As we have discussed ad nauseam on this blog, spinal manipulation therapy (SMT) can cause serious adverse events, including spinal epidural hematoma (SEH), an emergency that can cause severe neurological dysfunction. Chinese surgeons have reported three cases of SEH after SMT.
- The first case was a 30-year-old woman who experienced neck pain and numbness in both upper limbs immediately after SMT. Her symptoms persisted after 3 d of conservative treatment, and she was admitted to our hospital. Magnetic resonance imaging (MRI) demonstrated an SEH, extending from C6 to C7.
- The second case was a 55-year-old man with sudden back pain 1 d after SMT, numbness in both lower limbs, an inability to stand or walk, and difficulty urinating. MRI revealed an SEH, extending from T1 to T3.
- The third case was a 28-year-old man who suddenly developed symptoms of numbness in both lower limbs 4 h after SMT. He was unable to stand or walk and experienced mild back pain. MRI revealed an SEH, extending from T1 to T2.
All three patients underwent surgery after failed conservative treatment. Blood clots were found during the operation in case 1 and case 2, and the postoperative pathology confirmed a hematoma. In case three, a vein ruptured during the operation, causing massive bleeding. The three patients recovered to ASIA grade E on day 5, 1 wk, and day 10 after surgery, respectively. All patients returned to normal after 3 mo of follow-up.
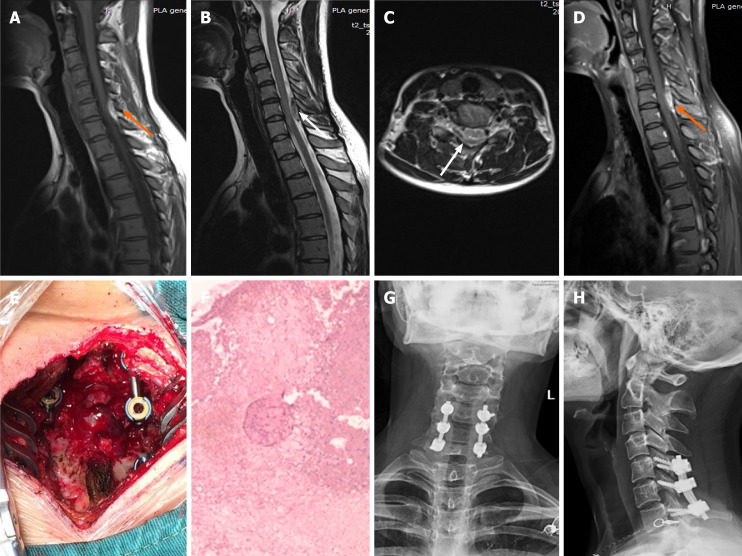
Imaging examinations of case 1. A: T1-weighted preoperative magnetic resonance imaging (MRI) image shows high signal intensity (orange arrow); B and C: Preoperative T2-weighted image shows low signal intensity, and an axial T2-weighted image demonstrates that the hematoma occurred in the posterior region (white arrow); D: Preoperative enhanced MRI suggests an enhanced hematoma signal (orange arrow); E: Intraoperative photograph shows that spinal cord compression has recovered; F: Postoperative pathology suggested a hematoma; G and H: X-ray at the 3-mo follow-up indicated intact internal fixation.
The authors concluded that before proceeding with SMT, each patient should be evaluated in detail and checked for risk factors. In cases where the physical condition changes rapidly, physicians should be alert to the danger and send the patient to the emergency department for a complete MRI examination. We recommend surgery if neurological symptoms appear.
In their paper, the authors also review 15 further cases of SEH that have been previously published. They stress several times in their article that this complication is rare. In my view, this begs the question: how do they know? As there is no post-marketing surveillance of chiropractors or other clinicians doing SMT, I would insist that nobody can be sure about the true incidence of SEH or any other complication after SMT.
PMS itself will not provide the true incidence or establish causation.
but it is an essential step towards these goals
PMS has been instrumental in many drugs being discontinued. Why not SMT?
I didn’t state it couldn’t.
DC: you are truly tiresome
Please reply to the question, “DC”
PMS would/could provide information that has value. It’s unlikely PMS alone would be enough to discontinue SMT.
“The FDA’s system for reporting drug- and device-related health problems is voluntary. The reports are not verified, and critics say this system is underutilized and filled with incomplete and late information.”
https://www.npr.org/sections/health-shots/2017/05/09/527575055/one-third-of-new-drugs-had-safety-problems-after-fda-approval
It may help lead to research to see if a weekend course on SMT is sufficient.
https://ptonice.com/courses-events/total-spine-thrust-manipulation-june-13-14-2020
Or it may help lead us to research potentially unknown contraindications (ex estrogen levels)
Or lead to research to see if some approaches might carry a greater risk of AE (ex Y strap).
So yes PMS has value…never stated otherwise. It just has limitations.
Seems like you do not understand the issue. No surprise.
https://en.wikipedia.org/wiki/Postmarketing_surveillance?wprov=sfti1
Reference in Wikipedia page
“ Drug registries do, however, have some limitations, including a potential for bias and confounding, long periods of follow-up and high cost.”
do you have a point?
If you wish to propose a more effective monitoring system for tracking the adverse effects of SMT, please do so. Throwing your hands in the air saying “that’s not sufficient (so let’s not do anything at all)” is not an adequate response.
At the very least, you should be telling patients (in plain writing) that the chiropractic profession does not perform post-market surveillance so you cannot given them accurate information on the inherent risks in their procedures. You can’t have Informed Consent without the information part, even if that information is an unhelpful but honest “We can’t tell you how dangerous this is because we don’t know ourselves.”
I never said don’t do anything at all. Again you assume.
There are several studies that have calculated the potential risk of serious AE. Most currently conclude they are rare.
“There are several studies that have calculated the potential risk of serious AE.”
Oh, please. “Calculated” is all too easily an evasive euphemism for guesswork. Steve Kirsch calculated that COVID vaccines have killed 200,000 Americans. He never tried to check the excess death statistics for 2021 to see if his calculation actually matched reality before screaming his message over the internet, and now more people will die because they’ve been scared off vaccinating by Kirsch and others like him. (Hint: Excess deaths are still tracking infection rates, not vaccination rates.)
Until you knuckle down and gather the real numbers from the ground—all the numbers, both good and bad—your “calculated studies” don’t prove squat. They might be on the nose; they could be completely astray. Either way, they are at best a testable hypothesis waiting to be tested. Because they’re built on speculation and bias, not on cold hard dispassionate analysis of all the available evidence. This is the problem with AltMed: it assumes; it doesn’t test. It doesn’t matter whether that’s because they’re too arrogant to think they could possibly be wrong, because they fear it might not give them the answer they’re looking for, or holy-rolling evangelists impatient to make their sale.
When people are injured and killed if you’re wrong, it’s deliberate negligence not to confirm to a very high degree of confidence that you are not before proceeding any further. And that’s “confidence” as in “the absolute numbers don’t lie”, not “I choose to believe in it really really hard”.
current view:
“Serious adverse events associated with manipulative therapies are typically defined as conditions that lead to hospital admission or death, but these are rare.” Am Fam Physician. 2019 Feb 15;99(4):248-252.
“…but these are rare”
HOW DO THEY KNOW?
there is no PMS and thus nobody knows!
Here’s the actual paper, since @DC neglected to link it. I’ve only quickly skimmed it, but it’s worth noting that it is not limited to chiro but covers osteopathy and other procedures as well, and looks to extrapolate its risk numbers from trial data, not collect them directly from post-treatment surveillance.
That’s pretty weak sauce: without full monitoring, how do we know which procedures are the riskiest, and how do we know if the rate of serious AEs is going up or down? And without knowing these things, how can we hope to correct for them? Or is @DC fine with N patients being injured and killed each year, and nothing being done about it?
Also worth noting as a takeaway (and stop us if you’ve heard this one before):
Business as usual, in other words. (Not only do we not know how dangerous it is, we don’t even know if that danger is worth it!)
So, @DC, do patients not deserve to have these questions accurately answered? Or is it all about you?
Sigh. I have on several occasions stated in these blogs that a support a PMS.
Until then they base the estimates on the information that is available. Currently this indicates that these serious AE are rare.
I know some of the chiropractors who are involved in setting up such systems. If anyone here has a background in said projects and wants to become part of their team let me know. Otherwise you are just complaining for the sake of complaining.
I’m moving on.
” they base the estimates on the information that is available”
exactly! and the information that is available is the tip of an iceberg.
@DC: “If anyone here has a background in said projects and wants to become part of their team let me know.”
It is not our job to do your (chiropractors) job for you. Perhaps if you’d had to set up your PMS before you set up your billing, you might have got it done by now. Says something about AltMed’s order of priorities: practice, profit, patient.
@Prof Ernst: “the information that is available is the tip of an iceberg”
Maybe, maybe not. Hence the need to reliable monitoring to capture the actual numbers instead of sampling and guesswork, and hoping it’s representative. That said, an upper limit might be reasonably estimated by counting the total number of characteristic injuries occuring annually in the population, as reported by A&Es and pathologists. (There might be some percentage that do not show up in the conventional medical system at all, but I’m guessing most folks who are stroking out or whatever get called an ambulance, whether they want it or not.)
EE exactly! and the information that is available is the tip of an iceberg.
As is what is currently being reported elsewhere under a “mandatory” system.
https://link.springer.com/article/10.2165%2F00002018-200629050-00003
I support PMS within chiropractic. As more information becomes available the risk can be recalculated.
Geesh.
I don’t think anyone here cares a toss what you support.
we want the chiropractic organizations to support PMS and get on with it.
has: It is not our job to do your (chiropractors) job for you.
I never said it was. I wrote “become part of the team”
You know, be a team player instead of a heckler on the sidelines. But perhaps that is all some have to offer.
@DC: “You know, be a team player instead of a heckler on the sidelines.”
That is a very silly comment. I am not a chiropractor. I am not even medically trained (flunked 1st year premed and work in a totally different field now). It is not my job to play on your team. It is for you and your fellow chiropractors to get your act together and sort it out yourselves.
It is laudable that you personally support the introduction of PMS and I do commend you for that attitude. But, talk is easy. You and your likeminded colleagues seriously need to light a fire under ALL of your fellow chiropractors as, a hundred years on, it is clear that far too many of them are happy to cruise along on “business as usual”, performing the procedures and taking the money, and not doing due dilligence in identifying adverse effects and correcting when they occur.
It is well known that conventional medicine, thanks to various perverse incentives, all too often turns a blind eye to its own problems, at cost of patients’ trust, health, and even lives. But at least those failures eventually see light of day, because some are paying attention and refuse to let it slide forever.
With AltMed, all too often the collective attitude is “as long as we never look for problems in our own house, then those problems don’t exist”, while simultaneously being first in line to screech and hoot loudly about conventional medicines screwups, real and imagined. The stench of that hypocrisy is both staggering and infuriating, given the double standard. But since few within AltMed wish to (or will dare) call out its own failings, that only leaves us outsiders to sit on the sidelines and, as you put it, remind y’all repeatedly that your first duty is to PATIENTS, not yourselves. No, we shouldn’t have to do that job either, but AltMed refuses to do it for themselves. And that is on all of you too.
Heck, when your professional bodies won’t even censure lying incompetents like Arleen Scholten who kill vulnerable patients and still continue to practise, it clearly has a long way to go.
Sigh. I was simply pointing out the limitations of such a system with regards to “true incidence “.
Strange that ruffled feathers, well, not really.
FAERS Limitations
• Passive, voluntary surveillance
• Underreporting occurs and is variable from drug to drug and over time
– Some literature cites 1-10%
– ActualisunknownsoFDAdoesnotassumeextent
• Reporting bias exists
• Quality of the reports is variable and often incomplete
• Duplicate reporting of the same case occurs
• Not population-based data source
– Cannotreliablyestimateincidenceorprevalence
– Numeratoruncertain,denominatorcanonlybeprojectedfromdrug utilization data
https://www.fda.gov/files/about%20fda/published/Drug-Safety-Surveillance-and-the-FDA-Adverse-Event-Reporting-System-%28PDF—1.31MB%29.pdf
everyone knows the limitations of PMS
everyone knows the limitations of seatbelts
BUT IT’S FAR WORSE DO CONTINUE WITHOUT THEM
has, perhaps you missed this requirement “If anyone here has a background in said projects…”
You don’t, that’s OK.
And yes there are folks working on this and related projects within chiropractic , which is unlike the medical profession that was “forced” by the FDA to report to an AE reporting system (1990’s if I recall)
An example of efforts:
“International stakeholders are being invited to participate, with individuals in the following categories: academic researchers, manual therapy clinicians, patients, medical doctors, manual therapy students, professional regulatory-body representatives, malpractice insurance representatives, lawyers or judges, and data analysts/informatics/electronic health record representatives. At least 75 participants will be recruited in this e-Delphi study to ensure that all stakeholder roles, international perspectives, and multidisciplinary professions are represented.”
https://redcap.parker.edu/surveys/?s=AD3DNXWEL7
EE: BUT IT’S FAR WORSE DO CONTINUE WITHOUT THEM
And yet I am not aware of one allied health profession that has a PMS. Physical Therapy? Dentistry? Massage Therapy? Optometry?
Perhaps chiropractic will lead the way.
and I am not aware of reports of practitioners of Physical Therapy, Dentistry, Massage Therapy, Optometry, to be associated with hundreds of serious complications and deaths. in this respect, chiros certainly lead the way
EE and I am not aware of reports of practitioners of Physical Therapy, Dentistry, Massage Therapy, Optometry, to be associated with hundreds of serious complications and deaths.
Well I could share the research but you would probably just dismiss it.
I very much doubt that you have it!
Apparently you haven’t looked into it. Dental anesthesia, LASIK, falls, etc.
Of course without a PMS system we really don’t know the “true incidence”. Until then we look at the information that is available.
remember: hundreds
remember: Physical Therapy, Dentistry, Massage Therapy, Optometry
You can start with these limited studies…
Death was the most important side effect of anaesthesia in dentistry. In this article we reviewed more than 20 studies with adequate data focusing on death associated with dental procedures since 1955 and found 218 deaths out of 71,435,282 patients (3 deaths per 1,000,000 persons) with the mortality rate of 1:327,684.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5535496/
In the LASIK group, there were 287 SAEs (271 eyes of 226 patients; incidence of 0.4% or 1:228 eyes), and the number of SAEs in PRK group was 65 (65 eyes of 39 patients; incidence 0.7% or 1:146 eyes). Combining LASIK and PRK data, the loss of 2 or more lines of CDVA was recorded in 0.37% of eyes.
https://www.ajo.com/article/S0002-9394(19)30504-5/fulltext
” Physical Therapy, Dentistry, Massage Therapy, Optometry”
I think you may have forgotten some
You could just deal with the ones presented.
Regardless:Extrapolate just this one procedure to the whole profession. (Psst…missed dx and delayed care are considered the most common AEs followed by falls)
“Twenty major AE’s were reported out of the 20,494 treatments for a rate of <0.1% (1 per 1,024 TDN treatments).”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7015026/
But we really don’t know the extent
“ It is clear that standardized reporting of harms is not properly undertaken within orthopaedic physical therapy efficacy research and not well followed in long-term surveillance.” journal of orthopaedic & sports physical therapy | volume 40 | number 8 | august 2010 | 455
“ Overall, a small body of literature addresses AEs associated with rehabilitation practices. Few studies evaluate AEs resulting from interventions prescribed by rehabilitation professionals. There are no studies on the full spectrum of risks associated with treatment by these disciplines.”
“ During the 11-year period, 40 reports of 138 AEs were associated with massage.” Ping Yin et al. Evid Based Complement Alternat Med. 2014.
ok, you don’t want to admit that, once again, you were blowing hot air.
fair enough
cognitive dissonance?
did you learn a new word?
well done!!!