This meta-analysis aimed “to provide better evidence of the efficacy of manual therapy (MT) on adolescent idiopathic scoliosis (AIS)”. 
All RCTs of MT for the management of patients with AIS were included in the present study. The treatment difference between the experimental and control group was mainly MT. The outcomes consisted of the total effective rate, the Cobb angle, and Scoliosis Research Society-22 (SRS-22) questionnaire score. Electronic database searches were conducted from database inception to July 2022, including the Cochrane Library, PubMed, Web of Science, Embase, Wanfang Data, CNKI, and VIP. The pooled data were analyzed using RevMan 5.4 software.
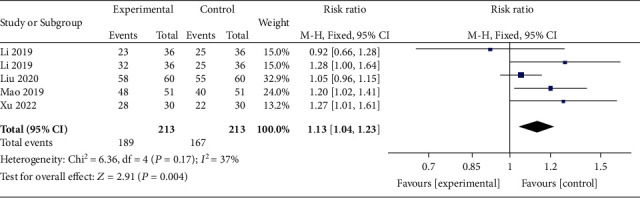
Four RCTs with 213 patients in the experimental groups were finally included. There are 2 studies of standalone MT in the experimental group and 3 studies of MT with identical conservative treatments in the control group. Three trials reported the total effective rate and a statistically significant difference was found (P = 0.004). Three trials reported Cobb angle; a statistical difference was found (P = 0.01). Then, sensitivity analysis showed that there was a significant difference in the additional MT subgroup (P < 0.00001) while not in the standalone MT subgroup (P = 0.41). Three trials reported SRS-22 scores (P = 0.55) without significant differences.
The authors concluded that there is insufficient data to determine the effectiveness of spinal manipulation limited by the very low quality of included studies. High-quality studies with appropriate design and follow-up periods are warranted to determine if MT may be beneficial as an adjunct therapy for AIS. Currently, there is no evidence to support spinal manipulation. 
The treatment of idiopathic scoliosis depends on the age, curve size, and progression of the condition. Therapeutic options include observation, bracing, physiotherapy, and surgery. They do NOT include MT because it is neither a plausible nor effective solution to this problem. It follows that further studies are not warranted and should be discouraged.
And, even if you disagree with me here and feel that further studies might be justified, let me remind you that proper research is never aimed at providing better evidence that a therapy works (as the authors of this odd paper seem to think); it must be aimed at testing whether it is effective!
There are studies showing that Scroth therapy for AIS is effective for smaller curves. Scroth is s specific targeted manual therapy.. No mention is made in this study of where the curves are- more than one – dextro or levo etc. These sort of studies are harmful as while it is possible to conclude mt is ineffective it discourages proper research into AIS which is a much overlooked condition causing huge deformity and pain
you probably mean Schroth therapy (https://www.hopkinsmedicine.org/health/conditions-and-diseases/scoliosis/schroth-method-for-scoliosis):
The Schroth Method is a nonsurgical option for scoliosis treatment. It uses exercises customized for each patient to return the curved spine to a more natural position. The goal of Schroth exercises is to de-rotate, elongate and stabilize the spine in a three-dimensional plane. This is achieved through physical therapy that focuses on:
Restoring muscular symmetry and alignment of posture
Breathing into the concave side of the body
Teaching you to be aware of your posture
This approach to scoliosis treatment was developed by Katharina Schroth and further popularized by her daughter Christa. Born in Germany in late 1800s, Katharina Schroth had scoliosis that was unsuccessfully treated with bracing. She developed her own breathing technique and exercises to manage her scoliosis. She and her daughter opened a clinic, where they treated more than 150 patients at a time.
Who claimed that Chrisa Schroth’s scoliosis “was unsuccessfully treated with bracing” ?
What is the evidenceis for that statement exactly?
(“Please remember: if you make a claim in a comment, support it with evidence.” Ernst. E.)
What might have been the progression of her scoliosis if she had not had bracing?
The general approach today is to have experts assess the rate of progression, and the age of the patient (not so old that growth has ceased), and a modest curve of <40degrees (in many experts opinion).
Then a surgical reduction and maintenance until skeletal maturity can be offered (e.g. with rods as depicted).
The rods could be taken out at two years – but why bother, unless complications ensue?
The force required to straighten a curve, even with surgical dissection and instrumentation, is considerable and no MT could possibly do it.
Breathing exercises are always helpful.
Nice try Katharina, and 'Burdle'.
I believe it was Katerina’s scoliosis that was unsuccessfully treated by bracing and it was she herself who said this.
I think you.misunderstand my point which was that Schroth has evidence of stopping curve progression. It us a luxury to stop progression,reducing is a bonus. Why would anyone bother with a study that wants to.prove mobilisation does not halt AIS. of course it can’t be expected to if it is just MT out of the box. Targeted therapy is what we need. And for anyone who thinks that bone fusion is a solution -;think again. In the short term it can straighten a spine. But down the line the spine degenerates bit by bit especially if the fusion extends below l2. It leaves the patient in pain and immobile. The spine was meant to move.
Furthermore the experts that you speak of do not in the main exists. Too.many orthos have incorrect info regarding scoliosis. We need more research but not meaningless research like this.
Guess what condition I have
.. ?
Dear ‘Burdle’,
I am sorry to hear you have scoliosis (I don’t need to guess, I’m a mindreader), and I wish you well.
I am intrigued by your statement that I “…misunderstand my point which was that Schroth has evidence of stopping curve progression.”
The anecdotal opinion of a single patient does not constitute evidence acceptable to the rational scientific community who take these things seriously.
‘Bone fusion’ does not ‘straighten a spine’. Who told you that?
Fusion holds in place a spine that has been straightened (e.g. by considerable force at open operation plus rods).
You are of course correct that over time all spines degenerate, and scoliosis surgeons most certainly have concerns that fixing some levels will add strain to others.
But at present, that is the best we can do.
Trust me, I’ve done scoliosis surgery, and seen many patients.
And believe me, if MT held any advantage – we’d all be in there like a shot.
If you think otherwise, your’re on the wrong blog site.
Take care.
Richard
The current surgery is called fusion surgery ? The vertebrae are ” pulled straight’ , fixed with pedicle screws and bone packed in to create one bony mass.
I am on this blog because
1. I am frustrated by chiros and dodgy therapists claiming to be able to straighten a spine with a simple manual therapy and in general.promote a pseudo science that actually harms people like me
2. I am frustrated by the lack of any real progress in scoliosis research which creates this vacuum where charlatans and anecdotal evidence can flourish.
3. I am frustrated that so.much stupid research like this exists that results in less meaningful research being performed.
In reply specifically to your opinion on fusion oncomment – I am frustrated that fusion surgery is still.promoted as being the gold standard when in fact no other solution exists. So it is a rock.and a hard place scenario. Surgeons claim that fusion surgery is successful if there if no pseudo arthroses and the hardware doesn’t break. They do not factor in pain. Patients down the line having pain and lack.of mobility from a fusion just get lumped in with another pt. With back.pain. I welcome the recent advances in VBT and ASC surgery- sadly not yet available on NHS but being performed in this country as well as worldwide
There is evidence showing Scroth as a targeted manual therapy for AIS is successful. Enough that our NHS is now allowing some physios to be trained.
The sooner we get scoliosis taken seriously so that narrative and understanding is consistent and that treatment is overseen by orthopaedic surgeons expert in the condition and not what I would call ‘ordinary’ othos the sooner we can get charlatans like chiros to.pack.up and go.
I know that this in anecdotal but I have letters to.prove – I am on the surgical list for a fusion for a progressive scoliosis ( which I am avoiding ) yet when I saw an orthopaedic for another matter in this crazy disjointed NHS I was told by an orthopaedic surgeon that nothing could be done as I am an adult and it won’t get any worse as I am fully grown.
I only mention this which is a bit off piste to emphasise the lack of a consistent understanding of scoliosis !
o
There’s been some interesting research on the possible role of the vestibular system.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8561148/
In my daughter’s case her scoliosis was due to her spina bifida. We ended up placing rods from T2-L2. No other option.
Again- we need a consistent narrative and understanding of Scoliosis. Neuromuscular and Syndromic scoliosis are different from AIS. As for that matter is Congenital scoliosis.
Referring as ‘Scoliosis’ is dangerous and confuses pathways of treatment!
So a SR/MA out of China that looked at 4 studies done in China.
“All RCTs of MT for the management of patients with AIS were included in the present study.”
“The present review collected a total of 4 RCTs published between 2019 and 2022 from China.”
that’s from the results section – they did not find any other studies but looked further that you seem to imply:
Electronic database searches were conducted from database inception to July 2022, including the Cochrane Library, PubMed, Web of Science, Embase, Wanfang Data, China National Knowledge Infrastructure (CNKI), and Chinese Scientific Journal Database (VIP). The combinations of MeSH Terms and relevant keywords were as follows: “Manual Therapy” (MeSH Terms) OR “Manipulation” OR “Massage” OR “Chiropractic” OR “Osteopathy” OR “Acupressure” OR “Myofascial release” OR “Tuina” OR “Shiatsu” OR “mobilization” AND “Scoliosis” (MeSH Terms) OR “Adolescent Idiopathic Scoliosis” OR “Spinal Curvatures” AND “Randomized Controlled Trial” (MeSH Terms). Also, the search strategy was determined for each database. In addition, the language was restricted to English or Chinese, with no limitation on subheadings. We searched reference lists of the identified papers to explore other studies, and trials not covered in the databases mentioned above were additionally searched once identified. Duplicate studies were deleted after reviewing the abstracts and full texts. This study mainly referred to the PRISMA 12 reporting guidelines for the meta-analysis of intervention trials [11].
We need to be absolutely clear what management means. Does it mean reducing curve, stopping progression or providing relief from pain ? Sufferers would take the latter 2
👉 1. Non-surgical interventions for adolescents with idiopathic scoliosis remain highly controversial.
2. Despite the publication of numerous reviews no explicit methodological evaluation of papers labeled as, […] is available.👈
Płaszewski M, Bettany-Saltikov J. Non-surgical interventions for adolescents with idiopathic scoliosis: an overview of systematic reviews. PLoS One. 2014 Oct 29;9(10):e110254. doi: 10.1371/journal.pone.0110254. PMID: 25353954; PMCID: PMC4213139.
I would recommend that you attend SpineWeek in Melbourne, Australia (May 1-5) and see and listen to what treatments are effective. The company ScoliCare whose CEO is a chiropractor is a leading innovator in spinal remodelling traction combined with bracing and muscle exercise. Spinal manipulation, either using an electromechanical percussive device or manual is an acceptable adjunctive therapy to what I listed above. https://www.sosort.org/
thank you – but I prefer evidence to advertising.
What a shame that I can find no plausible reproducible evidence that the treatments offered by this firm provide for any lasting benefit.
Michael: “Spinal manipulation, either using an electromechanical percussive device or manual is an acceptable adjunctive therapy to what I listed above.”
Acceptable to whom?
I hope that you can understand the statement of the abstract!
1. All “non-surgical interventions for adolescents with idiopathic scoliosis” are “controversial”.
2. No clear method for evaluating the numerous studies is described.
🙈 🙉 🙊
If you like it, you can also try the method of the former martial arts instructor Roland Liebscher-Bracht!
https://image.kurier.at/images/cfs_landscape_1864w_1049h/3507559/46-146279324.jpg
https://www.liebscher-bracht.com/schmerzlexikon/skoliose-fehlstellung-wirbelsaeule/
If it is ScoliSmart you refer to then then is no evidence other than their own manipulated evidence (carefully managed xray positioning ) to support their methods.
Furthermore wasn’t the ‘traction chair that they used actually found to increase a curve.
I dont belive chiro treatment is held in any esteem by scoliosis medical clinicians ?
Attendance at a conference is not a measure of acceptance – it could be to shoot you down ?
Dear Burdle,
I will reply to you!
You know “Application of the Schroth Method in the Treatment of Idiopathic Scoliosis: A Systematic Review and Meta-Analysis”?
https://doi.org/10.3390%2Fijerph192416730
In the meta-analysis by Vanja Dimitrijević, a total of 278 patients were examined. He cites two studies by Sanja Schreiber with a total of 100 patients, i.e. 36%.
But 💁
The results of the study were never (!) published! Really!
“No study results were published on ClinicalTrials.gov for this study”
https://clinicaltrials.gov/ct2/show/results/NCT01610908
Why, when such impressive results were achieved?
🙅 🙅♂️ 🙅♀️
https://pubmed.ncbi.nlm.nih.gov/36700244/
SOSORT – previously known a HARMS are a genuine not for profit organisation.
Up till now they have not included chiropractors
It is a shame you cannot attend. Nevertheless, I look forward to the publications coming out of SpineWeek. You may want to correspond with the SpineWeek committee member Dr Robert Gunzburg, Editor-in-Chief of the European Spine Journal on the importance of attending this multidisciplinary conference considering that for the first time includes chiropractic professional associations.
so, you are saying that to date there is no evidence?
While I agree with you Edzard in regards to Michael Epstein having a history of posting here to advertise, this time he has made a point.
SOSORT is a multidisciplinary international society with Ortho’s, MD’s, EP’s, Physio’s, Chiro’s etc.
Scolicare were the hosts for SOSORT during the recent Spine Week conference in Melbourne and ran their presentations and multidisciplinary workshops.
Spine Week involved many associations from all over the world – https://www.spineweek.org/societies/
Scolicare is a multidisciplinary clinic, works closely with doctors and ortho’s and the vast majority of their referrals comes from medico’s/specialists.
Jeb McIveney who founded Scolicare saw there was a need for scoliosis management prior to surgery and went to the US and Europe to work with the medical experts in bracing, exercises and rehab, then returned to Australia and founded Sciolicare. People post about the Schroth exercises and they have been around for a very long time, but what is new? There are the more recent SEAS exercises from Italy and advances in bracing and rehab. Scolicare integrate all of these, there was a void and they have filled it with best evidence from multiple professions. Their doing a good job and the doctors/orthos and using them.
@Richard Rawlins
There is a time and place for surgery.
Question is what should be done before surgery?
@Critical Chiro – You know full well that Scolicare , Scolismart and chriro who claim to treat scoliosis all claim that Surgery is not necessary if patients follow the therapy they offer?
Your claims that it is something that could complement surgery is disingenuous – These clinics scare their clients about surgery
@buurdle
I’ve visited Scolicare, referred patients to them, discussed/received reports about my patient’s care plans and received CC’d reports from the orthopedic/neuro surgeons they have subsequently referred the patient’s to for surgery.
“Your claims that it is something that could complement surgery is disingenuous – These clinics scare their clients about surgery”.
“disingenuous”
I do know full well how Scolicare operate.
Oh and BTW I also have referral relationships with the same orthopod’s and neurosurgeons so I get feedback on what they think of Scolicare.
When I look at the website for scolicare – there are no doctors – mainly chiropractors. The latter have for some tears now tried to fill a vacuum by claiming that their therapies, exercises etc can ‘cure’ a scoliosis. Newer surgical treatments have come along require earlier age intervention like VBT – this which rather scuppers the chiros. So they have to rely on scaremongering about surgery.
I am a big proponent of PSEAS but only if it is offered properly – part of a targeted approach by proper clinicians.
If you dispute what I am saying…take a look at Scolismart!!!
@Burdle
If you dispute what I’m saying take a closer look at Scolicare before before making generalizations.
Properly certified clinicians in SEAS, Schroth, bracing, use exercise physiologists, discusses surgical referral etc.
Scolicare work in a medical centre at St George General Hospital/Kogarah Private Hospital.
ZERO “Scaremongering” about surgery.
“I am a big proponent of SEAS but only if it is offered properly” – would you a Scolicare referral pad?
VBT (2019) look interesting:
“Vertebral body tethering is a surgical option for some children with idiopathic scoliosis whose spinal curves have not improved with bracing or who can not tolerate bracing.”
Also best for a subset of scoliosis.
So bracing (Soft/hybrid/rigid) and targeted exercises first.
Rather scuppers your statement.
Had a look at Scolismart who use soft braces and they recommend rigid bracing if soft don’t work.
If bracing and targeted exercises don’t work THEN surgery.
And even the surgeons say that surgery is always the last option.
Maybe that is why the majority of Scolicare’s referral are from medico’s.
I am not making generalizations my comment comes from actual personal experience.
If you would care to join Scolismart Facebook Page- I cannot as I and MANY other have been blocked for challenging what is claimed there which is:
1. the majority of patients who have spinal fusion end up disabled. All surgery is unnecessary
2. Scoliosis curves can be straightened by chiropractic
3. If they are not straightened then it is down to non-compliance on part of patients.
The reality is:
1. Small curves at a young age can benefit by PSEAS ( DOES NOT NEED TO BE GIVEN by CHIRO) Benefit is halting progression. This may well be your ‘referrals’
2 Bracing for curves over 40 degrees does not work- in that it does not halt progression- the best it will do is hold a spine until surgery.
3 There is a window of opportunity for VBT surgery which is when the spine is still growing and the tether does its work. This is for best effective outcome. VBT done after growth or ASC done on adult or inflexible curves can still be effective but the limited straightening is done at time of surgery. The Chiros from Scolismart openly deny this best window. Check St**zel out if you don’t believe me. Also ask him why he removes anyone who challenges from his facebook group??
4. I support PSEAS not because of spine straightening but because it is a targeted method of PHYSIOTHERAPHY that has evidence of arresting smaller curves and which can benefit those who have to live with the condition to ease muscles and help with pain I do not support the targeting of the vulnerable or the misrepresentation of treatment!
I too have the ear of Dr B and I know exactly what he thinks regarding chirpractic for scoliosis.