Monthly Archives: August 2021
The objective of this systematic review was to assess the effects and reliability of sham procedures in manual therapy (MT) trials in the treatment of back pain (BP) in order to provide methodological guidance for clinical trial development. Different databases were screened up to 20 August 2020. Randomised clinical trials involving adults affected by BP (cervical and lumbar), acute or chronic, were included. Hand contact sham treatment (ST) was compared with different MT (physiotherapy, chiropractic, osteopathy, massage, kinesiology, and reflexology) and to no treatment. Primary outcomes were BP improvement, the success of blinding, and adverse effect (AE). Secondary outcomes were the number of drop-outs. Dichotomous outcomes were analysed using risk ratio (RR), continuous using mean difference (MD), 95% CIs. The minimal clinically important difference was 30 mm changes in pain score.
A total of 24 trials were included involving 2019 participants. Different manual treatments were provided:
- SM/chiropractic (7 studies, 567 participants).
- Osteopathy (5 trials, 645 participants).
- Kinesiology (1 trial, 58 participants).
- Articular mobilisations (6 trials, 445 participants).
- Muscular release (5 trials, 304 participants).
Very low evidence quality suggests clinically insignificant pain improvement in favour of MT compared with ST (MD 3.86, 95% CI 3.29 to 4.43) and no differences between ST and no treatment (MD -5.84, 95% CI -20.46 to 8.78).ST reliability shows a high percentage of correct detection by participants (ranged from 46.7% to 83.5%), spinal manipulation being the most recognised technique. Low quality of evidence suggests that AE and drop-out rates were similar between ST and MT (RR AE=0.84, 95% CI 0.55 to 1.28, RR drop-outs=0.98, 95% CI 0.77 to 1.25). A similar drop-out rate was reported for no treatment (RR=0.82, 95% 0.43 to 1.55).

Forest plot of comparison ST versus MT in back pain outcome at short term. MT, manual therapy; ST, sham treatment.
The authors concluded that MT does not seem to have clinically relevant effect compared with ST. Similar effects were found with no treatment. The heterogeneousness of sham MT studies and the very low quality of evidence render uncertain these review findings. Future trials should develop reliable kinds of ST, similar to active treatment, to ensure participant blinding and to guarantee a proper sample size for the reliable detection of clinically meaningful treatment effects.
Essentially these findings suggest that the effects patients experience after MT are not due to MT per see but to placebo effects. The review could be criticised because of the somewhat odd mix of MTs lumped together in one analysis. Yet, I think it is fair to point out that most of the studies were of chiropractic and osteopathy. Thus, this review implies that chiropractic and osteopathy are essentially placebo treatments.
The authors of the review also provide this further comment:
Similar findings were found in other reviews conducted on LBP. Ruddock et al included studies where SM was compared with what authors called ‘an effective ST’, namely a credible sham manipulation that physically mimics the SM. Pooled data from four trials showed a very small and not clinically meaningful effect in favour of MT.52
Rubinstein et al 53 compared SM and mobilisation techniques to recommended, non-recommended therapies and to ST. Their findings showed that 5/47 studies included attempted to blind patients to the assigned intervention by providing an ST. Of these five trials, two were judged at unclear risk of participants blinding. The authors also questioned the need for additional studies on this argument, as during the update of their review they found recent small pragmatic studies with high risk of bias. We agree with Rubinstein et al that recent studies included in this review did not show a higher quality of evidence. The development of RCT with similar characteristic will probably not add any proof of evidence on MT and ST effectiveness.53
If we agree that chiropractic and osteopathy are placebo therapies, we might ask whether they should have a place in the management of BP. Considering the considerable risks associated with them, I feel that the answer is obvious and simple:
NO!
Multiple sclerosis (MS) causes a range of different symptoms. Patients with MS have looked for alternative therapies to control their MS progress and treat their symptoms. Non-invasive therapeutic approaches such as massage can have benefits to mitigate some of these symptoms. However, there is no rigorous review of massage effectiveness for patients suffering from MS.
The present systematic review was aimed at examining the effectiveness of different massage approaches on common MS symptoms, including fatigue, pain, anxiety, depression, and spasticity.
A total of 12 studies met the inclusion criteria. The authors rated 5 studies as being of fair and 7 studies of good methodological quality. Fatigue was improved by different massage styles, such as reflexology, nonspecific therapeutic massage, and Swedish massage. Pain, anxiety, and depression were effectively improved by reflexology techniques. Spasticity was reduced by Swedish massage and reflexology techniques.
The authors concluded that different massage approaches effectively improved MS symptoms such as fatigue, pain, anxiety, depression, and spasticity.
Clinical trials of massage therapy face formidable obstacles including:
- difficulties in obtaining funding,
- difficulties in finding expert researchers who are interested in the subject,
- difficulties to control for placebo effects,
- difficulties in blinding patients,
- impossibility of blinding therapists,
- confusion about the plethora of different massage techniques.
Thus, the evidence is often less convincing than one would hope. This, however, does not mean that massage therapy does not have considerable potential for a range of indications. One could easily argue that this situation is similar to spinal manipulation. Yet, there are at least three important differences:
- massage therapy is not as heavily burdened with frequent adverse effects and potentially life-threatening complications,
- massage therapy has a rational basis,
- the existing evidence is more uniformly encouraging.
Consequently, massage therapy (particularly, classic or Swedish massage) is more readily being accepted even in the absence of solid evidence. In fact, in some countries, e.g. Germany and Austria, massage therapy is considered to be a conventional treatment.
This multicenter, randomized, sham-controlled trial was aimed at assessing the long-term efficacy of acupuncture for chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS). Men with moderate to severe CP/CPPS were recruited, regardless of prior exposure to acupuncture. They received sessions of acupuncture or sham acupuncture over 8 weeks, with a 24-week follow-up after treatment. Real acupuncture treatment was used to create the typical de qi sensation, whereas the sham acupuncture treatment (the authors state they used the Streitberger needle, but the drawing looks more as though they used our device) does not generate this feeling.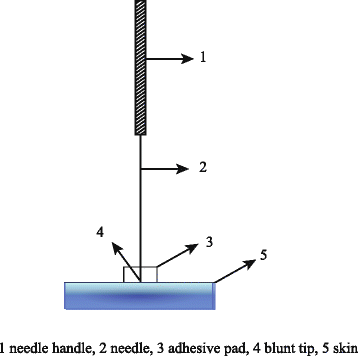
The primary outcome was the proportion of responders, defined as participants who achieved a clinically important reduction of at least 6 points from baseline on the National Institutes of Health Chronic Prostatitis Symptom Index at weeks 8 and 32. Ascertainment of sustained efficacy required the between-group difference to be statistically significant at both time points.
A total of 440 men (220 in each group) were recruited. At week 8, the proportions of responders were:
- 60.6% (95% CI, 53.7% to 67.1%) in the acupuncture group
- 36.8% (CI, 30.4% to 43.7%) in the sham acupuncture group (adjusted difference, 21.6 percentage points [CI, 12.8 to 30.4 percentage points]; adjusted odds ratio, 2.6 [CI, 1.8 to 4.0]; P < 0.001).
At week 32, the proportions were:
- 61.5% (CI, 54.5% to 68.1%) in the acupuncture group
- 38.3% (CI, 31.7% to 45.4%) in the sham acupuncture group (adjusted difference, 21.1 percentage points [CI, 12.2 to 30.1 percentage points]; adjusted odds ratio, 2.6 [CI, 1.7 to 3.9]; P < 0.001).
Twenty (9.1%) and 14 (6.4%) adverse events were reported in the acupuncture and sham acupuncture groups, respectively. No serious adverse events were reported. No significant difference was found in changes in the International Index of Erectile Function 5 score at all assessment time points or in peak and average urinary flow rates at week 8.
The authors concluded that, compared with sham therapy, 20 sessions of acupuncture over 8 weeks resulted in greater improvement in symptoms of moderate to severe CP/CPPS, with durable effects 24 weeks after treatment.
The study was sponsored by the China Academy of Chinese Medical Sciences and the National Administration of Traditional Chinese Medicine. The trialists originate from the following institutions:
- 1Guang’anmen Hospital, China Academy of Chinese Medical Sciences, Beijing, China (Y.S., B.L., Z.Q., J.Z., J.W., X.L., W.W., R.P., H.C., X.W., Z.L.).
- 2Key Laboratory of Chinese Internal Medicine of Ministry of Education, Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, China (Y.L.).
- 3ThedaCare Regional Medical Center – Appleton, Appleton, Wisconsin (K.Z.).
- 4Hengyang Hospital Affiliated to Hunan University of Chinese Medicine, Hengyang, China (Z.Y.).
- 5The First Hospital of Hunan University of Chinese Medicine, Changsha, China (W.Z.).
- 6Guangdong Provincial Hospital of Traditional Chinese Medicine, Guangzhou, China (W.F.).
- 7The First Affiliated Hospital of Anhui University of Chinese Medicine, Hefei, China (J.Y.).
- 8West China Hospital of Sichuan University, Chengdu, China (N.L.).
- 9China Academy of Chinese Medical Sciences, Beijing, China (L.H.).
- 10Yantai Hospital of Traditional Chinese Medicine, Yantai, China (Z.Z.).
- 11Shaanxi Provincial Hospital of Traditional Chinese Medicine, Xi’an, China (T.S.).
- 12The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, China (J.F.).
- 13Beijing Fengtai Hospital of Integrated Traditional and Western Medicine, Beijing, China (Y.D.).
- 14Xi’an TCM Brain Disease Hospital, Xi’an, China (H.S.).
- 15Dongfang Hospital Beijing University of Chinese Medicine, Beijing, China (H.H.).
- 16Luohu District Hospital of Traditional Chinese Medicine, Shenzhen, China (H.Z.).
- 17Guizhou University of Traditional Chinese Medicine, Guiyang, China (Q.M.).
These facts, together with the previously discussed notion that clinical trials from China are notoriously unreliable, do not inspire confidence. Moreover, one might well wonder about the authors’ claim that patients were blinded. As pointed out above, the real and sham acupuncture were fundamentally different: the former did generate de qi, while the latter did not! A slightly pedantic point is my suspicion that the trial did not test the efficacy but the effectiveness of acupuncture, if I am not mistaken. Finally, one might wonder what the rationale of acupuncture as a treatment of CP/CPPS might be. As far as I can see, there is no plausible mechanism (other than placebo) to explain the effects.
So, is the evidence that emerged from the new study convincing?
No, in my view, it is not!
In fact, I am surprised that a journal as reputable as the Annals of Internal Medicine published it.
A case report was published of a 35-year-old Chinese man with no risk factors for stroke. He presented with a 2-day history of expressive dysphasia and a 1-day history of right-sided weakness. The symptoms were preceded by multiple sessions of the neck, shoulder girdle, and upper back massage for pain relief in the prior 2 weeks. A CT-scan of the brain demonstrated an acute left middle cerebral artery infarct and left internal carotid artery dissection. The MRI cerebral angiogram confirmed left carotid arterial dissection and intimal oedema of bilateral vertebral arteries. In the absence of other vascular comorbidities and risk factors, massage-induced internal carotid arterial dissection was deemed to be the most likely cause of the near-fatal cerebrovascular event.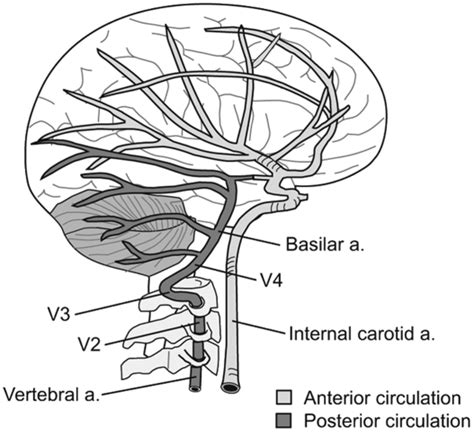
INSIDER reported further details of the case: the patient told the doctors who treated him that he had seen the chiropractor for two weeks before he experienced trouble reading, writing and talking. After experiencing those symptoms for two days and one day of pain on his right side, a friend convinced the patient to consult a neurologist. This led to the hospital admission, the above-named tests, and diagnosis. After three months of therapy and rehab, the patient showed “significant improvement,” according to the doctors.
What remains unclear is the exact nature of the neck treatment that is believed to have caused the arterial dissection. A massage is mentioned but massages have rarely been associated with such problems. Neck manipulations, on the other hand, are the hallmark therapy of chiropractors and have, as I have pointed out regularly, often been reported to cause arterial dissections.
Chiropractors usually deny this fact; alternatively, they claim that only poorly trained practitioners cause these adverse events or that their frequency is exceedingly small. However, without a proper post-marketing surveillance system, this argument is hardly convincing.
Weleda, the firm founded by Rudolf Steiner and Ita Wegman originally for producing and selling their anthroposophic remedies, celebrates its 100th anniversary. It is a truly auspicious occasion for which I feel compelled to offer a birthday present.
I hope they like it!
On the Weleda UK website, we find an article entitled ‘ An introduction to Homeopathy‘ which contains the following statements:
- Homeopathy works by stimulating the body’s own natural healing capacity. The remedy triggers the body’s own healing forces and so a remedy is prescribed on a very individual basis.
- If you do experience complex, persistent or worrying symptoms then please seek the advice of a doctor who specialises in homeopathy.
- Today there are four homeopathic hospitals offering treatment under the National Health Service – in London, Glasgow, Liverpool and Bristol.
- It’s still the only alternative medicine incorporated into the NHS.
- Homeopathy can be used to treat the same wide range of illness as conventional medicine, and may even prove successful when all other forms of treatment have failed.
- Over-the-counter homeopathic medicines are made using natural plant, mineral and, occasionally, animal substances
- … active elements are in infinitesimally small quantities.
As I understand a bit about the subject – not as much as my friend Dana Ullman, of course, but evidently more than the Weleda team – I thought I might offer them, as a birthday present, a free correction of these 7 passages. Here we go:
- Homeopathy is claimed to work by stimulating the body’s own natural healing capacity. In fact, it does not work. Yet, believers argue that the remedy triggers the body’s own healing forces and so a remedy is prescribed on a very individual basis.
- If you do experience complex, persistent or worrying symptoms then please seek the advice of a doctor who specializes in something other than homeopathy.
- Today there are no homeopathic hospitals offering treatment under the National Health Service – the ones in London, Glasgow, Liverpool, and Bristol all closed or changed their names.
- It’s no longer incorporated into the NHS.
- Homeopathy cannot be used to treat the same wide range of illnesses as conventional medicine and is not successful when all other forms of treatment have failed.
- Over-the-counter homeopathic medicines are made using any imaginable substance and even non-material stuff like vacuum or X-rays.
- … active elements are absent.
HAPPY BIRTHDAY, WELEDA!
 So-called alternative medicine (SCAM) for cancer is the title of my new book. I was informed that it has been published but, in reality, the hard copy might still take a few days until it is available (there were major problems at the proof-reading stage which caused a considerable delay). To give you a flavor of the book, allow me to show you my introduction; here it is:
So-called alternative medicine (SCAM) for cancer is the title of my new book. I was informed that it has been published but, in reality, the hard copy might still take a few days until it is available (there were major problems at the proof-reading stage which caused a considerable delay). To give you a flavor of the book, allow me to show you my introduction; here it is:
In February 2013, my wife and I were in good spirits. I had recently retired from my post at Exeter University, and we were heading off to celebrate Danielle’s round birthday with her family in Brittany. There was just one thing that bothered us: Danielle had recurring abdominal pains. She had seen our GP in England several times about it. The last time, she had received a prescription for some antibiotics. I knew they would not help; her symptoms were not due to an infection.
After our arrival in France, things got worse, and Danielle consulted a gynaecologist at the out-patient clinic of the local hospital. More tests were ordered; an ultrasound showed an abnormality; a subsequent MRI revealed a tumour of the uterus. The gynaecologist advised to operate as soon as possible, and Danielle agreed.
The operation went well, but the gynaecologist, Dr Matthieu Jacquot, was concerned and said he had to be more radical than he had anticipated. The diagnosis was still uncertain until the results from the histology lab were in. A few days later, when we saw Dr Jacquot again, our hopes that all was fine were thoroughly dashed. He explained that Danielle had cancer of the endometrium and laid out the treatment plan which an entire team of oncologists had designed after an in-depth review of her case: a second, much more extensive operation, followed by six sessions of chemotherapy, followed by months of daily radiotherapy, followed by two sessions of brachytherapy.
Dr Jacquot could not have been more empathetic. He explained in detail what consequences all this would have. Danielle’s life would be dominated for the next year by a long series of treatments that were unpleasant to say the least. We were both shocked and close to tears.
Before arriving at a decision, we talked to friends and experts in this area. Opinions differed marginally. Two days later, we had made up her mind: we would stay in Brittany for the entire year and get Danielle treated exactly as Dr Jacquot suggested.
The second operation was much tougher than the first, but Danielle recovered well. Ten days later, she was back in our home and looked after by a nurse who came daily to change the bandages and give injections. On her third visit, the nurse broached the subject of chemotherapy which was scheduled to start soon. She explained how unpleasant it would be and what horrendous side effects Danielle was facing. Then she said: ‘You know, you don’t need to go through all this. They only pump you full with poison. There is a much better approach. Just follow the anti-cancer diet of Dr Schwartz.[1] It is natural and has no side effects. It would surely cure your cancer.’ When Danielle told me about this conversation, I informed the nurse that from now on I would myself take charge of the post-operative care of my wife and that her services were no longer required.
Today, Danielle is cancer-free. Had she listened to the nurse, she would almost certainly no longer be with us. But the lure of a ‘natural’ cancer cure with no side effects is almost irresistible. Faced with a serious diagnosis like cancer, most patients would consider any therapy that promises help without harm. Inevitably, they encounter a myriad of so-called alternative medicines (SCAMs), and many patients give SCAM a try.
In addition to Dr Schwartz’s cancer diet, there are hundreds of SCAMs that specifically target vulnerable cancer patients like Danielle. How can patients not be confused, and who might give them responsible advice? Conventional doctors rarely do. A recent summary of 29 relevant papers concluded that physicians will discuss complementary therapies only when a patient him/herself raises this issue within a consultation.[2] But cancer patients are often too embarrassed to ask about SCAM. Those who are courageous enough usually get short shrift. Many conventional doctors are not just critical about SCAM, but also know very little about the subject.[3]
Patients deserve evidence-based information, instead they often get unhelpful blanket statements from their GPs such as:
- ‘there is no evidence’;
- ‘that’s all rubbish, best to stay well clear of it’;
- ‘if you want to try it, go ahead, it cannot do much harm’.
All of these are untrue. Frustrated by such erroneous platitudes, patients might go on the Internet for help where they are bombarded with uncritical promotion. We investigated the information on SCAM for cancer provided by popular websites and found that they offer information of extremely variable quality. Many endorse unproven therapies and some are outright dangerous.[4] Sadly, the advice patients might glean from newspapers[5] or health-food stores[6] tends to be equally misleading and potentially harmful.
Subsequently, some patients might visit a library and read one of the many books on the subject. If anything, they are even worse. We have repeatedly analysed the contents of consumer guides on SCAM and always concluded that following their recommendations would shorten the life of the reader.[7] To give you a flavour, here are a few titles currently on sale:
- Cancer Medicine from Nature
- Outsmart Your Cancer: Alternative Non-Toxic Treatments That Work
- Cancer Medicine from Nature
- Perfect Guide on How to Cure Breast Cancer Through Curative Approved Alkaline Diets & Herbs
- How to Starve Cancer
- Healing the Prostate: The Best Holistic Methods to Treat the Prostate and Other Common Male-Related Conditions
- Outsmart Cancer: Defeat Cancer With Vitamin B17, Healthy Nutrition and Alternative Medicine
Cancer patients would, of course, all like to ‘outsmart cancer’; they are desperate and vulnerable. In this state of mind, they easily fall victim to anyone who sells false hope at inflated prices. The consequences can be tragic.
In 2016, the actress English Leah Bracknell, for example, raised ~£50 000 to treat her lung cancer in the German ‘Hallwang Private Oncology Clinic’. The SCAMs used there included homeopathy, micronutrients, natural supplements, whole-body hyperthermia, and ozone therapy, none of which cures cancer. If cancer patients fall for bogus treatments, they not just lose their money but also their lives. Leah Bracknell died of her cancer in 2019.[8]
Three basic facts are indisputably clear:
- a high percentage of cancer patients use SCAM,
- misinformation about SCAM is rife,
- misinformation endangers the lives of cancer patients.
It follows that there is an obvious and urgent need for an evidence-based text naming the SCAMs that are potentially harmful and discussing those that might be helpful.
My book is aimed at doing just that.
[1] Dr Laurent Schwartz cancérologue iconoclaste — Guérir du Cancer (guerir-du-cancer.fr)
[2] Stub T, Quandt SA, Arcury TA, et al. Perception of risk and communication among conventional and complementary health care providers involving cancer patients’ use of complementary therapies: a literature review. BMC Complement Altern Med. 2016;16(1):353. Published 2016 Sep 8. doi:10.1186/s12906-016-1326-3
[3] Ziodeen KA, Misra SM. Complementary and integrative medicine attitudes and perceived knowledge in a large pediatric residency program. Complement Ther Med. 2018;37:133-135. doi:10.1016/j.ctim.2018.02.004
[4] Schmidt K, Ernst E. Assessing websites on complementary and alternative medicine for cancer. Ann Oncol. 2004;15(5):733-742. doi:10.1093/annonc/mdh174
[5] Milazzo S, Ernst E. Newspaper coverage of complementary and alternative therapies for cancer–UK 2002-2004. Support Care Cancer. 2006;14(9):885-889. doi:10.1007/s00520-006-0068-z
[6] Mills E, Ernst E, Singh R, Ross C, Wilson K. Health food store recommendations: implications for breast cancer patients. Breast Cancer Res. 2003;5(6):R170-R174. doi:10.1186/bcr636
[7] https://edzardernst.com/2013/09/drowning-in-a-sea-of-misinformation-part-8-books-on-alternative-medicine/
[8] https://edzardernst.com/2019/10/leah-blacknell-1964-2019-another-victim-of-cancer-quackery/
____________________________________________
The publication of this book is perhaps the right occasion to publicly thank two regular and one occasional contributor to this blog. I am grateful to
- Prof. Michael Baum, emeritus professor, for writing the foreword,
- Dr. Julian Money-Kyrle, retired consultant oncologist, for his constructive comments on chapter 1.4,
- Richard Rasker for his corrections and advice on the entire text.
Thank you all.
It has been reported that an Australian naturopath would refuse entry to her business to anyone who has received a COVID-19 vaccine in the past two weeks. In her original Facebook post, Ms. Holland said that vaccinated people would have to wait a minimum of two weeks after vaccination before attending her clinic due to “the shedding of spike proteins” caused by “these experimental treatments”.
Christine Pope, who is on the Australian Traditional Medicine Society (ATMS) board of directors, said she believed the views shared by the Warrnambool naturopath were part of the alternative medicine sector’s “fringe” and didn’t represent the industry. “We’re always very careful to tell our practitioners about posting appropriately and within their scope of practice,” Ms. Pope said. “These sort of comments to me look like they’re outside their scope of practice. We do a lot of training about making sure that you’re posting appropriately within your scope of practice and about things about which you are qualified in. As an association supporting natural medicine practitioners, it’s not really our job to promote or comment on the vaccination program – we’re not public health experts … and this is really outside my scope of practice. But from a public health perspective (vaccination) is the best option we’ve got.”
Sharon Holland, who runs a clinic in Warrnambool, cited on Facebook a number of discredited medical professionals who have become figureheads of the anti-vax and COVID conspiracy movements, including Judy Mikovits, Robert Malone, Peter McCullogh, and J Bart Classen. “Often de-bunked and fact-checked (by whom) can mean silenced,” Ms. Holland wrote. “We still have free speech available to some extent. This is a very emotive and divisive subject so my post was bound to ‘ruffle feathers’.”
The ATMS says its accredited practitioners need to “stay within their scope of practice” and avoid posting about vaccines they haven’t studied. Ms. Pope urged people to lodge a complaint about bogus health claims through the ATMS website or the healthcare complaint commissioner in the appropriate state.
___________________________
This course of events begs several questions. In my view, the most important are:
- Is Sharon Holland an exception, or are many/most naturopaths of her opinion?
- Instructing practitioners about “posting appropriately and within their scope of practice” sounds fine but might miss the point entirely. What really matters are the messages ATMS members orally convey to their patients. Is there any evidence on this issue?
- Surely, the anti-vax sentiments of naturopaths must originate from their education. Is there any evidence as to what they are taught about the subject?
- Is the ATMS going to take action against Ms. Holland and other members who endanger the public with their anti-vax stance?
Having recently mentioned that bullshit is accepted as a proper term in scientific circles, I hasten to add that chiropractors often excel in putting out bullshit. Most of us probably knew that but I was reminded of it when reading this paper by an Irish chiropractor who employs nit just spinal manipulations but also offers CranioSacral Technique, Counselling together with Neuro-developmental training, and Pre and Peri-natal education:
There are essential ethical elements required for a chiropractor to establish an authentic professional relationship in order to maintain the integrity of a healing relationship with their patients. Ethically, chiropractors also have an ongoing responsibility to do their own personal and professional development. Therapeutic presence is the capacity to hold a healing space for another person by developing trust and rapport and providing them with a safe energetic container influenced by one’s calm and centered state of being. The Polyvagal Theory provides a neurobiological narrative that focuses on the importance of ‘safety’ and the adaptive consequences of detecting risk on our physiological state, social behavior, psychological experience, and health to achieve presence. To fulfill our biological imperative of connectedness, our personal, professional and ethical agenda needs to be directed toward making patients feel safe in the moment and getting into right-relationship. Recognizing and interpreting the mother/baby dyad’s adaptive behaviors provides an insight into their pre & perinatal imprints which reflect the child’s Baby Body Language patterns.
And here are the rather pithy conclusions of this paper:
Practicing the principles of therapeutic presence requires patience, experience and ongoing commitment as it is an invaluable model or paradigm of conscious awareness for helping others. A chiropractor who chooses the path of self-development to help them be more present for others in each moment, in a space of caring and compassion, would enable them to receive as well as give. The ability to serve in presence for someone else’s healing brings the professional into a deeper state of grace and resonance.
When both the chiropractor and mother/child dyad respect their own individual body’s physiological responses, they move towards a more evaluative state in which they become more respectful of themselves and the treatment outcomes. The PVT provides the neuroscience in understanding the continuum between the physiological states of fight, flight, freeze and dissociation. The application of the ongoing evaluation of these states functionally contributes to the treatment and healing process and facilitates a sound basis for the ongoing connectedness of the mother/child dyad.
The way in which practitioners are grounded in themselves, open to others (while holding appropriate boundaries) and participate fully in the life of the mind and body, are important aspects of practicing therapeutic presence which is at the heart of relationships that help others to grow. This inside-out view helps chiropractors to see the ongoing personal development work they need to do as professionals to develop the essential receptive starting place of therapeutic presence for all clinical encounters.
After having read it several times and repeatedly drowned in this abundant mixture of bullshit and platitude, my main question is this:
DOES ANYONE UNDERSTAND WHAT IT MEANS?
If so, please explain.
I was alerted the these Chiropractic Paediatric Courses. After studying the material, I was truly stunned. Now that I have recovered, I feel I should share it with you:
Chiropaeds Australia is an approved and accredited provider of the Diplomate of Australian College of Chiropractic Paediatrics program.
Diplomate of Australian College of Chiropractic Paediatrics Offered for the first time in 2013, the Diplomate program is a two-year chiropractic paediatric course. This course is ideal for the family chiropractor wanting to improve his or her knowledge in chiropractic paediatrics. The emphasis is on conditions and management issues which are commonly seen by the family chiropractor.
The course is structured around 20 four-week modules over two years. Each module consists of required reading, exercises and at the end of each four-week module there is a six-hour seminar. Each six-hour seminar will reinforce the reading and develop the practical and management skills needed to feel confident in providing optimal chiropractic care for children…
Registration post 31 December – $AUD 6050 (includes GST) This covers the cost of all materials and seminars but does not include any books or texts you may decide to purchase.
To provide you with an impression of the content of the modules, I have chosen three of them. Here they are:

Module 7
Neurological assessment of the infant
1. Neurological examination of the infant (Infanib)
2. Motor issues: diagnosis and chiropractic management
a. Gross motor developmental delay
b. Hyper/ hypotonia
c. Cerebral palsy
It is only by knowing how to assess the infant’s neurological system that you can start to fully appreciate and understand the immense impact of the subluxation. The information covered in this module allows you to demonstrate to your parents the impact the subluxation has on their infant’s nervous system. As a result your subluxation diagnosis, treatment and management with infants will be enhanced. We look at muscle function issues which occur in this age group with particular emphasis on gross motor developmental delay and hyper/hypotonia.
Module 8
Neurological assessment of the pre-schooler and the school aged child
1. Gross motor function
2. Fine motor function
3. Cerebellar function
4. Assessment of higher cognitive functions
5. Visual processing
6. Auditory processing
7. Language development
Syndrome management
1. Auditory processing syndromes
2. Visual processing syndromes
Chiropractic has a major role to play in treating and managing children with learning difficulties. Crucial to optimal outcomes is an ability to fully assess and determine the particular issues and neurological problems your patient experiences. This module is very practical: you will learn how to accurately test cortical and cerebellar function in preschool and school aged children to a very advanced level. Being able to perform extensive testing of learning ability in children will assist you to accurately find and monitor their learning difficulties. The interplay of higher cortical function, cerebellar function and the subluxation is explored and the impact of your consultation assessment routine on the subluxation is addressed. Management of learning difficulties is emphasised.
Module 11
The child’s ear, nose and throat
1. Acute otitis media
2. Chronic otitis media
3. Serous otitis media
4. Nose and throat issues with children
5. Tonsillitis, epiglottitis, coup and neck abscesses
Chiropractors have a key role to play in the treatment and management of otitis media along with other conditions associated with recurrent viral infection as well as decreased or imbalanced immune system function. We cover the diagnosis of each condition along with chiropractic treatment and management, including the interaction of the subluxation and the immune system. Nutritional management is also covered. Key management issues are explored and literature based knowledge is provided to allow you to educate you patient’s parents. This fosters improved compliance with your care and permits you to expand the boundaries of your chiropractic care of children.
____________________________________
I wonder whether some chiropractor feels like defending this outright charlatanry.
I know of no evidence to assume that chiropractors can provide effective care for children. I see, however, many reasons to fear that they may cause considerable harm. I also see no reason to take a profession seriously that tolerates or even supports such extreme quackery.
I have expressed these concerns often enough, e.g.:
- The effectiveness of chiropractic spinal manipulations/mobilisation for children is unproven. TIME TO STOP TREATING KIDS!
- Chiropractic for kids: a ‘complete disregard for the evidence and scientific facts’
- Chiropractic for kids: a pack of offensive lies
- Chiropractic spinal care for children is dangerous, unwarranted and must cease immediately
- Don’t let a chiropractor near your kids!
- Chiro for kids? No!
In my view, it is high time to stop this dangerous nonsense.
Former chiropractor Malcolm Hooper, 61, and hyperbaric oxygen therapy provider Oxymed Pty Ltd have been fined following the death of a customer in 2016. They were each convicted of three work safety-related charges, all of failing to ensure a workplace is safe and without risks to health. Hooper was fined $176,750, while the company was fined $550,000. Oxymed was trading as HyperMed at its South Yarra premises in April 2016 when a long-term client with multiple sclerosis and a history of life-threatening seizures came in for treatment. He was later found unconscious in a single-person hyperbaric chamber, taken to hospital, and placed on life support, but died five days later.
The County Court heard that both the company and Hooper had an inadequate system in place for assessing the risks oxygen therapy could pose to clients, and an inadequate system too for developing plans to eliminate or reduce those risks. In her judgment, County Court judge Amanda Fox said HyperMed wasn’t a hospital nor a medical practice and had been described as an “alternative health facility”. Hooper had already been deregistered in 2013 by the national board for chiropractors for misleading and deceptive advertising about the benefits of hyperbaric treatment.
Hyperbaric oxygen therapy involves administering pure oxygen in a pressurised environment, with the heightened air pressure allowing a patients’ lungs to gather much more oxygen than would be possible under normal conditions. The therapy is not based on strong data. A systematic review failed to find good evidence for hyperbaric oxygen therapy as a treatment of multiple sclerosis:
Multiple sclerosis (MS) is a chronic, inflammatory, and degenerative neurological illness with no cure. It has been suggested that Hyperbaric Oxygen Therapy (HBO(2)T) may slow or reverse the progress of the disease. This article summarizes the clinical evidence for the use of HBO(2)T in the treatment of MS. We conducted a literature review focused on the interaction of hyperbaric oxygenation and MS. In particular, we appraised the clinical data regarding treatment and performed a meta-analysis of the randomized evidence using the methodology of the Cochrane Collaboration. We found 12 randomized studies in the area, all of which were performed between 1983 and 1987. A meta-analysis of this evidence suggests there is no clinically significant benefit from the administration of HBO(2)T. The great majority of randomized trials investigated a course of 20 treatments at pressures between 1.75ATA and 2.5ATA daily for 60-120 min over 4 weeks against a placebo regimen. None have tested the efficacy of HBO(2)T against alternative current best practice. No plausible benefit of HBO(2)T on the clinical course of MS was identified in this review. It remains possible that HBO(2)T is effective in a subgroup of individuals not clearly identified in the trials to date, but any benefit is unlikely to be of great clinical significance. There is some case for further human trials in selected subgroups and for prolonged courses of HBO(2)T at modest pressures, but the case is not strong. At this time, the routine treatment of MS with HBO(2)T is not recommended.
The case reminds me of that of John Lawler. Mr. Lawlwer’s chiropractor also used a therapy that was not indicated, broke his neck (to put it crudely), and subsequently proved herself more than inept in saving his life. It suggests to me that some chiros may not be trained adequately to deal with emergencies. If that is true, they should perhaps focus less on practice-building courses and more on first aid instructions.