Monthly Archives: March 2021
In March 2020, ITV reported that a faith healer has been accused of “exploiting” people’s anxiety about the coronavirus crisis by selling a “plague protection kit” for £91. Bishop Climate Wiseman, head of the Kingdom Church in Camberwell, south London, has promised his followers the small bottle of oil and piece of red yarn will protect them from Covid-19. In a blog post, Bishop Wiseman claimed his concoction of cedar wood, hyssop and scarlet yarn acts as “an invisible barrier to the powers of darkness”. He wrote: “It is by faith that you can be saved from the coronavirus pandemic by covering yourself with the divine plague protection oil and wearing the scarlet yarn on your body. That is why I want to encourage you, if you haven’t done so already, to get your divine plague protection kit today!”
He claimed that the remedy was based on a passage from chapter 14 of the Old Testament Book of Leviticus. It reads: “Then he is to take the cedar wood, the hyssop, the scarlet yarn, and the live bird, dip them into the blood of the dead bird and the fresh water, and sprinkle the house seven times. In this way, he will make atonement for the house, and it will be clean.”
Bishop Wiseman told the PA news agency the church had sold more than 1,000 of the kits. “This is based on the Bible – I’m a Christian and there is a way that the Bible says to protect us from plagues.” One can also buy miracle money house blessing oil and anointed oil for court cases. On the Kingdom Church’s website, it claims thousands of people have been healed from “all sorts” of sickness and disease since it was founded in 2005.
Now, the Charity Commission has appointed an interim manager to the church following concerns raised by the National Secular Society about ‘plague protection kits’ sold by its bishop. England and Wales’s charity regulator announced that it appointed an interim manager to The Kingdom Church GB in February, who will “consider the charity’s future operation and viability”.
Elsewhere, the oil is advertised as follows:
Plagues Divine Protection Anointing Oil Have you been battling with countless amount of fear due to an economical wide spread of plaques and viruses? Then this Anointing Oil is for you.
The Plagues Divine Protection Anointing Oil was created by Master Prophet, Prophet Climate Wiseman through divine guidance and instruction from the Holy Spirit. This oil contains two biblical integrant which is biblically proven to remove plagues of all kind. These two Integrants are Hyssop and Cedar wood. The Bible clearly tells us in the book of Leviticus 14:51-53 “Then he is to take the cedar wood, the hyssop, the scarlet yarn and the live bird, dip them into the blood of the dead bird and the fresh water, and sprinkle the house seven times. He shall purify the house with the bird’s blood, the fresh water, the live bird, the cedar wood, the hyssop and the scarlet yarn. Then he is to release the live bird in the open fields outside the town. In this way he will make atonement for anointedoils
The commission said it had “serious ongoing concerns” about the charity’s administration and the financial relationship with its two subsidiary companies. It found the charity does not have a bank account and charity funds have instead been deposited into the charity’s subsidiaries’ bank accounts. It is investigating the legality of this relationship. The commission only appoints interim managers to charities “after very careful consideration” if there is misconduct or mismanagement in the administration of a charity, or if it is necessary or desirable to protect the charity’s property.
The post originally included claims that “every coronavirus and any other deadly thing” would “pass over” those using the oil and yarn. It was later edited to remove some specific references to coronavirus, but continued to claim people could “be saved from every pandemic” by using the oil and string.
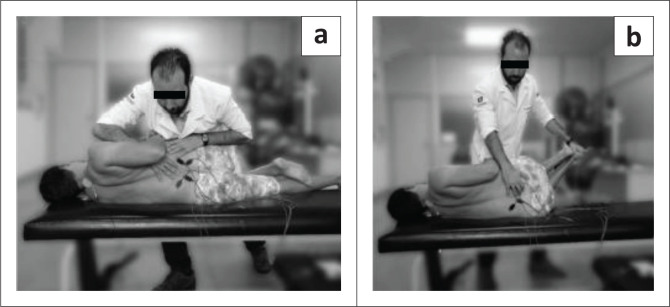
This study compared the effectiveness of two osteopathic manipulative techniques on clinical low back symptoms and trunk neuromuscular postural control in male workers with chronic low back pain (CLBP).
Ten male workers with CLBP were randomly allocated to two groups: high-velocity low-amplitude (HVLA) manipulation or muscle energy techniques (MET). Each group received one therapy per week for both techniques during 7 weeks of treatment.

Pain and function were measured by using the Numeric Pain-Rating Scale, the McGill Pain Questionnaire, and the Roland Morris Disability Questionnaire. The lumbar flexibility was assessed by Modified Schober Test. Electromyography (EMG) and force platform measurements were used for evaluation of trunk muscular activation and postural balance, respectively at three different times: baseline, post-intervention, and 15 days later.
Both techniques were effective (p < 0.01) in reducing pain with large clinical differences (-1.8 to -2.8) across immediate and after 15 days. However, no significant effect between groups and times was found for other variables, namely neuromuscular activation, and postural balance measures.
The authors concluded that both techniques (HVLA thrust manipulation and MET) were effective in reducing back pain immediately and 15 days later. Neither technique changed the trunk neuromuscular activation patterns nor postural balance in male workers with LBP.
There is, of course, another conclusion that fits the data just as well: both techniques were equally ineffective.
A report just published by the UK GENERAL CHIROPRACTIC COUNCIL (the regulator of chiropractors in the UK) entitled Public perceptions research Enhancing professionalism, February 2021 makes interesting reading. It is based on a consumer survey for which the national online public survey was conducted by djs research in 2020 with a nationally representative sample of 1,002 UK adults (aged 16+). From this sample, 243 UK adults had received chiropractic treatment and were surveyed on their experiences of visiting a chiropractor.
Hidden amongst intensely boring stuff, we find a heading entitled Communicating potential risks. This caught my interest. Here is the unabbreviated section:
The findings show that patients want to understand the potential risks of treatment – alongside information on cost, this is the most important factor for patients considering chiropractic care. In fact, having any risks communicated before embarking on treatment scores 83 out of 100 on a scale of importance.
Many patients report receiving this information from their chiropractor. Seventy per cent of those who have received chiropractic treatment agree that risks were communicated before treatment commenced.
What does that suggest?
- Patients want to know about the risks of the treatments chiropractors administer.
- 30% of all patients are not being given this information.
This roughly confirms what has long been known:
MANY CHIROPRACTORS DO NOT OBTAIN INFORMED CONSENT FROM THEIR PATIENTS AND THUS VIOLATE MEDICAL ETHICS.
The questions that arise from this information are these:
- As the GCC has long known about this situation, why have they not adequately addressed it?
- Now that they are reminded of this flagrant ethical violation, what are they planning to do about it?
- What measures will they put in place to make sure that all chiropractors observe the elementary rules of medical ethics in the future?
- What reprimands do they plan for members who do not comply?
Two recent reviews have evaluated the evidence for acupuncture as a means of preventing migraine attacks.
The first review assessed the efficacy and safety of acupuncture for the prophylaxis of episodic or chronic migraine in adult patients compared to pharmacological treatment.
The authors included randomized controlled trials published in western languages that compared any treatment involving needle insertion (with or without manual or electrical stimulation) at acupuncture points, pain points or trigger points, with any pharmacological prophylaxis in adult (≥18 years) with chronic or episodic migraine with or without aura according to the criteria of the International Headache Society.
Nine randomized trials were included encompassing 1,484 patients. At the end of the intervention, a small reduction was found in favor of acupuncture for the number of days with migraine per month: (SMD: -0.37; 95% CI -1.64 to -0.11), and for response rate (RR: 1.46; 95% CI 1.16-1.84). A moderate effect emerged in the reduction of pain intensity in favor of acupuncture (SMD: -0.36; 95% CI -0.60 to -0.13), and a large reduction in favor of acupuncture in both the dropout rate due to any reason (RR 0.39; 95% CI 0.18 to 0.84) and the dropout rate due to adverse event (RR 0.26; 95% CI 0.09 to 0.74). The quality of the evidence was moderate for all these primary outcomes. Results at longest follow-up confirmed these effects.
The authors concluded that, based on moderate certainty of evidence, we conclude that acupuncture is mildly more effective and much safer than medication for the prophylaxis of migraine.
The second review aimed to perform a network meta-analysis to compare the effectiveness and acceptability between topiramate, acupuncture, and Botulinum neurotoxin A (BoNT-A).
The authors searched OVID Medline, Embase, the Cochrane register of controlled trials (CENTRAL), the Chinese Clinical Trial Register, and clinicaltrials.gov for randomized controlled trials (RCTs) that compared topiramate, acupuncture, and BoNT-A with any of them or placebo in the preventive treatment of chronic migraine. A network meta-analysis was performed by using a frequentist approach and a random-effects model. The primary outcomes were the reduction in monthly headache days and monthly migraine days at week 12. Acceptability was defined as the number of dropouts owing to adverse events.
A total of 15 RCTs (n = 2545) could be included. Eleven RCTs were at low risk of bias. The network meta-analyses (n = 2061) showed that acupuncture (2061 participants; standardized mean difference [SMD] -1.61, 95% CI: -2.35 to -0.87) and topiramate (582 participants; SMD -0.4, 95% CI: -0.75 to -0.04) ranked the most effective in the reduction of monthly headache days and migraine days, respectively; but they were not significantly superior over BoNT-A. Topiramate caused the most treatment-related adverse events and the highest rate of dropouts owing to adverse events.
The authors concluded that Topiramate and acupuncture were not superior over BoNT-A; BoNT-A was still the primary preventive treatment of chronic migraine. Large-scale RCTs with direct comparison of these three treatments are warranted to verify the findings.
Unquestionably, these are interesting findings. How reliable are they? Acupuncture trials are in several ways notoriously tricky, and many of the primary studies were of poor quality. This means the results are not as reliable as one would hope. Yet, it seems to me that migraine prevention is one of the indications where the evidence for acupuncture is strongest.
A second question might be practicability. How realistic is it for a patient to receive regular acupuncture sessions for migraine prevention? And finally, we might ask how cost-effective acupuncture is for that purpose and how its cost-effectiveness compares to other options.
The objective of this survey was to determine the prevalence of Osteopathic Manipulative Treatment (OMT) use, barriers to its use, and factors that correlate with increased use.
The American Osteopathic Association (AOA) distributed its triannual survey on professional practices and preferences of osteopathic physicians, including questions on OMT, to a random sample of 10,000 osteopathic physicians in August 2018 through Survey Monkey (San Mateo, CA). Follow-up efforts included a paper survey mailed to nonrespondents one month after initial distribution and three subsequent email reminders. The survey was available from August 15, 2018, to November 5, 2018. The OMT questions focused on the frequency of OMT use, perceived barriers, and basic demographic information of osteopathic physician respondents. Statistical analysis (including a one-sample test of proportion, chi-square, and Spearman’s rho) was performed to identify significant factors influencing OMT use.
Of 10,000 surveyed osteopathic physicians, 1,683 (16.83%) responded. Of those respondents, 1,308 (77.74%) reported using OMT on less than 5% of their patients, while 958 (56.95%) did not use OMT on any of their patients. Impactful barriers to OMT use included lack of time, lack of reimbursement, lack of institutional/practice support, and lack of confidence/proficiency. Factors positively correlated with OMT use included female gender, being full owner of a practice, and practicing in an office-based setting.
The authors concluded that OMT use among osteopathic physicians in the US continues to decline. Barriers to its use appear to be related to the difficulty that most physicians have with successfully integrating OMT into the country’s insurance-based system of healthcare delivery. Follow-up investigations on this subject in subsequent years will be imperative in the ongoing effort to monitor and preserve the distinctiveness of the osteopathic profession.
What can one conclude from a three-year-old survey with a 17% response rate?
The answer is almost nothing!
Yet, it seems fair to say that OMT-use by US osteopaths is not huge. It might even be fair to speculate that, in reality, it is smaller than 17%. It stands to reason that the non-responders in this survey were the ones who could not care less about OMT. I would argue that this would be a good thing!
On 20 February 2021, I published on my blog a comment on a new study of an Ayurvedic remedy for COVID-19. The study was in my view suspect, and I expressed this as follows:
I have the following concerns or questions about this trial:
- Why do the authors call it a pilot study? A pilot study is merely for testing the feasibility of a trial design and is not meant to yield definitive efficacy results.
- The authors state that the patients were asymptomatic yet in the discussion they claim they were asymptomatic or mildly symptomatic.
- Some of the effect sizes reported here are extraordinary and seem almost too good to be true.
- The claim of no adverse effect is implausible; even placebos would cause perceived adverse effects in a percentage of patients.
- If the study is solid and withstands the scrutiny of the raw data, it is of huge relevance for public health. So, why did the authors publish it in PHYTOMEDICINE, a relatively minor and little-known journal?
An article in The Economic Times’ reported this:
Patanjali Ayurved released what it called the first “evidence-based” medicine for Covid-19 on Friday. It claimed it has been “recognised by the WHO (World Health Organization) as an ayurvedic medicine for corona”. Patanjali promoter, yoga guru Baba Ramdev, released a scientific research paper in this regard at the launch, presided over by Union health minister Harsh Vardhan and transport minister Nitin Gadkari. The Ayurveda products maker said it has received a certification from the Ayush ministry. “Coronil has received the Certificate of Pharmaceutical Product (CoPP) from the Ayush section of Central Drugs Standard Control Organisation (CDSCO) as per the WHO certification scheme,” it said in a statement. Under the CoPP, Coronil can be exported to 158 countries, the company said, adding that based on the presented data, the ministry has recognised Coronil as medicine for “supporting measure in Covid-19”.
Am I the only one who fears that something is not entirely kosher about the study? (This is an honest question, and I would be pleased to receive answers from my readers)
What happened next is most puzzling. After putting it on Facebook several times, I got banned for 72 hours from posting this article or anything else on Facebook. When this period had elapsed, I put the article in question again on Facebook. Subsequently, I was banned again but this time for 7 days. Facebook gave the following explanation:
You can’t post or comment for 7 days
This is because your previous posts didn’t follow our Community Standards.
No one else can see these posts.
1 Mar
Your post goes against our Community Standards on misinformation that could cause physical harm
We usually offer the chance to request a review, and follow up if we’ve gotten decisions wrong.
We have fewer reviewers available at the moment because of the coronavirus (COVID-19) outbreak. We’re trying hard to prioritise reviewing content with the most potential for harm.
This means that we may not be able to follow up with you, though your feedback helps us do better in the future.
Thank you for understanding.
On Twitter, the hype had begun even before its text was available. Priti Gandhi, for instance, tweeted:
Yet another feather in India’s cap!! 1st evidence-based, CoPP-WHO GMP certified medicine for Covid-19 released today. Congratulations to @yogrishiramdev ji, @Ach_Balkrishna ji & the team of scie…
EDZARDERNST.COM An RCT on the efficacy of ayurvedic treatment on asymptomatic COVID-19 patients
________________________________
As I did not feel I had broken any rules, I protested against the bans each time. When the 2nd ban was over, I posted my article yet again and, sure enough, yesterday I got banned again, this time for 30 days. Here is how they let me know:
You can’t post or comment for 30 days
This is because you previously posted something that didn’t follow our Community Standards.
This post goes against our standards on misinformation that could cause physical harm, so only you can see it.
Learn more about updates to our standards. On Twitter, the hype had begun even before its text was available. Priti Gandhi, for instance, tweeted: Yet another feather in India’s cap!! 1st evidence-based, CoPP-WHO GMP certified medicine for Covid-19 released today. Congratulations to @yogrishiramdev ji, @Ach_Balkrishna ji & the team of scie…
EDZARDERNST.COM An RCT on the efficacy of ayurvedic treatment on asymptomatic COVID-19 patients
As the reason for the ban always seems to be the Ayurvedic study, I suspect that some party interested in the product is behind the complaints that lead to the bans. I find it extraordinary that I can be banned repeatedly without having done anything wrong and without my objections ever being considered.
This recent article is truly remarkable:
There is a faction within the chiropractic profession passionately advocating against the routine use of X-rays in the diagnosis, treatment and management of patients with spinal disorders (aka subluxation). These activists reiterate common false statements such as “there is no evidence” for biomechanical spine assessment by X-ray, “there are no guidelines” supporting routine imaging, and also promulgate the reiterating narrative that “X-rays are dangerous.” These arguments come in the form of recycled allopathic “red flag only” medical guidelines for spine care, opinion pieces and consensus statements. Herein, we review these common arguments and present compelling data refuting such claims. It quickly becomes evident that these statements are false. They are based on cherry-picked medical references and, most importantly, expansive evidence against this narrative continues to be ignored. Factually, there is considerable evidential support for routine use of radiological imaging in chiropractic and manual therapies for 3 main purposes: 1. To assess spinopelvic biomechanical parameters; 2. To screen for relative and absolute contraindications; 3. To reassess a patient’s progress from some forms of spine altering treatments. Finally, and most importantly, we summarize why the long-held notion of carcinogenicity from X-rays is not a valid argument.
Not only is low dose radiation not detrimental, but it also protects us from cancer, according to the authors:
Exposures to low-dose radiation incites multiple and multi-hierarchical biopositive mechanisms that prevent, repair or remove damage caused mostly by endogenous reactive oxygen species (ROS) and H2O2 from aerobic metabolism. Indeed, non-radiogenic (i.e. naturally occurring) molecular damage occurs daily at rates many orders of magnitude greater than the rate of damage caused by low-dose radiation such as diagnostic X-rays. It is estimated that the endogenous genetic damage caused on a daily basis from simply breathing air is about one million times the damage initially resulting from an X-ray. We concur that “it is factually preposterous to have radiophobic cancer concerns from medical X-rays after considering the daily burden of endogenous DNA damage.”
And, of course, radiological imaging makes sense in cases of non-specific back pain due to ‘malalignment’ of the spine:
Pressures to restrict the use of “repeat” (i.e. follow-up) X-rays for assessing patient response to treatment shows a complete disregard for the evidence discussed that definitively illustrates how modern spine rehabilitation techniques and practices successfully re-align the spine and pelvis for a wide variety of presenting subluxation/deformity patterns. The continued anti-X-ray sentiment from “consensus” and opinion within chiropractic needs to stop; it is antithetical to scientific reality and to the practice of contemporary chiropractic practice. We reiterate a quote from the late Michael A. Persinger: “what is happening in recent years is that facts are being defined by consensus. If a group of people think that something is correct, therefore it’s true, and that’s contradictory to science.”
Thus, the authors feel entitled to conclude:
Routine and repeat X-rays in the nonsurgical treatment of patients with spine disorders is an evidence-based clinical practice that is warranted by those that practice spine-altering methods. The evidence supporting such practices is based on definitive evidence supporting the rationale to assess a patient’s spinopelvic parameters for biomechanical diagnosis, to screen for relative and absolute contraindications for specific spine care methods, and to re-assess the spine and postural response to treatment.
The traditional and underlying presumption of the carcinogenicity from X-rays is not a valid notion because the LNT is not valid for low-dose exposures. The ALARA radiation protection principle is obsolete, the threshold for harm is high, low-dose exposures prevent cancers by stimulating and upregulating the body’s innate adaptive protection mechanisms, the TCD concept in invalid, and aged cohort studies assumed to show cancers resulting from previous X-rays are not generalizable to the wider population because they represent populations predisposed to cancers.
Red flags, or suspected serious underlying disease is a valid consideration warranting screening imaging by all spine care providers. We contend, however, that as long as the treating physician or rehabilitation therapist is practicing evidence-based methods, proven to improve spine and postural parameters in order to provide relief for the myriad of spinal disorders, spinal X-rays are unequivocally justified. Non-surgical spine care guidelines need to account for proven and evolving non-surgical methods that are radiographically guided, patient-centered, and competently practiced by those specialty trained in such methods. This is over and above so-called “red flag only” guidelines. The efforts to universally dissuade chiropractors from routine and repeat X-ray imaging is neither scientifically justified nor ethical.
There seems to be just one problem here: the broad consensus is against almost anything these authors claim.
Oh, I almost forgot: this paper was authored and sponsored by CBP NonProfit.
“The mission of Chiropractic BioPhysics® (CBP®) Non-Profit is to provide a research based response to these changing times that is clinically, technically, and philosophically sound. By joining together, we can participate in the redefinition and updating of the chiropractic profession through state of the art spine research efforts. This journey, all of us must take as a Chiropractic health care profession to become the best we can be for the sake of the betterment of patient care. CBP Non-Profit’s efforts focus on corrective Chiropractic care through structural rehabilitation of the spine and posture. Further, CBP Non-Profit, Inc. has in its purpose to fund Chiropractic student scholarships where appropriate as well as donate needed chiropractic equipment to chiropractic colleges; always trying to support chiropractic advancement and education.”