Monthly Archives: May 2023
It has recently been reported that a 39-year-old woman (a mother-of-three died) died after immersing herself in a river as part of a cold water therapy session. The woman died after paramedics were called to attend a riverside in Derbyshire. The session was run by Kevin O’Neill of ‘Breatheolution’, whose previous clients include Coleen Rooney and actor Stephen Graham. The woman, who was visiting with two friends after paying up to £200 for a two-hour cold water therapy session, was rushed to hospital where she died.

Mr. O’Neill commented: “I am heartbroken. I’ve not slept and I’m finding it hard to process. I cannot stop thinking about her family. It’s tragic.” An inquest is expected to be opened into the woman’s death. East Midlands Ambulance Service said they were called to Bankside, in Bridgemont. “The caller reported a medical emergency,” a spokesperson said. “We sent a paramedic in a fast response car and a double-crewed ambulance. The air ambulance was also in attendance.”
Derbyshire Fire and Rescue Service, which was called to assist the paramedics, has warned people about the dangers of entering open water. “While we cannot and will not comment or speculate on the circumstances and cause of this tragic death, we would like to remind people of the dangers of entering open water and cold water shock,” said group manager Lee Williams.
_____________________
Breatheolution’ has a website where a whole page is dedicated to its leader Kevin O’Neill. I wondered what qualifications Kevin has, but all it tells us about him is this: “I struggled for so long with alcohol and other substance abuse that something had to give, I lost my sister Yvonne in 2019 and I think it was enough trauma to make me think a lot more about my own life”
The website also explains what the cold water sessions are about:
1-2-1 Breath Coaching, practice & Cold water session (river or tank)
2 hours @ £110.00
These sessions are proving popular with those who are not keen on group sessions or just prefer to have a more personal experience. The 2-3 hour sessions will be tailored to you and your breathing and will include potentially life-changing tools and methods to allow you to witness your breathing and physiology differently in the future, its all about feeling and awareness.
Another section of the site is dedicated to celebrities who Kevin seems to have treated. And then there is a video of the treatment. What I did not find anywhere, however, are the conditions that Kevin claims to treat with his cold water therapy.
In any case, it would have been wise for Kevin to read up about the risks of cold water immersion (CWI) before going into business. Perhaps this review would have helped:
In 2012, an estimated 372,000 people (42 per hour) died from immersion, assumed to be drowning. Immersion is the third leading cause of unintentional injury-related death, accounting for 7% of all such deaths (World Health Organization, 2014). These figures are underestimations owing to poor reporting in many Third World countries that have a high number of deaths. The data also do not include life-long morbidity caused by immersion-related injuries, estimated to be a much bigger numerical problem.
There is no strict definition of ‘cold water’. Given that some of the hazardous responses to cold water appear to peak on immersion somewhere between 15 and 10°C, it is reasonable to say that cold water is water <15°C (Tipton et al. 1991). However, the thermoneutral water temperature for a resting naked individual is ∼35°C, so it is possible for individuals to become very cold, with time, on immersion in water below this temperature. The corresponding temperature for those exercising (including shivering) is ∼25°C (Tipton & Golden, 1998).
Historically, the threat associated with CWI was regarded in terms of hypothermia or a reduction in deep body temperature below 35°C. This belief was established as a result of the Titanic disaster and supported by data obtained during maritime conflicts of World War II. However, more recently, a significant body of statistical, anecdotal and experimental evidence has pointed towards other causes of death on immersion. For example, in 1977 a Home Office Report revealed that ∼55% of the annual open water deaths in the UK occurred within 3 m of a safe refuge (42% within 2 m), and two-thirds of those who died were regarded as ‘good swimmers’. This evidence suggests more rapid incapacitation than can occur with whole-body cooling and consequent hypothermia.
The following four stages of immersion have been associated with particular risks (Golden & Hervey, 1981; Golden et al. 1991); the duration of these stages and the magnitude of the responses evoked within them vary significantly, depending on several factors, not least of which is water temperature:
- Initial immersion (first 3 min), skin cooling;
- Short-term immersion (3 min plus), superficial neuromuscular cooling;
- Long-term immersion (30 min plus), deep tissue cooling (hypothermia); and
- Circum-rescue collapse: immediately before, during or soon after rescue.
As a result of laboratory-based research, the initial responses to immersion, or ‘cold shock’, were identified as particularly hazardous (Tipton, 1989), accounting for the majority of immersion deaths (Tipton et al. 2014). These deaths have most often been ascribed to drowning, with the physiological responses of a gasp and uncontrollable hyperventilation, initiated by the dynamic response of the cutaneous cold receptors, resulting in the aspiration of the small volume of water necessary to initiate the drowning process (Bierens et al. 2016). Relatively little is known about the minimal rates of change of cold receptor temperature necessary to cause cold shock. The response has been reported to begin in water as warm as 25°C but is easy to suppress consciously at that temperature. In laboratory conditions, the respiratory frequency response (an indication of respiratory drive) peaks on naked immersion in a water temperature between 15 and 10°C, and is no greater on immersion in water at 5°C (Tipton et al. 1991). The corresponding average rates of change of chest skin temperature over the first 20 s of these immersions was 0.42 (water temperature 15°C), 0.56 (water temperature 10°C) and 0.68°C s−1 (water temperature 5°C). This suggests that an average rate of change in chest skin temperature between 0.42 and 0.56°C s−1 on the first 20 s of immersion is sufficient to evoke a maximal respiratory cold shock response.
More recently, it has been suggested (Shattock & Tipton, 2012) that a larger number of deaths than once thought may be attributable to arrhythmias initiated on immersion by the coincidental activation of the sympathetic and parasympathetic division of the autonomic nervous system by stimulation of cutaneous cold receptors around the body [sympathetic activation (cold shock)] and in the oronasal region on submersion or with wave splash [vagal stimulation (diving response)]. This ‘autonomic conflict’ is a very effective way of producing dysrhythmias and arrhythmias even in otherwise young and healthy individuals, particularly, but not necessarily, if a prolonged breath hold is involved in the immersion (Tipton et al. 1994). It seems that predisposing factors, such as long QT syndrome, ischaemic heart disease or myocardial hypertrophy, are necessary for fatal arrhythmias to evolve (Shattock & Tipton, 2012); many of these factors, including drug-induced long QT syndrome, are acquired. Non-fatal arrhythmias could still indirectly lead to death if they cause incapacitation and thereby drowning (Tipton, 2013). The hazardous responses associated with the cold shock response are presented in Fig. 2.
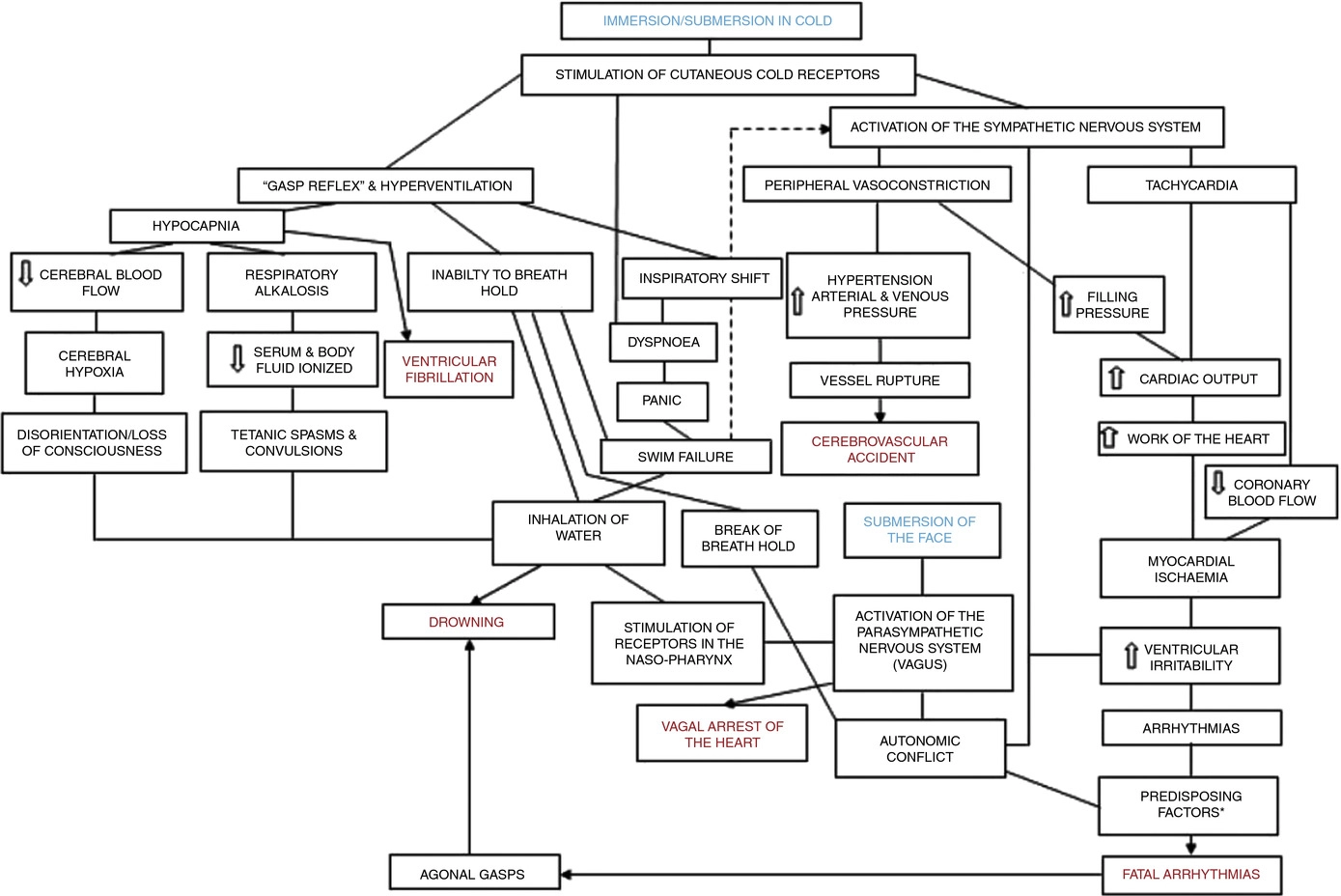
Figure 2. A contemporary view of the initial responses to immersion and submersion in cold water (‘cold shock’)
The problems encountered in short-term immersions are primarily related to physical incapacitation caused by neuromuscular cooling (Castellani & Tipton, 2015). The arms are particularly susceptible because of their high surface area to mass ratio. Low muscle temperatures affect chemical and physical processes at the cellular level. This includes metabolic rate, enzymatic activity, calcium and acetylcholine release and diffusion rate, as well as the series elastic components of connective tissues (Vincent & Tipton, 1988). Maximal dynamic strength, power output, jumping and sprinting performance are related to muscle temperature, with reductions ranging from 4 to 6% per degree Celsius reduction in muscle temperature down to 30°C (Bergh & Ekblom, 1979). At nerve temperatures below ∼20°C, nerve conduction is slowed and action potential amplitude is decreased (Douglas & Malcolm, 1955). Nerve block may occur after exposure to a local temperature of between 5 and 15°C for 1–15 min. This can lead to dysfunction that is equivalent to peripheral paralysis and can, again, result in drowning owing to the inability to keep the airway clear of the water (Clarke et al. 1958; Basbaum, 1973; Golden & Tipton, 2002; Fig. 3).

Figure 3. The ‘physiological pathways to drowning’ after immersion or submersion in cold water, with possible interventions for partial mitigation (dashed)
Abbreviations: EBA, emergency breathing aid; IS, immersion suit; and LJ, lifejacket. Reproduced with permission, from Tipton (2016b).
Even in ice-cold water, the possibility of hypothermia does not arise for at least 30 min in adults. Hypothermia affects cellular metabolism, blood flow and neural function. In severe hypothermia, the patient will be deeply unconscious. The progressive signs and symptoms (approximate deep body temperature) are shivering (36°C), confusion, disorientation, introversion (35°C), amnesia (34°C), cardiac arrhythmias (33°C), clouding of consciousness (33–30°C), loss of consciousness (30°C), ventricular fibrillation (28°C) and death (25°C) (Bierens et al. 2016). There is great variability between deep body temperature and the signs and symptoms of hypothermia. For example, although the deep body temperature associated with death is often quoted as 25°C, the lowest temperature recorded to date after accidental exposure to cold (air) and with full recovery was 12.7°C in a 28-month-old child (Associated Press, 2014). The coldest adult survivor of CWI followed by submersion had a body temperature of 13.7°C (Gilbert et al. 2000). There is also a large amount of variation in the rate at which people cool on immersion in cold water, owing to a combination of thermal factors (including water temperature and water movement, internal and external insulation) and non-thermal factors (including body size and composition, blood glucose, motion illness, racial and sex differences; Haight & Keatinge, 1973; Gale et al. 1981; White et al. 1992; Mekjavic et al. 2001; Golden & Tipton, 2002).
The most significant practical consequence of hypothermia in water is loss of consciousness; this prevents individuals from undertaking physical activity to maintain a clear airway and avoid drowning. Thus, once again, drowning is often the end-point (Fig. 3).
About 17% of those who die as a result of immersion die immediately before, during or after rescue (Golden et al. 1991). The deaths immediately before rescue are intriguing and probably related to behavioural changes at this time or the relief and psychophysiological alterations associated with imminent rescue, including a reduction in circulating stress hormone concentration and an increase in vagal tone. Death during rescue is most commonly associated with a collapse in arterial pressure when lifted vertical from the water and kept in that position for some time (Golden et al. 1991).
_____________________________
The tragic death of the woman should perhaps remind us that
- there is no SCAM or wellness treatment that is entirely harmless,
- and there are only few ‘would-be gurus’ who know what they are doing.
Richard Rasker has been one of our most loyal commentators with hundreds of sensible contributions to his credit. And now he has published a book! “This book”, he writes in his introduction, “is perhaps best described as a kind of travel guide for exploring different worlds, some of which are probably familiar, while others may be completely alien to you. Some of those worlds only exist in the minds of people, while others are very real indeed, yet often go unnoticed or have unexpected things to offer. This journey is also my personal exploration, during which I try to look through the eyes of the inhabitants of worlds that are wildly different from my own, to try and understand why those people believe certain things, and why I myself believe different things.”
Richard is not a medic, he is a man who understands science and empathizes with the many people who try to make sense of the often confusing concepts of healthcare. In his book, he takes the reader by the hand and carefully guides him or her through some of the issues that are of concern to so many of us. The journey takes us to so-called alternative medicine (SCAM) and beyond. At its end, the reader is wiser, more knowledgeable, and has learned the art of critical thinking.
Most chapters start with a story or anecdote that enables the reader to identify with the subject at hand. This serves the purpose of focusing the reader’s mind on the issue at hand which is then explained in full detail. The fact that Richard is not a medic turns out to be a strength of this book. Richard is not even tempted (as medics invariably are) to use jargon or to assume that the reader has prior knowledge of the subject. Instead, he starts from first principles and makes it impossible to get lost on the journey. What may seem complicated and confusing thus becomes clear and straightforward; what might have appeared to be dry and off-putting thus becomes lively and fascinating.
The range of topics that this book tackles is vast. It covers much of SCAM, of course. But it also includes topics that are way beyond SCAM, such as radiation and vaccination. In essence, the book deals with most things that people concerned about their health tend to worry about. Because Richard is a gifted writer who can render things simple without making them unduly simplistic, the book is a joy to read.
In my view, this book is a MUST-READ for anyone who wants to find his/her way safely through the maze of seemingly complex problems in healthcare.
‘Spagyric’ is a so-called alternative medicine (SCAM) based on the alchemy of Paracelsus (1493-1541). Paracelsus borrowed the term from “separate” (spao) and “combine” (ageiro) to indicate that spagyric preparations are based on the “separation”, “extraction” and “recombination” of the active ingredients of a substance. Plant, mineral as well as animal source materials are used.
The production of spagyric remedies is based on a complex process of maceration and fermentation of a plant extract in alcohol. It takes place in dark, thick-walled glass flasks that are hermetically sealed and kept at a controlled temperature of 37 °C for 28 days. The tincture thus obtained is then decanted and the drug residue is removed from the solution, completely dried, and burned to ash to recover the inorganic components of the plant material. The ash is subsequently dissolved in the alcoholic solution of maceration, and the finished spagyric preparation is left for 12 days before use.
Spagyric is not the most popular of all SCAMs but it certainly does have a significant following. One enthusiast claims that “spagyric essences work on a vibrational level in their action upon the emotional/mind and physical spheres and can be employed in numerous situations. Most people seek help to relieve physical symptoms. Even so, it is often necessary to address the emotional and psychological aspects which may predispose the illness or imbalance. In an era where many people are experiencing life-changing events, the ability to transition smoothly is essential for well-being and vitality. Guidance and help are required to maintain homeostasis. These medicines can help the patient to understand the root cause of their illness and learn to regain control of their lives. Some medicine systems appear to be less effective than in previous times. It has been suggested that the energetic frequency of both the earth and human organism are changing. Therefore these systems may no longer be a vibrational match for the changing frequencies. Spagyric Medicine is designed to ‘tune in with’ these current frequencies. Research suggests that the Spagyric essences may instigate improved health by energetically influencing DNA.”
After reading such weird statements, I ask myself, is there any evidence that spagyric remedies work? In my search for robust studies, I was unsuccessful. There does not seem to be a single controlled study on the subject. However, there are fragmentary reports of a study initiated and conducted by a now largely unknown healer named Karl Hann von Weyhern.
Von Weyhern (1882 – 1954) had taken a few semesters of pharmacy and medicine in Freiburg but remained without a degree. In 1930, he became a member of the NSDAP (Hitler’s Nazi party) and in 1940 he joined the SS. Around 1935, he settled in Munich as a non-medical practitioner (Heilpraktiker), and Heinrich Himmler who has a soft spot for SCAM enlisted as one of his patients. By then von Weyhern had by then made a steep career in the Nazi hierarchy, and he managed to convince Himmler that his spagyric remedies could cure tuberculosis, which was still rampant at the time. They decided to carry out experiments in this regard in the Dachau concentration camp.
Thus, von Weyhern was allowed to test spagyric remedies on forcibly recruited concentration camp prisoners. These experiments lasted for about one year and included around 150 patients who, according to von Weyhern’s iridology diagnosis, suffered from tuberculosis. Half of them were treated with spagyric remedies and the others with conventional treatments. At the end of the experiment, 27 persons were reportedly released into everyday concentration camp life as ‘fit for work’. How many of the 150 prisoners lost their lives due to these experiments is not known. Von Weyhern never filed a final report. It is to be feared that the death toll was considerable. [1]
After the war, von Weyhern denied belonging to the SS, claimed that he had ‘sacrificed himself’ for his patients in the concentration camp, merely had to pay a fine, and was ‘denazified’ in 1948. Subsequently, he resumed his work as a ‘Heilpraktiker’ in Olching, a village near Dachau. [1]
Of course, these infamous experiments cannot be blamed on spagyric medicine. Yet, I feel they are nevertheless important, not least because they seem to reveal the only thing remotely resembling something like evidence.
[1] Die Ärzte der Nazi-Führer: Karrieren und Netzwerke : Mathias Schmidt (Hg.), Dominik Groß (Hg.), Jens Westemeier (Hg.): Amazon.de: BooksA ‘manifesto’ is not something that I come across often in my area of research, i.e. so-called alternative medicine (SCAM). This one is in German, I, therefore, translated it for you:
Manifesto for healthy medicine
With the Manifesto for healthy medicine, we, the citizens and patients alliance weil’s hilft! (‘BECAUSE IT HELPS’) demand a fundamental change in our healthcare system, towards a diverse medicine that focuses on people and health. Be part of it! Sign the manifesto and become part of the movement.
It’s of paramount importance, the Manifesto for healthy medicine. About the way we live. It’s about our health. It’s about you and it’s about me.
We want our healthcare system to actually focus on health.
We want a medicine that doesn’t ask what’s missing, but what is possible.
We want a medicine that cares about people, that takes care, gets to the bottom of things, and uses innovative technologies to do so.
We want more bio, so that the chemistry is right, and we want naturopathic procedures and naturally effective medicines to be recognized, promoted, and researched further.
We want research that creates knowledge because, in addition to studies, it also takes into account the experience of physicians and the needs of patients.
We want carers and doctors to be able to work in a way that is good for their patients and for themselves.
We want people from all healthcare professions to work together as equals.
We want a medicine that creates awareness for a good and healthy life because climate protection also begins in one’s own body.
We want an integrative medicine that puts people at the center and self-evidently combines conventional and natural healing methods.
And we want this medicine to be accessible and affordable for everyone.
We fight for a healthy medicine of the future.
Be part of it!
(sorry, if some of it might sound badly translated but the German original is in parts pure gibberish)
_____________________
Who writes such tosh composed of every thinkable platitude and then pompously calls it a MANIFESTO?
BECAUSE IT HELPS! (weil’s hilft!) is a citizens’ movement that demands a change in the health care system – towards the needs and preferences of patients, towards a holistic view of people, and a focus on health instead of disease. The sensible combination of natural medicine and conventional medicine, an integrative medicine, makes an indispensable contribution to this. This is because it relies fully on the patients and involves them as active partners in the treatment. Modern medicine of the future, therefore, needs the equal cooperation of natural medicine and conventional medicine – in the everyday life of physicians and patients, in the reimbursement by the health insurance companies as well as in research and teaching.
On the information platform www.weils-hilft.de weil’s hilft! informs about current developments in integrative medicine, provides background information, and publishes a podcast once a month. The movement is also active on social media at www.facebook.com/weilshilft and www.instagram.com/weilshilft.
weil’s hilft! is supported by the health and patient organizations GESUNDHEIT AKTIV, KNEIPP-BUND, and NATUR UND MEDIZIN. Together, the alliance represents the interests of more than 220,000 people.
_______________________
One could easily disclose the funny side of this, the utter stupidity of the arguments, the platitudes, fallacies, misunderstandings, ignorance, etc. Yes, that would hardly be difficult. But it would ignore how worrying this and similar movements are. They systematically misinform consumers with the sole aim of persuading them that the integration of unproven or disproven treatments into medical routine is in their interest. Yet, if we only scratch the surface of their arguments, we realize that it is exclusively in the interest of those who profit from this type of misinformation.
There are debates in acupuncture-related systematic reviews and meta-analyses on whether searching Chinese databases to get more Chinese-language studies may increase the risk of bias and overestimate the effect size, and whether the treatment effects of acupuncture differ between Chinese and non-Chinese populations.
For this meta-epidemiological study, a team of investigators searched the Cochrane Library from its inception until December 2021, and identified systematic reviews and meta-analyses with acupuncture as one of the interventions. Paired reviewers independently screened the reviews and extracted the information. They repeated the meta-analysis of the selected outcomes to separately pool the results of Chinese- and non-Chinese-language acupuncture studies and presented the pooled estimates as odds ratios (OR) with 95% confidence interval (CI). They calculated the Ratio of ORs (ROR) by dividing the OR of the Chinese-language trials by the OR of the non-Chinese-language trials, and the ROR by dividing the OR of trials addressing Chinese population by the OR of trials addressing non-Chinese population. The researchers thus explored whether the impact of a high risk of bias on the effect size differed between studies published in Chinese- and in non-Chinese-language, and whether the treatment effects of acupuncture differed between Chinese and non-Chinese populations.
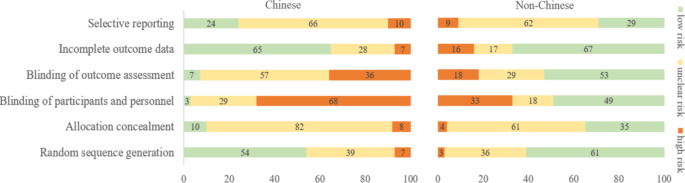
The researchers identified 84 Cochrane acupuncture reviews involving 33 Cochrane groups, of which 31 reviews (37%) searched Chinese databases. Searching versus not searching Chinese databases significantly increased the contribution of Chinese-language literature both to the total number of included trials (54% vs. 15%) and the sample size (40% vs. 15%). When compared with non-Chinese-language trials, Chinese-language trials were associated with a larger effect size (pooled ROR 0.51, 95% CI 0.29 to 0.91). The researchers also observed a higher risk of bias in Chinese-language trials in blinding of participants and personnel (97% vs. 51%) and blinding of outcome assessment (93% vs. 47%). The higher risk of bias was associated with a larger effect estimate in both Chinese language (allocation concealment: high/unclear risk vs. low risk, ROR 0.43, 95% CI 0.21 to 0.87) and non-Chinese-language studies (blinding of participants and personnel: high/unclear risk vs. low risk, ROR 0.41, 95% CI 0.23 to 0.74). However, the team found no evidence that the higher risk of bias would increase the effect size of acupuncture in Chinese-language studies more often than in non-Chinese-language studies (the confidence intervals of all ROR in the high-risk group included 1, Table 3). The researchers further found acupuncture appeared to be more effective in Chinese than in non-Chinese populations.

The authors concluded that the findings of this study suggest the higher risk of bias may lead to an overestimation of the treatment effects of acupuncture but would not increase the treatment effects in Chinese-language studies more often than in other language studies. The difference in treatment effects of acupuncture was probably associated with differences in population characteristics.
The authors discuss that, although searching Chinese databases can substantially increase the number of eligible studies and sample size in acupuncture reviews, the potentially higher risk of bias is an argument that needs to be considered in the inclusion of Chinese-language studies. Patients, investigators, and guideline panels should be cautious when adopting evidence from acupuncture reviews where studies with a high risk of bias contributed with a high weight to the meta-analysis.
The authors observed larger treatment effects of acupuncture in Chinese-language studies than in studies published in other languages. Although the treatment effects of acupuncture tended to be greater in studies with a high risk of bias, this potential overestimation did not differ between studies published in Chinese and in other languages. In other words, the larger treatment effects in Chinese-language studies cannot be explained by a high risk of bias. Furthermore, our study found acupuncture to be more effective in Chinese populations than in other populations, which could at least partly explain the larger treatment effects observed in Chinese-language studies.
I feel that this analysis obfuscates more than it clarifies. As we have discussed often here, acupuncture studies by Chinese researchers (regardless of what language they are published in) hardly ever report negative results, and their findings are often fabricated. It, therefore, is not surprising that their effect sizes are larger than those of other trials.
The only sensible conclusion from this messy and regrettable situation, in my view, is to be very cautious and exclude them from systematic reviews.
Traute Lafrenz Page was the last survivor of a non-violent resistance movement in Nazi Germany. On 6 March 2023, she died of natural causes at her farm in Yonges Island, S.C. aged 103.

Born Traute Lafrenz in Hamburg, Germany, Traute was a medical student in Munich when she became acquainted with other medical students like the Scholl siblings who opposed the Nazi regime. She and Hans Scholl were briefly romantically involved. Together they formed the Weisse Rose (White Rose). The students and one professor at the University of Munich (Willi Graf, Kurt Huber, Christoph Probst, Alexander Schmorell, Hans Scholl, and Sophie Scholl) began producing and distributing leaflets urging Germans to rise up in peaceful opposition to the Nazis. “Out of their readings of great writers evolved the initial idea about putting together these pamphlets that were focused on not only rebuking the Nazis but also invoking great names in literature and philosophy, and also rebuking the German people for not standing up,” Lafrenz Page’s daughter said.
Hans and Sophie Scholl, were arrested in 1943, convicted of high treason, and executed. Lafrenz Page attended their funerals and soon was arrested on charges of association. During her interrogation by the Gestapo, Lafrenz Page succeeded in disguising the full extent of her involvement in the distribution of leaflets. She was sentenced to serve a year in prison. After her release was arrested again by the Gestapo and faced trial in April 1945. Her life was spared as an advancing US Army liberated the prison just days before her trial was to begin.

Traute Lafrenz Page (Family photo)
“She knew the date of that trial for a long time, maybe even a year before it came up,” Lafrenz Page’s daughter said. “So what carried through the time of imprisonment and these experiences was the idea that the human spirit needed protection.”
After the war, Lafrenz Page completed her medical studies and moved to the US, where she served a medical residency in San Francisco and met her future husband, Vernon Page. He was an ophthalmologist who ran a medical practice in Hayfork, California, where she then practiced as a general practice physician. Traute hardly ever spoke about her involvement in the resistance against the Nazi regime and is quoted as saying; “Every complaint is forbidden in view of the fate of the others.”
Later, Lafrenz Page spent a year learning how to care for developmentally delayed children in Switzerland and became an enthusiast of Steiner’s anthroposophy. She began working as director of the Esperanza School in 1972. “She loved that work,” her daughter said. “On one level she just liked working with children, and on Marshfield, they also worked to address a child’s spirit, even if that child was handicapped or debilitated.”
In 2019, Lafrenz Page received the Order of Merit of the Federal Republic of Germany on the occasion of her 100th birthday. Her only Medline-listed article might provide some insight into her motivation in looking after disabled children:
This article examines the actions and testimonies of 14 nurses who killed psychiatric patients at the state hospital of Meseritz-Obrawalde in the Nazi ‘euthanasia’ program. The nurses provided various reasons for their decisions to participate in the killings. An ethical analysis of the testimonies demonstrates that a belief in the relief of suffering, the notion that the patients would ‘benefit’ from death, their selection by physicians for the ‘treatment’ of ‘euthanasia’, and a perceived duty to obey unquestioningly the orders of physicians were the primary ethical reasons that were stated for their behavior. However, 20 years had elapsed between the killings and the trial, thus giving ample opportunity for the defendants to develop comfortable rationales for their actions and for their attorneys to have observed successful defenses of others accused of euthanasia.
Exceptionally, this post is unrelated to so-called alternative medicine (SCAM). It addresses a new and worrisome development in UK healthcare. The UK has fewer doctors per population than most other developed countries. This shortage has now reached a level where it puts patients in danger. Recently, the government has unveiled a new NHS plan aimed to fix the problem.
The apprenticeship scheme could allow one in 10 doctors to start work without a traditional medical degree, straight after their A-levels. A third of nurses are also expected to be trained under the “radical new approach”. It is the centerpiece of a long-delayed NHS workforce strategy, following warnings that staff shortages in England could reach half a million without action to find new ways to train and recruit health workers. Amanda Pritchard, the head of NHS England, said: “This radical new approach could see tens of thousands of school-leavers becoming doctors and nurses or other key healthcare roles, after being trained on the job over the next 25 years.” She added that the plan offered a “once-in-a-generation opportunity to put the NHS on a sustainable footing”.
The “medical doctor degree apprenticeship” involves the same training and standards as traditional education routes, including a medical degree and all the requirements of the General Medical Council. Candidates will be expected to have similar A-levels as those for medical school, with qualifications in sciences, as well as options for graduates with non-medical degrees. The key difference behind such models is that apprentice medics would be available on the wards almost immediately, working under supervision, while being paid.
The medical degree apprenticeship is due to launch this autumn.
_______________________________
I am impressed!
Sadly, not in a positive way.
In fact, I cannot remember having ever heard of a more stupid idea for dealing with doctor shortages.
As incompetent amateurs, do the Tories really think that a similar level of incompetence might work also in healthcare?
Such shortages have happened before.
They are regrettable and need swift and firm action.
The only countermeasure that works is to train more doctors.
REAL DOCTORS!
The German Heilpraktiker (HP), a non-medically trained practitioner of so-called alternative medicine (SCAM), has repeatedly been the subject of my posts. In a nutshell: the profession was created by the Nazis and was originally destined to disappear within one generation. But this did not happen, and today there are ~100 000 HPs who are allowed to treat almost any condition without mandatory training or experience. Many HP schools exist but you can also become an HP without formal training.
Now a report has been published by undercover journalists investigating these HP schools in Germany. Here I have summarized a few crucial passages for you (if you read German, I strongly recommend reading the original article):
There are more than 150 HP schools in Germany. On average, training costs several thousand euros. There is no uniform and state regulation for the training. The curricula are mostly created by the schools themselves.
In addition to medical and psychological content, the schools often offer seminars that are not based on scientific knowledge. The curricula sometimes include courses such as astrology, homeopathy, or so-called quantum healing. HP organizations give indeed training guidelines. However, these are not met by about 83% of the schools.
The students were isolated at the HP school from their environment and urged to break off contact with their families. “Without us you are nothing. That came so often and I then, unfortunately, believed in it, because I was alone. If I had had no one else from school, then I would really have been completely alone,” explains a former student in an interview. “During that time, I also thought for the first time: Are we in some kind of cult here?
The school’s principal rejects the cult accusation: “We have been confronted with the allegation that we are a cult for some time and have always dealt with it very openly because we are not a cult. The principal also denies other accusations made by former students, saying that the allegations of suggestion, coercion, compulsion, or sweeping statements are simply false. He said he would be happy to face them “in a personal conversation outside the public eye to answer their questions.”
In order to get to the bottom of the treatment methods, the reporter also had herself treated by the principal of the school in an undercover self-experiment. In the first session, she determined that the reporter’s sciatica had been passed on to her by her mother, which is why she should sever her ties with her. In the second session, she recommended that she no longer visit her cancer-stricken grandfather. When the principal learned that the ill grandpa was of the zodiac sign Cancer, she concluded, “Cancer gets cancer.” The cancer, she said, was due to the fact that he had done nothing for his soul. And further, the patient runs the risk of adopting the grandfather’s cancer symptoms when she visits him.
The Hamburg health authority, which is listed as a “supervisory authority” on the school’s homepage, explains in response to an inquiry that no official supervision exists for HP schools. To obtain permission for opening a school, no training is necessary. Neither possible training courses nor institutions offering such training courses are regulated by the state.
The journalist also asked the Federal Health Ministry whether it sees the need for action and legal control. The Ministry’s response was evasive: “If necessary,” the HP law should be reformed in the future.
____________________
This is shocking news for many Germans who believe that HPs are well-trained healthcare professionals. However, those who have read my recently published book cannot be surprised. Poor training is only one of a myriad of deficits of HPs. It is time that the government realizes that the current is unacceptable and endangers public health. It is time, in other words, that the government does something about the HP profession.
How often do we hear that chiropractic is safe because numerous trials reported no adverse events? This systematic review tested whether there has been a change in the reporting of adverse events associated with spinal manipulation in randomized clinical trials (RCTs) since 2016.
Databases were searched from March 2016 to May 2022: MEDLINE (Ovid), Embase, CINAHL, ICL, PEDro, and Cochrane Library. Domains of interest (pertaining to adverse events) included: completeness and location of reporting; nomenclature and description; spinal location and practitioner delivering manipulation; methodological quality of the studies and details of the publishing journal. Frequencies and proportions of studies reporting on each of these domains were calculated. Univariable and multivariable logistic regression models were fitted to examine the effect of potential predictors on the likelihood of studies reporting on adverse events.
5399 records were identified by the electronic searches, of which 154 (2.9%) were included in the analysis. Of these, 94 (61.0%) reported adverse events with only 23.4% providing an explicit description of what constituted an adverse event. Reporting of adverse events in the abstract has increased (n=29, 30.9%) while reporting in the results section has decreased (n=83, 88.3%) over the past 6 years. Spinal manipulation was delivered to 7518 participants in the included studies. No serious adverse events were reported in any of these studies.
The authors concluded as follows: while the current level of reporting of adverse events associated with spinal manipulation in RCTs has increased since our 2016 publication on the same topic, the level remains low and inconsistent with established standards. As such, it is imperative for authors, journal editors and administrators of clinical trial registries to ensure there is more balanced reporting of both benefits and harms in RCTs involving spinal manipulation.
This article is clearly relevant to our discussions about adverse events after spinal manipulation. However, I find it far too uncritical. This might be due to the affiliations of some of the authors:
- Integrative Spinal Research Group, Department of Chiropractic Medicine, University Hospital Balgrist and University of Zurich, Zurich, Switzerland.
- Department of Chiropractic, Faculty of Medicine, Health and Human Sciences, Macquarie University, Sydney, New South Wales, Australia.
Interestingly, the authors stated that they have no conflict of interest. Also interesting is the fact that they do not cite our paper from 2012. I, therefore, take the liberty of doing it:
Objective: To systematically review the reporting of adverse effects in clinical trials of chiropractic manipulation.
Data sources: Six databases were searched from 2000 to July 2011. Randomised clinical trials (RCTs) were considered, if they tested chiropractic manipulations against any control intervention in human patients suffering from any type of clinical condition. The selection of studies, data extraction, and validation were performed independently by two reviewers.
Results: Sixty RCTs had been published. Twenty-nine RCTs did not mention adverse effects at all. Sixteen RCTs reported that no adverse effects had occurred. Complete information on incidence, severity, duration, frequency and method of reporting of adverse effects was included in only one RCT. Conflicts of interests were not mentioned by the majority of authors.
Conclusions: Adverse effects are poorly reported in recent RCTs of chiropractic manipulations.
In percentage terms the results are similar. What is very different is that the authors of the new paper merely lament that the level remains low and inconsistent with established standards, while we make it clear in the abstract that adverse effect reporting is poor and in the paper identify this deficit as a violation against research ethics and thus as a form of scientific misconduct.
In view of all this, let me re-phrase the last sentence of the authors’ conclusion:
it is imperative for authors, journal editors, and administrators of clinical trial registries to ensure that researchers adhere to accepted ethical standards and that scientific misconduct no longer gets published.
Following the death from cancer of a 14-year-old Carinthian girl, the Klagenfurt public prosecutor’s office has launched an investigation against the girl’s parents. In February this year, the 14-year-old was taken to a hospital in Graz, Austria, where she died a few days later from cancer. The hospital filed charges because the tumor had been treated incorrectly with so-called alternative medicine (SCAM).
Investigations are underway on suspicion of torturing or neglecting underage, younger, or defenseless persons. Currently, the accused and witnesses are being questioned. The parents’ lawyer, Alexander Todor-Kostic, stated that the accusations were without any basis and claimed that the 14-year-old girl had decided of her own free will against being treated with chemotherapy and surgery. The parents respected this, allowed her alternative treatment methods, and acted in accordance with the applicable legal situation.
The girl had developed cancer the previous year that was not detected. Instead of seeing conventional oncologists for a reliable diagnosis and effective treatments, the parents consulted private doctors. Instead of chemotherapy, radiation, and surgery, the girl had deliberately chosen “alternative treatments” herself, the lawyer stressed.
Even though the case has been reported in several Austrian papers, I did not succeed in finding further details about it. In particular, it is unclear what type of cancer the girl had been suffering from and what type of SCAMs she received.
The Austrian skeptic Christian Kreil commented: “Sugar pills in the pharmacies, homeopathic advanced training for doctors, a proliferation of energetics offering every conceivable bullshit … the dead girl is the logical result of this esoteric foolishness covered by politics and chambers.”
I am afraid that he might have a point here: as we have discussed repeatedly on this blog, Austria is currently particularly prone to misinformation about SCAM. Here are a few examples of previous blog posts on this subject:
- Austrian osteopaths seem to violate legal, ethical and moral rules and conventions
- An open letter to the President of the Austrian Medical Association aims to stop medical quackery
- Has the ‘Vienna Medical Association’ taken leave of its senses?
- When politicians become snake-oil salesmen
- Michael Frass’ research into homeopathy for cancer: “numerous breaches of scientific integrity”
- A well-known opponent of vaccination has died of COVID after self-treatment with MMS
- The case of a boy tortured to death with homeopathy
- A truly perplexing homeopath – is it time for an official investigation?
Misinformation about SCAM can be lethal. This is one of the reasons why responsible information is so very important.