case-control study
A team of chiropractic researchers conducted a review of the safety of spinal manipulative therapy (SMT) in children under 10 years. They aimed to:
1) describe adverse events;
2) report the incidence of adverse events;
3) determine whether SMT increases the risk of adverse events compared to other interventions.
They searched MEDLINE, CINAHL, and Index to Chiropractic Literature from January 1, 1990 to August 1, 2019. Eligible studies were case reports/series, cohort studies and randomized controlled trials. Studies of high and acceptable methodological quality were included.
Most adverse events are mild (e.g., increased crying, soreness). One case report describes a severe adverse event (rib fracture in a 21-day-old) and another an indirect harm in a 4-month-old. The incidence of mild adverse events ranges from 0.3% (95% CI: 0.06, 1.82) to 22.22% (95% CI: 6.32, 54.74). Whether SMT increases the risk of adverse events in children is unknown.
The authors concluded that the risk of moderate and severe adverse events is unknown in children treated with SMT. It is unclear whether SMT increases the risk of adverse events in children < 10 years.
Thanks to their ingenious methodology, the authors managed to miss 11 of the 13 studies included in the review by Vohra et al which reported 9 serious adverse events and 20 cases of delayed diagnosis associated with SMT. Another review reported 15 serious adverse events and 775 mild to moderate adverse events following manual therapy. As far as I can see, the authors of the new review make just one reasonable point:
We recommend the implementation of a population-based active surveillance program to measure the incidence of severe and serious adverse events following SMT treatment in this population.
In the absence of such a surveillance system, any incidence figures are not just guess-work but also a depiction of the tip of a much bigger iceberg. So, why do the authors of this review not make this point clearly and powerfully? Why does the review read mostly like an attempt to white-wash a thorny subject? Why do they not provide a breakdown of the adverse events according to profession? The answer to these questions can be found at the very end of the paper:
This study was supported by the College of Chiropractors of British Columbia to Ontario Tech University. The College of Chiropractors of British Columbia was not involved in the design, conduct or interpretation of the research that informed the research. This research was undertaken, in part, thanks to funding from the Canada Research Chairs program to Pierre Côté who holds the Canada Research Chair in Disability Prevention and Rehabilitation at Ontario Tech University, and from the Canadian Chiropractic Research Foundation to Carol Cancelliere who holds a Research Chair in Knowledge Translation in the Faculty of Health Sciences at Ontario Tech University.
This study was supported by the College of Chiropractors of British Columbia to Ontario Tech University. The College of Chiropractors of British Columbia was not involved in the design, conduct or interpretation of the research that informed the research. This research was undertaken, in part, thanks to funding from the Canada Research Chairs program to Pierre Côté who holds the Canada Research Chair in Disability Prevention and Rehabilitation at Ontario Tech University, and funding from the Canadian Chiropractic Research Foundation to Carol Cancelliere who holds a Research Chair in Knowledge Translation in the Faculty of Health Sciences at Ontario Tech University.
I have often felt that chiropractic is similar to a cult. An investigation by cult members into the dealings of a cult is not the most productive of concepts, I guess.
This review provides published data on so-called alternative medicine (SCAM)-related liver injuries (DILI) in Asia, with detail on incidences, lists of most frequently implicated herbal remedies, along with analysis of patient population and their clinical outcomes.
Its authors conclude that SCAM use is widely prevalent in Asia and is associated with, among other adverse effects, hepatotoxicity. Both proprietary as well as non-proprietary or traditional SCAMs have been implicated in hepatotoxicity. Acute hepatocellular pattern of liver injury is the most common type of liver injury seen, and the spectrum of liver-related adverse events range from simple elevation of liver enzymes to the very serious ALF and ACLF, which may, at times, require liver transplant.
SCAM-related liver injury is one among the major causes for hepatotoxicity, including ALF and ACLF worldwide, with high incidence among Asian countries. Patient outcomes associated with SCAM-DILI are generally poor, with very high mortality rates in those with chronic liver disease. Stringent regulations, at par with that of conventional modern medicine, are required, and may help improve safety of patients seeking SCAM for their health needs. Regional surveillance including post-marketing analysis from government agencies associated with drug regulation and control in tandem with national as well as regional level hepatology societies are important for understanding the true prevalence of DILI associated with SCAM. An integrated approach used by practitioners combining conventional and traditional medicine to identify safety and efficacy of SCAMs is an unmet need in most of the Asian countries. Endorsement of scientific methodology with good quality preclinical and clinical trials and abolishment of unhealthy publication practices is an area that needs immediate attention in SCAM practice. Such holistic standard science-based approaches could help ameliorate liver disease burden in the general and patient population.
I congratulate the authors to this excellent paper. It contains a wealth of information and is well worth reading in full. The review will serve me as a valuable source of data for many years to come.
A systematic review of the evidence for effectiveness and harms of specific spinal manipulation therapy (SMT) techniques for infants, children and adolescents has been published by Dutch researchers. I find it important to stress from the outset that the authors are not affiliated with chiropractic institutions and thus free from such conflicts of interest.
They searched electronic databases up to December 2017. Controlled studies, describing primary SMT treatment in infants (<1 year) and children/adolescents (1–18 years), were included to determine effectiveness. Controlled and observational studies and case reports were included to examine harms. One author screened titles and abstracts and two authors independently screened the full text of potentially eligible studies for inclusion. Two authors assessed risk of bias of included studies and quality of the body of evidence using the GRADE methodology. Data were described according to PRISMA guidelines and CONSORT and TIDieR checklists. If appropriate, random-effects meta-analysis was performed.
Of the 1,236 identified studies, 26 studies were eligible. In all but 3 studies, the therapists were chiropractors. Infants and children/adolescents were treated for various (non-)musculoskeletal indications, hypothesized to be related to spinal joint dysfunction. Studies examining the same population, indication and treatment comparison were scarce. Due to very low quality evidence, it is uncertain whether gentle, low-velocity mobilizations reduce complaints in infants with colic or torticollis, and whether high-velocity, low-amplitude manipulations reduce complaints in children/adolescents with autism, asthma, nocturnal enuresis, headache or idiopathic scoliosis. Five case reports described severe harms after HVLA manipulations in 4 infants and one child. Mild, transient harms were reported after gentle spinal mobilizations in infants and children, and could be interpreted as side effect of treatment.
The authors concluded that, based on GRADE methodology, we found the evidence was of very low quality; this prevented us from drawing conclusions about the effectiveness of specific SMT techniques in infants, children and adolescents. Outcomes in the included studies were mostly parent or patient-reported; studies did not report on intermediate outcomes to assess the effectiveness of SMT techniques in relation to the hypothesized spinal dysfunction. Severe harms were relatively scarce, poorly described and likely to be associated with underlying missed pathology. Gentle, low-velocity spinal mobilizations seem to be a safe treatment technique in infants, children and adolescents. We encourage future research to describe effectiveness and safety of specific SMT techniques instead of SMT as a general treatment approach.
We have often noted that, in chiropractic trials, harms are often not mentioned (a fact that constitutes a violation of research ethics). This was again confirmed in the present review; only 4 of the controlled clinical trials reported such information. This means harms cannot be evaluated by reviewing such studies. One important strength of this review is that the authors realised this problem and thus included other research papers for assessing the risks of SMT. Consequently, they found considerable potential for harm and stress that under-reporting remains a serious issue.
Another problem with SMT papers is their often very poor methodological quality. The authors of the new review make this point very clearly and call for more rigorous research. On this blog, I have repeatedly shown that research by chiropractors resembles more a promotional exercise than science. If this field wants to ever go anywhere, if needs to adopt rigorous science and forget about its determination to advance the business of chiropractors.
I feel it is important to point out that all of this has been known for at least one decade (even though it has never been documented so scholarly as in this new review). In fact, when in 2008, my friend and co-author Simon Singh, published that chiropractors ‘happily promote bogus treatments’ for children, he was sued for libel. Since then, I have been legally challenged twice by chiropractors for my continued critical stance on chiropractic. So, essentially nothing has changed; I certainly do not see the will of leading chiropractic bodies to bring their house in order.
May I therefore once again suggest that chiropractors (and other spinal manipulators) across the world, instead of aggressing their critics, finally get their act together. Until we have conclusive data showing that SMT does more good than harm to kids, the right thing to do is this: BEHAVE LIKE ETHICAL HEALTHCARE PROFESSIONALS: BE HONEST ABOUT THE EVIDENCE, STOP MISLEADING PARENTS AND STOP TREATING THEIR CHILDREN!
Many cancer patients use so-called alternative medicine (SCAM) such as Traditional Chinese Medicine (TCM). On this blog, we have repeatedly discussed whether this does more good than harm. This study sheds new light on the question. Specifically, it aims to explore the benefits of TCM therapy in the long-term survival of patients with hepatocellular carcinoma in China.
In total, 3483 patients with HCC admitted to the Beijing Ditan Hospital of Capital Medical University were enrolled. The researchers used 1:1 frequency matching by sex, age, diagnosis time, Barcelona Clinic Liver Cancer staging, and type of treatments to compare the TCM users (n = 526) and non-TCM users (n = 526). A Cox multivariate regression model was employed to evaluate the effects of TCM therapy on the HR value and Kaplan-Meier survival curve for mortality risk in HCC patients. A log-rank test was performed to analyse the effect of TCM therapy on the survival time of HCC patients.
The Cox multivariate analysis indicated that TCM therapy was an independent protective factor for 5-year survival in patients with HCC. The Kaplan-Meier curve also showed that after PS matching, TCM users had a higher overall survival rate and a higher progression-free survival rate than non-TCM users. TCM users, regardless of the classification of etiology, tumor stage, liver function level, or type of treatment, all benefited significantly from TCM therapy. The most commonly used Chinese patent medications used were Fufang Banmao Capsule, Huaier Granule, and Jinlong Capsule.
The authors concluded that using traditional Chinese medications as adjuvant therapy can probably prolong median survival time and improve the overall survival among patients with HCC. Further scientific studies and clinical trials are needed to examine the efficiency and safety.
I was unable to access the full article and therefore am unable to provide a detailed critique of it. From reading the abstract, I should point out, however, that this was not an RCT. To minimise bias, the researchers used a matching technique to generate two comparable groups. Such methods can be successful in matching for the named parameters, but they cannot match for the plethora of variables that might be relevant but were not measured. Therefore, the survival difference between the two groups might be due not to the therapies they received, but to the fact that the groups were not comparable in terms of factors that impact on survival.
Another important point about this paper is the obvious fact that it originates from China. We know from several independent investigations that such studies almost never report negative findings. We also know that TCM is a hugely important export item for China. Adding two and two together should therefore make us sceptical. I for one take the present findings with more than a pinch of salt.
Glucosamine supplements are often advocated for the treatment of osteoarthritis. But there is evidence that they might convey other benefits as well. This prospective observational study assessed the association of habitual glucosamine use with risk of cardiovascular disease (CVD) events. The UK Biobank data of 466 039 participants without CVD at baseline was used. They completed a questionnaire on supplement use, which included glucosamine. These participants were enrolled from 2006 to 2010 and were followed up to 2016. The main outcome measures were incident CVD events, including CVD death, coronary heart disease, and stroke.
During a median follow-up of seven years, there were 10 204 incident CVD events, 3060 CVD deaths, 5745 coronary heart disease events, and 3263 stroke events. After adjustment for age, sex, body mass index, race, lifestyle factors, dietary intakes, drug use, and other supplement use, glucosamine use was associated with a significantly lower risk of total CVD events (hazard ratio 0.85, 95% confidence interval 0.80 to 0.90), CVD death (0.78, 0.70 to 0.87), coronary heart disease (0.82, 0.76 to 0.88), and stroke (0.91, 0.83 to 1.00).
The authors concluded that habitual use of glucosamine supplement to relieve osteoarthritis pain might also be related to lower risks of CVD events.
This is an impressive study! It incorporates both a huge sample size and a long observation period. Moreover, the authors analysed the data expertly and interpreted their results with the necessary caution.
The association between glucosamine intake and CVD risk were independent of CVD risk factors, such as gender, age, income, body mass index, physical activity, healthy diet, alcohol intake, smoking status, diabetes, hypertension, high cholesterol, arthritis, drug use, and other supplement use. Moreover, the findings are in line with several previous studies that show inverse associations of glucosamine use with CVD risk and mortality. And finally, the authors discuss several biologically plausible mechanisms that could explain the observed findings.
Yet, it is conceivable that the association is not of a causal nature. There might be a host of confounders responsible for the finding. Therefore, before we now all rush to the next health-food store to buy glucosamine supplements – they are not all that cheap! – we should perhaps wait for further independent replications and research.
Fibromyalgia (FM) is one of the most frequent generalized pain disorders. It accounts for a sizable proportion of healthcare costs. Despite extensive research, the etiology (the ‘root cause’) of FM remains unknown – except, of course, to SCAM practitioners!
Most types of SCAM are said to be effective for FM (while the evidence for such claims is less than solid).
And almost every one of them claims to treat the ‘root cause’ of the condition. Which must mean that they are able to tackle its etiology, usually some disturbance of the ‘vital force’ or ‘energy’ flow. To patients, this sadly sounds impressive.
But what, if the etiology of FM is something entirely different?
New research shows that most (if not all) patients with FM belong to a distinct population that can be segregated from a control group by their glycated haemoglobin A1c (HbA1c) levels, a surrogate marker of insulin resistance (IR). This was demonstrated by analysing the data after introducing an age stratification correction into a linear regression model. This strategy showed highly significant differences between FM patients and control subjects (p < 0.0001 and p = 0.0002, for two separate control populations, respectively).
A subgroup of FM patients meeting criteria for pre-diabetes or diabetes (patients with HbA1c values of 5.7% or greater) who had undergone treatment with metformin showed dramatic improvements of their widespread myofascial pain. This was shown comparing pre and post-treatment numerical pain rating scale (NPRS). Response to metformin plus standard treatment (ST) was followed by complete resolution of the pain (report of 0 of 10 in the NPRS) in 8 of 16 patients who had been treated with metformin (50%), a degree of improvement never observed before in such a large proportion of FM patients subjected to any available treatment. In contrast, patients treated with ST alone improved, but complete resolution of pain was generally not observed. Interestingly, some patients responded only to metformin and not to ST with NSRIs or membrane stabilizing agents. Importantly, there was a long-term retention of the analgesic effect of metformin.
The authors concluded that these findings suggest a pathogenetic relationship between FM and IR, which may lead to a radical paradigm shift in the management of this disorder.
From my perspective, these findings also suggest that all the many SCAMs allegedly claiming to tackle the ‘root cause’ of FM have been barking up the wrong tree. In fact, all these claims of SCAM practitioners about treating the ‘root causes’ can easily be disclosed as a simple (and sadly effective) marketing gimmick. Six years ago, I even challenged the world of SCAM to name a single treatment that treats the ‘root cause’ of any disease. As yet, nobody has come forward with a convincing suggestion.
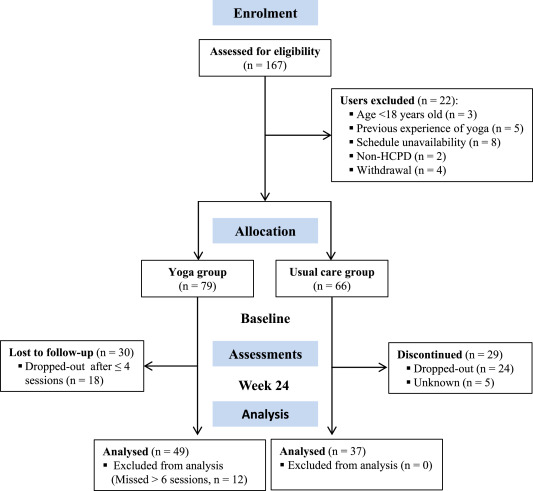
A recent blog-post pointed out that the usefulness of yoga in primary care is doubtful. Now we have new data to shed some light on this issue.
The new paper reports a ‘prospective, longitudinal, quasi-experimental study‘. Yoga group (n= 49) underwent 24-weeks program of one-hour yoga sessions. The control group had no yoga.
Participation was voluntary and the enrolment strategy was based on invitations by health professionals and advertising in the community (e.g., local newspaper, health unit website and posters). Users willing to participate were invited to complete a registration form to verify eligibility criteria.
The endpoints of the study were:
- quality of life,
- psychological distress,
- satisfaction level,
- adherence rate.
The yoga routine consisted of breathing exercises, progressive articular and myofascial warming-up, followed by surya namascar (sun salutation sequence; adapted to the physical condition of each participant), alignment exercises, and postural awareness. Practice also included soft twists of the spine, reversed and balance postures, as well as concentration exercises. During the sessions, the instructor discussed some ethical guidelines of yoga, as for example, non-violence (ahimsa) and truthfulness (satya), to allow the participant to have a safer and integrated practice. In addition, the participants were encouraged to develop their awareness of the present moment and their body sensations, through a continuous process of self-consciousness, keeping a distance between body sensations and the emotional experience. The instructor emphasized the connection between breathing and movement. Each session ended with a guided deep relaxation (yoga nidra; 5–10 min), followed by a meditation practice (5–10 min).
The results of the study showed that the patients in the yoga group experienced a significant improvement in all domains of quality of life and a reduction of psychological distress. Linear regression analysis showed that yoga significantly improved psychological quality of life.
The authors concluded that yoga in primary care is feasible, safe and has a satisfactory adherence, as well as a positive effect on psychological quality of life of participants.
Are the authors’ conclusions correct?
I think not!
Here are some reasons for my judgement:
- The study was far to small to justify far-reaching conclusions about the safety and effectiveness of yoga.
- There were relatively high numbers of drop-outs, as seen in the graph above. Despite this fact, no intention to treat analysis was used.
- There was no randomisation, and therefore the two groups were probably not comparable.
- Participants of the experimental group chose to have yoga; their expectations thus influenced the outcomes.
- There was no attempt to control for placebo effects.
- The conclusion that yoga is safe would require a sample size that is several dimensions larger than 49.
In conclusion, this study fails to show that yoga has any value in primary care.
PS
Oh, I almost forgot: and yoga is also satanic, of course (just like reading Harry Potter!).
The objective of this ‘real world’ study was to evaluate the effectiveness of integrative medicine (IM) on patients with coronary artery disease (CAD) and investigate the prognostic factors of CAD in a real-world setting.
A total of 1,087 hospitalized patients with CAD from 4 hospitals in Beijing, China were consecutively selected between August 2011 and February 2012. The patients were assigned to two groups:
- Chinese medicine (CM) plus conventional treatment, i.e., IM therapy (IM group). IM therapy meant that the patients accepted the conventional treatment of Western medicine and the treatment of Chinese herbal medicine including herbal-based injection and Chinese patent medicine as well as decoction for at least 7 days in the hospital or 3 months out of the hospital.
- Conventional treatment alone (CT group).
The endpoint was a major cardiac event [MCE; including cardiac death, myocardial infarction (MI), and the need for revascularization].
A total of 1,040 patients finished the 2-year follow-up. Of them, 49.4% received IM therapy. During the 2-year follow-up, the total incidence of MCE was 11.3%. Most of the events involved revascularization (9.3%). Cardiac death/MI occurred in 3.0% of cases. For revascularization, logistic stepwise regression analysis revealed that age ⩾ 65 years [odds ratio (OR), 2.224], MI (OR, 2.561), diabetes mellitus (OR, 1.650), multi-vessel lesions (OR, 2.554), baseline high sensitivity C-reactive protein level ⩾ 3 mg/L (OR, 1.678), and moderate or severe anxiety/depression (OR, 1.849) were negative predictors (P<0.05); while anti-platelet agents (OR, 0.422), β-blockers (OR, 0.626), statins (OR, 0.318), and IM therapy (OR, 0.583) were protective predictors (P<0.05). For cardiac death/MI, age ⩾ 65 years (OR, 6.389) and heart failure (OR, 7.969) were negative predictors (P<0.05), while statin use (OR, 0.323) was a protective predictor (P<0.05) and IM therapy showed a beneficial tendency (OR, 0.587), although the difference was not statistically significant (P=0.218).
The authors concluded that in a real-world setting, for patients with CAD, IM therapy was associated with a decreased incidence of revascularization and showed a potential benefit in reducing the incidence of cardiac death or MI.
What the authors call ‘real world setting’ seems to be a synonym of ‘lousy science’, I fear. I am not aware of good evidence to show that herbal injections and concoctions are effective treatments for CAD, and this study can unfortunately not change this. In the methods section of the paper, we read that the treatment decisions were made by the responsible physicians without restriction. That means the two groups were far from comparable. In their discussion section, the authors state; we found that IM therapy was efficacious in clinical practice. I think that this statement is incorrect. All they have shown is that two groups of patients with similar diagnoses can differ in numerous ways, including clinical outcomes.
The lessons here are simple:
- In clinical trials, lack of randomisation (the only method to create reliably comparable groups) often leads to false results.
- Flawed research is currently being used by many proponents of SCAM (so-called alternative medicine) to mislead us about the value of SCAM.
- The integration of dubious treatments into routine care does not lead to better outcomes.
- Integrative medicine, as currently advocated by SCAM-proponents, is a nonsense.
Patients with rheumatoid arthritis (RA) have a higher risk of coronary heart disease (CHD). Despite good evidence for effectiveness, acupuncture is often advocated for RA, and it has not been reported to prevent CHD in patients with RA.
The authors of this analysis aimed to assess the risk of developing CHD in acupuncture-users and non-users of patients with RA. They identified 29,741 patients with newly diagnosed RA from January 1997 to December 2010 from the Registry of Catastrophic Illness Patients Database from the Taiwanese National Health Insurance Research Database. Among them, 10,199 patients received acupuncture (acupuncture users), and 19,542 patients did not receive acupuncture (no-acupuncture users). After performing 1:1 propensity score matching by sex, age, baseline comorbidity, conventional treatment, initial diagnostic year, and index year, there were 9932 patients in both the acupuncture and no-acupuncture cohorts. The main outcome was the diagnosis of CHD in patients with RA in the acupuncture and no-acupuncture cohorts.
Acupuncture users had a lower incidence of CHD than non-users (adjusted HR = 0.60, 95% CI = 0.55-0.65). The estimated cumulative incidence of CHD was significantly lower in the acupuncture cohort (log-rank test, p < .001). Subgroup analysis showed that patients receiving manual acupuncture of traditional Chinese medicine style, electroacupuncture, or combination of both all had a lower incidence of CHD than patients never receiving acupuncture treatment. The beneficial effect of acupuncture on preventing CHD was independent of age, sex, diabetes mellitus, hypertension, hyperlipidemia, and statins use.
The authors concluded that this is the first large-scale study to reveal that acupuncture might have beneficial effect on reducing the risk of CHD in patients with RA. This study may provide useful information for clinical utilization and future studies.
Pigs might fly, but – call me a sceptic – I somehow doubt it almost as much as I doubt that acupuncture might have beneficial effect on reducing the risk of CHD.
Why?
Because of two reasons mainly:
- For the life of me, I cannot see a mechanism by which acupuncture achieves this extraordinary feast (the authors allege an anti-inflammatory effect of acupuncture which I find wholly unconvincing).
- There is a much simpler explanation for the observed outcomes.
The propensity score used here did, of course, only match the groups for a hand-full of factors. Yet there are many more that could play a part which the authors could not consider because they did not have the data to do so. The one that foremost comes to my mind is a generally healthier life-style of the patients using acupuncture. I think it stands to reason that people who bother to have and pay for an additional treatment are higher motivated to adhere to a life-style (e. g. smoking-cessation, exercise, nutrition, stress) that reduces the CHD-risk. And the influence of this factor could be very significant indeed. As the devil’s advocate, I could therefore even postulate that acupuncture itself had a slightly detrimental effect which, however, was over-ridden by the massive effect of the healthier life-style.
And the lesson to learn from all this?
Before we conclude about ‘beneficial effects’ of acupuncture or any other therapy, we need RCTs that effectively eliminate these rather obvious confounders.
 The notion that ‘chiropractic adds years to your life’ is often touted, particularly of course by chiropractors (in case you doubt it, please do a quick google search). It is logical to assume that chiropractors themselves are the best informed about what they perceive as the health benefits of chiropractic care. Chiropractors would therefore be most likely to receive some level of this ‘life-prolonging’ chiropractic care on a long-term basis. If that is so, then chiropractors themselves should demonstrate longer life spans than the general population.
The notion that ‘chiropractic adds years to your life’ is often touted, particularly of course by chiropractors (in case you doubt it, please do a quick google search). It is logical to assume that chiropractors themselves are the best informed about what they perceive as the health benefits of chiropractic care. Chiropractors would therefore be most likely to receive some level of this ‘life-prolonging’ chiropractic care on a long-term basis. If that is so, then chiropractors themselves should demonstrate longer life spans than the general population.
Sounds logical?
Perhaps, but is the theory supported by evidence?
Back in 2004, a chiropractor, Lon Morgan, courageously tried to test the theory and published an interesting paper about it.
He used two separate data sources to examine the mortality rates of chiropractors. One source used obituary notices from past issues of Dynamic Chiropractic from 1990 to mid-2003. The second source used biographies from Who Was Who in Chiropractic – A Necrology covering a ten year period from 1969-1979. The two sources yielded a mean age at death for chiropractors of 73.4 and 74.2 years respectively. The mean ages at death of chiropractors is below the national average of 76.9 years; it also is below the average age at death of their medical doctor counterparts which, at the time, was 81.5.
So, one might be tempted to conclude that ‘chiropractic substracts years from your life’. I know, this would be not very scientific – but it would probably be more evidence-based than the marketing gimmick of so many chiropractors trying to promote their trade by saying: ‘chiropractic adds years to your life’!
In any case, Morgan, the author of the paper, concluded that this paper assumes chiropractors should, more than any other group, be able to demonstrate the health and longevity benefits of chiropractic care. The chiropractic mortality data presented in this study, while limited, do not support the notion that chiropractic care “Adds Years to Life …”, and it fact shows male chiropractors have shorter life spans than their medical doctor counterparts and even the general male population. Further study is recommended to discover what factors might contribute to lowered chiropractic longevity.
Another beautiful theory killed by an ugly fact!