The purpose of this survey was to quantify and describe the clinical practice beliefs and behaviors associated with US chiropractors. A 10% random sample of US chiropractors (n = 8975) was selected from all 50 state regulatory board lists and invited to participate in a survey. The survey consisted of a 7-item questionnaire; 6 items were associated with chiropractic ideological and practice characteristics and 1 item was related to the self-identified role of chiropractic in the healthcare system which was utilized as the dependent variable to identify chiropractic subgroups. Multinomial logistic regression with predictive margins was used to analyze which responses to the 6 ideology and practice characteristic items were predictive of chiropractic subgroups.
The survey instrument used in this study was developed by the authors and modeled after similar chiropractic identity analyses. The survey instrument included a total of 7 items intended to elicit divergent ideologies and practice behaviors. The figure below is a copy of the survey instrument.

A total of 3538 responses were collected (39.4% response rate). Respondents self-identified into three distinct subgroups based on the perceived role of the chiropractic profession in the greater healthcare system:
- 57% were spine/neuromusculoskeletal focused;
- 22% were primary care focused;
- 21% were vertebral subluxation focused.
Patterns of responses to the 6 ideologies and practice characteristic items were substantially different across the three professional subgroups.
The authors concluded that respondents self-identified into one of three distinct intra-professional subgroups. These subgroups can be differentiated along themes related to clinical practice beliefs and behaviors.
Here are the results in more detail as sated by the authors:
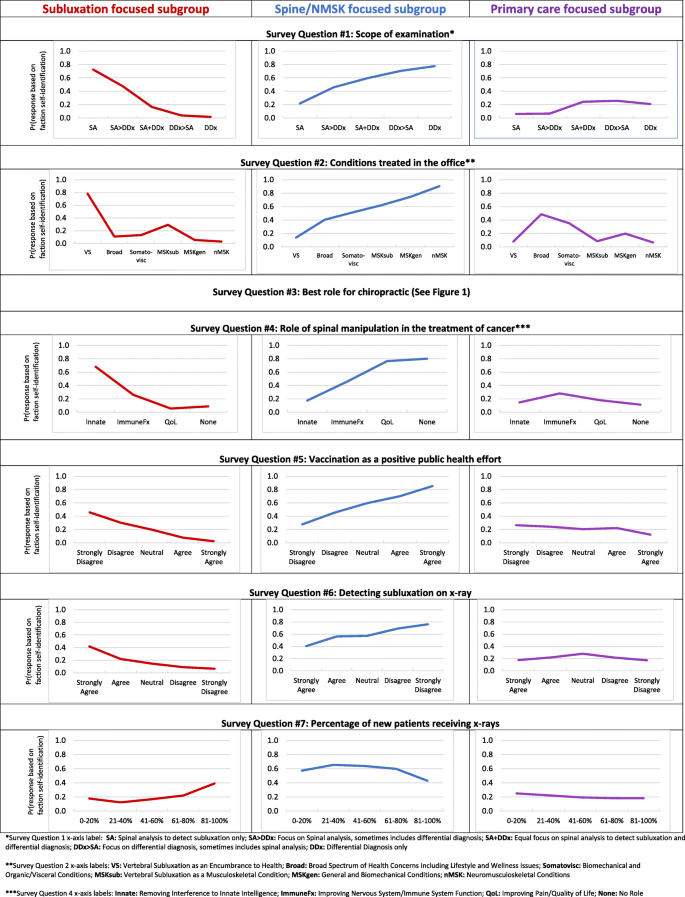
Regarding scope of examination (survey question 1), respondents reporting the scope of their clinical examination to only include spinal analysis for the assessment of vertebral subluxation had a 70% probability of belonging to the subluxation focused subgroup, a 20% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup. Conversely, respondents who reported the scope of their clinical examination only includes a differential diagnosis had a 0% probability of belonging to the vertebral subluxation focused subgroup, an 80% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 20% probability of belonging to the primary care focused subgroup.
Concerning conditions treated (survey question 2), respondents who reported predominantly treating vertebral subluxation as an encumbrance to health had an 80% probability of belonging to the vertebral subluxation focused subgroup, a 10% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup. In contrast, respondents reporting predominantly treating neuromusculoskeletal conditions had a 0% probability of belonging to the vertebral subluxation focused subgroup, a 90% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup.
Regarding the role of spinal manipulation for those with cancer (survey question 4), respondents reporting the role of spinal manipulation for those with cancer is to remove interference to innate intelligence had a 70% probability of belonging to the vertebral subluxation focused subgroup, a 20% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup. Respondents reporting there is no role of spinal manipulation in those with cancer also had a 10% probability of belonging to the subluxation focused subgroup, an 80% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup.
Regarding vaccination (survey question 5), respondents who strongly disagreed that vaccinations have had a positive effect on global public health had a 50% probability of belonging to the vertebral subluxation focused subgroup, an approximately 25% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and an approximately 25% probability of belonging to the primary care focused subgroup. In contrast, respondents who strongly agreed that vaccinations have had a positive effect on global public health had a 0% probability of belonging to the vertebral subluxation focused subgroup, a 90% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup.
Concerning the detection of vertebral subluxation on x-ray (survey question 6), respondents who strongly agreed that x-ray is helpful in detecting vertebral subluxations had a 40% probability of belonging to the vertebral subluxation focused subgroup, a 40% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 20% probability of belonging to the primary care focused subgroup. Respondents who strongly disagreed that x-ray is helpful in detecting vertebral subluxations had a near 0% probability of belonging to the vertebral subluxation focused subgroup, an 80% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and slightly below a 20% probability of belonging to the primary care focused subgroup.
Regarding use of x-rays for new patients (survey question 7), respondents who reported prescribing x-rays for 0–20% of new patients had a 20% probability of belonging to the vertebral subluxation focused subgroup, a 60% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 20% probability of belonging to the primary care focused subgroup. Respondents reporting prescribing x-rays for 81–100% of new patients had a 40% probability of belonging to the vertebral subluxation focused subgroup, a 40% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 20% probability of belonging to the primary care focused subgroup.
END OF QUOTE
While I am not sure that the division into the 3 subgroups is valid and suspect that there must be a substantial overlap between them, I must admit that the paper is rich in fascinating information. Generally speaking, I find all subgroups somewhat mysterious and would ask them the following questions:
Subgroup 1: why did you not study medicine or physiotherapy?
Subgroup 2: does it not bother you that your education and training are woefully insufficient for primary care?
Subgroup 3: is it not time to abandon the obsolete nonsense of your guru, the old charlatan DD Palmer?
Please, Mr. Ed Ernst, the bibliographic reference
if you mean the link to the original paper, click on the words “the survey” of the 1st sentence.
Thanks
1. I wanted a wider variety of tools than physio have (that is why so many of them go to chiro schools in the US and EU), and I wanted the diagnostic training which is the basis of chiropractic training.
2. that is your political assessment. thankfully the regulatory agencies especially in north America think differently and so does all the comparative analysis made between MD and DC courses. Sorry to disappoint you but you are grossly uninformed on that matter. please look at the report by the American National Health Federation comparing the education at 22 MD and 11 DC courses.
3. DD palmer ideas are no better or worse than those of surgeons in the US civil war. Nice story but completely irrelevant for today practice.
‘Dr’ G. Almog has courteously responded to the question posed by Ernst (and myself) so often:
“Why did you not go to physiotherapy school”.
But he has failed to answer: “Why did you not go to medical school and become an MD? Then you’d have even more ‘tools at your disposal.’
And I also ask: “Why did you not go to a school of osteopathy/”
If there is no perceived differnce between a chiropractic and a medical education, why not choose medicine?
What is the USP of ‘chiropractic’?
Once again a survey indicates that the majority of chiropractors focus on the MSK system and don’t practice based on the original Palmer beliefs.
only if you believe that the way they categorized the 3 groups is valid
It was piloted and it reflects similar findings from other research.
“The survey instrument was piloted in a group of licensed chiropractors (n = 10) in Canada. The survey instrument was revised to improve clarity based on feedback provided during pilot testing, prior to administration to the randomly selected sample.”
Of course if you have evidence that questions it’s validity…
and I had always thought that
1) a pilot does not prove the validity
2) that those who make a claim (and not those who doubt) have to prove it
in any case, as I state in the post, the overlap is likely to be substantial.
Of course there are an overlaps. Most likely looks like a Gaussian distribution, but may be shifted depending on the question. The purpose of the paper was predictability based upon beliefs and practices. Putting into three groups or five or ten, the overall theme remains the same.
“Once the draft questionnaire finalized through preliminary pilot testing and subsequent revisions from
experts is ready, the researcher can conduct a full-fledged pilot test among the intended respondents for
initial validation. The pilot testing consists of administering the final version of the questionnaire to a
considerable number of intended respondents. If the sample size of pilot test is small, then the possible
errors may decrease the statistical power required to validate the questionnaire. In this stage, based on
the intended statistical tests and validation on the collected pilot samples, the questionnaire can be
refined further to a level which can minimize the statistical errors in the final solution. ” https://mpra.ub.uni-muenchen.de/103996/1/MPRA_paper_103996.pdf