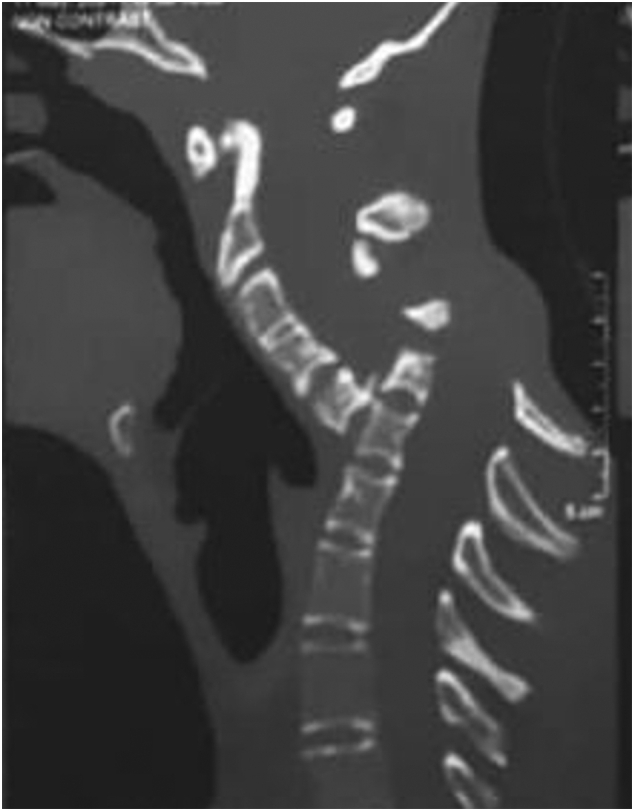
Spondyloptosis is a grade V spondylolisthesis – a vertebra having slipped so far with respect to the vertebra below that the two endplates are no longer congruent. It is usually seen in the lower lumbar spine but rarely can be seen in other spinal regions as well. Spondyloptosis is most commonly caused by trauma. It is defined as the dislocation of the spinal column in which the spondyloptotic vertebral body is either anteriorly or posteriorly displaced (>100%) on the adjacent vertebral body. Only a few cases of cervical spondyloptosis have been reported. The cervical cord injury in most patients is complete and irreversible. In most cases of cervical spondyloptosis, regardless of whether there is a neurologic deficit or not, reduction and stabilization of the fracture-dislocation is the management of choice
The case of a 16-year-old boy was reported who had been diagnosed with spondyloptosis of the cervical spine at the C5-6 level with a neurologic deficit following cervical manipulation by a traditional massage therapist. He could not move his upper and lower extremities, but the sensory and autonomic function was spared. The pre-operative American Spinal Cord Injury Association (ASIA) Score was B with SF-36 at 25%, and Karnofsky’s score was 40%. The patient was disabled and required special care and assistance.

The surgeons performed anterior decompression, cervical corpectomy at the level of C6 and lower part of C5, deformity correction, cage insertion, bone grafting, and stabilization with an anterior cervical plate. The patient’s objective functional score had increased after six months of follow-up and assessed objectively with the ASIA Impairment Scale (AIS) E or (excellent), an SF-36 score of 94%, and a Karnofsky score of 90%. The patient could carry on his regular activity with only minor signs or symptoms of the condition.
The authors concluded that this case report highlights severe complications following cervical manipulation, a summary of the clinical presentation, surgical treatment choices, and a review of the relevant literature. In addition, the sequential improvement of the patient’s functional outcome after surgical correction will be discussed.
This is a dramatic and interesting case. Looking at the above pre-operative CT scan, I am not sure how the patient could have survived. I am also not aware of previous similar cases. This does, however, not mean they don’t exist. Perhaps most affected patients simply died without being diagnosed. So, do we need to add spondyloptosis to the (hopefully) rare but severe complications of spinal manipulation?
the patient had a fall and hit his head 5 months prior to diagnosis could that cause the spondyloaptosis on its own? probably not
the patient had a cervical SMT by some kind of untrained therapist 4 months prior to diagnosis could that be the prime cause? probably not
the patient appears to have multiple Cafe au lait spots most indicative of neurofibromatosis type 1… he was undiagnosed and still not tested for it as far as we know. could that destabilize the cervical spine? probably YES
but please don’t let me trouble you with the complexity of clinical reality lets just say SMT caused the spondyloaptosis 🙂
did I say that SMT caused the spondyloaptosis?
did you miss the ‘?’ behind the last sentence?
perhaps an easy mistake when one is blinded by chiro zeal?
An interesting case. SMT by a massage person likely aggravated a pre-existing condition.
I did find this interesting:
“Two days following the cervical manipulation, the patient noticed weakness in his upper and lower extremities and had difficulty standing or walking. His parents initially brought him to a nearby hospital and got oral medication. After two months of therapy, the weakness was not improved, so the patient was referred to our hospital.”
Oral meds for these symptoms? No imaging? They scream red flags.
perhaps not the best hospital on the planet?
They say in the paper
But surely people would have noticed if a piece of his spine was sticking out that way before the massage therapist did things to him.
It sounds like he was unusually vulnerable, and then subjected to a violent manipulation which injured him very badly.
Poor guy 🙁
I note a tone of disbelief in the Professor’s post and I agree – in part.
Had I been asked to review these radiographs and the single CT slice shown in the article, I would have asked at first glance if the corpse had been buried yet. It does not seem to make sense that the boy was alive with a neck like this if this was due solely to trauma. On the side view there seems to be complete discontinuity of the spinal canal at the C5-6 level which would normally mean a total transection of the spinal cord IF this was an acute injury, which it obviously is not. There certainly is a dissociation/discontinuity of the vertebral column (spondyloptosis) that must have happened over an extended period, probably years. What I think saved this boy’s spinal cord was that part of his birth defect was a missing posterior wall of the spinal canal above C6 so the cord was not transected but moved posteriorly out of the canal as the cervical column (slowly over time), collapsed due to it not being normally built from birth. I am guessing the boy had a spina bifida occulta (look it up), i.e. the vertebral rings 5,4,3 at least, have not closed normally behind the cord during fetal development but also not bulged out like usually is seen in most bifid (split) spines. The authors touch on this on page 6 as an explanation of the incompleteness of cord compression but fail to explain it clearly. The birth defect has caused an instability of the column as the facet joints are probably missing or incomplete and did not support the columnar stability in the saggital plane and allowed it to slip over time but the open canal allowed this without causing more than partial compression of the cord as it had room to move out of the canal above the slip at C5-6.
Then along came some fool who started manhandling his neck and making things worse, which seems to have brought the boy to the attention of some smart surgeons who fixed his spine. The article is really about theway they saved him and the manipulation is only a sideline.
The appearance of the vertebral column, especially the upper part looks absolutely “funky” with some peculiar calcifications and deformed vertebral bodies indicating that this is absolutely not an acute injury. Apart of course from the extra damage done by the manipulator which demonstrates yet again the perils of manhandling necks, not the least aching oneks
I would have liked to see the whole CT study, at least some horisontal slices or even a 3D reconstruction af the bony parts that prabably can show all this much more clearly than is described in this, in my opinion, poorly written case presentation.
I want to emphasise that I am not a spinal surgeon or otherwise an expert in this field. I am only an old surgeon with quite extended experience in trauma who has studied more images of broken and injured necks treated more victims and cried silently over more corpses with broken necks than I care to remember.
One thing sounds incredible though, in this story. It is claimed that the patient was riding a bicycle six months after surgery!?! I was half inclined to call a bluff on this claim till proven wrong, but who knows? Life is also full of good things and small miracles actually happen, not seldom aided along by a good and smart ösurgeon, like in this case 🙂
There is so much that has to be assumed from this poorly written case report regarding the history and the role SMT probably played in this case. When dealing with such countries spinal manipulation can mean many different things. For example: https://www.youtube.com/watch?v=jNfG9rL2gi8
And what kind of training does a “massage therapist” in Indonesia have in doing “spinal manipulation”? I would think even a basic exam would have raised caution.
Anyway, Julian, my mom passed away this past weekend, thought you’d like to know. She went in her sleep.
DC,
I am sorry to hear this sad news. Although there can be an element of relief when a terminal illness ends, it does not make up for the loss of somebody who has been a part of your entire life. Please accept my condolences.
With Best Wishes,
Julian
Thank you. She battled her myelodysplasia for many years but she elected to stop the infusions. Her oncologist gave her 6 months, she made it 5. She did live long enough to celebrate her 65th wedding anniversary last month with dad.
Bjorn,
This is one of the most extraordinary CT images I have seen, and I was struggling to make sense of it until I read your comment describing a neural tube defect. My first thought was that it was a scan of someone who had been executed by hanging, though the classic gibbus wasn’t apparent. I also wondered about connective tissue disorders such as Ehrlers-Danlos syndrome. The patchy pigmentation could be relevant to an inherited condition; if the dark patches on the lower torso really are cafe-au-lait spots, then there are enough of them to be strongly suggestive of neurofibromatosis, as Dr Almog suggests, though possibly they could be islands in an extensive area of vitiligo. If that is the baseline skin colour, however, then the hyperpigmentation in the upper torso and neck needs to be explained.
It is such a strange case that I do wonder whether there is mroe than one underlying problem. Fascinating, but not really my area of expertise.
Yes Julian. I believe café au lait spots or even hairy patches overlying the spine may indicate underlying defects/abnormalities in the spinal column. As you probably also recall from the fascinating subject of embryology, the nervous system develops from the same structure in the embryo. This supposedly explains why skin abnormalities are found with many hereditary or developmental defects of the nervous system e.g. neurofibromatosis or dysraphism. Dysraphism is, I believe, the collective term for neural tube defects where the neural tube fails more or less to close in the back. Sometimes the spinal cord is exposed through a defect in the overlying skin and needs to be surgically repaired after birth. But in this patient the posterior arches and perhaps more structures of the vertebral bones seem to have failed to close and form properly in the neck even if the overlying skin has closed. This is absolutely not my field either but I am guessing he might also have defects lower in the spine, indicated by the strangely dark skin there?
I suppose that in a country of more than a billion people, you will find any imaginable oddity, even a youngster whose head almost fell off without quite killing him and the surgeons put it back on, so to speak, even after a masseur playing chiropractor had almost finished him off. 😳
“ Sometimes the spinal cord is exposed through a defect in the overlying skin and needs to be surgically repaired after birth. ”
This was the case with my daughter…spina bifida. We were fortunate to have an excellent surgeon. No shunt for her hydrocephalus.
https://physicians.wustl.edu/people/t-s-park-md/
He later did a cervical decompression in the upper cervical spine due to chiari. and a few surgeries for tethered cord and syrinx. Unfortunately, due to progressive scoliosis, she had to have spinal fusion from T2 thru L2. She hasn’t walked since the fusion but we have gotten her to stand with aides.
Was this after a rotational manipulation like a chiro would do or was it post a tradition “rubbing” massage?
We don’t know. In countries where there is little to no regulation it could be a variety of possible approaches. I think it’s safe to assume whomever did whatever didn’t know how to do a proper history and exam. Blame the person not the procedure.
There’s some kind of spinal manipulation in Balinese traditional medicine. But how it compares with what chiropractors do, and whether chiropractic manipulation might separate someone’s spine like this if they have a neural tube defect, and what exactly the traditional practitioner did to this boy, isn’t clear.
The message is simple. Don’t manipulate a hurting neck. It doesn’t help and it can do a lot of damage.
Bjorn:
The message is simple. Don’t manipulate a hurting neck. It doesn’t help and it can do a lot of damage.
Yes, cSMT can cause damage if done in the presence of contraindications or poorly performed.
Regarding it doesn’t help, well, I’ll save that discussion for another day.
Why? This is the deciding issue in this debate. If you have information that supports the efficacy and utility of cervical manipulation then you might be holding on to Nobel-worthy discoveries that may revolutionise medical care. Why not tell us about it and see if we can help you make something of it?
Because I’m planning my moms funeral over the next week. This can wait.
I am sorry for your loss. You have my sincere condolences.
From a pro/con on cervical manipulation:
It seems to be a question of not enough benefit to justify the risks, not that there’s no benefit.
Link for the above quote: https://www.bmj.com/bmj/section-pdf/187604?path=/bmj/345/7869/Head_to_Head.full.pdf
@Robin H
It is important to note that David Cassidy is the “for manipulation” voice in this 2012 debate article. Although an ardent scientist, he does have a few horses in this race. We have discussed before that Cassidy, in a hearing before the Connecticut State Board of Chiropractic Examiners Cassidy admitted upon a direct question, that a patient of his suffered stroke after spinal manipulation. He was asked whether he considered the manipulation to have caused the stroke. His reply was to the effect that he did think so at first but after researching the matter he no longer did. There are strong indications that Cassidy let his own search for atonemet influence his research, which has since been reviewed critically and found to be severely flawed https://edzardernst.com/2017/04/we-have-an-ethical-legal-and-moral-duty-to-discourage-chiropractic-neck-manipulations/#comment-108040
@Björn Geir
The quote I gave is not from David Cassidy, it’s from the other side: several people who are saying cervical spine manipulation should not be done.
The pdf I linked to doesn’t have the references. But here are the references for the quote I gave:
1 Debette S, Leys D. Cervical-artery dissections: predisposing factors, diagnosis and outcome. Lancet Neurol 2009;8:668-78.
2 Boyle E, Côte P, Grier AR, Cassidy JD. Examining vertebrobasilar artery stroke in two Canadian provinces. J Manipulative Physiol Ther 2009;32:S194-200.
3 Ernst E. Adverse effects of spinal manipulation: a systematic review. J R Soc Med 2007;100:330-8.
4 Smith WS, Johnston SC, Skalabrin EJ, Weaver M, Azari P, Albers GW, et al. Spinal manipulative therapy is an independent risk factor for vertebral artery dissection. Neurology 2003;60:1424-8.
5 Thomas LC, Rivett DA, Attia JR, Parsons M, Levi C. Risk factors and clinical features of craniocervical arterial dissection. Manual Therapy 2011;16:351-6.
6 Rothwell DM, Bondy SJ, Williams JI, Bousser MG. Chiropractic manipulation and stroke: a population-based case-control study. Stroke 2001;32:1054-60.
7 Cassidy JD, Boyle E, Côté P, He Y, Hogg-Johnson S, Silver FL, Bondy SJ. Risk of vertebrobasilar stroke and chiropractic care. Results of a population-based case-control and case-crossover study. Spine 2008;33 (suppl 4):S176-83.
8 Kawchuk GN, Jhangri GS, Hurwitz EL, Wynd S, Haldeman S, Hill MD. The relation between the spatial distribution of vertebral artery compromise and exposure to cervical manipulation. J Neurol 2008;255:371-7.
9 Ernst E. Vascular accidents after neck manipulation: cause or coincidence? Int J Clin Pract 2010;64:673-7.
Including a couple from our own Dr. Ernst 🙂
I would suggest one looks closely at the Cai, et al study paying attention to both inclusion and exclusion criteria as well as the assumptions they made in their paper.
https://www.sciencedirect.com/science/article/abs/pii/S1052305714001438
In reply to cSMT doesn’t help. Although this is a response to a vague statement I pulled the MA and SR on cSMT from the past 10 years from PubMed. I’m not sure one can claim it doesn’t help.
combining different forms of MT with exercise is better than MT or exercise alone
https://pubmed.ncbi.nlm.nih.gov/28826164/
There was moderate level evidence to support the immediate effectiveness of cervical spine manipulation in treating people with cervical radiculopathy.
https://pubmed.ncbi.nlm.nih.gov/25681406/
The quality of evidence for chronic lumbar spine-related extremity symptoms and cervical spine-related extremity symptoms of any duration is low or very low.
https://pubmed.ncbi.nlm.nih.gov/21292148/
Our review adds new evidence to the Neck Pain Task Force and suggests that mobilization, manipulation, and clinical massage are effective interventions for the management of neck pain.
https://pubmed.ncbi.nlm.nih.gov/26707074/
Upper cervical spine thrust manipulation or mobilisation techniques are more effective than control (low to high evidence), while thoracic manipulations are not.
https://pubmed.ncbi.nlm.nih.gov/26059857/