children
Today is ‘World Bedwetting Day’!
No, don’t laugh; the event is initiated and supported by the World Bedwetting Day Steering Committee, which consists of the International Children’s Continence Society (ICCS) and the European Society for Paediatric Urology (ESPU) along with professional groups across the globe (see website for details).
A good day to remember that the British Chiropractic Association once sued my friend Simon Singh because he had disclosed that they were happily claiming that chiropractic was an effective therapy for bedwetting (and a few other childhood problems). An equally good day to remind ourselves that most alternative therapies are highly effective for this condition. At least this is what practitioners will tell you. For instance:
- homeopaths say that they can effectively treat bedwetting (~35 000 websites)
- chiropractors claim they can help (~84 000 websites)
- naturopaths insist they can treat it (~ 12 000 websites)
- Reiki is promoted for bedwetting (~ 12 000 websites)
- herbal medicine is said to be good for it ( (~37 000 websites)
- etc., etc.
“Stop, stop! This blog is about evidence!!!” I hear you shout impatiently.
Alright, here is a full and unabbreviated list of all alternative therapies that have been scientifically proven to work for bedwetting:
–
–
–
–
–
–
–
–
–
–
–
—
–
–
–
–
–
–
–
–
–
–
–
–
–
–
–
HAPPY BEDWETTING DAY EVERYBODY!
The aim of this paper was to systematically review surveys of 12-month prevalence of homeopathy use by the general population worldwide. Studies were identified via database searches to October 2015. Study quality was assessed using a six-item tool. All estimates were in the context of a survey which also reported prevalence of any complementary and alternative medicine use. A total of 36 surveys were included. Of these, 67% met four of six quality criteria.
Twelve-month prevalence of treatment by a homeopath was reported in 24 surveys of adults (median 1.5%, range 0.2–8.2%). Estimates for children were similar to those for adults. Rates in the USA, UK, Australia and Canada all ranged from 0.2% to 2.9% and remained stable over the years surveyed (1986–2012). Twelve-month prevalence of all use of homeopathy (purchase of over-the-counter homeopathic medicines and treatment by a homeopath) was reported in 10 surveys of adults (median 3.9%, range 0.7–9.8%) while a further 11 surveys which did not define the type of homeopathy use reported similar data. Rates in the USA and Australia ranged from 1.7% to 4.4% and remained stable over the years surveyed. The highest use was reported by a survey in Switzerland where homeopathy is covered by mandatory health insurance.
The authors concluded that each year a small but significant percentage of these general populations use homeopathy. This includes visits to homeopaths as well as purchase of over-the-counter homeopathic medicines.
These data thus indicate that the percentage of the adult general population using homeopathy over the previous 12 months was in the range of 0.7–9.8%, with a median estimate of 3.9%, and the percentage accessing treatment by a homeopath over the previous 12 months was in the range of 0.2–8.2%, with a median estimate of 1.5%. The data also suggest that, over the last few decades, use of homeopathy has remained fairly stable. These facts are in sharp contrast to the claims by homeopaths that:
- Homeopathy is hugely popular.
- Homeopathy is being used by more and more people across the globe.
- Homeopathy is the medicine of the future.
The well-documented and undeniable unpopularity of homeopathy begs the question, I think, why so many people seem to get so excited about homeopathy. The level of usage is nothing to write home about! Therefore, why don’t we just put it down to an aberration like believing the earth is flat? Why don’t we just concede that some minor, harmless stupidity will always exist in some people’s minds?
Here are some reasons why:
- It is not about the amount of people using homeopathy, but about the principle that any of the increasingly scarce public funds for healthcare are wasted on something as irrational and useless as homeopathy.
- Homeopathy makes a mockery of EBM.
- Homeopathy and homeopaths are by no means harmless.
- Homeopaths tell too many lies to be allowed to get away with them.
- Homeopathy and its followers systematically undermine rational thought.
You may recall, we have dealt with the JCAM many times before; for instance here, here, here and here. Now they have come out with another remarkable paper. This study – no, the authors called it a ‘pilot study’ – was to compare the efficacy of Emotional Freedom Techniques (EFT) with that of Cognitive-Behavioral Therapy (CBT) in reducing adolescent anxiety. Sixty-three American high-ability students in grades 6–12, ages 10–18 years, who scored in the moderate to high ranges for anxiety on the Revised Children’s Manifest Anxiety Scale-2 (RCMAS-2) were randomly assigned to one of three groups:
- CBT (n = 21),
- EFT (n = 21),
- or waitlist control (n = 21).
EFT is an alternative therapy that incorporates acupoint stimulation. Students assigned to the CBT or EFT treatment groups received three individual sessions of the identified protocols from trained graduate counseling, psychology, or social work students enrolled at a large northeastern research university. The RCMAS-2 was used to assess preintervention and postintervention anxiety levels in participants.
EFT participants showed significant reduction in anxiety levels compared with the waitlist control group with a moderate to large effect size. CBT participants did not differ significantly from the EFT or control.
The authors concluded that EFT is an efficacious intervention to significantly reduce anxiety for high-ability adolescents.
They also state in their abstract that EFT is an evidence-based treatment for anxiety…
Are you happy with these conclusions?
Are you convinced that this trial lends itself to establish efficacy of anything?
Are you impressed with the trial design, the sample size, etc?
Are you sure that EFT is plausible, credible or evidence-based in any way?
No?
Me neither!
If you look up EFT, you will find that there is a surprising amount of papers on it. Most of them have one thing in common: they were published in highly dubious journals. The field does not inspire trust or competence. The authors of the study state that EFT is an easily implemented strategy that uses such techniques as awareness building, exposure, reframing of interpretation, and systematic desensitization, while teaching the participant to self-stimulate protocol-identified acupoints (i.e., acupuncture points) by tapping. The effectiveness of acupuncture for treating anxiety has been well documented. Rather than using acupuncture needles, EFT relies on the manual stimulation of the acupoints. A recent meta-analysis indicated that interventions using acupoint stimulation had a moderate effect size (Hedge’s g = −0.66 95% CI [−0.99, −0.33]) in reducing symptoms. In EFT, the client stimulates the protocol-identified acupoints by tapping on them. Preliminary studies have suggested that tapping and other alternative ways of stimulating acupuncture points to be as effective as acupuncture needling. The EFT protocol and identified acupoints that were used in this study are the ones recommended for research purposes by the Association for Comprehensive Energy Psychology…
Wikipedia tells us that “Emotional Freedom Techniques (EFT) is a form of counseling intervention that draws on various theories of alternative medicine including acupuncture, neuro-linguistic programming, energy medicine, and Thought Field Therapy (TFT). It is best known through Gary Craig’s EFT Handbook, published in the late 1990s, and related books and workshops by a variety of teachers. EFT and similar techniques are often discussed under the umbrella term “energy psychology”. Advocates claim that the technique may be used to treat a wide variety of physical and psychological disorders, and as a simple form of self-administered therapy.[1] The Skeptical Inquirer describes the foundations of EFT as “a hodgepodge of concepts derived from a variety of sources, [primarily] the ancient Chinese philosophy of chi, which is thought to be the ‘life force’ that flows throughout the body.” The existence of this life force is “not empirically supported”.[2] EFT has no benefit as a therapy beyond the placebo effect or any known-effective psychological techniques that may be provided in addition to the purported “energy” technique.[3] It is generally characterized as pseudoscience and it has not garnered significant support in clinical psychology.”
A recent systematic review of EFT concluded that “there were too few data available comparing EFT to standard-of-care treatments such as cognitive behavioral therapy, and further research is needed to establish the relative efficacy of EFT to established protocols.”
Notwithstanding these and many other verdicts on EFT, we now are asked to agree with the new study that EFT IS EFFICACIOUS.
Is this a joke?
They want us to believe this on the basis of a PILOT STUDY? Such studies are not even supposed to test efficacy! (Yet the authors of the trial state that this study was designed to meet the American Psychological Association (APA) Division 12 quality control criteria and the Consolidated Standards for Reporting Trials (CONSORT) criteria. I have to admit, they could have fooled me!)
No, it is not a joke, it is yet another nonsense from the ‘The Journal of Complementary and Alternative Medicine’ which, in my view, should henceforth be called THE JOURNAL OF ALTERNATIVE FACTS (JAF).
This new RCT was embargoed until today; so, I had to wait until I was able to publish my comments. Here are the essentials of the study:
The Swedish investigators compared the effect of two types of acupuncture versus no acupuncture in infants with colic in public child health centres (CHCs). The study was designed as a multicentre, randomised controlled, single-blind, three-armed trial (ACU-COL) comparing two styles of acupuncture with no acupuncture, as an adjunct to standard care. Among 426 infants whose parents sought help for colic and registered their child’s fussing/crying in a diary, 157 fulfilled the criteria for colic and 147 started the intervention.
Parallel to usual care, study participants visited the study CHC twice a week for 2 weeks. Thus, all infants received usual care plus 4 extra visits to a CHC, during which parents met a nurse for 20–30 min and were able to discuss their infant’s symptoms. Together these were considered to represent gold standard care. The nurse listened, and gave evidence-based advice and calming reassurance. Breastfeeding mothers were encouraged to continue breastfeeding. At each visit, the study nurse carried the infant to a separate treatment room where they were left alone with the acupuncturist for 5 min.
The acupuncturist treated the baby according to group allocation and recorded the treatment procedures and any adverse events. Disposable stainless steel 0.20×13 mm Vinco needles (Helio, Jiangsu Province, China) were used. Infants allocated to group A received standardised MA at LI4. One needle was inserted to a depth of approximately 3 mm unilaterally for 2–5 s and then withdrawn without stimulation. Infants allocated to group B received semi-standardised individualised acupuncture, mimicking clinical TCM practice. Following a manual, the acupuncturists were able to choose one point, or any combination of Sifeng, LI4 and ST36, depending on the infant’s symptoms, as reported in the diary. A maximum of five insertions were allowed per treatment. Needling at Sifeng consisted of 4 insertions, each to a depth of approximately 1 mm for 1 s. At LI4 and ST36, needles were inserted to a depth of approximately 3 mm, uni- or bilaterally. Needles could be retained for 30 seconds. De qi was not sought, therefore stimulation was similarly minimal in groups A and B. Infants in group C spent 5 min alone with the acupuncturist without receiving acupuncture.
The effect of the two types of acupuncture was similar and both were superior to gold standard care alone. Relative to baseline, there was a greater relative reduction in time spent crying and colicky crying by the second intervention week (p=0.050) and follow-up period (p=0.031), respectively, in infants receiving either type of acupuncture. More infants receiving acupuncture cried <3 hours/day, and thereby no longer fulfilled criteria for colic, in the first (p=0.040) and second (p=0.006) intervention weeks. No serious adverse events were reported.
The authors concluded that acupuncture appears to reduce crying in infants with colic safely.
Notice that the investigators are cautious and state in the abstract that “acupuncture appears to reduce crying…” Their conclusions from the actual article are, however, quite different; here they state the following:
Among those initially experiencing excessive infant crying, the majority of parents reported normal values once the infant’s crying had been evaluated in a diary and a diet free of cow’s milk had been introduced. Therefore, objective measurement of crying and exclusion of cow’s milk protein are recommended as first steps, to avoid unnecessary treatment. For those infants that continue to cry >3 hours/day, acupuncture may be an effective treatment option. The two styles of MA tested in ACU-COL had similar effects; both reduced crying in infants with colic and had no serious side effects. However, there is a need for further research to find the optimal needling locations, stimulation and treatment intervals.
Such phraseology is much more assertive and seems to assume acupuncture caused specific therapeutic effects. Yet, I think, this assumption is not warranted.
In fact, I believe, the study shows almost the opposite of what the authors conclude. Both minimal and TCM acupuncture seemed to reduce the symptoms of colic compared to no acupuncture at all. I think, this confirms previous research showing that acupuncture is a ‘theatrical placebo’. The study was designed without an adequate placebo group. It would have been easy to use some form of sham acupuncture in the control group. Why did the authors not do that? Heaven knows, but one might speculate that they were aiming for a positive result – and what better way to ensure it than with a ‘no treatment’ control group?
There are, of course, numerous other flaws. For instance, Prof David Colquhoun FRS, Professor of Pharmacology at University College London, criticised the study because of its lousy statistics:
START OF QUOTE
“It is truly astonishing that, in the 21st century, the BMJ still publishes a journal devoted to a form of pre-scientific medicine which after more than 3000 trials has still not been able to produce convincing evidence of efficacy1. Like most forms of alternative medicine, acupuncture has been advocated for a vast range of problems, and there is little evidence that it works for any of them. Colic has not been prominent in these claims. What parent would think that sticking needles into their baby would stop it crying? The idea sounds bizarre. It is. This paper certainly doesn’t show that it works.
“The statistical analysis in the paper is incompetent. This should have been detected by the referees, but wasn’t. For a start, the opening statement, ‘A two-sided P value ≤0.05 was considered statistically significant’ is simply unacceptable in the light of all recent work about reproducibility. Still worse, Table 1 uses the description ‘statistical tendency towards significance (p=0.051–0.1)’.
“Worst of all, Table 1 reports 24 different P values, of which three are (just) below 0.05. Yet no correction has been used for multiple comparisons. This is very bad practice. It’s highly unlikely that, if the proper correction had been done, any of the results would have given a type 1 error rate below 5%.
“Even were it not for this, most of the ‘significant’ P values are marginal (only slightly less than 0.05). It is now well known that the type 1 error rate gives an optimistic view. What matters is the false positive rate – the chance that a ‘significant’ result is a false positive. A p-value close to 0.05 implies that there is at least a 30% chance that they are false positives. If one thought, a priori, that the chance of colic being cured by sticking needles into a baby was less than 50%, the false positive rate could easily be greater than 80%2. It is now recognised that this misinterpretation of p-values is a major contributor to the crisis of reproducibility.
“Other problems concern the power calculation. A priori calculations of power are well-known to be overoptimistic, because small trials usually overestimate the effect size. In this case the initial estimated sample size was not attained, and a rather mysterious recalculation of power was used.
“Another small problem: the discussion points out that ‘the majority of infants in this cohort did not have colic’.
“The nature of the control group is not very clear. An appropriate control might have been to cuddle the baby – this was used in a study in which another implausible treatment, chiropractic, was shown not to work. This appears not to have been done.
“Lastly, p-values are reported in the text without mention of effect sizes. This is contrary to all statistical advice.
“In conclusion, the design of the trial is reasonable (apart from the control group) but the statistical analysis is appalling. It’s very likely that there aren’t any real effects of acupuncture at all. This paper serves more to muddy the waters than to add useful information. It’s a model for the sort of mistakes that have led to the crisis in reproducibility. The BMJ should not be publishing this sort of stuff, and the referees seem to have no understanding of statistics.”
END OF QUOTE
Despite these rather obvious – some would say fatal – flaws, the editor of ACUPUNCTURE IN MEDICINE (AIM) thought this trial to be so impressively rigorous that he issued a press-release about it. This, I think, is particularly telling, perhaps even humorous: it shows what kind of a journal AIM is, and also provides an insight into the state of acupuncture research in general.
The long and short of it is that conclusions about specific therapeutic effects of acupuncture are not permissible. We know that colicky babies respond even to minimal attention, and this trial confirms that even a little additional TLC in the form of acupuncture will generate an effect. The observed outcome is most likely unrelated to acupuncture.
The WDDTY is not my favourite journal – far from it. The reason for my dislike is simple: far too many of its articles are utterly misleading and a danger to public health. Take this recent one entitled ‘Paleo-type diet reversing Crohn’s and ulcerative colitis’, for instance:
START OF QUOTE
Crohn’s disease and ulcerative colitis are being reversed solely by diet—essentially a Paleo diet. The non-drug approach has been successful in 80 per cent of children who’ve been put on the special diet.
The diet—called the specific carbohydrate diet (SCD)—has been pioneered by Dr David Suskind, a gastroenterologist at Seattle Children’s Hospital. The diet excludes grains, dairy, processed foods and sugars, other than honey, and promotes natural, nutrient-rich foods, including vegetables, fruits, meats and nuts.
Children are going into complete remission after just 12 weeks on the diet, a new study has discovered. Ten children with inflammatory bowel disease (IBD)—an umbrella term for Crohn’s and ulcerative colitis—were put on the diet, and eight were completely symptom-free by the end of the study. Suskind started exploring a dietary approach to IBD because he became convinced that the standard medical treatment of steroids or other medication was inadequate. “For decades, medicine has said diet doesn’t matter, that it doesn’t impact disease. Now we know that diet does have an impact, a strong impact. It works, and now there’s evidence,” he said.
END OF QUOTE
“For decades, medicine has said diet doesn’t matter, that it doesn’t impact disease”.
Really?
In this case, I must have studied an entirely different subject all these years ago at university – I had been told it was medicine but perhaps…???…!!!
It took me some time to find the original paper – they cited a wrong reference (2017 instead of 2016). But eventually I located it. Here is its abstract:
GOAL:
To determine the effect of the specific carbohydrate diet (SCD) on active inflammatory bowel disease (IBD).
BACKGROUND:
IBD is a chronic idiopathic inflammatory intestinal disorder associated with fecal dysbiosis. Diet is a potential therapeutic option for IBD based on the hypothesis that changing the fecal dysbiosis could decrease intestinal inflammation.
STUDY:
Pediatric patients with mild to moderate IBD defined by pediatric Crohn’s disease activity index (PCDAI 10-45) or pediatric ulcerative colitis activity index (PUCAI 10-65) were enrolled into a prospective study of the SCD. Patients started SCD with follow-up evaluations at 2, 4, 8, and 12 weeks. PCDAI/PUCAI, laboratory studies were assessed.
RESULTS:
Twelve patients, ages 10 to 17 years, were enrolled. Mean PCDAI decreased from 28.1±8.8 to 4.6±10.3 at 12 weeks. Mean PUCAI decreased from 28.3±23.1 to 6.7±11.6 at 12 weeks. Dietary therapy was ineffective for 2 patients while 2 individuals were unable to maintain the diet. Mean C-reactive protein decreased from 24.1±22.3 to 7.1±0.4 mg/L at 12 weeks in Seattle Cohort (nL<8.0 mg/L) and decreased from 20.7±10.9 to 4.8±4.5 mg/L at 12 weeks in Atlanta Cohort (nL<4.9 mg/L). Stool microbiome analysis showed a distinctive dysbiosis for each individual in most prediet microbiomes with significant changes in microbial composition after dietary change.
CONCLUSIONS:
SCD therapy in IBD is associated with clinical and laboratory improvements as well as concomitant changes in the fecal microbiome. Further prospective studies are required to fully assess the safety and efficacy of dietary therapy in patients with IBD.
What does this mean?
The WDDTY report bears very little resemblance to the journal article (let alone with the title of their article or any other published research by David Suskind).
How come?
I cannot be sure, but I would not be surprised to hear that the latter was ‘egged up’ to make the former appear more interesting.
If that is so, WDDTY are (once again) guilty of misleading the public to the point of endangering lives of vulnerable patients.
SHAME ON EVERY OUTLET THAT SELLS WDDTY, I’d say.
Perhaps I have a weak spot for fish oil; more likely, however, I just like positive news – and, in alternative medicine, there is not much of it. That’s why I have written about the potential benefits of fish-oil again and again and again and again.
Reduced intake of fish oil, i.e. n−3 long-chain polyunsaturated fatty acids (LCPUFAs), may be a contributing factor to the increasing prevalence of asthma and other wheezing disorders. Yet the evidence is neither clear nor strong. This study was aimed at shedding more light on the issue; specifically, it tested the effect of supplementation with n−3 LCPUFAs in pregnant women on the risk of persistent wheeze and asthma in their offspring.
The investigators randomly assigned 736 pregnant women at 24 weeks of gestation to receive 2.4 g of n−3 LCPUFA (fish oil) or placebo (olive oil) per day. Their children were followed prospectively with extensive clinical phenotyping. Neither the investigators nor the participants were aware of group assignments during follow-up for the first 3 years of the children’s lives, after which there was a 2-year follow-up period during which only the investigators were unaware of group assignments. The primary end point was persistent wheeze or asthma, and the secondary end points included lower respiratory tract infections, asthma exacerbations, eczema, and allergic sensitization.
A total of 695 children were included in the trial, and 95.5% completed the 3-year, double-blind follow-up period. The risk of persistent wheeze or asthma in the treatment group was 16.9%, versus 23.7% in the control group (hazard ratio, 0.69; 95% confidence interval [CI], 0.49 to 0.97; P=0.035), corresponding to a relative reduction of 30.7%. Prespecified subgroup analyses suggested that the effect was strongest in the children of women whose blood levels of eicosapentaenoic acid and docosahexaenoic acid were in the lowest third of the trial population at randomization: 17.5% versus 34.1% (hazard ratio, 0.46; 95% CI, 0.25 to 0.83; P=0.011). Analyses of secondary end points showed that supplementation with n−3 LCPUFA was associated with a reduced risk of infections of the lower respiratory tract (31.7% vs. 39.1%; hazard ratio, 0.75; 95% CI, 0.58 to 0.98; P=0.033), but there were no statistically significant associations between supplementation and asthma exacerbations, eczema, or allergic sensitization.
The authors concluded that supplementation with n−3 LCPUFA in the third trimester of pregnancy reduced the absolute risk of persistent wheeze or asthma and infections of the lower respiratory tract in offspring by approximately 7 percentage points, or one third.
The authors must be congratulated. This trial is stunning in many ways: it was carefully designed and executed; its results are clear and important; its write-up is excellent. The research was supported by private and public research funds, all of which are listed at www.copsac.com. The Lundbeck Foundation, the Danish Ministry of Health, the Danish Council for Strategic Research, the Danish Council for Independent Research, and the Capital Region Research Foundation provided core support.
It is debatable whether the intake of fish oil falls under the umbrella of alternative medicine. In a way, it reminds me of the famous saying: what do we call alternative medicine that works? We call it medicine. It also holds an important reminder for all who make claims about the benefit of alternative therapies: extraordinary claims require extraordinary evidence.
Can these findings be translated into practical advice to consumers? The NEJM discussed this question in an accompanying article in which the case of a fictional pregnant woman (Ms. Franklin) was considered. Here is what they concluded: …there is benefit and little risk associated with n−3 LCPUFA supplementation. Even though we do not know Ms. Franklin’s EPA and DHA levels, there is likely to be a benefit for her child, at little risk, cost, or inconvenience. She should start taking n−3 LCPUFA supplements.
Despite my soft spot for fish oil, I might add that, while we give advice of this nature, we nevertheless need to insist on independent replications to have certainty.
We had HOMEOPATHS WITHOUT BORDERS and now, I suggest, we acknowledge a similar organisation which could aptly be called CHIROPRACTORS WITHOUT SCRUPLES. This remarkable text from NATURAL NEWS explains it all, I think:
START OF QUOTE
The following chiropractors are speaking up to inform the public about the dangers of vaccines.
Dr. David Jockers, D.C.
Vaccines are one of medicine’s prized attempts to improve human performance. They use artificial laboratory derived medical technology to produce an immune response within the body in hopes it will lead to a long-term positive antibody response.
The vaccine ideology is based on the belief that people are created with inferior immune systems that are unable to keep up with the demands of the environment and need modern technology in the form of man-made vaccine formulations in order to bolster immunity.
According to the Centers for Disease Control, “The following substances are found in flu vaccines: aluminum, antibiotics, formaldehyde, human aborted fetal apparatus (dead human tissue), monosodium glutamate (MSG), and thimerosal (mercury).” Many of these same ingredients are in childhood vaccines. They are all very toxic for human physiology and have a track record for insulting the body’s immune system.
I would prefer to trust the innate ability of the body to overcome infectious microorganisms and I will fully support my body through healthy diet and lifestyle along with natural supplements and proper spinal alignment. I absolutely reject the idea that injecting a group of toxic, immune insulting chemicals into my bloodstream will improve someone’s long-term immune response.
Nancy Tarlow, D.C.
When you inject chemicals into your body that are toxic, there will be an effect. It may not be obvious at first. A child might have a fever that the doctor says is “normal”, but it isn’t. A fever or screaming could be that the brain is swelling and causing damage. The real problem is that children cannot convey to us how they feel. It’s not like an adult who can tell us that they felt great prior to a vaccination but then started having health problems.
Dr. Haroot Tovanyan, D.C.
I am a doctor of Chiropractic and I primarily work with autistic children.
… Every single parent in my practice that has an autistic child has the same story. Child was born normal; child was developing normal. Child went in for their 12-month, 18-month, normal usually 24 or 36-month shots and regressed. This may be anecdotal, but when you hear it over and over and over again, there’s something to be said. These are children that have severe neurological issues. They’re not verbal; 8-10-year-old children that are still wearing diapers.
I have a quadriplegic niece in my family who received 4 shots, a total of 10 vaccines in 1 day. She was born normal. She developed normal until about a year and a half. At a year and a half she received 4 shots, 1, 2, 3, 4, and she … This was 1990 when they started doing multiple vaccines and they also quadrupled the number of shots that you’re normally receiving. She basically regressed. She’s a vegetable. I mean, she became a quadriplegic. Nowhere in nature would your child go to get exposed to let’s say 6 or 7 or 8 or 9, or in the case of my niece, 10 viruses and bacteria at the same time.
In nature that just doesn’t happen. They don’t co-exist like that. It’s not natural to put a combination of vaccines, combinations of viruses and bacteria that just don’t belong together or don’t co-exist in nature in a vial and inject it into a child and expect them to be healthy. The CDC schedule has never been tested for safety. There have never been double-blind studies. It’s never been tested for synergistic effect. They’ve refused to study un-vaccinated versus vaccinated.
END OF QUOTE
On this blog, we have discussed the issues related to chiropractic and immunisations repeatedly (for instance here, here, here and here).
In case you wonder about the origins of this odd and unethical behaviour, you best look into the history of chiropractic. D. D. Palmer, the magnetic healer who ‘invented’ chiropractic some 120 years ago, left no doubt about his profound disgust for immunisation: “It is the very height of absurdity to strive to ‘protect’ any person from smallpox and other malady by inoculating them with a filthy animal poison… No one will ever pollute the blood of any member of my family unless he cares to walk over my dead body… ” (D. D. Palmer, 1910)
D. D. Palmer’s son, B. J. Palmer provided a more detailed explanation for chiropractors’ rejection of immunisation: “Chiropractors have found in every disease that is supposed to be contagious, a cause in the spine. In the spinal column we will find a subluxation that corresponds to every type of disease… If we had one hundred cases of small-pox, I can prove to you, in one, you will find a subluxation and you will find the same condition in the other ninety-nine. I adjust one and return his function to normal… There is no contagious disease… There is no infection…The idea of poisoning healthy people with vaccine virus… is irrational. People make a great ado if exposed to a contagious disease, but they submit to being inoculated with rotten pus, which if it takes, is warranted to give them a disease” (B. J. Palmer, 1909)
We are often told that such opinions have all but died out in today’s chiropractic profession. But is this true? I see precious little evidence to assume this to be true.
Today the anti-vaxx notions of chiropractors are mostly expressed in a less abrupt, more politically correct language: The International Chiropractors Association recognizes that the use of vaccines is not without risk. The ICA supports each individual’s right to select his or her own health care and to be made aware of the possible adverse effects of vaccines upon a human body. In accordance with such principles and based upon the individual’s right to freedom of choice, the ICA is opposed to compulsory programs which infringe upon such rights. The International Chiropractors Association is supportive of a conscience clause or waiver in compulsory vaccination laws, providing an elective course of action for all regarding immunization, thereby allowing patients freedom of choice in matters affecting their bodies and health.
Yes, I do realise that some chiropractors now acknowledge that immunisations have been one of the most successful interventions in the history of medicine. Yet, far too many others still vehemently adhere to the gospel of the Palmers, and statements like the following abound:
Vaccines. What are we taught? That vaccines came on the scene just in time to save civilization from the ravages of infectious diseases. That vaccines are scientifically formulated to confer immunity to certain diseases; that they are safe and effective. That if we stop vaccinating, epidemics will return…And then one day you’ll be shocked to discover that … your “medical” point of view is unscientific, according to many of the world’s top researchers and scientists. That many state and national legislatures all over the world are now passing laws to exclude compulsory vaccines….
Our original blood was good enough. What a thing to say about one of the most sublime substances in the universe. Our original professional philosophy was also good enough. What a thing to say about the most evolved healing concept since we crawled out of the ocean. Perhaps we can arrive at a position of profound gratitude if we could finally appreciate the identity, the oneness, the nobility of an uncontaminated unrestricted nervous system and an inviolate bloodstream. In such a place, is not the chiropractic position on vaccines self-evident, crystal clear, and as plain as the sun in the sky?
So, the opinions by chiropractors cited above seem more the rule than the exception. NATURAL NEWS is not normally one of my favourite publications; on this occasion, however, I am thankful to the editor for alerting us to what I might call CHIROPRACTORS WITHOUT SCRUPLES.
Yes, to a large extend, quacks make a living by advertising lies. A paper just published confirms our worst fears.
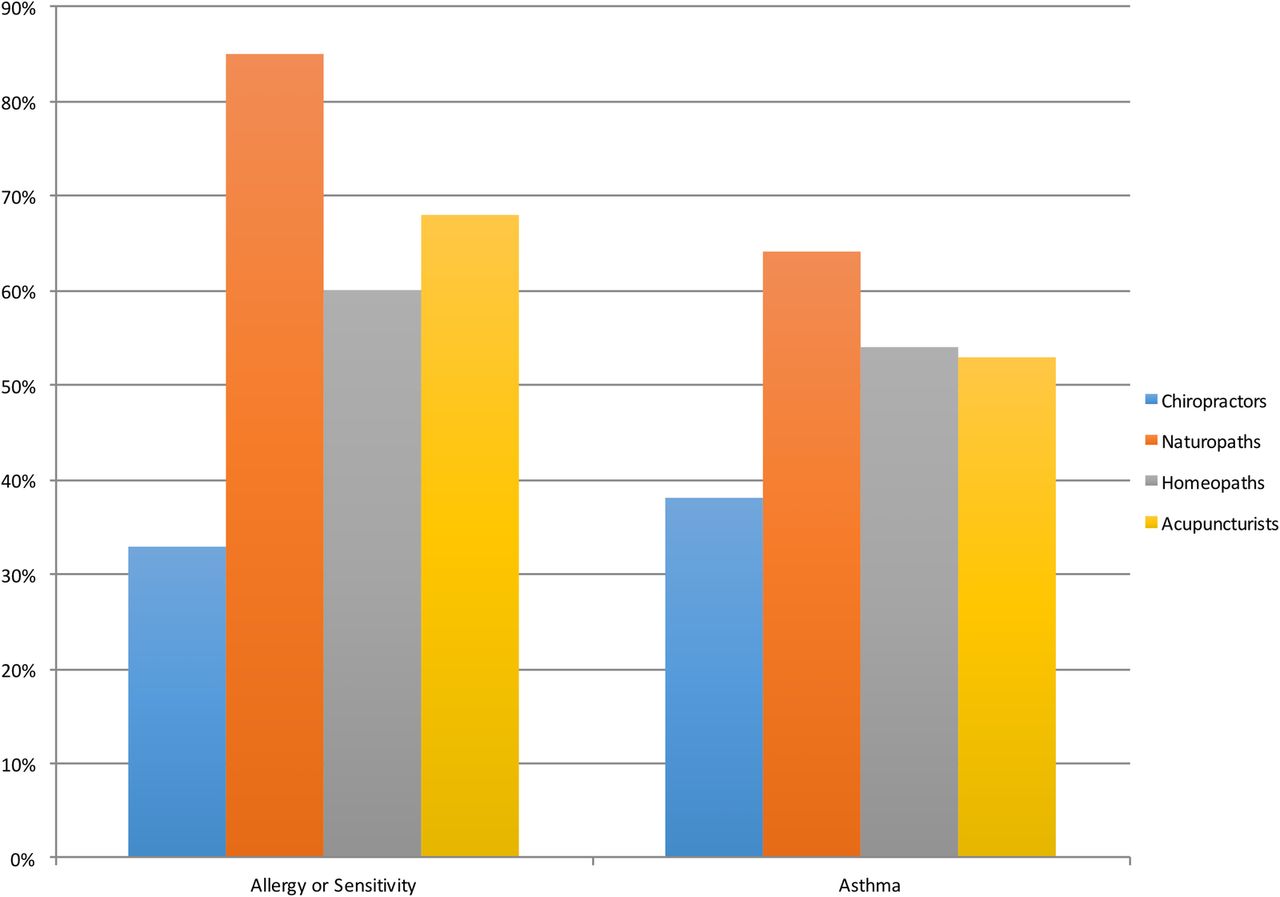
This survey was aimed at identifying the frequency and qualitative characteristics of marketing claims made by Canadian chiropractors, naturopaths, homeopaths and acupuncturists relating to the diagnosis and treatment of allergy and asthma.
A total of 392 chiropractic, naturopathic, homeopathic and acupuncture clinic websites were located in 10 of the largest metropolitan areas in Canada. The main outcome measures were: mention of allergy, sensitivity or asthma, claim of ability to diagnose allergy, sensitivity or asthma, claim of ability to treat allergy, sensitivity or asthma, and claim of allergy, sensitivity or asthma treatment efficacy. Tests and treatments promoted were noted as qualitative examples.
The results show that naturopath clinic websites had the highest rates of advertising at least one of diagnosis, treatment or efficacy for allergy or sensitivity (85%) and asthma (64%), followed by acupuncturists (68% and 53%, respectively), homeopaths (60% and 54%) and chiropractors (33% and 38%). Search results from Vancouver were most likely to advertise at least one of diagnosis, treatment or efficacy for allergy or sensitivity (72.5%) and asthma (62.5%), and results from London, Ontario were least likely (50% and 40%, respectively). Of the interventions advertised, few are scientifically supported; the majority lack evidence of efficacy, and some are potentially harmful.
The authors concluded that the majority of alternative healthcare clinics studied advertised interventions for allergy and asthma. Many offerings are unproven. A policy response may be warranted in order to safeguard the public interest.
In the discussion section, the authors state: “These claims raise ethical issues, because evidence in support of many of the tests and treatments identified on the websites studied is lacking. For example, food-specific IgG testing was commonly advertised, despite the fact that the Canadian Society of Allergy and Clinical Immunology has recommended not to use this test due to the absence of a body of research supporting it. Live blood analysis, vega/electrodiagnostic testing, intravenous vitamin C, probiotics, homeopathic allergy remedies and several other tests and treatments offered all lack substantial scientific evidence of efficacy. Some of the proposed treatments are so absurd that they lack even the most basic scientific plausibility, such as ionic foot bath detoxification…
Perhaps most concerning is the fact that several proposed treatments for allergy, sensitivity or asthma are potentially harmful. These include intravenous hydrogen peroxide, spinal manipulation and possibly others. Furthermore, a negative effect of the use of invalid and inaccurate allergy testing is the likelihood that such testing will lead to alterations and exclusions in diets, which can subsequently result in malnutrition and other physiological problems…”
This survey originates from Canada, and one might argue that elsewhere the situation is not quite as bad. However, I would doubt it; on the contrary, I would not be surprised to learn that, in some other countries, it is even worse.
Several national regulators have, at long last, become aware of the dangers of advertising of outright quackery. Consequently, some measures are now beginning to be taken against it. I would nevertheless argue that these actions are far too slow and by no means sufficiently effective.
We easily forget that asthma, for instance, is a potentially life-threatening disease. Advertising of bogus claims is therefore much more than a forgivable exaggeration aimed at maximising the income of alternative practitioners – it is a serious threat to public health.
We must insist that regulators protect us from such quackery and prevent the serious harm it can do.
The common cold is one of the indications for which homeopathy is deemed to be effective… by homeopaths that is! Non-homeopaths are understandably critical about this claim, not least because there is no good evidence for it. But, hold on, there is a new study which might change all this.
This study was recently published in COMPLEMENTARY THERAPIES IN MEDICINE which is supposed to be one of the better journals in this area. According to its authors, it was conducted “to determine if a homeopathic syrup was effective in treating cold symptoms in preschool children.” Children diagnosed with an upper respiratory tract infection were randomized to receive a commercial homeopathic cold syrup containing allium cepa 6X, hepar sulf calc 12X, natrum muriaticum 6X, phosphorous 12X, pulsatilla 6X, sulphur 12X, and hydrastasis 6X or placebo. Parents administered the study medication as needed for 3 days. The primary outcome was change in symptoms one hour after each dose. Parents also assessed the severity of each of the symptoms of runny nose, cough, congestion and sneezing at baseline and twice daily for 3 days, using a 4-point rating scale. A composite cold score was calculated by combining the values for each of the four symptoms. Among 261 eligible participants, data on 957 doses of study medication in 154 children were analyzed. There was no significant difference in improvement one hour after the dose for any symptom between the two groups. Analysis of twice daily data on the severity of cold symptoms compared to baseline values found that improvements in sneezing, cough and the composite cold score were significantly greater at both the first and second assessments among those receiving the cold syrup compared to placebo recipients.
The authors concluded that the homeopathic syrup appeared to be effective in reducing the severity of cold symptoms in the first day after beginning treatment.
Where to start? There are so many problems with this study that I find it difficult to chose the most crucial ones:
- The study had a clearly defined primary endpoint; it was not affected by the homeopathic treatment which doubtlessly makes the study a negative trial. The only correct conclusion therefore is that THE HOMEOPATHIC SYRUP FAILED TO AFFECT THE PRIMARY OUTCOME MEASURE OF THIS STUDY. THEREFORE THE TRIAL DID NOT PRODUCE ANY EVIDENCE TO ASSUME THAT THE EXPERIMENTAL TREATMENT WAS EFFICACIOUS.
- I don’t think that many of the primary or secondary outcome measures are validated or reliable.
- All the positive results reported in the abstract and the article relate to secondary endpoints which are purely explanatory by nature. They should, in my view, not be mentioned in the conclusions at all.
- The fact that some results turned out to be positive can be explained by the fact that the investigators ran dozens of tests for statistical significance which means that, by simple chance, some will turn out to produce a positive result.
- A further explanation for the seemingly positive results might be the fact disclosed in the text of the article that the children in the homeopathy group received more conventional drugs than those in the placebo group.
- Whatever the reason for these positive results, they certainly had nothing to do with the homeopathic syrup.
- The study was funded by the company producing the syrup and for which one of the authors was employed as a consultant. This might be an explanation for the abominably poor science. In other words, this paper is not an exercise in testing a hypothesis but one in marketing.
While I might forgive the company for trying to maximise their sales figures, I do find it harder to forgive the authors, reviewers and editors for publishing such overtly false conclusions. In my view, they are all guilty of scientific misconduct.
WHAT DOCTORS DON’T TELL YOU (WDDTY) is probably the most vile publication I know. It systematically misleads its readers by alarming news about this or that conventional treatment, while relentlessly promoting pseudoscientific non-sense. This article , entitled “MMR can cause skin problems and ulcers if your immune system is compromised” is a good example (one of a multitude):
The MMR vaccine can cause serious adverse reactions, researchers have admitted this week. The rubella (German measles) component of the jab increases the risk of infection from the rubella virus itself, and can cause serious skin inflammation and ulcers in anyone whose immune system is compromised.
The risk is highest among people with primary immunodeficiency diseases (PIDD), chronic genetic disorders that cause the immune system to malfunction.
Although the risk for people with compromised immune systems has been known, and is even included in the package inserts supplied with the vaccine, it was theoretical, say researchers from the Children’s Hospital of Philadelphia, who say they have uncovered “genuine evidence of harm.”
The researchers analysed the health profile of 14 people—four adults and 10 children—who suffered some form of a PIDD. Seven of them still had the rubella virus in their tissues, suggesting that their immune systems were too weak to get rid of the virus in the vaccine. The virus can damage skin cells and cause ulcers, and makes the person more susceptible to the actual rubella virus, the researchers say.
People with a poor immune system already have compromised T-cells—which are responsible for clearing viral infections—and the MMR makes the problem worse.
END OF QUOTE
And what is wrong with this article?
The answer is quite a lot:
- The research seems to be about a very specific and rare condition, yet WDDTY seem to want to draw much more general conclusions.
- The research itself is not described in a way that it would be possible to evaluate.
- The sample size of what seems to have been a case-control study was tiny.
- The study is not properly cited for the reader to verify and check; for all we know, it might not even exist.
- I was not able to find the publication on Medline, based on the information given.
Collectively, these points render the article not just useless, in my view, but make it a prime example of unethical, unhelpful and irresponsible scaremongering.