chiropractic
Two chiropractors conducted a retrospective review of publicly available data from the California Board of Chiropractic Examiners. Their aim was to determine categories of offense, experience, and gender of disciplined doctors of chiropractic (DC) in California and compare them with disciplined medical physicians in California.
Retrospective reviews of publicly available data from the California Board of Chiropractic Examiners.
The DC disciplinary categories, in descending order, were
- fraud (44%),
- sexual boundary issues (22%),
- other offences (13%),
- abuse of alcohol or drugs (10%),
- negligence or incompetence (6%),
- poor supervision (2%),
- mental impairment (.3%).
The authors concluded that the professions differ in the major reasons for disciplinary actions. Two thirds (67%) of the doctors of chiropractic were disciplined for fraud and sexual boundary issues, compared with 59% for negligence and substance misuse for medical physicians. Additional study in each profession may reveal methods to identify causes and possible intervention for those who are at high risk.
The two authors of this paper should be congratulated for their courage to publish such a review. These figures seem shocking. But I think that in reality some of them might be far higher. Take the important matter of competence, for instance. If you consider it competent that chiropractors treat conditions other than back pain, you might arrive at the above-mentioned figure of 6%. If you consider this as incompetent, as I do, the figure might be one order of magnitude higher (for more on unprofessional conduct by chiropractors see here).
The abstract of the paper does not provide comparisons to the data related to the medical profession. Here they are; relative to doctors, chiropractors are:
- 2x more likely to be involved in malpractice,
- 9x more likely to be practising fraud,
- 2x more likely to transgress sexual boundaries.
The frequency of fraud is particularly striking. Come to think of it, however, it is not all that amazing. I have said it before: chiropractic is in my view mostly about money.
It has been reported that B.C.’s chiropractors are deeply divided about the future of their profession, disagreeing on everything from false advertising to the use of routine X-rays.
Chiropractors attending an extraordinary general meeting of the College of Chiropractors of B.C. were split nearly down the middle on a series of non-binding resolutions addressing actions the College has taken in recent years. By the narrowest of margins, with at most 54% support, the members voted in favor of the college’s moves to limit the use of diagnostic X-rays and ban claims that aren’t supported by scientific evidence. The question that remains is who represents the bulk of the profession in B.C. — chiropractors advocating for what they describe as evidence-based practice targeting the musculoskeletal system, or “vitalists” who argue that chiropractic treatment can help with everything from immunity to brain function.
The modernizers see it as “a deliberate attempt to take over the college by a small group of chiropractors with no respect or knowledge of regulation … funded by organizations out of the province and out of the country,” Victoria chiropractor Clark Konczak told the virtual meeting.
At issue was a series of policies the college introduced in the wake of what Konczak called “the smoothie episode.” He was referring to a video posted on Facebook in 2017 by the then-vice chair of the college’s board, Avtar Jassal, in which he falsely suggested fruit smoothies are better than vaccines at preventing the flu.
Earlier this year, the college introduced amendments that bar chiropractors from performing routine and repeat X-rays, saying radiography is only scientifically supported when there are red flags that something is seriously wrong. The policy change on X-rays was the flashpoint in the long-simmering tension within the profession. A group of chiropractors has filed a petition in B.C. Supreme Court, alleging the college is preventing them from providing “safe, ethical, and effective care to their patients.” Their legal action has backing from national and international vitalistic organizations. During the recent meeting, a group of chiropractors argued unsuccessfully for the new X-ray policy to be tossed. Some suggested that chiropractors who don’t perform X-rays as a matter of routine are actually harming their patients. Another extraordinary general meeting has been called for July 20 to vote on resolutions calling for the removal of four college board members.
As I have often pointed out, chiropractic is all about money. The ‘chiro-wars’ have been going on for quite a while now, and they are by no means confined to B. C. or Canada. In a nutshell, they suggest to me that a significant proportion of chiropractors prefer money to progress.
Vertebral artery dissections (VAD) are a rare but important cause of ischemic stroke, especially in younger patients. Many etiologies have been identified, including motor vehicle accidents, cervical fractures, falls, physical exercise, and, as I have often discussed on this blog, cervical chiropractic manipulation. The goal of this study was to investigate the subgroup of patients who suffered a chiropractor-associated injury and determine how their prognosis compared to other-cause VAD.
The researchers, neurosurgeons from Chicago, conducted a retrospective chart review of 310 patients with vertebral artery dissections who presented at their institution between January 2004 and December 2018. Variables included demographic data, event characteristics, treatment, radiographic outcomes, and clinical outcomes measured using the modified Rankin Scale.
Overall, 34 out of our 310 patients suffered a chiropractor-associated injury. These patients tended to be younger (p = 0.01), female (p = 0.003), and have fewer comorbidities (p = 0.005) compared to patients with other-cause VADs. The characteristics of the injuries were similar, but chiropractor-associated injuries appeared to be milder at discharge and at follow-up. A higher proportion of the chiropractor-associated group had injuries in the 0-2 mRS range at discharge and at 3 months (p = 0.05, p = 0.04) and no patients suffered severe long-term neurologic consequences or death (0% vs. 9.8%, p = 0.05). However, when a multivariate binomial regression was performed, these effects dissipated and the only independent predictor of a worse injury at discharge was the presence of a cervical spine fracture (p < 0.001).
The authors concluded that chiropractor-associated injuries are similar to VADs of other causes, and apparent differences in the severity of the injury are likely due to demographic differences between the two populations.
The authors of the present paper are clear: “chiropractic manipulations are a risk factor for vertebral artery dissections.” This fact is further supported by a host of other investigations. For instance, the Canadian Stroke Consortium found that 28% of strokes following cervical artery dissection were preceded by chiropractic neck manipulation. Dziewas et al. obtained a similar rate in patients with vertebral artery dissections. Many chiropractors are in denial; however, this is merely due to their overt conflicts of interest.
My conclusions from the accumulated evidence are this:
Spinal manipulations of the upper spine should not be routinely used for any condition. Patients who nevertheless insist on having them must be made aware of the risks and give informed consent.
I have reported about the risks of chiropractic manipulation many times before. This is not because, as some seem to believe, I have an axe to grind but because the subject is important. This week, another case of stroke after chiropractic manipulation was in the news. Some will surely say that it is alarmist to mention such reports which lack lots of crucial details. Yet, as long as chiropractors do not establish a proper monitoring system where serious adverse effects of spinal manipulation are noted, I think it is important to record even incomplete cases in this fashion.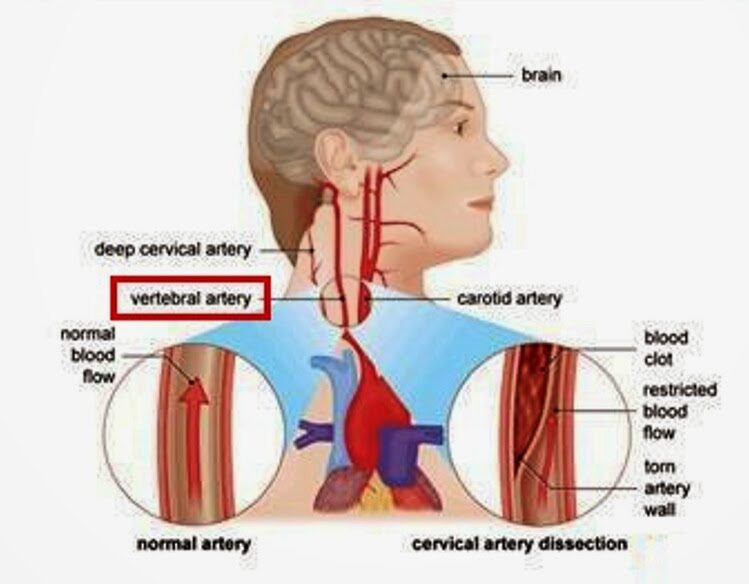
Barbara Shand is a working mom who lives in Alberta, Canada. She went to see a chiropractor because she had neck pain. “Near the very end of the appointment, the chiropractor asked: ‘Do you want your neck adjusted?’ I said: ‘Sure.’” “As soon as she did it, everything went black,” Shand recalls.
The patient was then rushed to a hospital by ambulance. “When I did open my eyes, I couldn’t focus. It was all blurry, I had massive vertigo, I didn’t know what was up or down,” Shand told the journalist. The diagnosis, Shand explains, was a right vertebral artery dissection, followed by a stroke. Mrs. Sands continues to struggle with coordination and balance.
The Alberta College and Association of Chiropractors acknowledges “there have been reported cases of stroke associated with visits to various healthcare practitioners, including those that provide cervical spine manipulation.” But they claim it is rare. They did not comment on the informed consent which, according to Shand’s description, was more than incomplete.
The fact that the ACAC admits that such events have happened before is laudable and a step in the right direction (some chiropractic organizations don’t even go that far). Yet, their caveat that such cases are rare is problematic. Without a monitoring system, nobody can tell how frequent they are! What we do see is merely the tip of a much bigger iceberg. There have been hundreds of cases like Mrs. Shand. The truth of the matter is this: Chiropractic neck manipulations are not supported by sound evidence of effectiveness for any condition. This means that even rare risks (if they are truly rare) would tilt the risk/benefit balance into the negative.
The conclusion is, I think, to avoid neck manipulations at all costs. Or, as one neurologist once put it:
don’t let the buggars touch your neck!
This systematic review assessed the effects and reliability of sham procedures in manual therapy (MT) trials in the treatment of back pain (BP) in order to provide methodological guidance for clinical trial development.
Different databases were screened up to 20 August 2020. Randomized controlled trials involving adults affected by BP (cervical and lumbar), acute or chronic, were included. Hand contact sham treatment (ST) was compared with different MT (physiotherapy, chiropractic, osteopathy, massage, kinesiology, and reflexology) and to no treatment. Primary outcomes were BP improvement, the success of blinding, and adverse effects (AE). Secondary outcomes were the number of drop-outs. Dichotomous outcomes were analyzed using risk ratio (RR), continuous using mean difference (MD), 95% CIs. The minimal clinically important difference was 30 mm changes in pain score.
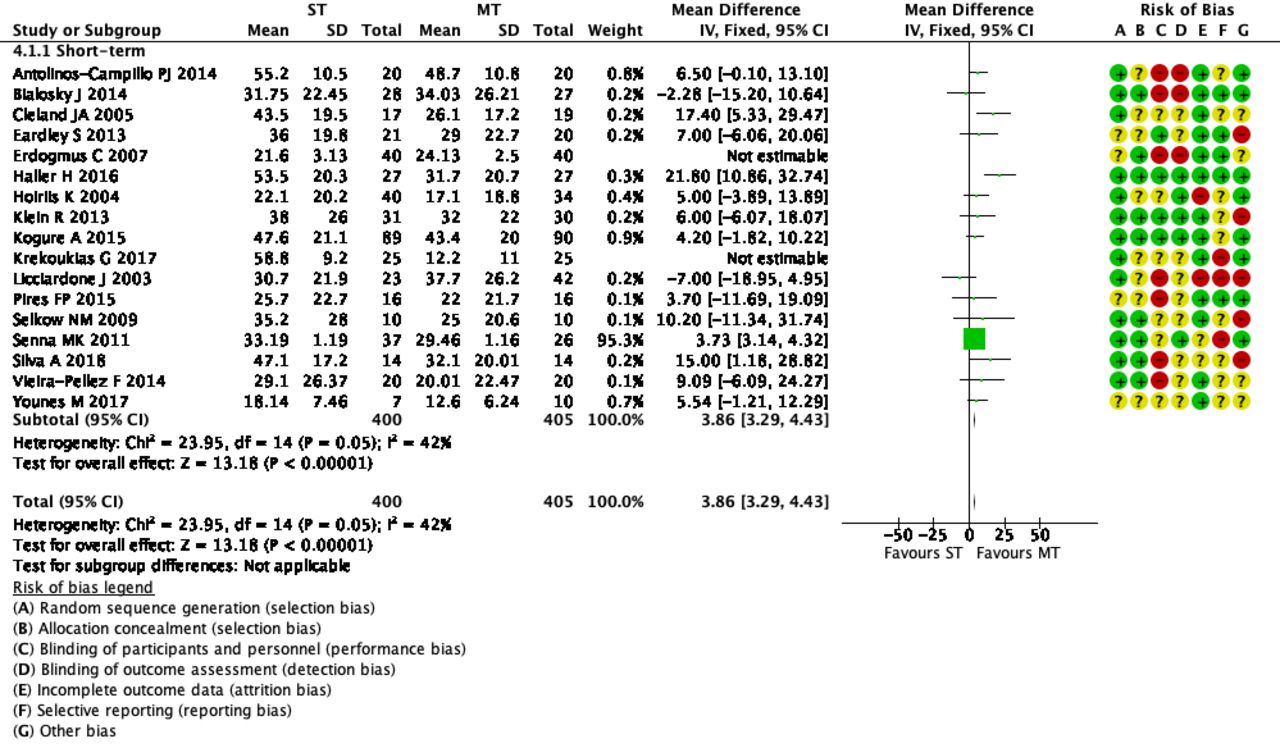
A total of 24 trials were included involving 2019 participants. Most of the trials were of chiropractic manipulation. Very low evidence quality suggests clinically insignificant pain improvement in favor of MT compared with ST (MD 3.86, 95% CI 3.29 to 4.43) and no differences between ST and no treatment (MD -5.84, 95% CI -20.46 to 8.78).ST reliability shows a high percentage of correct detection by participants (ranged from 46.7% to 83.5%), spinal manipulation is the most recognized technique. Low quality of evidence suggests that AE and drop-out rates were similar between ST and MT (RR AE=0.84, 95% CI 0.55 to 1.28, RR drop-outs=0.98, 95% CI 0.77 to 1.25). A similar drop-out rate was reported for no treatment (RR=0.82, 95% 0.43 to 1.55).
 The authors concluded that MT does not seem to have clinically relevant effect compared with ST. Similar effects were found with no treatment. The heterogeneousness of sham MT studies and the very low quality of evidence render uncertain these review findings. Future trials should develop reliable kinds of ST, similar to active treatment, to ensure participant blinding and to guarantee a proper sample size for the reliable detection of clinically meaningful treatment effects.
The authors concluded that MT does not seem to have clinically relevant effect compared with ST. Similar effects were found with no treatment. The heterogeneousness of sham MT studies and the very low quality of evidence render uncertain these review findings. Future trials should develop reliable kinds of ST, similar to active treatment, to ensure participant blinding and to guarantee a proper sample size for the reliable detection of clinically meaningful treatment effects.
The optimal therapy for back pain does not exist or has not yet been identified; there are dozens of different approaches but none has been found to be truly and dramatically effective. Manual therapies like chiropractic and osteopathy are often used, and some data suggest that they are as good (or as bad) as most other options. This review confirms what we have discussed many times previously (e.g. here), namely that the small positive effect of MT, or specifically spinal manipulation, is largely due to placebo.
Considering this information, what is the best treatment for back pain sufferers? The answer seems obvious: it is a therapy that is as (in)effective as all the others but causes the least harm or expense. In other words, it is not chiropractic nor osteopathy but exercise.
My conclusion:
avoid therapists who use spinal manipulation for back pain.
The purpose of this study was to describe changes in opioid-therapy prescription rates after a family medicine practice included on-site chiropractic services. It was designed as a retrospective analysis of opioid prescription data. The database included opioid prescriptions written for patients seeking care at the family medicine practice from April 2015 to September 2018. In June 2016, the practice reviewed and changed its opioid medication practices. In April 2017, the practice included on-site chiropractic services. Opiod-therapy use was defined as the average rate of opioid prescriptions overall medical providers at the practice.
There was a significant decrease of 22% in the average monthly rate of opioid prescriptions after the inclusion of chiropractic services (F1,40 = 10.69; P < .05). There was a significant decrease of 32% in the prescribing rate of schedule II opioids after the inclusion of chiropractic services (F2,80 = 6.07 for the Group × Schedule interaction; P < .05). The likelihood of writing schedule II opioid prescriptions decreased by 27% after the inclusion of chiropractic services (odds ratio, 0.73; 95% confidence interval, 0.59-0.90). Changes in opioid medication practices by the medical providers included prescribing a schedule III or IV opioid rather than a schedule II opioid (F6,76 = 29.81; P < .05) and a 30% decrease in the daily doses of opioid prescriptions (odds ratio, 0.70; 95% confidence interval, 0.50-0.98).
The authors concluded that this study demonstrates that there were decreases in opioid-therapy prescribing rates after a family medicine practice included on-site chiropractic services. This suggests that inclusion of chiropractic services may have had a positive effect on prescribing behaviors of medical physicians, as they may have been able to offer their patients additional nonpharmaceutical options for pain management.
The authors are correct in concluding the inclusion of chiropractic services MAY have had a positive effect. And then again, it may not!
Cause and effect cannot be established by correlation alone.
CORRELATION IS NOT CAUSATION!
And even if the inclusion of chiropractic services caused the positive effect, it would not prove that chiropractic is effective in the management of pain. It would only mean that the physicians had an option that helped them to write fewer opioid prescriptions. Had they hired a crystal healer or a homeopath or a faith healer or any other practitioner of an ineffective therapy, the findings might have been very similar.
The long and short of it is this: if we want to use fewer opioids, there is only one way to achieve it: we must prescribe less.
The objective of this systematic review was to examine whether back pain is associated with increased mortality risk and, if so, whether this association varies by age, sex, and back pain severity.
A systematic search of published literature was conducted and English-language prospective cohort studies evaluating the association of back pain with all-cause mortality with follow-up periods >5 years were included. Three reviewers independently screened studies, abstracted data, and appraised risk of bias using the Quality in Prognosis Studies (QUIPS) tool. A random-effects meta-analysis estimated combined odds ratios (OR) and 95% confidence intervals (CI), using the most adjusted model from each study. Potential effect modification by a priori hypothesized factors (age, sex, and back pain severity) was evaluated with meta-regression and stratified estimates.
Eleven studies with a total of 81,337 participants were included. Follow-up periods ranged from 5 to 23 years. The presence of any back pain, compared to none, was not associated with an increase in mortality (OR, 1.06; 95% CI, 0.97 to 1.16). However, back pain was associated with mortality in studies of women (OR, 1.22; 95% CI, 1.02 to 1.46) and among adults with more severe back pain (OR, 1.26; 95% CI, 1.14 to 1.40).
The authors concluded that back pain was associated with a modest increase in all-cause mortality among women and those with more severe back pain.
I bet that back pain is associated with hundreds of things. The question is whether there might be a causal association; could it be that people die earlier BECAUSE of back pain?
Unless someone’s back pain is so unbearable that she commits suicide, I cannot see how the two can be directly linked in a cause/effect relationship. But there could be indirect causal links. For instance, certain cancers can cause both back pain and death. Or someone’s back pain might make him take treatment against a life-threatening condition less seriously and thus hasten his death.
It has also occurred to me that chiropractors might jump on the bandwagon and use the association between back pain and mortality for boosting their business. Something like this:
Back pain is a risk factor for premature death.
Come to us, and we treat your back pain.
This will make you live longer.
Chiropractic prolongs life!
That would, of course, be daft. Firstly, chiropractic is not all that effective for back pain (or anything else). Secondly, getting rid of back pain is unlikely to prolong your life.
Correlation is not causation!
Many chiropractors seem to view the present pandemic as a business opportunity and make no end of false claims to attract customers. This has now been outlawed in the US. Medscape reported that a US district court will decide whether a chiropractor who is charged with 10 counts of making false marketing claims related to COVID-19 will be the first person convicted under a new federal law.
On his website, chiropractor ‘Dr.’ Eric Neptune advertises his services as follows:
Have you ever been told by your medical doctor that you or a member of your family had a specific disease, syndrome, or sickness? Did your doctor then recommend a drug or surgery to fix the issue, or tell you that you would have to live with it for the rest of your life? If so, you are not alone!
Nepute Wellness Center is unlike any medical clinic you may have been to. The clinic team is focused on finding and fixing the CAUSE of your problem vs. seeking out and treating only the SYMPTOMS. Nepute Wellness Center is equipped with state-of-the-art diagnostic equipment and testing, as well as medical doctors, nurses, and chiropractors who have been uniquely trained to treat your whole body, regardless of age, and return your body to a healthy balance so that it can heal itself the way God intended.
If you are tired of trying to treat your symptoms using prescription and over-the-counter pills, or even considering surgery, then Nepute Wellness Center may be right for you! Or like many, you want to be proactive with your health and prevent sickness and disease before you begin to suffer any symptoms, allowing you to live the full life you deserve, then make Nepute Wellness Center your partner in health!
Already over a year ago, Eric Nepute, the owner of Quickwork, based in St. Louis, Missouri, managed to make headlines. He had recorded a video that racked up more than 21 million views and suggested that drinking tonic water would prevent COVID-19 infections. Now, Mr. Neptune is the first person charged by the Federal Trade Commission (FTC) under the new COVID- 19 Consumer Protection Act. His company which has several locations in St. Louis County advertised its vitamin D and zinc products on social media and the internet as drugs that could treat or prevent COVID-19 claiming that their products are “more effective than the available COVID-19 vaccines”.
The FTC warned Nepute’s company in May 2020 about making unsubstantiated claims for other products regarding efficacy against COVID-19 and advised him to immediately stop making claims that were not supported by scientific evidence. However, Nepute seemed undeterred.
The FTC is seeking to fine Nepute and Quickwork up to US$43,792 for each violation of the COVID-19 Consumer Protection Act. In addition, the FTC seeks to bar the company from making health claims unless they are true and can be substantiated by scientific evidence.
Through his attorney, Neptune told the local NBC TV news affiliate, “I feel that I have not done anything wrong. I encourage everyone to live a healthy lifestyle during this unprecedented time. My attorneys are reviewing the complaint and I have no further comments at this time.”
In 2008, the British Chiropractic Association sued Simon Singh because he disclosed that they were promoting chiropractic for infant colic. The BCA lost the case, plenty of money, and all its reputation. Ever since the issue is a very sore point for chiropractic pride. The data show that Simon was quite correct in stating that they are happily promoting bogus treatments without a jot of evidence. Here for instance is my systematic review:
Some chiropractors claim that spinal manipulation is an effective treatment for infant colic. This systematic review was aimed at evaluating the evidence for this claim. Four databases were searched and three randomised clinical trials met all the inclusion criteria. The totality of this evidence fails to demonstrate the effectiveness of this treatment. It is concluded that the above claim is not based on convincing data from rigorous clinical trials.
But chiropractors steadfastly refuse to accept defeat and keep on trying to find positive results. Now Danish chiropractors have made another attempt.
The purpose of this study is to evaluate the effect of chiropractic care on infantile colic. This multicenter, single-blind randomized controlled trial was conducted in four Danish chiropractic clinics, 2015–2019. Information was distributed in the maternity wards and by maternal and child health nurses. Children aged 2–14 weeks with unexplained excessive crying were recruited through home visits and randomized (1:1) to either chiropractic care or control group. Both groups attended the chiropractic clinic twice a week for 2 weeks. The intervention group received chiropractic care, while the control group was not treated. The parents were not present in the treatment room and unaware of their child’s allocation.
The primary outcome was change in daily hours of crying before and after treatment. Secondary outcomes were changes in hours of sleep, hours being awake and content, gastrointestinal symptoms, colic status and satisfaction. All outcomes were based on parental diaries and a final questionnaire.
Of 200 recruited children, 185 completed the trial (treatment group n = 96; control group n = 89). Duration of crying in the treatment group was reduced by 1.5 h compared with 1 h in the control group (mean difference − 0.6, 95% CI − 1.1 to − 0.1; P = 0.026), but when adjusted for baseline hours of crying, age, and chiropractic clinic, the difference was not significant (P = 0.066). The proportion obtaining a clinically important reduction of 1 h of crying was 63% in the treatment group and 47% in the control group (p = 0.037), and NNT was 6.5. We found no effect on any of the secondary outcomes.

The authors concluded that excessive crying was reduced by half an hour in favor of the group receiving chiropractic care compared with the control group, but not at a statistically significant level after adjustments. From a clinical perspective, the mean difference between the groups was small, but there were large individual differences, which emphasizes the need to investigate if subgroups of children, e.g. those with musculoskeletal problems, benefit more than others from chiropractic care.
This seems to be a rigorous trial. However, I don’t quite understand why the authors even mention that, before adjusting, the results seemed to favor chiropractic. This only makes a squarely negative study look positive! Why would anyone want to do that? Could this perhaps hint at a reason for this odd behavior? “The study was primarily funded by the Foundation for Chiropractic Research and Postgraduate Education.”
Absurd claims about spinal manipulative therapy (SMT) improving immune function have increased substantially during the COVID-19 pandemic. Is there any basis at all for such notions?
The objective of this systematic review was to identify, appraise, and synthesize the scientific literature on the efficacy and effectiveness of SMT in preventing the development of infectious disease or improving disease-specific outcomes in patients with infectious disease and to examine the association between SMT and selected immunological, endocrine, and other physiological biomarkers.
A literature search of MEDLINE, the Cumulative Index to Nursing and Allied Health Literature, the Index to Chiropractic Literature, the Cochrane Central Register of Controlled Trials, and Embase was conducted. Randomized clinical trials and cohort studies were included. Eligible studies were critically appraised, and evidence with high and acceptable quality was synthesized using the Synthesis Without Meta-Analysis guideline.
A total of 2593 records were retrieved; after exclusions, 50 full-text articles were screened, and 16 articles reporting the findings of 13 studies comprising 795 participants were critically appraised. No clinical studies were located that investigated the efficacy or effectiveness of SMT in preventing the development of infectious disease or improving disease-specific outcomes among patients with infectious disease. Eight articles reporting the results of 6 high- and acceptable-quality RCTs comprising 529 participants investigated the effect of SMT on biomarkers. Spinal manipulative therapy was not associated with changes in lymphocyte levels or physiological markers among patients with low back pain or participants who were asymptomatic compared with sham manipulation, a lecture series, and venipuncture control groups. Spinal manipulative therapy was associated with short-term changes in selected immunological biomarkers among asymptomatic participants compared with sham manipulation, a lecture series, and venipuncture control groups.
The authors concluded that no clinical evidence was found to support or refute claims that SMT was efficacious or effective in changing immune system outcomes. Although there were limited preliminary data from basic scientific studies suggesting that SMT may be associated with short-term changes in immunological and endocrine biomarkers, the clinical relevance of these findings is unknown. Given the lack of evidence that SMT is associated with the prevention of infectious diseases or improvements in immune function, further studies should be completed before claims of efficacy or effectiveness are made.
I fully agree with the data as summarised in this paper. Yet, I find the conclusions a bit odd. The authors of this paper are chiropractors who declare the following conflicts of interest: Dr Côté reported receiving grants from the College of Chiropractors of British Columbia during the conduct of the study and grants from the Canadian Chiropractic Research Foundation, travel expenses from the World Federation of Chiropractic, and personal fees from the Canadian Chiropractic Protective Association outside the submitted work. Dr Cancelliere reported receiving grants from the Canadian Chiropractic Research Foundation outside the submitted work. Dr Mior reported receiving grants from the College of Chiropractors of British Columbia during the conduct of the study and grants from the Canadian Chiropractic Association and the Ontario Chiropractic Association outside the submitted work. Dr Hogg-Johnson reported receiving grants from the College of Chiropractors of British Columbia during the conduct of the study and grants from the Canadian Chiropractic Research Foundation outside the submitted work. No other disclosures were reported. The research was supported by funding from the College of Chiropractors of British Columbia to Ontario Tech University, the Canada Research Chairs program (Dr Côté), and the Canadian Chiropractic Research Foundation (Dr Cancelliere).
Would authors independent of chiropractic influence have drawn the same conclusions? I doubt it! While I do appreciate that chiropractors published these negative findings prominently, I feel the conclusions could easily be put much clearer:
There is no clinical evidence to support claims that SMT is efficacious or effective in changing immune system outcomes. Further studies in this area are not warranted.