case-control study
The well-known Dr. Chris van Tulleken recently joined forces with Professor Michael Heinrich and Dr. Anthony Booker from the University College London School of Pharmacy to test a range of herbal products on sale in the UK. They bought over 70 herbal products from various high street stores and internet retailers. Some of the products were ‘THR’ (traditional herbal registration) herbal medicines, and some were marketed as food supplements. They then analyzed their chemistry to see whether each one really contained what the label says. The three popular herbal remedies we tested were:-
- Milk thistle (Silybum marianum),
- Ginkgo (Ginkgo biloba),
- Evening primrose (Oenothera).
The team at UCL used two different methods of analysis to verify the identity of these herbal products and extracts. High-performance thin-layer chromatography (HPTLC) is a sophisticated technique for the analysis of herbal products and is one of the most commonly used methods in the industry. HPTLC analysis creates a chemical fingerprint of the product which the researchers can then compare to an accepted reference standard for the herb. They look for a broad spectrum of ‘marker compounds’ these are the pharmacologically active and/or chemical constituents within a plant that can be used to verify its potency or identity. For complex samples or where additional confirmation is required, researchers often turn to ¹H nuclear magnetic resonance spectroscopy (¹H-NMR) which allows individual samples to be compared in detail against other samples or to the whole group.
In every THR product tested, the product contained what was claimed on the label. However, the food supplements showed a wide range of quality.
- Of the food supplement products labeled as Ginkgo, 8 out of 30 (27%) contained little or no ginkgo extract.
- 36% of the food supplement milk thistle products contained no detectable milk thistle. Although this is quite a small sample size it is still a startling result. Furthermore, in one case of milk thistle, unidentified adulterants suspected to be synthetic compounds were present in place of milk thistle.
- All of the evening primrose food products we tested did contain what the packet claimed.
The researchers concluded that their investigation shows that a regulatory system for herbal products, like the THR scheme, ensures that people have access to safe herbal medicine products. So, if you are considering buying herbal products then do look out for the THR mark– otherwise, you might not just be wasting your money, you might be consuming other, potentially dangerous, ingredients.
_______________________________
This is an interesting investigation. The researchers should be commended for it! However, I disagree with some of their conclusions. Here is why:
- The investigation merely tested the quality of the products and NOT THEIR SAFETY! To claim that the THR ensures access to safe herbal medicines is incorrect. A product might be of adequate quality but can still be unsafe. The THR only implies safety because the herbal has been used for years without problems being noted. This is not the same as ensuring that it is safe. A direct test of safety is usually not available.
- The recommendation to buy a product with a THR mark is also somewhat misleading. It implies that these products are effective. I fail to see convincing evidence that either MILK THISTLE, GINKGO, or EVENING PRIMROSE are effective for any disease or condition. Thus the responsible recommendation should, in my view, be to NOT buy them regardless of whether they are of good quality or not.
Imagine you have caught a cold. You think it is not necessary to see a doctor, but you want to take something that helps your body to get better. What is your choice of remedy? There are many options provided by conventional medicine as well as by so-called alternative medicine (SCAM).
Many people opt for SCAM to address health issues or prevent diseases. Yet, the evidence for SCAMs is either lacking or controversial due to methodological weaknesses. Thus, practitioners and patients primarily rely on subjective references rather than credible evidence from systematic research.
This study investigated whether cognitive and personality factors explain the differences in belief in SCAM and homeopathy. The researchers investigated the robustness of 21 predictors when examined together to obtain insights into some key determinants of such beliefs in a sample of 599 participants (60% female, 18-81 years). A combination of predictors explained 20% of the variance in SCAM belief. These predictors were:
- ontological confusions,
- spiritual epistemology,
- agreeableness,
- death anxiety,
- gender.
Approximately 21% of the variance in belief in homeopathy was explained by the following predictors:
- ontological confusions,
- illusory pattern perception,
- need for cognitive closure,
- need for cognition,
- honesty-humility,
- death anxiety,
- gender,
- age.
The authors concluded that some of the predictors from previous research replicated whereas others did not. Demographics and certain cognitive variables seem to be key determinants associated with beliefs in SCAM and homeopathy. Those individual differences and cognitive biases might result in a different perception of the world. However, variables related to abilities did not predict the beliefs. Thus, they might not be a result of inability but rather of ignorance.
Previous studies have shown that SCAM believers tend to believe in paranormal phenomena and conspiracies. I think that, in the discussion sections of this blog, we have ample evidence for this to be true. Paranormal beliefs are usually built on a magical worldview without reasoned review, which is shared by SCAM proponents. Such beliefs advocate emotional criteria for truth instead of data and logical considerations. Another belief, namely spirituality, is closely related to paranormal beliefs and religiosity and also associated with being a SCAM user. Lindeman found that SCAM belief could be best explained by intuitive reasoning, paranormal beliefs, and ontological confusions, defined as category mistakes in which properties of living and lifeless entities are mixed.
The authors point out that their results do not replicate previous findings that showed predictive value of certain cognitive variables such as cognitive style. An explanation could be that rather inattention to accuracy than the inability to consider empirical evidence fosters the beliefs. People might simply not be aware of the absence of evidence. Another possibility is that people are aware of the absence of evidence but are reluctant to engage with it. Practitioners and patients often claim “whatever works is good” or “the main thing is that it works”. Thus, it is ignorance rather than a lack of capacity to appropriately process the evidence.
The authors of this study are well aware of the limitations of their research:
“As with most cross-sectional studies using questionnaires, our results are based on self-reports. Additionally, single items were used for measuring belief strength. Even if multi-item measures often have advantages, single items can be advantageous in terms of practical benefits, e.g., adapting to subjects’ limited attention and time resources. There are several single item measures successfully used to measure diverse concepts including attitudes. Also, the variance on those items in our sample shows that participants were able to reflect their beliefs and rank them on the scale provided. Another limitation is that the findings are based on regression analyses, which do not provide insight into causality. Thus, the relationship remains correlational. Even if our sample was broader than in many other psychological studies—it was slightly unbalanced, especially in comparison to the German population. It over-represented educated individuals which may lead to an inadequate variation of the cognitive variables if we consider the relationship between cognition and education. However, education and the cognitive variables are only weakly correlated. Thus, it can be assumed that the unbalanced sample did not affect the distribution of cognitive variables to a great extent.”
The ‘keto diet’ is a currently popular high-fat, low-carbohydrate diet; it limits the intake of glucose which results in the production of ketones by the liver and their uptake as an alternative energy source by the brain. It is said to be an effective treatment for intractable epilepsy. In addition, it is being promoted as a so-called alternative medicine (SCAM) for a wide range of conditions, including:
- weight loss,
- cognitive and memory enhancement,
- type II diabetes,
- cancer,
- neurological and psychiatric disorders.
Now, it has been reported that the ‘keto diet’ may be linked to higher levels of cholesterol and double the risk of cardiovascular events. In the study, researchers defined a low-carb, high-fat (LCHF) diet as 45% of total daily calories coming from fat and 25% coming from carbohydrates. The study, which has so far not been peer-reviewed, was presented Sunday at the American College of Cardiology’s Annual Scientific Session Together With the World Congress of Cardiology.
“Our study rationale came from the fact that we would see patients in our cardiovascular prevention clinic with severe hypercholesterolemia following this diet,” said Dr. Iulia Iatan from the Healthy Heart Program Prevention Clinic, St. Paul’s Hospital, and University of British Columbia’s Centre for Heart Lung Innovation in Vancouver, Canada, during a presentation at the session. “This led us to wonder about the relationship between these low-carb, high-fat diets, lipid levels, and cardiovascular disease. And so, despite this, there’s limited data on this relationship.”
The researchers compared the diets of 305 people eating an LCHF diet with about 1,200 people eating a standard diet, using health information from the United Kingdom database UK Biobank, which followed people for at least a decade. They found that people on the LCHF diet had higher levels of low-density lipoprotein and apolipoprotein B. Apolipoprotein B is a protein that coats LDL cholesterol proteins and can predict heart disease better than elevated levels of LDL cholesterol can. The researchers also noticed that the LCHF diet participants’ total fat intake was higher in saturated fat and had double the consumption of animal sources (33%) compared to those in the control group (16%). “After an average of 11.8 years of follow-up – and after adjustment for other risk factors for heart disease, such as diabetes, high blood pressure, obesity, and smoking – people on an LCHF diet had more than two times higher risk of having several major cardiovascular events, such as blockages in the arteries that needed to be opened with stenting procedures, heart attack, stroke, and peripheral arterial disease.” Their press release also cautioned that their study “can only show an association between the diet and an increased risk for major cardiac events, not a causal relationship,” because it was an observational study, but their findings are worth further investigation, “especially when approximately 1 in 5 Americans report being on a low-carb, keto-like or full keto diet.”
I have to say that I find these findings not in the slightest bit surprising and would fully expect the relationship to be causal. The current craze for this diet is concerning and we need to warn consumers that they might be doing themselves considerable harm.
Other authors have recently pointed out that, within the first 6-12 months of initiating the keto diet, transient decreases in blood pressure, triglycerides, and glycosylated hemoglobin, as well as increases in HDL and weight loss may be observed. However, the aforementioned effects are generally not seen after 12 months of therapy. Despite the diet’s favorable effect on HDL-C, the concomitant increases in LDL-C and very-low-density lipoproteins (VLDL) may lead to increased cardiovascular risks. And another team of researchers has warned that “given often-temporary improvements, unfavorable effects on dietary intake, and inadequate data demonstrating long-term safety, for most individuals, the risks of ketogenic diets may outweigh the benefits.”
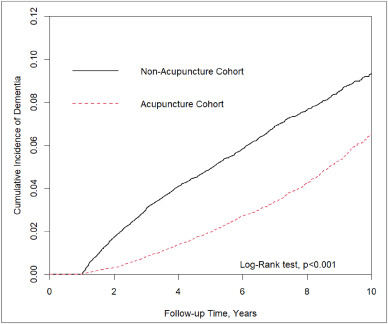
In this retrospective matched-cohort study, Chinese researchers investigated the association of acupuncture treatment for insomnia with the risk of dementia. They collected data from the National Health Insurance Research Database (NHIRD) of Taiwan to analyze the incidence of dementia in patients with insomnia who received acupuncture treatment.
The study included 152,585 patients, selected from the NHIRD, who were newly diagnosed with insomnia between 2000 and 2010. The follow-up period ranged from the index date to the date of dementia diagnosis, date of withdrawal from the insurance program, or December 31, 2013. A 1:1 propensity score method was used to match an equal number of patients (N = 18,782) in the acupuncture and non-acupuncture cohorts. The researchers employed Cox proportional hazards models to evaluate the risk of dementia. The cumulative incidence of dementia in both cohorts was estimated using the Kaplan–Meier method, and the difference between them was assessed through a log-rank test.
Patients with insomnia who received acupuncture treatment were observed to have a lower risk of dementia (adjusted hazard ratio = 0.54, 95% confidence interval = 0.50–0.60) than those who did not undergo acupuncture treatment. The cumulative incidence of dementia was significantly lower in the acupuncture cohort than in the non-acupuncture cohort (log-rank test, p < 0.001).
The researchers concluded that acupuncture treatment significantly reduced or slowed the development of dementia in patients with insomnia.
They could be correct, of course. But, then again, they might not be. Nobody can tell!
As many who are reading these lines know: CORRELATION IS NOT CAUSATION.
But if acupuncture was not the cause for the observed differences, what could it be? After all, the authors used clever statistics to make sure the two groups were comparable!
The problem here is, of course, that they can only make the groups comparable for variables that were measured. These were about 20 parameters mostly related to medication intake and concomitant diseases. This leaves a few hundred potentially relevant variables that were not quantified and could thus not be accounted for.
My bet would be lifestyle: it is conceivable that the acupuncture group had acupuncture because they were generally more health-conscious. Living a relatively healthy life might reduce the dementia risk entirely unrelated to acupuncture. According to Occam’s razor, this explanation is miles more likely that the one about acupuncture.
So, what this study really demonstrates or implies is, I think, this:
- The propensity score method can never be perfect in generating completely comparable groups.
- The JTCM publishes rubbish.
- Correlation is not causation.
- To establish causation in clinical medicine, RCTs are usually the best option.
- Occam’s razor can be useful when interpreting research findings.
This prospective study aimed to identify an optimal lifestyle profile to protect against memory loss in older individuals from areas representative of the north, south, and west of China. Individuals aged 60 years or older who had normal cognition and underwent apolipoprotein E (APOE) genotyping at baseline in 2009 were included. Participants were followed up until death, discontinuation, or 26 December 2019.
Six lifestyle factors were assessed:
- a healthy diet (adherence to the recommended intake of at least 7 of 12 eligible food items),
- regular physical exercise (≥150 min of moderate intensity or ≥75 min of vigorous intensity, per week),
- active social contact (≥twice per week),
- active cognitive activity (≥twice per week),
- never or previously smoked,
- never drinking alcohol.
Participants were categorised into the favourable group if they had 4-6 healthy lifestyle factors, into the average group for two to three factors, and into the unfavourable group for zero to one factor.
Memory function was assessed using the World Health Organization/University of California-Los Angeles Auditory Verbal Learning Test, and global cognition was assessed via the Mini-Mental State Examination. Linear mixed models were used to explore the impact of lifestyle factors on memory in the study sample.
A total of 29 072 participants were included (mean age of 72.23 years; 48.54% (n=14 113) were women; and 20.43% (n=5939) were APOE ε4 carriers). Over the 10-year follow-up period (2009-19), participants in the favourable group had slower memory decline than those in the unfavourable group (by 0.028 points/year, 95% confidence interval 0.023 to 0.032, P<0.001). APOE ε4 carriers with favourable (0.027, 95% confidence interval 0.023 to 0.031) and average (0.014, 0.010 to 0.019) lifestyles exhibited a slower memory decline than those with unfavourable lifestyles. Among people who were not carriers of APOE ε4, similar results were observed among participants in the favourable (0.029 points/year, 95% confidence interval 0.019 to 0.039) and average (0.019, 0.011 to 0.027) groups compared with those in the unfavourable group. APOE ε4 status and lifestyle profiles did not show a significant interaction effect on memory decline (P=0.52).
The authors concluded that a healthy lifestyle is associated with slower memory decline, even in the presence of the APOE ε4 allele. This study might offer important information to protect older adults against memory decline.
This is an important and meticulously reported study. It is the first large-scale investigation that assesses the effects of different lifestyle profiles, APOE ε4 status, and their interactions on longitudinal memory trajectories over a 10-year follow-up period. The results show that lifestyle is associated with the rate of memory decline in cognitively normal older individuals, including in people who are genetically susceptible to memory decline. The authors are rightly careful to avoid causal inferences between lifestyle and memory decline. To demonstrate causality beyond doubt, we would need different study designs.
The authors also discuss several weaknesses of the study:
- Firstly, the assessments of lifestyle factors were based on self-reports and are, therefore, prone to measurement errors.
- Secondly, several participants were excluded due to missing data or not returning for follow-up evaluations, which might have led to selection bias.
- Thirdly, the proportion of individuals with an unhealthy lifestyle might have been underestimated in the study because people with poor health were less likely to have participated in the study.
- Fourthly, given the nature of the study design, it could not assess whether maintaining a healthy lifestyle had already started influencing memory by the time of enrolment in the study.
- Fifthly, the evaluation of memory using a single neuropsychological test that does not comprehensively reflect overall memory function. However, the Auditory Verbal Learning Test is an effective instrument for memory assessment, and a composite score was used based on four Auditory Verbal Learning Test subscales to represent memory conditions to the greatest extent possible.
- Sixthly, as participants might become familiar with repeated cognitive testing, a learning effect could have influenced the results.
- Finally, memory decline was studied solely among older adults; however, memory problems commonly affect young individuals as well.
The authors, therefore, state that further studies should be conducted to facilitate a more extensive investigation into the effects of a healthy lifestyle on memory decline across the lifespan. This approach would help to elucidate the crucial age window during which a healthy lifestyle can exert the most favourable effect.
Migraines are common headache disorders and risk factors for subsequent strokes. Acupuncture has been widely used in the treatment of migraines; however, few studies have examined whether its use reduces the risk of strokes in migraineurs. This study explored the long-term effects of acupuncture treatment on stroke risk in migraineurs using national real-world data.
A team of Taiwanese researchers collected new migraine patients from the Taiwan National Health Insurance Research Database (NHIRD) from 1 January 2000 to 31 December 2017. Using 1:1 propensity-score matching, they assigned patients to either an acupuncture or non-acupuncture cohort and followed up until the end of 2018. The incidence of stroke in the two cohorts was compared using the Cox proportional hazards regression analysis. Each cohort was composed of 1354 newly diagnosed migraineurs with similar baseline characteristics. Compared with the non-acupuncture cohort, the acupuncture cohort had a significantly reduced risk of stroke (adjusted hazard ratio, 0.4; 95% confidence interval, 0.35–0.46). The Kaplan–Meier model showed a significantly lower cumulative incidence of stroke in migraine patients who received acupuncture during the 19-year follow-up (log-rank test, p < 0.001).

The authors concluded that acupuncture confers protective benefits on migraineurs by reducing the risk of stroke. Our results provide new insights for clinicians and public health experts.
After merely 10 minutes of critical analysis, ‘real-world data’ turn out to be real-bias data, I am afraid.
The first question to ask is, were the groups at all comparable? The answer is, NO; the acupuncture group had
- more young individuals;
- fewer laborers;
- fewer wealthy people;
- fewer people with coronary heart disease;
- fewer individuals with chronic kidney disease;
- fewer people with mental disorders;
- more individuals taking multiple medications.
And that are just the variables that were known to the researcher! There will be dozens that are unknown but might nevertheless impact on a stroke prognosis.
But let’s not be petty and let’s forget (for a minute) about all these inequalities that render the two groups difficult to compare. The potentially more important flaw in this study lies elsewhere.
Imagine a group of people who receive some extra medical attention – such as acupuncture – over a long period of time, administered by a kind and caring therapist; imagine you were one of them. Don’t you think that it is likely that, compared to other people who do not receive this attention, you might feel encouraged to look better after your health? Consequently, you might do more exercise, eat more healthily, smoke less, etc., etc. As a result of such behavioral changes, you would be less likely to suffer a stroke, never mind the acupuncture.
SIMPLE!
I am not saying that such studies are totally useless. What often renders them worthless or even dangerous is the fact that the authors are not more self-critical and don’t draw more cautious conclusions. In the present case, already the title of the article says it all:
Acupuncture Is Effective at Reducing the Risk of Stroke in Patients with Migraines: A Real-World, Large-Scale Cohort Study with 19-Years of Follow-Up
My advice to researchers of so-called alternative medicine (SCAM) and journal editors publishing their papers is this: get your act together, learn about the pitfalls of flawed science (most of my books might assist you in this process), and stop misleading the public. Do it sooner rather than later!
Chronic kidney disease is common, often progressive, and difficult to treat or prevent. Effective interventions would therefore be more than welcome. This paper explored the relation of habitual fish oil use with the risk of chronic kidney diseases (CKD).
A total of 408,023 participants (54.2% female) without prior CKD and with completed information regarding their consumption of major food groups and fish oil in the UK Biobank were enrolled. Fish oil use and dietary intakes were assessed by touch screen questionnaire and food frequency questionnaire, respectively. Incident CKD was recorded from hospital inpatient records.
At baseline, 128,843 (31.6%) participants reported taking fish oil supplements. During a median follow-up period of 12.0 years, a total of 10,782 (2.6%) participants developed CKD. With adjustments for important confounders, habitual fish oil use was associated with a significantly lower hazard of incident CKD (hazard ratio [HR], 0.90; 95% confidence interval [CI], 0.87-0.95), compared with non-use. Consistently, participants reporting ≥2 servings/week of oily fish (HR, 0.86; 95% CI, 0.79-0.94) and nonoily fish (HR, 0.86; 95% CI, 0.77-0.97) consumption had a lower hazard of incident CKD compared to those reporting no consumption ever. Additionally, among the 97,914 participants with data on plasma fatty acid, there were significant inverse relationships of plasma omega-3 polyunsaturated fatty acid (PUFA) (per SD increment, HR, 0.89, 95% CI, 0.84-0.94) and eicosatetraenoic acid (per SD increment, HR, 0.91, 95% CI, 0.87-0.96) with incident CKD.
The authors concluded that habitual fish oil use was associated with a lower hazard of CKD, which was further confirmed by the consistent inverse relations between fish consumption and circulating omega-3 PUFA concentration with incident CKD.
I like this paper! It shows in an exemplary fashion how to interpret an association between two variables: fish oil consumption does not necessarily CAUSE the lower risk, it is merely associated with it and there might be a number of non-causal explanations for the link. Whether there is a true cause-effect relationship needs to be investigated in further, differently designed studies. The present paper does not overstate its conclusions but it is nevertheless important, as it hopefully will prompt others to clarify the crucial issue of causality.
Wouldn’t it be nice, if researchers of so-called alternative medicine (SCAM) finally learned this simple lesson?
The impact of drug-induced liver injury (DILI) on patients with chronic liver disease (CLD) is unclear. There are few reports comparing DILI in CLD and non-CLD patients. In this study, the researchers aimed to determine the incidence and outcomes of DILI in patients with and without CLD.
They collected data on eligible individuals with suspected DILI between 2018 and 2020 who were evaluated systematically for other etiologies, causes, and the severity of DILI. They compared the causative agents, clinical features, and outcomes of DILI among subjects with and without CLD who were enrolled in the Thai Association for the Study of the Liver DILI registry. Subjects with definite, or highly likely DILI were included in the analysis.
The researchers evaluated the causal relationship between the clinical pattern of liver injury and the suspected drugs or SCAM products with the Roussel Uclaf Causality Assessment Method (RUCAM) system. RUCAM is a validated and established tool to quantitatively assess causality in cases of suspected DILI and/or SCAM product-induced liver injury. They also used the Clinical Assessment of Causality Scale to assess the association as definite (>95% likelihood), highly likely (75–95%), probable (50–74%), possible (25–49%) or unlikely (<25%).
A total of 200 subjects diagnosed with DILI were found in the registry. Of those, 41 had CLD and 159 had no evidence of CLD. So-called alternative medicine (SCAM) products were identified as the most common class of DILI agents. Approximately 59% of DILI in the CLD and 40% in non-CLD group were associated with SCAM use. Individuals with pre-existing CLD had similar severity including mortality. Twelve patients (6%) developed adverse outcomes related to DILI including seven (3.5%) deaths and five (2.5%) with liver failure. Mortality was 4.88% in CLD and 3.14% in non-CLD subjects over median periods of 58 (8-106) days and 22 (1-65) days, respectively.
The authors concluded that, in this liver disease registry, the causes, clinical presentation, and outcomes of DILI in subjects with CLD and without CLD patients were not different. Further study is required to confirm our findings.
Consumers often prefer SCAM to conventional medicine because SCAM is viewed as gentle and safe. The notions are that they
- are natural and therefore harmless;
- have been in use for ages and thus have stood the test of time.
Readers of this blog will appreciate that both notions are, in fact, fallacies:
- appeal to nature;
- appeal to tradition.
This new paper is an impressive reminder that SCAM’s reputation as a safe option is not justified, and that SCAM relies more on fallacies than on facts.
Gut microbiota can influence health through the microbiota–gut–brain axis. Meditation can positively impact the regulation of an individual’s physical and mental health. However, few studies have investigated fecal microbiota following long-term (several years) deep meditation. Therefore, this study tested the hypothesis that long-term meditation may regulate gut microbiota homeostasis and, in turn, affect physical and mental health.
To examine the intestinal flora, 16S rRNA gene sequencing was performed on fecal samples of 56 Tibetan Buddhist monks and neighboring residents. Based on the sequencing data, linear discriminant analysis effect size (LEfSe) was employed to identify differential intestinal microbial communities between the two groups. Phylogenetic Investigation of Communities by Reconstruction of Unobserved States (PICRUSt) analysis was used to predict the function of fecal microbiota. In addition, we evaluated biochemical indices in the plasma.
The α-diversity indices of the meditation and control groups differed significantly. At the genus level, Prevotella and Bacteroides were significantly enriched in the meditation group. According to the LEfSe analysis, two beneficial bacterial genera (Megamonas and Faecalibacterium) were significantly enriched in the meditation group. The functional predictive analysis further showed that several pathways—including glycan biosynthesis, metabolism, and lipopolysaccharide biosynthesis—were significantly enriched in the meditation group. Moreover, plasma levels of clinical risk factors were significantly decreased in the meditation group, including total cholesterol and apolipoprotein B.
The Chinese authors concluded that the intestinal microbiota composition was significantly altered in Buddhist monks practicing long-term meditation compared with that in locally recruited control subjects. Bacteria enriched in the meditation group at the genus level had a positive effect on human physical and mental health. This altered intestinal microbiota composition could reduce the risk of anxiety and depression and improve immune function in the body. The biochemical marker profile indicates that meditation may reduce the risk of cardiovascular diseases in psychosomatic medicine. These results suggest that long-term deep meditation may have a beneficial effect on gut microbiota, enabling the body to maintain an optimal state of health. This study provides new clues regarding the role of long-term deep meditation in regulating human intestinal flora, which may play a positive role in psychosomatic conditions and well-being.
This study is being mentioned on the BBC new-bulletins today – so I thought I have a look at it and check how solid it is. The most obvious question to ask is whether the researchers compared comparable samples.
The investigators collected a total of 128 samples. Subsequently, samples whose subjects had taken antibiotics and yogurt or samples of poor quality were excluded, resulting in 56 eligible samples. To achieve mind training, Tibetan Buddhist monks performed meditation practices of Samatha and Vipassana for at least 2 hours a day for 3–30 years (mean (SD) 18.94 (7.56) years). Samatha is the Buddhist practice of calm abiding, which steadies and concentrates the mind by resting the individual’s attention on a single object or mantra. Vipassana is an insightful meditation practice that enables one to enquire into the true nature of all phenomena. Hardly any information about the controls was provided.
This means that dozens of factors other than meditation could very easily be responsible for the observed differences; nutrition and lifestyle factors are obvious prime candidates. The fact that the authors fail to even discuss these possibilities and more than once imply a causal link between meditation and the observed outcomes is more than a little irritating, in my view. In fact, it amounts to very poor science.
I am dismayed that a respected journal published such an obviously flawed study without a critical comment and that the UK media lapped it up so naively.
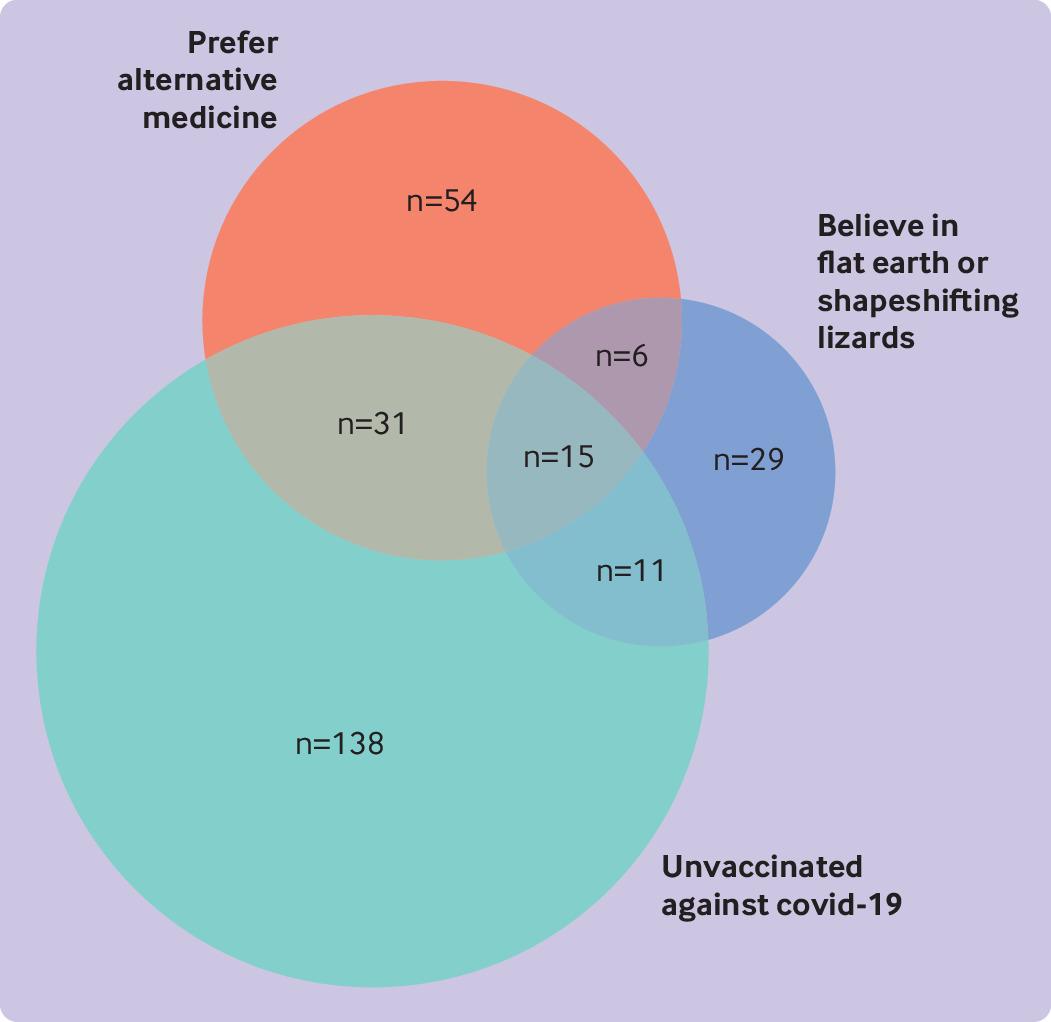
The objective of this cross-sectional survey was to evaluate the beliefs about and attitudes toward cancer prevention of people professing vaccination skepticism or conspiracy theories. Data were collected mainly from a well-known Spanish forum and other platforms, including Reddit (English), 4Chan (English), HispaChan (Spanish), and a Spanish-language website for cancer prevention (mejorsincancer.org) from January to March 2022.
Among 1494 responders, 209 were unvaccinated against covid-19, 112 preferred so-called alternative rather than conventional medicine, and 62 reported flat earth or reptilian beliefs. Cancer beliefs were assessed using the Cancer Awareness Measure (CAM) and Cancer Awareness Measure Mythical Causes Scale (CAM-MYCS), both validated tools.
Awareness of the actual causes of cancer was greater (median CAM score 63.6%) than that of mythical causes (41.7%). The most endorsed mythical causes of cancer were:
- eating food containing additives or sweeteners,
- feeling stressed,
- eating genetically modified food.
Awareness of the actual and mythical causes of cancer among the unvaccinated, alternative medicine, and conspiracy groups was lower than among their counterparts. A median of 54.5% of the actual causes was accurately identified among each of the unvaccinated, alternative medicine, and conspiracy groups, and a median of 63.6% was identified in each of the three corresponding counterparts (P=0.13, 0.04, and 0.003, respectively). For mythical causes, medians of 25.0%, 16.7%, and 16.7% were accurately identified in the unvaccinated, alternative medicine, and conspiracy groups, respectively; a median of 41.7% was identified in each of the three corresponding counterparts (P<0.001 in adjusted models for all comparisons).
In total, 673 (45.0%) participants agreed with the statement “It seems like everything causes cancer.” No significant differences were observed among the unvaccinated (44.0%), conspiracist (41.9%), or alternative medicine groups (35.7%), compared with their counterparts (45.2%, 45.7%, and 45.8%, respectively).

The authors’ conclusions were as follows: we evaluated the patterns of beliefs about cancer among people who believed in conspiracies, rejected the covid-19 vaccine, or preferred alternative medicine. We observed that the participants who belonged to these groups were more likely to endorse mythical causes of cancer than were their counterparts but were less likely to endorse the actual causes of cancer. Almost half of the participants, whether
conspiracists or not, agreed with the statement “It seems like everything causes cancer,” which highlights the difficulty that society encounters in differentiating actual causes of cancer from mythical causes owing to mass (veridical or not) information. This suggests a direct connection between digital misinformation and consequent potential erroneous health decisions, which may represent a further preventable fraction of cancer. Cultivating oriented medical education and scientific literacy, improving online ranking algorithms, building trust, and using effective health communication and social marketing campaigns may be possible ways to tackle this complex public health threat.
This is yet another study showing that so-called alternative medicine (SCAM) usage is linked to misinformation and conspiratorial thinking in other areas. We have discussed similar findings all too often. They are hardly surprising, in my view. As I have repeatedly been trying to point out:
- SCAM use is based mainly on misinformation
- And, to a large extent, SCAM is little more than a conspiracy theory in disguise.
The best way to prevent harm must therefore be to educate the public responsibly (which, of course, is one of the main aims of this blog.