a global federation we must continuously strive to advance awareness of chiropractic under a banner of ethical, evidence-based, people-centered care.
Through consensus-building, shared understanding and respectful dialogue with partners in the health system, chiropractic should become a valued partner in contributing enhanced population health.
Throughout our 7 world regions, we must advance public utilization of chiropractors to optimize the health of nations.
Through the identification of common values and a commitment to patient-centered care, we can advance the identity of chiropractors as spinal health care experts in the health care system.
The WFC will:
– Advance awareness of chiropractic among the general public, within health systems and among health professionals.
– Advance access to chiropractors for all people and broaden the integration of chiropractic services
– Advance interprofessional collaboration and the integration of chiropractic into health systems
_______________________________________________________________________
END OF QUOTE
The essence of the WFC strategy for the next 3 years thus seems to be as follows:
- Avoid any discussion about the lack of evidence of chiropractic.
- Promote chiropractic to the unsuspecting public at all cost.
- Make sure chiropractors’ cash flow is healthy.
There are some commentators on this blog who regularly try to make us believe that chiropractic is about to reform, leave obsolete concepts behind, and become a respectable, ethical and evidence-based healthcare profession. After reading the appalling drivel the WFC call their ‘strategic plan’, I am not optimistic that they are correct.
Japanese neurosurgeons reported the case of A 55-year-old man who presented with progressive pain and expanding swelling in his right neck. He had no history of trauma or infectious disease. The patient had undergone chiropractic manipulations once in a month and the last manipulation was done one day before the admission to hospital.
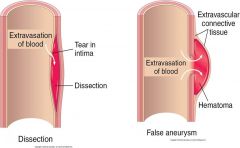
On examination by laryngeal endoscopy, a swelling was found on the posterior wall of the pharynx on the right side. The right piriform fossa was invisible. CT revealed hematoma in the posterior wall of the right oropharynx compressing the airway tract. Aneurysm-like enhanced lesion was also seen near the right common carotid artery. Ultrasound imaging revealed a fistula of approximately 1.2 mm at the posterior wall of the external carotid artery and inflow image of blood to the aneurysm of a diameter of approximately 12 mm. No dissection or stenosis of the artery was found. Jet inflow of blood into the aneurysm was confirmed by angiography. T1-weighted MR imaging revealed presence of hematoma on the posterior wall of the pharynx and the aneurysm was recognized by gadolinium-enhancement.
The neurosurgeons performed an emergency operation to remove the aneurysm while preserving the patency of the external carotid artery. The pin-hole fistula was sutured and the wall of the aneurysm was removed. Histopathological assessment of the tissue revealed a pseudoaneurysm (also called a false aneurism), a collection of blood that forms between the two outer layers of an artery.
The patient was discharged after 12 days without a neurological deficit. Progressively growing aneurysm of the external carotid artery is caused by various factors and early intervention is recommended. Although, currently, intravascular surgery is commonly indicated, direct surgery is also feasible and has advantages with regard to pathological diagnosis and complete repair of the parent artery.
The relationship between the pseudoaneurysm and the chiropractic manipulations seems unclear. The way I see it, there are the following three possibilities:
- The manipulations have causally contributed to the pseudo-aneurysm.
- They have exacerbated the condition and/or its symptoms.
- They are unrelated to the condition.
If someone is able to read the Japanese full text of this paper, please let us know what the neurosurgeons thought about this.
- the availability (numbers and where they are practising),
- quality (education and licensing),
- accessibility (entry and reimbursement),
- acceptability (scope of practice and legal rights).
An electronic survey was issued to contact persons of constituent member associations of the World Federation of Chiropractic (WFC). In addition, data were collected from government websites, personal communication and internet searches. Data were analysed using descriptive statistics.
Information was available from 90 countries in which at least one chiropractor was present. The total number of chiropractors worldwide was 103,469. The number of chiropractors per country ranged from 1 to 77,000. Chiropractic education was offered in 48 institutions in 19 countries. Direct access to chiropractic services was available in 81 (90%) countries, and services were partially or fully covered by government and/or private health schemes in 46 (51.1%) countries. The practice of chiropractic was legally recognized in 68 (75.6%) of the 90 countries. It was explicitly illegal in 12 (13.3%) countries. The scope of chiropractic practice was governed by legislation or regulation in 26 (28.9%) countries and the professional title protected by legislation in 39 (43.3%). In 43 (47.8%) countries, chiropractors were permitted to own, operate, or prescribe x-rays, in 22 (24.4%) countries they were lawfully permitted to prescribe advanced imaging (MRI or CT), and in 34 (38.8%) countries owning, operating or prescribing diagnostic ultrasound was permitted. Full or limited rights to the prescription of pharmaceutical medication were permitted in 9 (10%) countries, and authorization of sick leave was permitted in 20 (22.2%) countries. The care of children was subject to specific regulations and/or statutory restrictions in 57 (63.3%) countries.
The authors concluded as follows: We have provided information about the global chiropractic workforce. The profession is represented in 90 countries, but the distribution of chiropractors and chiropractic educational institutions, and governing legislations and regulations largely favour high-income countries. There is a large under-representation in low- and middle-income countries in terms of provision of services, education and legislative and regulatory frameworks, and the available data from these countries are limited.
The countries where chiropractic is explicitly illegal are the following:
- Egypt
- Argentina
- Columbia
- Austria,
- Estonia,
- Greece,
- Hungary,
- Lebanon,
- Republic of Korea,
- Taiwan,
- Turkey.
- Ukraine.
Forty-two countries (61.8%) have regulations and/or rules under the legislation to provide for registration or licensure of chiropractors. Chiropractors may be available in 90 countries, but 50% percent of these have 10 or fewer chiropractors. Importantly, the care of children is under regulation or restrictions in most countries.
- The World Federation of Chiropractic takes 3 years to publish data which, by then, are of course out-dated.
- In most countries, the chiropractic care for children is restricted.
- In many countries chiropractic is illegal.
- In many countries, there are only very few or no chiropractors at all.
- There are about 4 times more physiotherapists than chiropractors.
- In 9 countries, chiropractors have the right to prescribe medicines.
Much of the data revealed in this survey suggests to me that the world can do without chiropractors.
An article in the ‘Chronicle of Chiropractic’ defends the currently much debated chiropractic care for children. It is authored by ‘ChiroFuture‘, a Risk Purchasing Group founded by chiropractors. Here is the unabridged article (the references were added by me and refer to my comments below):
The chiropractic care of children has been the subject of increased media attention and scrutiny following decisions by chiropractic regulatory boards in Europe, Australia and Canada. These decisions were not based on science, research or data but rather a purposeful misrepresentation of the concept of evidence informed practice (1) and its application coupled with compelled speech.
As with the chiropractic care of adults, an evidence informed perspective (2) respects the needs and wants of parents for the care of their child, the published research evidence and the clinical expertise of chiropractors in the care of children.
ChiroFutures Malpractice Program does not base its malpractice insurance rates on the age of the patients a chiropractor sees. In fact, we are not aware of any actuarial data showing an increase in adverse events from the tens of millions of pediatric chiropractic visits per year (3). The vast majority of claims or incidents alleging chiropractic negligence involve adult patients (4).
What chiropractors do is minimally invasive and typically nothing else but their hands are used to gently ease any obstruction to the functioning of the patient’s nervous system (5). Since the nervous system controls and coordinates all functions of the body it is important to be sure it is functioning as best it can with no obstructions and no matter the disease afflicting the patient.
State and provincial laws, federal governments, international, national and state chiropractic organizations and chiropractic educational institutions all support the role and responsibility of chiropractors in the management of children’s health (6). The rationale for chiropractic care of children is supported by published protocols that are safe, efficacious, and valid (7). The scientific literature is sufficiently supportive of the usefulness of these protocols in regard to the chiropractic care of children (8).
Those contending that there is no evidence supporting the safety and efficacy of the chiropractic care of children demonstrate a complete disregard for the evidence and scientific facts related to the chiropractic care of children (9).
ChiroFutures encourages and supports a shared decision making process between doctors (10) and patients regarding health needs. As a part of that process, patients have a right to be informed about the state of their health as well as the risks, benefits and alternatives related to care. Any restriction on that dialogue or compelled statements inconsistent with the doctrine of informed consent present a threat to public health (11).
__________________________________________________________
Here are my comments:
- Why ‘evidence informed’ and not evidence-based’? The term ‘evidence informed’ is popular with SCAM practitioners. Barratt and Hodson noted, “The evidence-informed practitioner carefully considers what research evidence tells them in the context of a particular child, family or service, and then weighs this up alongside knowledge drawn from professional experience and the views of service users to inform decisions about the way forward.” This seems to imply that the two terms are synonymous. However, in reality they are not.
- Does that mean that ‘evidence-informed’ is defined as the practice wanted by patients, regardless of the evidence?
- There is no post-marketing surveillance in chiropractic. Therefore we do not have reliable data on adverse events.
- That might be true but it is unclear what it tells us. It might simply mean that chiropractors treat more adults than children.
- There is no good evidence to show that the function of the nervous system can be enhanced by manual therapy.
- Provincial laws and federal governments might tolerate but I don’t think they ‘support’ the role and responsibility of chiropractors. That chiropractic organisations support it surprises nobody.
- This sentence does not make sense to me. The facts, however, are clear: there is no sound rational for chiropractic manipulations and they are neither efficacious nor totally safe for children.
- The scientific evidence does not show that chiropractic care is effective for any paediatric condition.
- I think the complete disregard is shown not by critics but by the authors of these lines.
- Calling chiropractors ‘doctors’ gives the impression they have been to medical school and is therefore misleading the public.
- The threat to public health are those chiropractors who advise parents not to immunise their children.
Perhaps ChiroFuture need to brush up on their knowledge of the evidence. Chiropractic has no place in the healthcare of children. Parents should be warned!
As most of us know, the use of so-called alternative medicine (SCAM) can be problematic; its use in children is often most problematic:
- There are hardly any SCAMs that have been shown to work for paediatric conditions.
- Most SCAMs can cause considerable harm to children.
- Some might even amount to child abuse.
- Most SCAM practitioners lack adequate training to treat children.
- Many SCAM providers offer dangerous advice to parents.
- Parents are sometimes unable to differentiate between nonsense and medicine.
- Informed consent can present a trick subject when treating children.
In this context, the statement from the ‘Spanish Association Of Paediatrics Medicines Committee’ is of particular value and importance:
Currently, there are some therapies that are being practiced without adjusting to the available scientific evidence. The terminology is confusing, encompassing terms such as “alternative medicine”, “natural medicine”, “complementary medicine”, “pseudoscience” or “pseudo-therapies”. The Medicines Committee of the Spanish Association of Paediatrics considers that no health professional should recommend treatments not supported by scientific evidence. Also, diagnostic and therapeutic actions should be always based on protocols and clinical practice guidelines. Health authorities and judicial system should regulate and regularize the use of alternative medicines in children, warning parents and prescribers of possible sanctions in those cases in which the clinical evolution is not satisfactory, as well responsibilities are required for the practice of traditional medicine, for health professionals who act without complying with the “lex artis ad hoc”, and for the parents who do not fulfill their duties of custody and protection. In addition, it considers that, as already has happened, Professional Associations should also sanction, or at least reprobate or correct, those health professionals who, under a scientific recognition obtained by a university degree, promote the use of therapies far from the scientific method and current evidence, especially in those cases in which it is recommended to replace conventional treatment with pseudo-therapy, and in any case if said substitution leads to a clinical worsening that could have been avoided.
Of course, not all SCAM professions focus on children. The following, however, treat children regularly:
- acupuncturists
- anthroposophical doctors
- chiropractors
- craniosacral therapists
- energy healers
- herbalists
- homeopaths
- naturopaths
- osteopaths
I believe that all SCAM providers who treat children should consider the above statement very carefully. They must ask themselves whether there is good evidence that their treatments generate more good than harm for their patients. If the answer is not positive, they should stop. If they don’t, they should realise that they behave unethically and quite possibly even illegally.
The effectiveness of spinal manipulative therapy (SMT) for improving athletic performance in healthy athletes (or anything else for that matter) is unclear. The objective of this systematic review was to systematically review the literature on the effect of SMT on performance-related outcomes in asymptomatic adults.

The authors searched electronic databases from 1990 to March, 2018. Inclusion criteria was any study examining a performance-related outcome of SMT in asymptomatic adults. Methodological quality was assessed using the SIGN criteria. Studies with a low risk of bias were considered scientifically admissible for a best evidence synthesis.
Of 1415 articles screened, 20 studies had low risk of bias, seven were randomized crossover trials, 10 were randomized controlled trials (RCT) and three were RCT pilot trials. Four studies showed SMT had no effect on physiological parameters at rest or during exercise. There was no effect of SMT on scapular kinematics or transversus abdominus thickness. Three studies identified changes in muscle activation of the upper or lower limb, compared to two that did not. Five studies showed changes in range of motion (ROM). One study showed an increase lumbar proprioception and two identified changes in baropodometric variables after SMT. Sport-specific studies showed no effect of SMT except for a small increase in basketball free-throw accuracy.
The authors, who are all affiliated to the Canadian Memorial Chiropractic College, concluded that the preponderance of evidence suggests that SMT in comparison to sham or other interventions does not enhance performance-based outcomes in asymptomatic adult population. All studies are exploratory with immediate effects. In the few studies suggesting a positive immediate effect, the importance of such change is uncertain. Further high-quality performance specific studies are required to confirm these preliminary findings.
I think, this says it (almost) all: yet another lucrative claim made by many chiropractors and osteopaths turns out to be not backed up by good evidence. The only thing worth adding is the fact that only 4 of the studies mentioned adverse effects. This means the vast majority of studies failed to comply with this basic requirement of research ethics – and this really says it all!
Chiropractors often claim that they are working tirelessly towards increasing public health. But how seriously should we take such claims?
The purpose of this study was to investigate weight-loss interventions offered by Canadian chiropractors. It is a secondary analysis of data from the Ontario Chiropractic Observation and Analysis STudy (Nc = 42 chiropractors, Np = 2162 patient encounters). Its results show that around two-thirds (61.3%) of patients who sought chiropractic care were either overweight or had obesity. Very few patients had weight loss managed by their chiropractor. Among patients with body mass index equal to or greater than 18.5 kg/m2, guideline recommended weight management was initiated or continued by Ontario chiropractors in only 5.4% of encounters. Chiropractors did not offer weight management interventions at different rates among patients who were of normal weight, overweight, or obese (P value = 0.23). Chiropractors who graduated after 2005 who may have been exposed to reforms in chiropractic education to include public health were significantly more likely to offer weight management than chiropractors who graduated between 1995 and 2005.
The authors concluded that the prevalence of weight management interventions offered to patients by Canadian chiropractors in Ontario was low. Health care policy and continued chiropractic educational reforms may provide further direction to improve weight-loss interventions offered by doctors of chiropractic to their patients.
This paper seems to confirm my suspicion that the claim of chiropractors working for public heath is little more than an advertising gimmick. If we also consider the often negative attitude of chiropractors towards vaccination, the claim even deteriorates into a sick joke. Chiropractors, I have previously argued, are undermining public health and are being educated to become a danger to public health.