case report
I was alerted to the following short article from ‘The Blackpool Gazette‘:
Criminals have been using the brand name Pfizer to sell fake homeopathic vaccines to residents, according to police. The white tablets are sold under the pretence that they are an alternative to traditional vaccines, but actually contain no active ingredient. Analysis conducted by Lancashire Police revealed the tablets were nothing more than sugar pills. “Please note Pfizer do not produce any tablets as a cure or prophylactic for COVID-19,” a spokesman for the force added.
Homeopathy is a “treatment” based on the use of highly diluted substances, which practitioners claim can help the body heal itself, according to the NHS. A 2010 House of Commons Science and Technology Committee report on homeopathy said that homeopathic remedies perform no better than placebos. In 2017, NHS England said it would no longer fund homeopathy on the NHS as the lack of any evidence for its effectiveness did not justify the cost. This was backed by a High Court judgement in 2018.
I think there might be a slight misunderstanding here. The homeopathic remedy might not be fake, as it was produced according to the concepts of homeopathy. It is homeopathy itself that is fake. To me, it looks as though we are dealing with the German product I mentioned a while ago. Let me remind you:
Many people believe that homeopathy is essentially plant-based – but they are mistaken! Homeopathic remedies can be made from anything: Berlin wall, X-ray, pus, excrement, dental plaque, mobile phone rays, poisons … anything you can possibly think of. So, why not from vaccines?
This is exactly what a pharmacist specialized in homeopathy thought.
It has been reported that the ‘Schloss-Apotheke’ in Koblenz, Germany offered for sale a homeopathic remedy made from the Pfizer vaccine. This has since prompted not only the Chamber of Pharmacists but also the Paul Ehrlich Institute and Pfizer to issue statements. On Friday (30/4/2021) morning, the pharmacy had advertised homeopathic remedies based on the Pfizer/Biontech vaccine. The Westphalia-Lippe Chamber of Pharmacists then issued an explicit warning against it. “We are stunned by this,” said a spokesman. The offer has since disappeared from the pharmacy’s website.
Pfizer vaccine. This has since prompted not only the Chamber of Pharmacists but also the Paul Ehrlich Institute and Pfizer to issue statements. On Friday (30/4/2021) morning, the pharmacy had advertised homeopathic remedies based on the Pfizer/Biontech vaccine. The Westphalia-Lippe Chamber of Pharmacists then issued an explicit warning against it. “We are stunned by this,” said a spokesman. The offer has since disappeared from the pharmacy’s website.
On Friday afternoon, the manufacturer of the original vaccine also intervened. The Paul Ehrlich Institute released a statement making it clear that a vaccine is only safe “if it is administered in accordance with the marketing authorization.”
The Schloss-Apotheke had advertised the product in question with the following words:
“We have Pfizer/BioNTech Covid-19-Vaccine in potentized form up to D30 as globules or dilution (for discharge) in stock.”
The chamber of pharmacists countered with a warming under the heading “Facts instead of Fake News” on Facebook and Instagram:
“Whatever they might contain: These remedies are no effective protection against Covid-19.”
Pharmacy manager, Annette Eichele, of the Schloss-Apotheke claimed she had not sold homeopathic Corona vaccines and stressed that effective vaccines of this kind do not exist. According to Eichele, only an additional “mini drop” of the original Biontech vaccine had been used and “highly potentized” and prepared homeopathically. According to Eichele, Corona vaccinations that had already been administered were thus to have a “better and more correct effect with this supplementary product, possibly without causing side effects … but this is not scientifically proven”. The homeopathic product had been produced only on customer request and had been sold less than a dozen times in the past weeks. Ten grams of the remedy were sold for about 15 Euros. On Twitter, Eichele stated: „Wir haben nichts Böses getan, wir wollten nur Menschen helfen!“ (We have done nothing evil, we only wanted to help people). I am reminded yet again of Bert Brecht who observed:
“The opposite of good is not evil but good intentions”.
_______________________
If I am right, the remedy is not truly fake but a genuine product of a fake concept, namely homeopathy. In that case, the term ‘criminal’ might need to be applied to homeopathy itself – an interesting thought!
This story made the social media recently:
 Yes, I can well believe that many chiros are daft enough to interpret the incident in this way. Yet I think it’s a lovely story, not least because it reminds me of one of my own experiences:
Yes, I can well believe that many chiros are daft enough to interpret the incident in this way. Yet I think it’s a lovely story, not least because it reminds me of one of my own experiences:
I was on a plane to Toronto and had fallen asleep after a good meal and a few glasses of wine when a stewardess woke me saying: “We think you are a doctor!?”
“That’s right, I am a professor of alternative medicine”, I said trying to wake up.
“We have someone on board who seems to be dying. Would you come and have a look? We moved him into 1st class.”
Arrived in 1st class, she showed me the patient and a stethoscope. The patient was unconscious and slightly blue in the face. I opened his shirt and used the stethoscope only to find that this device is utterly useless on a plane; the sound of the engine by far overwhelms anything else. With my free hand, I tried to find a pulse – without success! Meanwhile, I had seen a fresh scar on the patient’s chest with something round implanted underneath. I concluded that the patient had recently had a pacemaker implant. Evidently, the electronic device had malfunctioned.
At this stage, two stewardesses were pressing me: “The captain needs to know now whether to prepare for an emergency stop in Newfoundland or to fly on. It is your decision.”
I had problems thinking clearly. What was best? The patient was clearly dying and there was nothing I could do about it. I replied by asking them to give me 5 minutes while I tried my best. But what could I do? I decided that I could do nothing but hold the patient’s hand and let him die in peace.
The Stewardesses watched me doing this and must have thought that I was trying some sort of energy healing, perhaps Reiki. This awkward situation continued for several minutes until – out of the blue – I felt a regular, strong pulse. Evidently, the pacemaker had started functioning again. It did not last long until the patient’s color turned pink and he began to talk. I instructed the pilot to continue our path to Toronto.
After I had remained with the patient for another 10 minutes or so, the Stewardesses came and announced: “We have moved your things into 1st class; like this, you can keep an eye on him.” The rest of the journey was uneventful – except the Stewardesses came repeatedly giving me bottles of champagne and fine wine to take with me into Toronto. And each time they politely asked whether my healing method would not also work for the various ailments they happened to suffer from – varicose veins, headache, PMS, fatigue …
So, here is my message to all the fellow energy healers out there:
We honor the creator’s design.
We know of the potential of the body is limitless.
Remember, you did not choose energy healing.
Energy healing chose you.
You were called for a time like this.
In case you are beginning to wonder whether I have gone round the bend, the answer is NO! I am not an energy healer. In fact, I am as much NOT an energy healer, as the chiropractor in the above story has NOT saved the life of his patient. Chiropractors and stewardesses, it seems to me, have one thing in common: they do not understand much about medicine.
PS
On arrival in Toronto, the patient was met by a team of fully equipped medics. I explained what had happened and they took him off to the hospital. As far as I know, he made a full recovery after the faulty pacemaker had been replaced. After my return to the UK, British Airways sent me a huge hamper to thank me.
Spinal cord injury after manual manipulation of the cervical spine is rare and has never been described as resulting from a patient performing a self-manual manipulation on his own cervical spine. This seems to be the first well-documented case of this association. 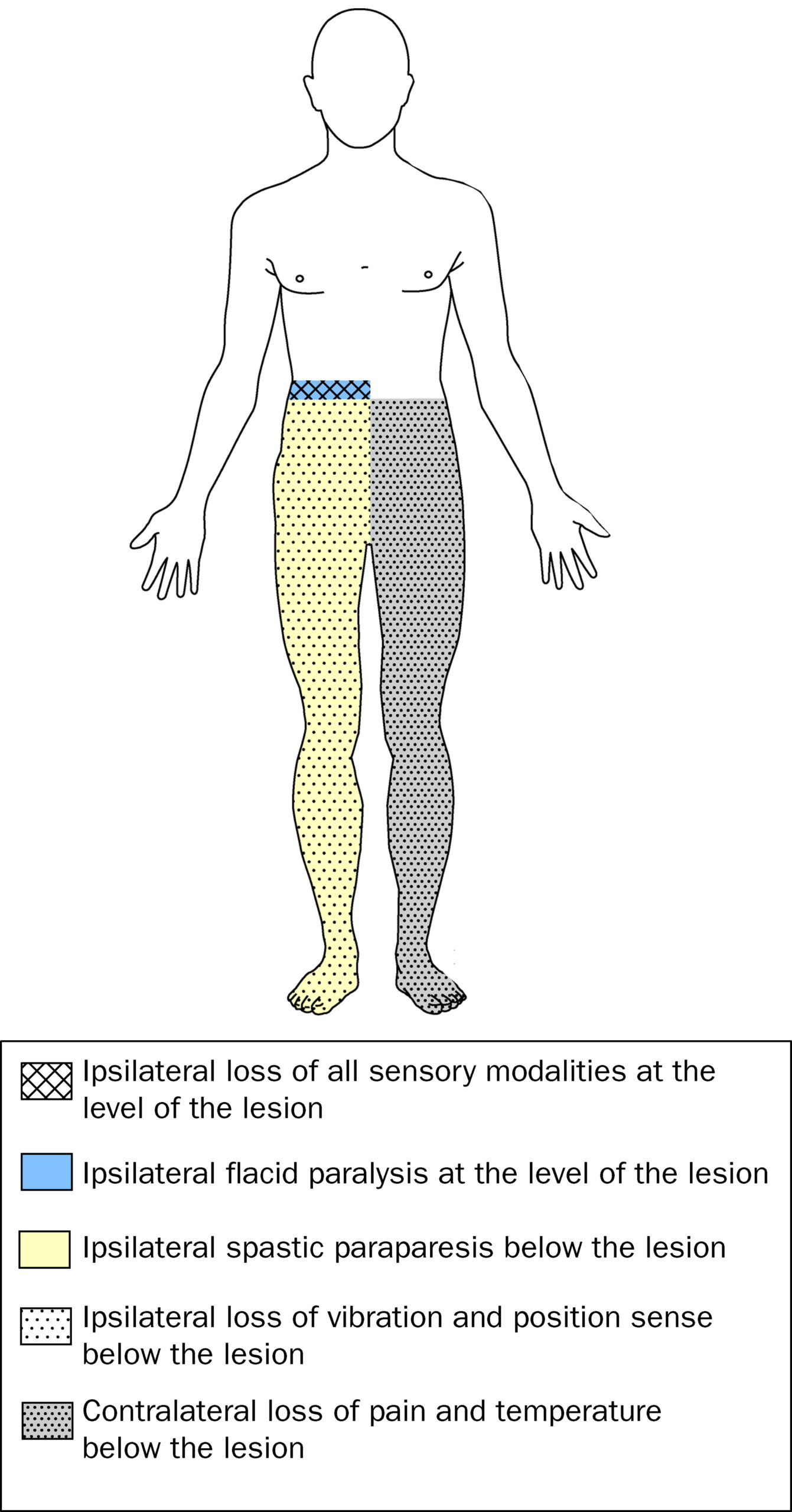
A healthy 29-year-old man developed Brown-Sequard syndrome immediately after performing a manipulation on his own cervical spine. Brown-Sequard syndrome is characterized by a lesion in the spinal cord which results in weakness or paralysis (hemiparaplegia) on one side of the body and a loss of sensation (hemianesthesia) on the opposite side.
Imaging showed large disc herniations at the levels of C4-C5 and C5-C6 with severe cord compression. The patient underwent emergent surgical decompression. He was discharged to an acute rehabilitation hospital, where he made a full functional recovery by postoperative day 8.
The authors concluded that this case highlights the benefit of swift surgical intervention followed by intensive inpatient rehab. It also serves as a warning for those who perform self-cervical manipulation.
I would add that the case also serves as a warning for those who are considering having cervical manipulation from a chiropractor. Such cases have been reported regularly. Here are three of them:
A spinal epidural hematoma is an extremely rare complication of cervical spine manipulation therapy (CSMT). The authors present the case of an adult woman, otherwise in good health, who developed Brown-Séquard syndrome after CSMT. Decompressive surgery performed within 8 hours after the onset of symptoms allowed for complete recovery of the patient’s preoperative neurological deficit. The unique feature of this case was the magnetic resonance image showing increased signal intensity in the paraspinal musculature consistent with a contusion, which probably formed after SMT. The pertinent literature is also reviewed.
Another case was reported of increased signal in the left hemicord at the C4 level on T2-weighted MR images after chiropractic manipulation, consistent with a contusion. The patient displayed clinical features of Brown-Séquard syndrome, which stabilized with immobilization and steroids. Follow-up imaging showed decreased cord swelling with persistent increased signal. After physical therapy, the patient regained strength on the left side, with residual decreased sensation of pain involving the right arm.
A further case was presented in which such a lesion developed after chiropractic manipulation of the neck. The patient presented with a Brown-Séquard syndrome, which has only rarely been reported in association with cervical epidural hematoma. The correct diagnosis was obtained by computed tomographic scanning. Surgical evacuation of the hematoma was followed by full recovery.
Brown-Séquard syndrome after spinal manipulation seems to be a rare event. Yet, nobody can provide reliable incidence figures because there is no post-marketing surveillance in this area.
Today is the start of chiropractic awareness week 2022. On this occasion the BCA states most categorically: First and foremost, chiropractic is a statutorily regulated healthcare profession, supported by evidence, which offers a safe form of treatment for patients with a range of conditions. Here I am tempted to cite my friend Simon Singh:
THEY HAPPILY PROMOTE BOGUS TREATMENTS
I am, of course, particularly impressed by the BCA’s assurance of safety. In my view, the safety issue needs to be addressed more urgently than any other in the realm of chiropractic. So, to make a meaningful contribution to the current chiropractic awareness week, I conducted a few Medline searches to identify all publications of 2022 on chiropractic/spinal manipulation risks.
This is what I found:
Objective: Patients can be at risk of carotid artery dissection and ischemic stroke after cervical chiropractic manipulation. However, such risks are rarely reported and raising awareness can increase the safety of chiropractic manipulations.
Case report: We present two middle-aged patients with carotid artery dissection leading to ischemic stroke after receiving chiropractic manipulation in Foshan, Guangdong Province, China. Both patients had new-onset pain in their necks after receiving chiropractic manipulations. Excess physical force during chiropractic manipulation may present a risk to patients. Patient was administered with recombinant tissue plasminogen activator after radiological diagnoses. They were prescribed 100 mg and clopidogrel 75 mg daily for 3 months as dual antiplatelet therapy. There were no complications over the follow-up period.
Conclusion: These cases suggest that dissection of the carotid artery can occur as the result of chiropractic manipulations. Patients should be diagnosed and treated early to achieve positive outcomes. The safety of chiropractic manipulations should be increased by raising awareness about the potential risks.
Spontaneous intracranial hypotension (SIH) still remains an underdiagnosed etiology of new-onset headache. Important risk factors include chiropractic manipulation (CM). We present a case of a 36-year-old Filipino woman who presented with severe bifrontal and postural headache associated with dizziness, vomiting, and doubling of vision. A cranial computed tomography scan was done which showed an acute subdural hematoma (SDH) at the interhemispheric area. Pain medications were given which afforded minimal relief. On history, the headaches occurred 2 weeks after cervical CM. Cranial and cervical magnetic resonance imaging revealed findings supportive of intracranial hypotension and neck trauma, respectively. The patient improved with conservative management. We found 12 articles on SIH and CM after a systematic review of literature. Eleven patients (90.9%) initially presented with orthostatic headache. Eight patients (66.7%) were initially treated conservatively but only 5 (62.5%) had complete recovery. Recovery was achieved within 14 days from start of supportive therapy. Among the 3 patients who failed conservative treatment, 2 underwent non-directed epidural blood patch and one required neurosurgical intervention. This report highlights that a thorough history is warranted in patients with new onset headache. A history of CM must be actively sought. The limited evidence from the case reports showed that patients with SIH and SDH but with normal neurologic examination and minor spinal pathology can be managed conservatively for less than 2 weeks. This review showed that conservative treatment in a closely monitored environment may be an appropriate first line treatment.
Introduction: Cranio-cervical artery dissection (CeAD) is a common cause of cerebrovascular events in young subjects with no clear treatment strategy established. We evaluated the incidence of major adverse cardiovascular events (MACE) in CeAD patients treated with and without stent placement.
Methods: COMParative effectiveness of treatment options in cervical Artery diSSection (COMPASS) is a single high-volume center observational, retrospective longitudinal registry that enrolled consecutive CeAD patients over a 2-year period. Patients were ≥ 18 years of age with confirmed extra- or intracranial CeAD on imaging. Enrolled participants were followed for 1 year evaluating MACE as the primary endpoint.
Results: One-hundred ten patients were enrolled (age 53 ± 15.9, 56% Caucasian, and 50% male, BMI 28.9 ± 9.2). Grade I, II, III, and IV blunt vascular injury was noted in 16%, 33%, 19%, and 32%, respectively. Predisposing factors were noted in the majority (78%), including sneezing, carrying heavy load, chiropractic manipulation. Stent was placed in 10 (10%) subjects (extracranial carotid n = 9; intracranial carotid n = 1; extracranial vertebral n = 1) at the physician’s discretion along with medical management. Reasons for stent placement were early development of high-grade stenosis or expanding pseudoaneurysm. Stented patients experienced no procedural or in-hospital complications and no MACE between discharge and 1 year follow up. CeAD patients treated with medical management only had 14% MACE at 1 year.
Conclusion: In this single high-volume center cohort of CeAD patients, stenting was found to be beneficial, particularly with development of high-grade stenosis or expanding pseudoaneurysm. These results warrant confirmation by a randomized clinical trial.
Background: Manipulation and mobilisation for low back pain are presented in an evidence-based manner with regard to mechanisms of action, indications, efficacy, cost-effectiveness ratio, user criteria and adverse effects. Terms such as non-specific or specific are replaced by the introduction of “entities” related to possible different low back pain forms.
Efficacy: MM is effective for acute and chronic low back pain in terms of pain relief, recovery of function and relapse prevention. It is equally effective but less risky compared to other recommended therapies. MM can be used alone in acute cases and not only in the case of chronic low back pain where it is always and necessarily part of a multimodal therapy programme, especially in combination with activating measures. The users of MM should exclusively be physician specialists trained according to the criteria of the German Medical Association (Bundesärztekammer) with an additional competence in manual medicine or appropriately trained certified therapists. The application of MM follows all rules of Good Clinical Practice.
Adverse effects: Significant adverse effects of MM for low back pain are reported in the international literature with a frequency of 1 per 50,000 to 1 per 3.7 million applications, i.e. MM for low back pain is practically risk-free and safe if performed according to the rules of the European Training Requirements of the UEMS.
Studies have reported that mild adverse events (AEs) are common after manual therapy and that there is a risk of serious injury. We aimed to assess the safety of Chuna manipulation therapy (CMT), a traditional manual Korean therapy, by analysing AEs in patients who underwent this treatment. Patients who received at least one session of CMT between December 2009 and March 2019 at 14 Korean medicine hospitals were included. Electronic patient charts and internal audit data obtained from situation report logs were retrospectively analysed. All data were reviewed by two researchers. The inter-rater agreement was assessed using the Cohen’s kappa coefficient, and reliability analysis among hospitals was assessed using Cronbach’s Alpha coefficient. In total, 2,682,258 CMT procedures were performed in 289,953 patients during the study period. There were 50 AEs, including worsened pain (n = 29), rib fracture (n = 11), falls during treatment (n = 6), chest pain (n = 2), dizziness (n = 1), and unpleasant feeling (n = 1). The incidence of mild to moderate AEs was 1.83 (95% confidence interval [CI] 1.36-2.39) per 100,000 treatment sessions, and that of severe AEs was 0.04 (95% CI 0.00-0.16) per 100,000 treatment sessions. Thus, AEs of any level of severity were very rare after CMT. Moreover, there were no instances of carotid artery dissection or spinal cord injury, which are the most severe AEs associated with manual therapy in other countries.
_______________________________
This is not too bad after all!
Five papers are clearly better than nothing.
What conclusions might be drawn from my mini-review?
I think it might be safe to say:
- There is not much but at least some research going on in this area.
- The risks of chiropractic/spinal manipulation are real and are being recognized.
- BUT NOT BY CHIROPRACTORS! The most remarkable feature of the 5 papers, I think, is that none originates from a chiropractic team.
Thus, allow me to make a suggestion to chiropractors worldwide: Instead of continuing with HAPPILY PROMOTING BOGUS TREATMENTS, what about using the ‘chiropractic awareness week’ to raise awareness of the urgent necessity to research the safety of your treatments?
Dr Akbar Khan, MD, represents a novel and exciting avenue through which, in this case, a conventionally- trained family physician has come to embrace a broad array of integrative techniques; he witnessed first hand the immense magnitude of safety and efficacy of the practice … Dr Khan describes with frustration the lack of interest displayed by conventional practitioners for safe and effective solutions simply because they come from the realm of natural medicine. “My greatest concern is helping patients.”

From left to right: Douglas Andrews, Akbar Khan, Silvana Marra and Humaira Khan
From left to right: Douglas Andrews, Akbar Khan, Silvana Marra and Humaira Khan[/caption]
An article in the ‘Toronto Sun’, however, tells a very different story. The doctor was found ‘incompetent’ in the treatment of cancer patients. Akbar Khan told one patient she had leukemia when she did not. He told others they were improving under his alternative remedies while their cancer was actually advancing. One of them was a little boy dying of a brain tumor.
Now the Toronto family doctor has been found guilty by the Ontario Physicians and Surgeons Discipline Tribunal of
- incompetence,
- failure to maintain the standard of practice,
- and conduct that’s disgraceful, dishonorable or unprofessional
in his care of a total of 12 patients between 2012 and 2017. “Whether it was ‘snake oil,’ ‘witches’ brew’ or otherwise, whatever it was that Dr. Khan was offering his patients, it was not what he claimed,” concluded the tribunal in its decision. “In doing so, Dr. Khan set aside his obligations as a physician to uphold the College’s CAM and consent policies, and in doing so, he failed his patients.”
Khan is the founder of the Medicor Cancer Centres, which offer “unique non-toxic approaches to cancer treatment.” He treated terminally-ill patients with the unproven treatments that he called “SAFE Chemotherapy” billed as “lifesaving” and more effective than conventional chemo.
There was insufficient science and evidence to support the conclusion that “SAFE chemotherapy” works, or that it can help people in the way that Dr. Khan claims it can, and he should not have used it,” the tribunal found. Yet, Khan never told his patients it wasn’t working. According to the college’s summary: “Therapy stopped only when his patients either could not afford it any longer, their condition had deteriorated to such a degree that they could not tolerate it, they were so ill that they were admitted to hospital, or they died.”
According to the tribunal, Khan’s patients paid (US)$4,200 for one cycle of “SAFE chemotherapy”, and they received between five to 24 cycles of it. One of the most heartbreaking cases involved Khan’s treatment of a six-year-old boy with brain cancer. In 2017, his parents rejected treating him with lifesaving chemo and radiation and transferred his care to Khan, who prescribed Dichloroacetate (DCA) — which is a medication usually used for metabolic disorders, and not a proven cancer treatment. When a follow-up MRI showed their son’s tumor had grown and progressed to his spine, Khan told them it must be wrong and “his current therapy is actually working very well!” The boy died in 2018.
In another disturbing case, Khan used an “unapproved” test to diagnose a 59-year-old woman with acute leukemia — and informed her by email. He treated the devastated woman with honokol, a biological extract from magnolia bark, and Low Dose Naltrexone (LDN) — both of which are “not informed by evidence and science,” and “not the appropriate treatment for this patient’s presumed cancer.” Khan referred her to an oncologist who performed a bone marrow biopsy and then gave her the good news: “You do not have cancer. You’ve never had cancer. Go home and enjoy your life.” Yet, Khan insisted the oncologist was wrong. “We were frankly shocked that instead of reassuring Ms. B that her ordeal of worrying that she had leukemia could come to a close, Dr. Khan insisted to Ms. B that indeed, she did still have leukemia and urged her to keep taking LDN ‘to keep this under control,’” the tribunal wrote. “In short, Dr. Khan gave Ms. B a diagnosis that she did not have, for which he sold her a remedy that she did not need, which — as per evidence and science — turned out to be no remedy at all.”Khan’s response to the newspaper: “Since the legal process is still ongoing with the CPSO, I know my lawyer Marie Henein would not like me to comment at this time. Perhaps in the near future, I will be able to share with you another side to the story. If so, I will contact you.”
A penalty hearing has yet to be scheduled.
In case you are interested, here is a short CV of Dr. Khan:
| 2019 | FAAO – Fellow of the American Academy of Ozone Therapy |
| 2018 | Certified medical ozone therapy doctor (general ozone therapy, basic ProlozoneTM therapy and advanced ProlozoneTM therapy), certified by the American Academy of Ozone Therapy |
| 2018 | IMD, Integrative Medical Doctor (Board of Integrative Medicine) DHS, Doctor of Humanitarian Service (Board of Integrative Medicine) |
| 1994 | CCFP, Certificant of the College of Family Physicians of Canada (University of Toronto). |
| 1992 | MD, Doctor of Medicine (University of Toronto). |
Neurosurgeons from the Philippines recently presented the case of a 36-year-old woman who presented with severe bifrontal and postural headache associated with dizziness, vomiting, and double vision. A cranial computed tomography scan showed an acute subdural hematoma (SDH) at the interhemispheric area. Pain medications were given which afforded minimal relief.
The headaches occurred 2 weeks after the patient had received a cervical chiropractic manipulation (CM). Cranial and cervical magnetic resonance imaging revealed findings supportive of intracranial hypotension and neck trauma. The patient improved with conservative management.
The authors found 12 articles of SIH and CM after a systematic review of the literature. Eleven patients (90.9%) initially presented with orthostatic headaches. Eight patients (66.7%) were initially treated conservatively but only 5 (62.5%) had a complete recovery. Recovery was achieved within 14 days from the start of supportive therapy. Among the 3 patients who failed conservative treatment, 2 underwent non-directed epidural blood patch, and one required neurosurgical intervention.
The authors concluded that this report highlights that a thorough history is warranted in patients with new-onset headaches. A history of CM must be actively sought. The limited evidence from the case reports showed that patients with SIH and SDH but with normal neurologic examination and minor spinal pathology can be managed conservatively for less than 2 weeks. This review showed that conservative treatment in a closely monitored environment may be an appropriate first-line treatment.
As the authors rightly state, their case report does not stand alone. There are many more. In 2014, an Australian chiropractor published this review:
Background: Intracranial hypotension (IH) is caused by a leakage of cerebrospinal fluid (often from a tear in the dura) which commonly produces an orthostatic headache. It has been reported to occur after trivial cervical spine trauma including spinal manipulation. Some authors have recommended specifically questioning patients regarding any chiropractic spinal manipulation therapy (CSMT). Therefore, it is important to review the literature regarding chiropractic and IH.
Objective: To identify key factors that may increase the possibility of IH after CSMT.
Method: A systematic search of the Medline, Embase, Mantis and PubMed databases (from 1991 to 2011) was conducted for studies using the keywords chiropractic and IH. Each paper was reviewed to examine any description of the key factors for IH, the relationship or characteristics of treatment, and the significance of CSMT to IH. In addition, other items that were assessed included the presence of any risk factors, neck pain and headache.
Results: The search of the databases identified 39 papers that fulfilled initial search criteria, from which only eight case reports were relevant for review (after removal of duplicate papers or papers excluded after the abstract was reviewed). The key factors for IH (identified from the existing literature) were recent trauma, connective tissue disorders, or otherwise cases were reported as spontaneous. A detailed critique of these cases demonstrated that five of eight cases (63%) had non-chiropractic SMT (i.e. SMT technique typically used by medical practitioners). In addition, most cases (88%) had minimal or no discussion of the onset of the presenting symptoms prior to SMT and whether the onset may have indicated any contraindications to SMT. No case reports included information on recent trauma, changes in headache patterns or connective tissue disorders.
Discussion: Even though type of SMT often indicates that a chiropractor was not the practitioner that delivered the treatment, chiropractic is specifically cited as either the cause of IH or an important factor. There are so much missing data in the case reports that one cannot determine whether the practitioner was negligent (in clinical history taking) or whether the SMT procedure itself was poorly administered.
The new case report can, of course, be criticized for being not conclusive and for not allowing to firmly establish the cause of the adverse event. This is to a large extent due to the nature of case reports. Essentially, they provide a ‘signal’, and once the signal is loud enough, we need to act. In this case, action would mean to prohibit the intervention that is under suspicion and initiate conclusive research to prove or disprove a causal relationship.
This is how it’s done in most areas of healthcare … except, of course in so-called alternative medicine(SCAM). Here we do not even have the most basic tool to get to the bottom of the problem, namely a transparent post-marketing surveillance system that monitors the frequency of adverse events.
And whose responsibility is it to put such a system in place?
I let you guess.
Guest post by Catherine de Jong
On the 22nd of February 2022, a criminal court in the Netherlands ruled in a case brought by a 33-year-old man who suffered a double-sided vascular dissection of his vertebral arteries during a chiropractic neck manipulation.
What happened?
On the 26th of January 2016, the man visited a chiropractor because he wanted treatment for his headache. The chiropractor treated him with manipulations of his neck. The first treatment was uneventful but apparently not effective. The man went back for a second time. Immediately after the second treatment, the patient felt a tingling sensation that started in his toes and spread all over his body. Then he lost consciousness. He was resuscitated by the chiropractor and transported to a hospital. Several days later he woke up in the ICU of the university hospital (Free University, now Amsterdam UMC). He was paralyzed and unable to speak. He stayed in the ICU for 5 weeks. After a long stay in a rehabilitation center, he is now at home. He is disabled and incapacitated for life.
Court battles
The professional liability insurance of the chiropractor recognized that the treatment of the chiropractor had caused the disability and paid for damages. The patient was thus able to buy a new wheelchair-adapted house.
Health Inspection investigated the case. They noticed that the chiropractor could not show that there was informed consent for the neck manipulation treatment, but otherwise saw no need for action.
Six days after the accident the man applied to the criminal court. The case was dropped because, according to the judge, proof of guilt beyond reasonable doubt was impossible.
In rare occasions, vertebral artery dissection (VAD) does occur spontaneously in people without trauma or a chiropractor manipulating their neck. The list of causes for VAD show, besides severe trauma to the head and neck (traffic accidents) also chiropractic treatment, and rare connective tissue diseases like Marfan syndrome. A spontaneous dissection is very rare.
It took several attempts to persuade the criminal court to start the case and the investigation into what had happened in the chiropractor’s office. Now the verdict has been given, and it was a disappointing one.
The chiropractor was acquitted. The defense of the chiropractor argued, as expected, that two pre-existent spontaneous dissections might have caused the headache and that, therefore, the manipulation of the neck would have played at most a secondary role.
It is this defense strategy, which is invariably followed in the numerous court cases in the US. Chiropractors in particular give credence to this argumentation.
The defense of the patient was a professor of neurology. He considered a causal link between manipulation to the neck and the double-sided VAD to be proven.
In the judgment, the judge refers 14 times to the ‘professional standard’ of the Dutch Chiropractors Association, apparently without realizing that this professional standard was devised by the chiropractors themselves and that it differs considerably from the guidelines of neurologists or orthopedics. In 2016, the Dutch Health Inspection disallowed neck manipulation, but chiropractors do not care.
The verdict of the judge can be found here: ECLI:EN:RBNHO:2022:1401
Chiropractic is a profession that is not recognized in the Netherlands. Enough has been written (also on this website) about the strange belief of chiropractors that a wrong position of the vertebrae (“subluxations”) is responsible for 95% of all health problems and that detecting and correcting them can relieve symptoms and improve overall health. There is no scientific evidence that chiropractic subluxations exist or that their alleged “detection” or “correction” provides any health benefit. In the Netherlands, there are about 300 practicing chiropractors. Most are educated in the UK or the USA. The training that those chiropractors receive is not recognized in the Netherlands.
Most chiropractic treatments do little harm, but that does not apply to neck manipulation. When manipulating the neck, the outstretched head is subjected to powerful stretches and rotations. This treatment can in rare cases cause damage to the arteries, which carry blood to the brain. In this case, a double-sided cervical arterial dissection can lead to strokes and cerebral infarctions. How often this occurs (where is the central complication registration of chiropractors?) is unknown, but given that the effectiveness of this treatment has never been demonstrated and that therefore its risk/benefit ratio is negative, any complication is unacceptable.
How big is the chance that a 33-year-old man walks into a chiropractor’s office with a headache and comes out with a SPONTANEOUS double-sided vertebral artery dissection that leaves him wheelchair-bound and invalid for the rest of his life? I hope some clever statisticians will tell me.
PS
Most newspaper reports of this case are in Dutch, but here is one in English
On this blog, I have been regularly discussing the risks of so-called alternative medicine (SCAM). In particular, I have often been writing about the risks of chiropractic spinal manipulations.
Why?
Some claim because I have an ax to grind – and, in a way, they are correct: I do feel strongly that consumers should be warned about the risks of all types of SCAM, and when it comes to direct risks, chiropractic happens to feature prominently.
But it’s all based on case reports which are never conclusive and usually not even well done.
This often-voiced chiropractic defense is, of course, is only partly true. But even if it were entirely correct, it would beg the question: WHY?
Why do we have to refer to case reports when discussing the risks of chiropractic? The answer is simple: Because there is no proper system of monitoring its risks.
And why not?
Chiropractors claim it is because the risks are non-existent or very rare or only minor or negligible compared to the risks of other therapies. This, I fear, is false. But how can I substantiate my fear? Perhaps by listing a few posts I have previously published on the direct risks of chiropractic spinal manipulation. Here is a list (probably not entirely complete):
- Chiropractic manipulations are a risk factor for vertebral artery dissections
- Vertebral artery dissection after chiropractic manipulation: yet another case
- The risks of (chiropractic) spinal manipulative therapy in children under 10 years
- A risk-benefit assessment of (chiropractic) neck manipulation
- The risk of (chiropractic) spinal manipulations: a new article
- New data on the risk of stroke due to chiropractic spinal manipulation
- The risks of manual therapies like chiropractic seem to out-weigh the benefits
- One chiropractic treatment followed by two strokes
- An outstanding article on the subject of harms of chiropractic
- Death by chiropractic neck manipulation? More details on the Lawler case
- Severe adverse effects of chiropractic in children Another serious complication after chiropractic manipulation; best to avoid neck manipulations altogether, I think
- Ophthalmic Adverse Effects after Chiropractic Neck Manipulation
- Is chiropractic treatment safe?
- Cervical artery dissection and stroke related to chiropractic manipulation
- We have an ethical, legal and moral duty to discourage chiropractic neck manipulations
- Cerebral Haemorrhage Following Chiropractic ‘Activator’ Treatment
- Vertebral artery dissection after chiropractic manipulation: yet another case
- Horner Syndrome after chiropractic spinal manipulation
- Phrenic nerve injury: a rare but serious complication of chiropractic neck manipulation
- Chiropractic neck manipulation can cause stroke
- Chiropractic and other manipulative therapies can also harm children
- Complications after chiropractic manipulations: probably rare but certainly serious
- Disc herniation after chiropractic
- Evidence for a causal link between chiropractic treatment and adverse effects
- More on the risks of spinal manipulation
- The risk of neck manipulation
- “As soon as the chiropractor manipulated my neck, everything went black”
- Spinal epidural haematoma after neck manipulation
- New review confirms: neck manipulations are dangerous
- Top model died ‘as a result of visiting a chiropractor’
- Another wheelchair filled with the help of a chiropractor
- Spinal manipulation: a treatment to die for?
Of course, one can argue about the conclusiveness of this or that case report, but I feel that the collective evidence discussed in these posts makes my point abundantly clear:
chiropractic spinal manipulation is not safe.
Vertebral artery dissection is an uncommon, but potentially fatal, vascular event. This case aimed to describe the pathogenesis and clinical presentation of vertebral artery dissection in a term pregnant patient. Moreover, the authors focused on the differential diagnosis, reviewing the available evidence.
A 39-year-old Caucasian woman presented at 38 + 4 weeks of gestation with a short-term history of vertigo, nausea, and vomiting. Symptoms appeared a few days after cervical spine manipulation by an osteopathic specialist. Urgent magnetic resonance imaging of the head was obtained and revealed an ischemic lesion of the right posterolateral portion of the brain bulb. A subsequent computed tomography angiographic scan of the head and neck showed a right vertebral artery dissection. Based on the correlation of the neurological manifestations and imaging findings, a diagnosis of vertebral artery dissection was established. The patient started low-dose acetylsalicylic acid and prophylactic enoxaparin following an urgent cesarean section.

Right vertebral artery dissection with ischemia in the posterolateral medulla oblongata. In DWI (a) and ADC map (b) the arrow shows a punctate, shiny ischemic lesion, with typical reduction of ADC in the right posterolateral medulla oblongata. c and d CT angiography (axial and 3D reformat, c and d, respectively) showing a focal dissection of the V2 distal segment of the right vertebral artery, with the arrow in figure c pointing to the dissection. e MRI angiography (time of flight, TOF) showing the absence of visualization of right PICA.
The authors concluded that vertebral artery dissection is a rare but potential cause of neurologic impairments in pregnancy and during the postpartum period. It should be considered in the differential diagnosis for women who present with headache and/or vertigo. Women with a history of migraines, hypertension, or autoimmune disorders in pregnancy are at higher risk, as well as following cervical spine manipulations. Prompt diagnosis and management of vertebral artery dissection are essential to ensure favorable outcomes.
In the discussion section, the authors point out that the incidence of VAD in pregnancy is twice as common as in the rest of the female population. They also mention that a review of the literature regarding adverse effects of spinal manipulation in the pregnant and postpartum periods identified adverse events in five pregnant women and two postpartum women. The authors also include a table that summarizes all cases of VAD reported both prior and after delivery, with 24 cases distributed with a prevalence during the postpartum period (19 of the 24 cases). The clinical presentation of these cases is varied, with a higher frequency of headaches, vertigo, and diplopia, and the risk factors most represented are hypertension and migraines.
The authors finish with this advice: practitioners who do spinal manipulations should be aware of the possible complications of neck manipulation in pregnancy and the postpartum period, particularly in mothers with underlying medical disorders that may predispose to vessel fragility and VAD.
I would add advice of a different nature: consumers should always question whether the risks of any intervention outweigh its benefit. In the case of neck manipulations, the answer is not positive.
We have discussed the use of bleach, MMS, and related products as a so-called alternative medicine (SCAM) several times before. This regularly prompts advocates of this approach to claim that they are effective and safe. A recent case report seems to suggest otherwise. 
A 9-year-old boy presented with his brother after they accidentally ingested a small amount of undiluted 22.4% sodium chlorite. Symptoms included nausea, vomiting, diarrhea, and dyspnea. Oxygen saturation remained 71% despite supplemental oxygen (15L/min). The patient was noted to have dark chocolate-appearing blood, minimal urine output, diffuse pallor, and cyanosis. He developed methemoglobinemia, renal failure requiring renal replacement therapy, and hemolysis requiring blood transfusion. The authors reveal that these are the 7th and 8th reported cases of sodium chlorite toxicity by ingestion and the second and third in children.
The authors conclude that Miracle Mineral Solution is a commonly purchased potentially lethal compound that can cause methemoglobinemia with respiratory failure, hemolytic anemia requiring transfusion, and renal failure requiring dialysis.
Despite such cases, MMS continues to be promoted for viral and many other diseases, including cancer. Anyone truthfully stating that it is ineffective and dangerous is branded as a pharma shill who is biased against MMS. Would the ‘bleach boys’ claim the same about an agency like the UK Food Standards Authority?
Let’s see!
This is what the FSA says about MMS:
… Sodium chlorite products vary in concentration, specific dosage and method of ingestion.
With products of weaker strength, any health impact from consuming these products is likely to be gastrointestinal irritation.
For stronger products, the effects can be severe nausea, vomiting and diarrhoea, potentially leading to dehydration and reduced blood pressure.
If the solution is diluted less than instructed, it could cause damage to the gut and red blood cells, potentially resulting in respiratory failure.
There are a range of alleged health benefits related to these products and all are unlikely to be authorised. Only nutrition claims listed in the GB NHC Register (Opens in a new window)may be used in Great Britain.
Health and nutrition claims are required to be authorised under retained Regulation 1924/2006 (Opens in a new window), as amended by The Nutrition (Amendment etc.) (EU Exit) Regulations 2019 (Opens in a new window)and The Nutrition (Amendment etc.) (EU Exit) Regulations 2020 (Opens in a new window). As well as being authorised and recorded on the GB NHC Register, the claim must not be ‘false, ambiguous or misleading’.
Some health claims about this product that relate to the treatment of cancer may also be in contravention of the Cancer Act 1939.
Claims range from generic statements about ‘purifying’ the body to more specific ones around cancer and autistic spectrum disorders…