case report
An article in THE TIMES seems worth mentioning. Here are some excerpts:
… Maternity care at Nottingham University Hospitals NHS Trust (NUH) is the subject of an inquiry, prompted by dozens of baby deaths. More than 450 families have now come forward to take part in the review, led by the expert midwife Donna Ockenden. The trust now faces further scrutiny over its use of aromatherapy, after experts branded guidelines at the trust “shocking” and not backed by evidence. Several bereaved families have said they recall aromatherapy being heavily promoted at the trust’s maternity units.
It is being prosecuted over the death of baby Wynter Andrews just 23 minutes after she was born in September 2019. Her mother Sarah Andrews wrote on Twitter that she remembered aromatherapy being seen as “the answer to everything”. Internal guidelines, first highlighted by the maternity commentator Catherine Roy, suggest using essential oils if the placenta does not follow the baby out of the womb quickly enough… the NUH guidelines say aromatherapy can help expel the placenta, and suggest midwives ask women to inhale oils such as clary sage, jasmine, lavender or basil, while applying others as an abdominal compress. They also describe the oils as “extremely effective for the prevention of and, in some cases, the treatment of infection”. The guidelines also suggest essential oils to help women suffering from cystitis, or as a compress on a caesarean section wound. Nice guidelines for those situations do not recommend aromatherapy…
The NUH adds frankincense “may calm hysteria” and is “recommended in situations of maternal panic”. Roy said: “It is shocking that dangerous advice seemed to have been approved by a team of healthcare professionals at NUH. There is a high tolerance for pseudoscience in NHS maternity care … and it needs to stop. Women deserve high quality care, not dangerous quackery.” …
________________________________
The journalist who wrote the article also asked me for a comment, and I emailed her this quote: “Aromatherapy is little more than a bit of pampering; no doubt it is enjoyable but it is not an effective therapy for anything. To use it in medical emergencies seems irresponsible to say the least.” The Times evidently decided not to include my thoughts.
Having now read the article, I checked again and failed to find good evidence for aromatherapy for any of the mentioned conditions. However, I did find an article and an announcement both of which are quite worrying, in my view:
Aromatherapy is often misunderstood and consequently somewhat marginalized. Because of a basic misinterpretation, the integration of aromatherapy into UK hospitals is not moving forward as quickly as it might. Aromatherapy in UK is primarily aimed at enhancing patient care or improving patient satisfaction, and it is frequently mixed with massage. Little focus is given to the real clinical potential, except for a few pockets such as the Micap/South Manchester University initiative which led to a Phase 1 clinical trial into the effects of aromatherapy on infection carried out in the Burns Unit of Wythenshawe Hospital. This article discusses the expansion of aromatherapy within the US and follows 10 years of developing protocols and policies that led to pilot studies on radiation burns, chemo-induced nausea, slow-healing wounds, Alzheimers and end-of-life agitation. The article poses two questions: should nursing take aromatherapy more seriously and do nurses really need 60 hours of massage to use aromatherapy as part of nursing practice?
My own views on aromatherapy are expressed in our now not entirely up-to-date review:
Aromatherapy is the therapeutic use of essential oil from herbs, flowers, and other plants. The aim of this overview was to provide an overview of systematic reviews evaluating the effectiveness of aromatherapy. We searched 12 electronic databases and our departmental files without restrictions of time or language. The methodological quality of all systematic reviews was evaluated independently by two authors. Of 201 potentially relevant publications, 10 met our inclusion criteria. Most of the systematic reviews were of poor methodological quality. The clinical subject areas were hypertension, depression, anxiety, pain relief, and dementia. For none of the conditions was the evidence convincing. Several SRs of aromatherapy have recently been published. Due to a number of caveats, the evidence is not sufficiently convincing that aromatherapy is an effective therapy for any condition.
In this context, it might also be worth mentioning that we warned about the frequent usage of quackery in midwifery years ago. Here is our systematic review of 2012 published in a leading midwifery journal:
Background: in recent years, several surveys have suggested that many midwives use some form of complementary/alternative therapy (CAT), often without the knowledge of obstetricians.
Objective: to systematically review all surveys of CAT use by midwives.
Search strategy: six electronic databases were searched using text terms and MeSH for CAT and midwifery.
Selection criteria: surveys were included if they reported quantitative data on the prevalence of CAT use by midwives.
Data collection and analysis: full-text articles of all relevant surveys were obtained. Data were extracted according to pre-defined criteria.
Main results: 19 surveys met the inclusion criteria. Most were recent and from the USA. Prevalence data varied but were usually high, often close to 100%. Much use of CATs does not seem to be supported by strong evidence for efficacy.
Conclusion: most midwives seem to use CATs. As not all CATs are without risks, the issue should be debated openly.
I am tired of saying ‘I TOLD YOU SO!’ but nevertheless find it a pity that our warning remained (yet again) unheeded!
Reports of serious complications of chiropractic manipulation keep on coming. Take this one, for instance:
My daughter went for a routine chiropractor appointment. Now she’s paralysed – 1:20 000 chiropractic neck manipulations result in stroke from vertebral artery dissection.

Or take a recent article by US neurosurgeons:
Cranio-cervical artery dissection (CeAD) is a common cause of cerebrovascular events in young subjects with no clear treatment strategy established. This study evaluated the incidence of major adverse cardiovascular events (MACE) in CeAD patients treated with and without stent placement. COMParative effectiveness of treatment options in cervical Artery diSSection (COMPASS) is a single high-volume center observational, retrospective longitudinal registry that enrolled consecutive CeAD patients over a 2-year period. Patients were ≥ 18 years of age with confirmed extra- or intracranial CeAD on imaging. Enrolled participants were followed for 1 year evaluating MACE as the primary endpoint.
One-hundred ten patients were enrolled (age 53 ± 15.9, 56% Caucasian, and 50% male, BMI 28.9 ± 9.2). Grade I, II, III, and IV blunt vascular injury was noted in 16%, 33%, 19%, and 32%, respectively. Predisposing factors were noted in the majority (78%), including
- sneezing,
- carrying a heavy load,
- chiropractic manipulation.
Stent was placed in 10 (10%) subjects (extracranial carotid n = 9; intracranial carotid n = 1; extracranial vertebral n = 1) at the physician’s discretion along with medical management. Reasons for stent placement were early development of high-grade stenosis or expanding pseudoaneurysm. Stented patients experienced no procedural or in-hospital complications and no MACE between discharge and 1 year follow up. CeAD patients treated with medical management only had 14% MACE at 1 year.
The authors concluded that in this single high-volume center cohort of CeAD patients, stenting was found to be beneficial, particularly with development of high-grade stenosis or expanding pseudoaneurysm. These results warrant confirmation by a randomized clinical trial.
Yes, I know: this study was not meant to investigate the link between chiropractic manipulations and CeAD. The finding that chiropractic manipulation is a predisposing factor for CeAD is entirely incidental. But it is an important finding nevertheless.
Chiropractors will laugh about the notion that manipulation is a risk factor akin to sneezing and thus try to trivialize the danger of their treatments. I would then point out that sneezing is unavoidable and fulfills a purpose. Chiropractic manipulations do neither.
It has been reported by several outlets that a young woman is fighting for her life after a chiropractic adjustment went horribly wrong. Caitlin Jensen had only recently graduated from University. When she went for what was meant to be a simple chiropractic adjustment on June 16, she suffered four dissected arteries in her neck, this damage led to cardiac arrest, stroke and her being without a pulse for over 10 minutes, requiring resuscitation.
She was rushed to the Memorial Hospital in Savannah, Georgia, where she was operated on. She was then taken to the neuro ICU in a critical condition with a traumatic brain injury. Every day since she’s been fighting. Currently, she is conscious and able to respond to verbal commands by blinking her eyes, as well as wiggling the toes of her left foot. However, most of her body remains paralyzed.
Her mother Darlene has been posting updates about her daughter’s condition on Facebook. On Saturday Darlene shared the latest news on the condition of her daughter. “She gave her best effort to smile today, and it was the most beautiful thing I’ve ever seen,” Darlene said. “She is progressing with her movements on the left side – wiggling and flexing. She can’t lift her arm yet, or turn her head. Her right side is unchanged – still no movement. Her face doesn’t move very much yet, but she can open her eyes widely to show surprise, and the left corner of her mouth tries to smile. Adorable. Still working on the pneumonia. The antiplatelet therapy seems to be going OK. We don’t see any signs of internal bleeding and are praying that it stays that way.”

And the day before, Darlene posted: “Two weeks ago tonight we didn’t know if Caitlin would make it through the night,” Darlene said. “Dire and catastrophic are two of the words that we heard from our ICU team. We knew they didn’t casually throw around words like that. But – she is alive, and every day is a little better. The accomplishments are both small and monumental at the same time. Today, she gave us a thumbs up. We have been working on this, and she got it! She also nodded again today. It helps to see these things because it reassures us that she is working hard to stay with us and recover. Caitlin is strong, disciplined, and well practised in exercising her brain, and I truly believe that her science background and all of her time studying is going to help her in this long journey. “
Studies have found that traumatic cervical artery dissection is one of the leading causes of stroke in patients under the age of 45, and recent chiropractic neck manipulation is among factors that can be associated with risk of vertebral artery dissection.
Following the tragedy, Caitlin’s mother, Darlene, launched a GoFundMe and has raised more than US$20,000 (AU $29,334 or £16,512) for her ongoing medical expenses.
It is clear that these news reports lack important medical details. What is equally clear is the fact that most such cases are never reported in the medical literature and are thus available only in this fragmented form. The reason for this lamentable situation is obvious: there is no post-marketing surveillance system for chiropractic (such a safeguard would be bad for business, of course).
Consequently, chiropractors across the globe continue to be able to say that such reports are unreliable. The medical literature, they are keen to point out, holds only very few case studies of serious risks of chiropractic spinal manipulation. Hence they falsely claim on every possible occasion that their adjustments are safe. The end effect is that many consumers continue to wrongly assume that chiropractic manipulations might be worth a try.
Guest post by Ken McLeod
Believe it or not, there are practitioners of a health system with little or no evidence of efficacy and safety who are registered with the Australian Health Practitioner Registration Agency. That is, so-called Traditional Chinese Medicine, whose practitioners are registered alongside evidence-based practitioners such as doctors, nurses, pharmacists, and dentists.
Governments who framed the relevant legislation evidently hoped that registration would enable the public to have confidence that they would be treated with evidence-based medicine. Such confidence is misplaced, as has been shown in The Skeptic and elsewhere many times.
Here’s another example of the failure of the health practitioner registration system.
Jamie Lloyd Allan is registered with AHPRA with the Chinese Medical Registration Number CMR0002096457, with no endorsements. He practices at his clinic in eastern Sydney. He advertises at his website meridianremedies.com.au.
And some of his claims are deeply worrying. Allan claims that he uses “Chinese Herbal medicine & Acupuncture in conjunction with testing and removal of accumulated toxins and heavy metals, developing comprehensive individualised herbal antimicrobial and detoxification protocols.”
He claims that “toxins and heavy metals … enter our bodies, disrupt normal healthy cell behaviour, impair our immune system, often contribute and sometimes cause many different types of illnesses and health conditions.”
His claims are designed to generate unfounded worries in people, offering a smorgasbord of claims how he can help people learn [the words and spelling are his]:
• how mercury from common amalgam fillings can be passed from mother to child to grandchild and why preconception detoxification is important;
• how to assess a dentist to know your [sic] getting the best and safest care during amalgam removal;
• about mercury/autism connection, heavy metal accumulation and neurological diseases such as Alzheimer’s, Parkinson’s and Dementia;
• more about mercury, aluminium, cadmium and lead toxicity;
• how heavy metal accumulation acts as an antenna for electromagnetic radiation from devices such as wifi, cell phone, cordless phones, thus focusing the frequencies on the areas where the metals are stored, causing changes in the proteins and even DNA;
• the science behind electromagnetic radiation and how it affects human cells;
• Glyphosate toxicity, and how many of us have it and how it affects our health, and lots more.
Allan goes into the alleged toxicity of mercury amalgam fillings further at his blog. I should not have to say it, but his claims are baseless and have been debunked many times. The US Food and Drug Administration has said that existing evidence shows that dental amalgam is not harmful to the general population (tinyurl.com/589mbrr6). And as Scientific American said “Mercury and Autism: Enough Already! The science shows that they have nothing to do with each other and never have.” (tinyurl.com/mwwdxxak)
Allan also writes extensively on “EMF Sensitivity Wi-Fi and Cell Phone radiation – Heavy Metals and EMF Sensitivity and Autism” – he claims “Autism rates double every 5 years and the only thing that parallels that in our environment is the increase of man made Electro magnetic Radiation and fields largely in the high frequencies from cell phone Wi-Fi, smart meters and other Electro magnetic devices.’ This is unconscionable; scaring potential clients with this, while conveniently forgetting that correlation does not mean causation.
Allan also offers the following techniques as a “Detox for autism”:
• Sauna or heat therapy (far infrared is best) Cold shower straight after to close pores and wash of toxins
• Clay plasters, Clay on scars, then shower
• Ionic Foot Cleanses, Detox baths, Takara foot Pads, or raw white potato strapped on soles of feet
• Fibre + Enemas or colonics, slippery elm, keep bowls [sic] moving
• Liver gall bladder flush with lemon oil
• Exercise, dry skin brush
• Chi Machine for lymph drainage and movement to parasympathetic dominance
• Olive or other healthy oils for swish and spit
• Genetic, vitamin, mineral testing to guide your diet and supplements
• Western and Chinese Herbs to detox bowls [sic], liver, kidney, lymph
• Homeopathic drops & plenty of water orally
• Laser Energetic detox
• Ozonized bath, Epson salt bath
• Enema for detox reactions in kids
• Stronger detox agents DMPS, DMSA, EDTA can be used in case of high-level toxicity. For children, the use of the above mention techniques over DMPS, DMSA and EDTA is preferred first.
“Raw white potato strapped on soles of feet”!! Come on! This is lunacy. And enemas for children? And what qualifications does Allan hold to diagnose and administer these dangerous pharmaceuticals?
Luckily, Allan offers the perfect scanner to diagnose what’s wrong with you, the Oligoscan.
As described, “This a [sic] spectrographic-based test. Every element on the periodic table has its own unique absorption spectra, meaning that different elements absorb certain wavelengths of light, and reflect others. The spectra of lead will be different from that of mercury, or calcium, or any other element. The Oligoscan shines a laser on different points on the hand, and based off of [sic] which wavelengths of light are absorbed or reflected back, the levels of different metals and minerals in the cells of your hand can be determined. This is similar to how astronomers can analyze the wavelengths of light emitted by distant stars to determine their chemical make-up.
“The Oligoscan has the advantage of testing the levels of metals that are actually in your cells, not what you are able to excrete. It tests the heavy metal load of the tissues. This is important because heavy metals have a affinity [sic] for tissues and are often store [sic] there and not in the blood. It can also measure aluminium, which most other tests will miss. Oligoscan results tend to correlate with other accurate tests.”
A search of the TGA’s register of therapeutic goods did not find the Oligoscan listed.
Clearly, Allan is engaged in a process of scaring potential clients with misinformation, then offering diagnostic and treatment processes that are deceptive, ineffective and dangerous, and not listed with the TGA; for all of which he is not qualified.
COMPLAINT PROCESS
A complaint was sent to the NSW Health Care Complaints Commission describing the above issues. (In NSW and Queensland, complaints concerning health care practitioners, registered and unregistered, are lodged with the relevant State authorities, the HCCC and OHO respectively.) We added that “This should not be treated as merely a case of misleading advertising; Allan is clearly endangering the public, so I recommend a thorough audit of his practice, and when my allegations are found to be proven, suitable disciplinary action taken and entered on the AHPRA register.”
The HCCC responded saying “Following consultation with the Chinese Medicine Council of New South Wales, it was decided to refer this matter to the Australian Health Practitioner
Regulation Agency (AHPRA) as AHPRA is the designated agency to manage concerns about advertising. We did not identify any other issues that would require further action by the Commission.” (We approached the Chinese Medicine Council of NSW – their response is quoted in the sidebar.)
The HCCC continued: “The Commission obtained a written response from Mr Allan. In his response to the Commission, Mr Allan stated that he had no record of providing any care and treatment to you.
“Mr Allan acknowledged that his website may have created a misunderstanding about what actual treatments are offered at his clinic, and what was on his website for educational purposes only.
“Mr Allan noted that he has never owned an Oligoscan or used it at his clinic, he has therefore removed that information from his website.
“Mr Allan confirmed that he does not offer the techniques under the heading ‘detox for autism’ at his clinic, the information was for educational purposes only, and he has now removed this information from his website.
“Further, Mr Allan has confirmed that he has removed the information on his website about Glyphosate Toxicity, Toxicity of Mercury Amalgam fillings, Nutrition for Autism, and all avenues of receiving mercury toxicity.
“Mr Allan also stated that he has since edited the information on EMF Sensitivity Wi-Fi and Cell Phone radiation – Heavy Metals and EMF Sensitivity Autism, as well as editing the information contained on the home and about pages of his website.
“Mr Allan stated that he has left the resources section with all the raw studies, and some information contained in other sections, as he feels that they are of use for anybody wanting to learn more about this specialised area.”
So, in spite of the detailed evidence and a call for a thorough audit of his practice, this was treated as merely a case of misleading advertising. This is standard operating procedure; the regulatory authorities cannot get over the divide between advertising and clinical practice. This has been shown in the hundreds of complaints sent to regulators; misleading advertising of dangerous practices and misinformation is simply treated as an advertising issue. The regulators cannot accept that if a practitioner advertises a therapy then they are more than likely using those therapies and, when those therapies have been found to be ineffective, they are engaging in practice in their clinics that deserves more than the dismissive response we received.
The public deserve much better than that.
Note: All of the quotes above were from Allan’s website until he removed them. The relevant pages have, nonetheless, can be accessed via the WayBack Machine, and can be supplied if required.
The Chinese Medicine Council’s position
The Chinese Medical Council were referred to the issues in the main article and were asked the following questions:
• Is the advice and those therapies [offered by Allan] of any concern to the Council?
• Should the complaint to the NSW Health Care Complaints Commission have led to an audit of his practice and when the allegations are proven, should there have been disciplinary action?
A spokesperson for the Chinese Medicine Council of NSW replied: “The Chinese Medicine Council of NSW (the Council) works in collaboration with the NSW Health Care Complaints Commission (HCCC) to receive and manage complaints about registered practitioners in
NSW. Our paramount legal obligation is to protect the public. We deal with practitioners whose conduct, performance or health may represent a risk to the public or is not in the public interest.
“We do this by assessing complaints, promoting compliance with professional standards and delivering programs to ensure practitioners provide safe care to the public and their patients. We do not have the legal power to discipline a NSW practitioner or to deregister them.
“By law, the Council cannot provide information about an individual practitioner. Only information that is publicly available can be disclosed, such as information recorded on the national register of practitioners which is maintained by the Australian Health Practitioner Regulation Agency (AHPRA), or publication of the outcomes of NCAT [New South Wales Civil and Administrative Tribunal] proceedings.
“Changes to a registered health practitioner’s registration status, such as the imposition of conditions or suspension, are published on the AHPRA online public register.
“The Council will not be making any further public comments at this time.
So, the Chinese Medicine Council have taken no action to protect the public and made no real comment. At least they have promised “Only information that is publicly available can be disclosed”, a statement of breathless inanity.
*‘first published in the Australian Skeptic magazine of June 2022.
In India, the homeopathic remedy, Arsenicum Album 30C (prepared from arsenic trioxide) is widely prescribed and publicly supplied to adults and children for preventing COVID infections. Inorganic arsenic, known as the “king of poisons” is a highly toxic substance with the potential to cause acute as well as chronic injury to multiple organ systems, mainly skin, lung, liver, and kidneys.
Indian researchers present three cases of acute liver injury, leading to the death of one patient with underlying non-alcoholic steatohepatitis (NASH) cirrhosis, after consumption of the homeopathic remedy AA30 for COVID-19 prevention.
Case one
A 70-year-old man with compensated non-alcoholic steatohepatitis (NASH)-related cirrhosis and diabetes mellitus consumed the homeopathic IB AA30 as prescribed for 12 weeks prior to the onset of symptoms. He presented with jaundice and abdominal distension within four weeks after the onset of loss of appetite and well-being. The patient was not on any other hepatotoxic agents, over-the-counter medications, or herbal and dietary supplements. Investigations revealed the presence of conjugated hyperbilirubinemia, ascites, and abnormal coagulation, suggestive of acute-on-chronic liver failure (ACLF). Further investigations to identify known causes of acute deterioration of underlying cirrhosis were performed, including a transjugular liver biopsy. All competing causes for acute liver injury were meticulously ruled out. These included infections-tests for immunoglobulin M (IgM) for viral hepatitis A and E; hepatitis B surface antigen and IgM antibody to hepatitis B core antigen; nucleic acid tests via polymerase chain reaction for hepatitis C; IgM for herpes zoster and herpes simplex, cytomegalovirus, parvovirus, Epstein-Barr virus. Complete auto-antibody testing for autoimmune hepatitis (AIH) was negative. The Roussel Uclaf Causality Assessment (RUCAM) demonstrated “probable” (score 7) drug-induced liver injury (DILI) and simplified AIH score was less than 5, revealing the cause of acute liver injury leading to ACLF as the homeopathic remedy, AA30. The liver biopsy revealed multiacinar hepatocyte necrosis, lymphocytic, neutrophilic, and eosinophilic inflammation in the absence of interface hepatitis, which were predominantly portal-based in the background of cirrhosis, suggestive of DILI. Analysis of drugs consumed could not be performed in view of inadequate sample availability. The patient and family consented to arsenic analysis in nail and hair samples which revealed extremely high levels of the heavy metal, supportive of arsenic toxicity and associated liver injury in the patient. Evaluation of hair and hair samples of two family members (below detection limits, method detection limit being 0.1 mg/kg), staying in the same household did not reveal levels signifying cluster arsenic poisoning from water or soil sources. The patient succumbed to complications related to ACLF, nine months after the initial diagnosis.
Case two
A 68-year-old male with systemic hypertension controlled on telmisartan who ingested AA30 as prescribed for four weeks prior to the onset of symptoms. There was no associated jaundice or cholestatic symptoms, but liver tests revealed acute hepatitis with an elevation of liver enzymes. The patient was not on any other hepatotoxic agents, over-the-counter medications, or herbal and dietary supplements. Further investigations did not reveal the presence of underlying chronic liver disease or portal hypertension. All competing causes for acute liver injury were meticulously ruled out similar to the extensive workup that was done in case one. The RUCAM demonstrated “probable” (score 8) DILI and simplified AIH score was less than 5, revealing the cause of acute non-icteric hepatitis as the homeopathic remedy, AA30. The liver biopsy revealed perivenular hepatocyte necrosis, with predominantly portal-based mixed cellular inflammation consisting of plasma cells, eosinophils, lymphocytes, and scattered neutrophils. Additionally, ballooning of hepatocytes was marked with scattered rosettes and moderate interphase hepatitis in the presence of mild portal and sinusoidal fibrosis suggestive of DILI. Acute hepatitis resolved after drug withdrawal and finite course of steroids within three months, without any recurrence on follow-up.
Case three
A 48-year-old overweight woman consumed homeopathic AA30 pills as COVID-19 preventive for one week prior to the onset of her symptoms of cholestatic jaundice. Prior to the development of jaundice, she had nonspecific gastrointestinal symptoms such as nausea and progressive loss of appetite. Liver tests revealed conjugated hyperbilirubinemia with highly raised liver enzymes. The patient was not on any other hepatotoxic prescription drugs, over-the-counter medications, or herbal and dietary supplements. Further investigations did not reveal the presence of underlying chronic liver disease or portal hypertension. All competing causes for acute liver injury were meticulously ruled out similar to the extensive workup that was done in case one. The RUCAM demonstrated “probable” (score 7) DILI and simplified AIH score was less than 5, revealing the cause of acute cholestatic hepatitis as the homeopathic remedy, AA30. The liver biopsy revealed spotty, focal hepatocyte necrosis, with predominantly portal-based neutrophilic and eosinophil-rich inflammation, moderate steatosis, and mild interface hepatitis with underlying mild perisinusoidal fibrosis, suggestive of DILI. The acute cholestatic hepatitis resolved after drug withdrawal and a finite course of steroids within six months, without any recurrence on follow-up.
The chemical analysis and toxicology (inductively coupled optical emission spectroscopy and triple-quadrupole gas chromatography with tandem mass spectroscopy method) on two sets of AA30 samples retrieved from case three revealed D-mannose, melezitose, and arsenic respectively, demonstrating batch-to-batch variation due to poor manufacturing practices.
The authors draw the following conclusions: Health regulatory authorities, physicians, general and patient population must be aware of the potential harms associated with the large-scale promotion of untested, alternative medical systems during a medical emergency so as to prevent an “epidemic” of avoidable DILI within the ongoing pandemic. Even though ultra-diluted homeopathic remedies, found ineffective as shown in large-scale meta-analysis, are considered safe for use due to the absence of any active compound beyond 12C dilution. Nonetheless, poor manufacturing practices, use of concentrated tincture formulations, and adulteration and contamination of homeopathic remedies can still pose considerable toxicity in predisposed persons. From a scientific and evidence-based standpoint, it is imperative that the general population and at-risk persons understand that vaccination, and not untested, misleading IBs, remains the best available armamentarium against COVID-19 which helps in fighting back the pandemic.
I came across an interesting case report recently published in an Austrian magazine. Here is my translation for non-German speakers:
A 42-year-old woman from Vienna has suffered from endometriosis since the age of 13. But it was only 8 years later that she found out what made the first two days of her menstruation so unbearable. She was not allowed to take painkillers to help herself during all that time. Her parents listened to medical “gurus” who distrusted conventional medicine.
“I grew up in a household where almost all illnesses were treated with homeopathy,” she wrote on Twitter. That’s exactly what became the IT expert’s undoing. In a recent interview, she looked back bitterly: “All infections and illnesses were treated with Bach flower remedies or homeopathics. Only in case of accidents or broken bones did my parents drive me to the hospital.” Her father suffered from an auto-immune disease. Because conventional medicine could not help him, he tried alternative approaches. “My parents slowly drifted more and more into this scene. At some point, they stopped listening to ‘normal’ doctors. It went downhill from there.”
As a girl, the Viennese had little chance of standing up to her parents’ “whisperers,” as she calls their esoteric advice. “When I got my period, I was in the worst pain. I fainted every month, even falling off my chair when I did it, once even at school. I vomited until I was so exhausted that I fell asleep.”
She begged her family to finally be allowed to consult a gynecologist. But he didn’t take the teenager seriously at the time and simply wanted to prescribe her the pill without a thorough examination. “I then went to my parents’ homeopathic ‘pill pusher’, who gave me homeopathics against my complaints. I wasn’t allowed to take painkillers because they ‘damage the liver’.” The guru persuaded the young woman that her health problems were her fault. “He said I just didn’t accept myself as a woman and that’s why I was in pain. I thought for a long time that I was just not strong and good enough.”
It wasn’t until she was already in her early 20s that her then-boyfriend took her to a gynecologist who finally took her condition seriously. “The ultrasound showed that I had quite a few cysts in my abdomen.” The diagnosis was also finally certain: she was now officially suffering from endometriosis. She was given the right medicine, and most of the endometriotic growths regressed. But a cyst had wrapped itself tightly around her right ovary, damaging it irrevocably over the years. It had died. “Homeopathy cost me my ovary,” the Viennese woman laments.
The fact that she nevertheless was able to become the mother of two children is thanks to her other ovary, which fortunately remained intact. But the feeling of having been treated wrongly, or not treated at all, for such a long time makes her angry. “I don’t blame my parents today. They have apologized and found their own way out of the gurus’ world of thought and out of the scene,” she emphasizes. “But I blame the people who pretend to be able to cure the majority of all diseases with homeopathy. Yet most of the time they can’t even find the right diagnosis and just give patients some stuff that has no side effects.” She now calls for an end to homeopathy.
_________________________
How many times have I said it?
His remedy might be risk-free, but the homeopath certainly isn’t!
Quackademia is a lovely term for describing quackery at the academic level. The name may be amusing but the phenomenon isn’t. And this seems to be nowhere more true than in the US. The Certificate in Holistic Health and Healing Arts (HHHA) at the University of New Mexico allegedly “lays the groundwork for careers in holistic health and the healing arts while familiarizing students with practices that promote self-healing, longevity, and vitality.” To me, it seems to be a prime example of quackademia. Here is a selection of the courses offered by the HHHA:
INTRODUCTION TO HEALING ARTS
HHHA 101 (3 credits)
This entirely-online class grounds students in the foundation of Holistic Health and Healing Arts, introducing a wide range of healing modalities so that students can discover what works best for them. Often offered in Fall semester and asynchronously online.
This course is required for the HHHA Certificate.
MEDITATION, CONSCIOUSNESS, and SELF-HEALING
HHHA 102 (3 credits)
This course invites students to explore the deeply rejuvenating effects of meditation and mindfulness. Often offered fall semester.
This course is required for the HHHA Certificate.
HATHA YOGA
HHHA 104 (3 credits)
Students practice of fundamental and accessible asanas and discuss philosophy and ethics through the lens of Patanjali’s Yoga Sutras and Iyengar’s Light on Yoga. Students will also lead practices and discussions of their choosing. Often offered in spring.
This course is required for the 200-Hour Yoga Teacher Training Diploma.
TAI-JI/QIGONG
HHHA 105 (3 credits)
Students practice meditative movements that restore vitality, improve balance, increase strength and promote the wellbeing of mind, body, and spirit. Often offered over Summer semester.
YOGA FOR WELLNESS
HHHA 110 (1-3 Credits)
This beginner-friendly movement class will focus on stress reduction, flexibility, and general wellbeing. Offered varying semesters, usually face-to-face.
INTRODUCTION TO ORIENTAL MEDICINE
HHHA 116 (3 credits)
This class illuminates the fundamentals of this ancient system of medicine which emphasizes the interconnectedness of the body and the world. Often offered in Fall semester.
DREAMS, VISIONS, AND ARTMAKING
HHHA 117 (3 credits)
Students are led on a journey of self-discovery through guided visualizations. The images and intuition students tap into serve as fodder for their own creative work. Often offered in Fall semester, face-to-face.
AYURVEDA
HHHA 118 (3 credits)
This class introduces the ancient Indian healing modality called “The Science of Life” and guides students to an awareness of their constitutions (doshas). Students learn the nutritional and lifestyle approaches that can help create greater energetic balance. Often offered in Fall semester.
YOGA STYLES AND SAFETY
HHHA 120 (3 credits)
This class explores the different styles of yoga as well as ways of sequencing and cuing poses. Students show their understanding of class concepts through practice teaching. Often offered in Fall semester.
This course is required for the 200-Hour Yoga Teacher Training Diploma.
YOGA FOR COMMON CONDITIONS
HHHA 121
(3 credits)
The class will prepare future yoga teachers and/or interested yoga students to design classes for themselves and others that safely accommodate many underlying injuries and conditions, observing, in the process, that a class that accommodates students with underlying conditions is a class for everyone. Often offered in Fall semester.
This course is required for the 200-Hour Yoga Teacher Training Diploma.
REIKI HEALING I
HHHA 146 (3 credits)
This introduction to energy work helps students to develop their energetic sensitivity and spiritual awareness while learning hands-on and intention-based techniques that encourage bodies to heal themselves. Often offered in Fall semester, face-to-face.
REIKI HEALING II
HHHA 147 (3 credits)
This class builds on the principles introduced in Reiki Healing I. Often offered in Fall semester, face-to-face.
INTRODUCTION TO HOMEOPATHY
HHHA 148 (3 credits)
Students learn the philosophical underpinnings and practical applications of homeopathy, a complete therapeutic system of medicine that aims to promote general health and reinforce the body’s own natural healing capacity. Often offered in Spring semester and asynchronously online.
YOGA AND PSYCHOLOGY OF THE CHAKRAS
HHHA 263 (3 credits)
Guided by Anodea Judith’s seminal Eastern Body, Western Mind, students explore the energetics as well as the biomechanics and alignment of the body chakra by chakra. Students will show their mastery of the concepts covered through practice teaching and reflective written assignments. May be offered spring or fall.
This course is required for the 200-Hour Yoga Teacher Training Diploma.
This amount of cheer nonsense taught at the university level beats everything I have seen before. Perhaps it is not that unusual in the US, yet after having been a university professor in three European countries, I find it truly baffling. Call me old-fashioned, but I had always assumed that the educational function of universities was about teaching knowledge and facts rather than myths and delusions. Universities must be the guardians of reason, not its destructors! How long will it be, I ask myself, until the first US university introduces a course in the design of flying carpets or a diploma in telekinesis?
Almost 10 years ago, I posted this:
When I decided to become a doctor I, like most medical students, did so mainly to help suffering individuals. When I became a researcher, I felt more removed from this original ideal. Yet I told myself that, by conducting research, I might eventually contribute to a better health care of tomorrow. Helping suffering patients was still firmly on the agenda. But then I realised that my articles in peer-reviewed medical journals somehow missed an important target: in alternative medicine, one ought to speak not just to health care professionals but also to consumers and patients; after all, it is they who often make the therapeutic decisions in this area.
Once I had realised this, I started addressing the general public by writing for The Guardian and other newspapers, giving public lectures and publishing books for a lay audience, like TRICK OR TREATMENT…The more I did this sort of thing, the more I noticed how important this activity was. And when a friend offered to help me set up a blog, I did not hesitate for long.
So, the reason for my enthusiasm for this blog turns out to be the same as the one that enticed me to go into medicine in the first place. I do believe that it is helpful for consumers to know the truth about alternative medicine. Considering the thousands of sources of daily misinformation in this area, there is an urgent need for well-informed, critical information. By providing it, I am sure I can assist people to make better therapeutic decisions. In a way, I am back where I started all those years ago: hoping to help suffering patients in the most direct way my expertise allows.
Helping vulnerable patients often means warning them from dangerous charlatans, and this is precisely what I frequently try to do with this blog. But how successful are my endeavors?
More often than not, I have no idea and can only hope for the best. Sometimes I do get some feedback that is encouraging and motivates me to carry on. Rarely, however, do I witness immediate, tangible success. And this is why the recent story is so remarkable:
- On 6 June, an Australian acquaintance from the FRIENDS OF SCIENCE IN MEDICINE sent me some material about a planned lecture in the UK by someone promoting dangerous quackery.
- I looked into it and published a blog post about it a few hours later.
- A reader then suggested in the comments section of this post alerting the UK press to it.
- Another reader contacted THE TIMES, and I wrote to several other journalists.
- THE TIMES turned out to be interested in the story.
- They did some research and interviewed Michael Marshall from the GOOD THINKING SOCIETY (and myself).
- Today, THE TIMES published an article about the planned event.
- Finally, a kind person made the article available to those who don’t want to pay for it.
The whole thing amounts to superb teamwork, in my view. It shows how like-minded people who do not even all know each other can manage to achieve a respectable result with little more than goodwill and dedication.
A respectable result?
Of course, the optimal result would be to stop Barbara O’Neill’s UK lectures. Let’s hope this is what eventually will happen – and please let me know if you know more.
Necrotizing infection (NI) of the breast associated with underlying malignancy is a rare phenomenon characterized by necrosis of breast parenchyma. It can cause a delay in diagnosis and even lead to sepsis. Researchers from the Aga Khan University Hospital in Karachi, PAK, present a case of a 42-year-old woman with NI of the right breast, while on homeopathic treatment for a right breast lump for six months. Tissue culture showed a polymicrobial infection and histopathology established the diagnosis of breast carcinoma. After treating the NI, her breast cancer was managed as per standard guidelines.
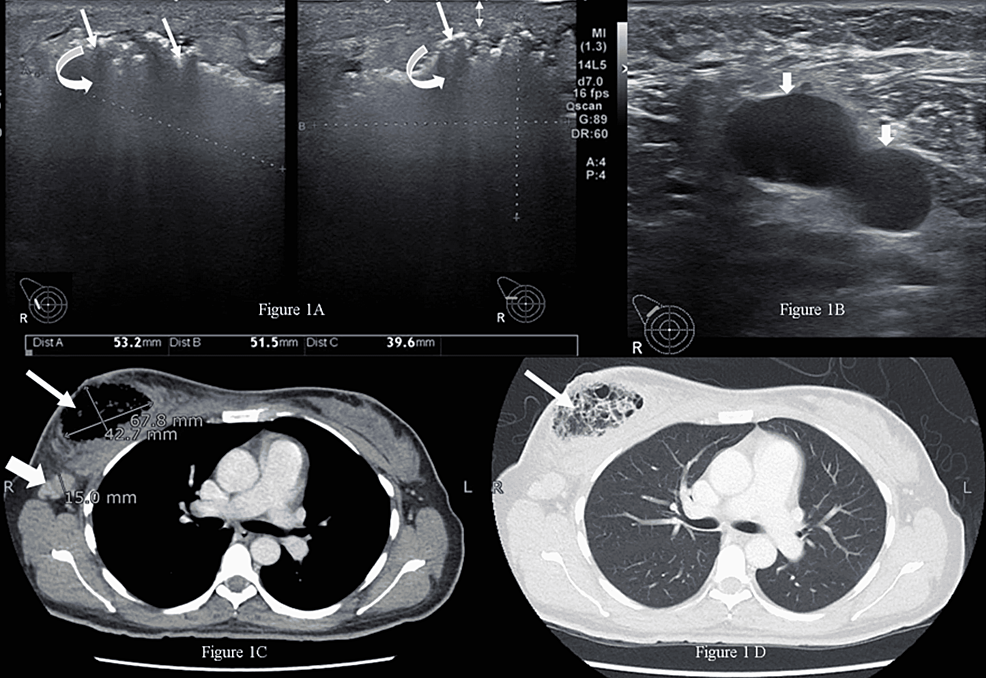
The married, nulliparous, diabetic, hypertensive patient was a non-smoker and presented to the emergency room with complaints of fever, severe pain, and foul-smelling bloody discharge from her right breast for two weeks. She had a history of a right breast lump for six months, for which she had been taking oral homeopathic remedies, the names of which were not recorded. On examination, she had a blood pressure of 132/76 mmHg, a pulse of 84 bpm, a temperature of 99 °F, and a respiratory rate of 14 breaths per minute. The right breast was tender and hard, with a 4 x 3-cm necrotic skin patch on the upper half with bleeding and a palpable right axillary lymph node. The rest of the examination was unremarkable.
The patient was advised to undergo a metastatic workup in the emergency room, which included a contrast-enhanced CT (CECT) of the chest, abdomen, and pelvis and a bone scan. The CT confirmed the presence of an air-filled cavity in the right breast with thin septations and enlarged right axillary lymph nodes; however, there was no enhancing mass to suggest neoplasm in either breast. The CT and bone scans were negative for metastasis. The presence of severely tender breast on clinical examination and air within the breast on ultrasound suggested the possibility of NI, which warranted an early surgical intervention to prevent impending sepsis.
Microscopic examination of the debrided tissue revealed an invasive breast carcinoma of no special type [invasive ductal carcinoma (IDC), NST grade III] along with extensive necrosis and dense acute and chronic inflammation. The right axillary node biopsy was positive for nodal metastasis, and the patient was staged as cT4N1MO. A tissue culture showed a few colonies of Staphylococcus aureus and Enterococcus species suggestive of NI. After a discussion at a multidisciplinary tumor board meeting, the patient underwent a right modified radical mastectomy. Her postoperative course was unremarkable.
____________________
I have said it often but I am afraid I need to say it again: the homeopathic remedy might be harmless, but that does not mean that homeopathy is not dangerous.
I did not know what a ‘body modification provider’ is. My first guess was that it is a car mechanic who specializes in making my vehicle look ok again after I had a minor accident. But I was wrong! In fact, it is a new healthcare profession – one that we are well-advised to avoid, as it turns out. A Media Release from the Health Care Complaints Commission of Australia dated 27 May, 2022 informed us that:
The NSW Health Care Complaints Commission (Commission) investigated the conduct of Mr Brendan Russell, a body modification provider.
In his capacity as a body modification provider, conducting invasive surgical procedures and administering sedation, Mr Russell is a non-registered health practitioner and subject to the Code of Conduct for non-registered health practitioners (Code of Conduct) set out in schedule 3 of the Public Health Regulation 2012.
Mr Russell was charged with criminal offences relating to services provided to three clients. One related to the removal of part of a client’s labia. Another related to the death of a client following a subdermal implant of a silicone object into the client’s right hand. Mr Russell also performed abdominal surgery on another client making incisions into her abdominal tissue to remove fat.
Following convictions in November 2021 for Intentionally Causing Grievous Bodily Harm, Aid/Abet/Counsel or Procure Female Genital Mutilation and Manslaughter, Mr Russell has breached numerous clauses of the Code of Conduct, and it has been determined that he poses a risk to the health and safety of members of the public.
An Interim Prohibition order has been in place to protect the public during the criminal proceedings. The Commission has now imposed a Permanent Prohibition Order under section 41A(2)(a) of the Health Care Complaints Act 1993 (Act):
Mr Brendan Russell, a body modification provider, is permanently prohibited from providing any health services, either in paid employment or voluntarily, to any member of the public.
___________________________________
What is all this about? Has this man gone doolally? In particular, what is the removal of a woman’s labia supposed to be for? Here is what Wikipedia says about it:
Labiaplasty (also known as labioplasty, labia minora reduction, and labial reduction) is a plastic surgery procedure for altering the labia minora (inner labia) and the labia majora (outer labia), the folds of skin surrounding the human vulva. There are two main categories of women seeking cosmetic genital surgery: those with congenital conditions such as intersex, and those with no underlying condition who experience physical discomfort or wish to alter the appearance of their genitals because they believe they do not fall within a normal range.[1]
The size, colour, and shape of labia vary significantly, and may change as a result of childbirth, aging, and other events.[1] Conditions addressed by labiaplasty include congenital defects and abnormalities such as vaginal atresia (absent vaginal passage), Müllerian agenesis (malformed uterus and fallopian tubes), intersex conditions (male and female sexual characteristics in a person); and tearing and stretching of the labia minora caused by childbirth, accident, and age. In a male-to-female sexual reassignment vaginoplasty for the creation of a neovagina, labiaplasty creates labia where once there were none.
A 2008 study reported that 32 percent of women who underwent the procedure did so to correct a functional impairment; 31 percent to correct a functional impairment and for aesthetic reasons; and 37 percent for aesthetic reasons alone.[2] According to a 2011 review, overall patient satisfaction is in the 90–95 percent range.[3] Risks include permanent scarring, infections, bleeding, irritation, and nerve damage leading to increased or decreased sensitivity. A change in requirements of publicly funded Australian plastic surgery requiring women to be told about natural variation in labias led to a 28% reduction in the number of surgeries performed.[4] Unlike public hospitals, cosmetic surgeons in private practice are not required to follow these rules, and critics say that “unscrupulous” providers are charging to perform the procedure on women who would not want it if they had more information.[4]
______________________________
So, now we know. The procedure belongs in the hands of plastic surgeons, not some ‘body modification provider’. S0-called alternative medicine (SCAM) really is a scam where anything goes. Homeopaths claim to cure cancer, chiropractors believe they can treat anything from deafness and heart disease, acupuncturists feel they can reduce body weight, and now ‘body modification providers’ think they are plastic surgeons. What is more, the amazing thing is: there are always some people gullible enough to believe them.
Brave new world!