The debate what might be the optimal treatment of back pain has been going on for many years. This new study provides important further insights.
The RCT assessed the comparative effectiveness of adding spinal manipulative therapy (SMT) or supervised rehabilitative exercise to home exercise in adults 65 or older suffering from sub-acute or chronic low back pain (LBP). Treatments were provided over 12-weeks and self-report outcomes were collected at 4, 12, 26, and 52 weeks. The primary outcome was pain severity. Secondary outcomes included back disability, health status, medication use, satisfaction with care, and global improvement. Linear mixed models were used to analyse outcomes. The primary analysis included longitudinal outcomes in the short (week 4–12) and long-term (week 4–52). An omnibus test assessing differences across all groups over the year was used to control for multiplicity. Secondary analyses included outcomes at each time point and responder analyses. This study was funded by the US Department of Health and Human Services, Health Resources and Services Administration.
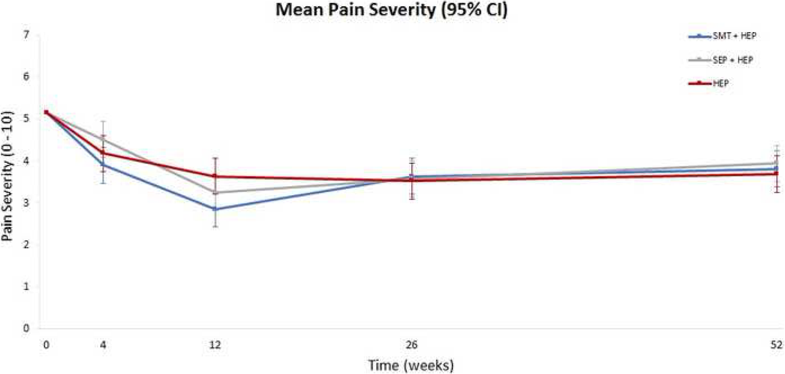
A total of 241 participants were randomized and 230 (95%) provided complete primary outcome data. The primary analysis showed group differences in pain over the one-year were small and not statistically significant. Pain severity was reduced by 30 to 40% after treatment in all 3 groups with the largest difference (eight percentage points) favouring SMT and home exercise over home exercise alone. Group differences at other time points ranged from 0 to 6 percentage points with no consistent pattern favouring one treatment. One-year post-treatment pain reductions diminished in all three groups. Secondary self-report outcomes followed a similar pattern with no important group differences, except satisfaction with care, where the two combination groups were consistently superior to home exercise alone.
The authors concluded that adding spinal manipulation or supervised rehabilitative exercise to home exercise alone does not appear to improve pain or disability in the short- or long-term for older adults with chronic low back pain, but did enhance satisfaction with care.
It is rare to find such a well designed, conducted and reported study in the realm of SCAM. Its results are clear and show that SMT offers no benefit over exercise in this LBP population. The better satisfaction rate with SMT is to be expected; it is probably due to the extra attention this option offers. The most recent systematic review addressing non-pharmacologic treatments for chronic LBP has found evidence of modest short-term improvements in function and/or pain for both exercise and SMT when compared to usual care, attention control, sham, or placebo, and no clear differences between exercise and SMT. In view of the facts that
- SMT might cause adverse effects,
- exercise is cheaper,
- exercise conveys benefits beyond back pain,
the new findings are a very clear verdict: exercise is preferable to SMT in the treatment of LBP.
None of the groups had achieved MTB at 12 weeks. Hence, one could say they stopped the interventions too early in the course of care. Would extending the care to MTB change the outcome? Unknown at this time.
Also note the population they studied…”…65 or older with sub-acute or chronic LBP.”
Also note that a majority also complained of neck pain. In a clinical setting one would most likely address this complaint as well. But that gets into addressing kinematic compensations in a closed chain….an area in need of research.
Also, AE events can occur with exercise. Example…
Fifty-three trials (44%) had no comments at all on AEs, 25 (21%) reported no AEs happened, and 43 (36%) reported some types of AEs. Among these 43 trials, 27 reported events that were musculoskeletal related (ie, muscle strain, bruising, or joint pain), 5 trials reported falls, 5 trials reported cardiovas- cular reactions (ie, increased blood pressure, arrhythmia, myo- cardial infarction), and 4 trials reported illness (ie, aggravation of existing arthritis).
Adverse Events Reported in Progressive Resistance Strength Training Trials in Older Adults: 2 Sides of a Coin. Arch Phys Med Rehabil Vol 91, September 2010
But since some have passed the verdict…
@DC: you have a myriad of excuses, explanations and apologies for your religious endeavor. Perhaps, in light of your capacious defenses YOU ought to be spending some of your donations in the pursuit of publishing research that proves what YOU obviously conclude is true….but no one else’s research can uncover: that YOU indeed know precisely what you’re doing BUT “those” researchers just don’t have the proper acumen to show it.
It is indeed easy to sit back and regularly critize negative-results as “wrong or unknown” while offering up none of your own. It is YOU who is responsible to over-come the null…..IF in fact this waste-of-resources-religion is to ever be seen as anything but a pseudoscience. You do have 15,000 close quacks all taking donations daily? Perhaps instead of buying toys that makes you look like a real-doctor put some aside and prove something. Until then the verdict IS indeed in….and it is seems to be ‘with prejudice’. Ehh?
If my pointing out the limitations and issues of a study (there are others i didnt mention) somehow bothers you Michael, well, thats your problem.
your pointing out the limitations and issues of this study does not bother me at all.
however, I still think it is a rigorous trial and fail to see many SMT studies that are better. can you name one?
How about addressing this.
How often do manual therapists stop treatment for subacute or chronic LBP even though the patient is showing signs of improvement?
I suggest you answer my query before you ask questions.
Actually, i was repeating from my original post….which has yet to be addressed.
Manual therapy might well have a part to play in supporting patients while nature takes its course.
But what is it that ‘chiropractic’ does that physiotherapy cannot?
In other words, what is the point of a chiropractor?
Thank you.
as far as therapeutics, there is little difference, other than in some areas PTs cannot do spinal manipulation.
also, in some areas, PTs cannot order or read imaging and make a diagnosis based up such findings.
also, in some areas, PTs cannot alter a treatment plan, only the referring physician can do that.
also, in some areas, PTs cannot treat a Medicare patient without a referral from a MD or DO.
Indeed, an interesting study… The senior population health requirements have changed dramatically in the past twenty years and it requires us to think and practice differently. Back in 2010 I arranged a day seminar with spine surgeons, pain specialists, physios, osteopaths and chiropractors all devoted to the “elderly spine”. Back than there was little literature aimed at that age group and I am glad this is changing.
As always with RCTs I believe in “show me your patient selection and I will show you your end results”… we know that those patients with increase axial pain in extension and rotation positions (Kemp test) have negative response to lumbar SMT. Since at that age group a lot of axial pain is due to facet arthritis and since these patients with positive Kemp test were not excluded from SMT the results are as can be expected.
DC. is right by saying that these cases are always slow to respond but also, they require other techniques in addition to or exclusive from SMT.
With regard to the conclusion “exercise is preferable to SMT in the treatment of LBP” I will respectfully avoid any comment ?
you speak as though you have conducted dozens of clinical trials. the truth, however, is that you have not done a single one – or am I wrong?
As we learn from these chats you are never wrong professor!!!
I fail to see your point but let’s role…
I took part in one RCT, I am invited to numerous conferences and I speak about clinical Chiropractic in the Tel Aviv University medical school postgraduate courses.
My main practice is clinical work. If there was a Chiropractic academy in Israel or any form of grants system to support such studies I guess things would have been different.
Now please let me ask you in return… how many patients do you see a week? In what form of clinical practice are you involved in?
fair question!
I am retired since 2012/3
before that I was a clinical researcher for 25 years
before that I was in charge of one of the largest outpatient departments at the university of Vienna
so, perhaps I have seen more patients than you ever will.
… as you say: I am never wrong!
@faux-doctor G: so if you “speak on clinical chiropractic”, perhaps you could finally enlighten us as to WHAT Chiroquackery really IS? NONE of the othe DCs who bloviate here seem to know. The study said the chiroquacker was allowed to choose the most appropriate treatment e.g. SMT, Drop-table or flexion-distraction (what a shame the profound “Activator” was excluded…THAT would have really cured some patients!). So are we to conclude chiroquackery is simply any entrepreneurial-theatric aimed at the spine?? Or is it just these 3? And are these all validated in terms of who, what, when and where? The “determinations” as to which theatric utilized by the study faux-doctors wasn’t expounded on. Does each clown-college teach a different set of theatrics? And “tests” to sucker the gullible? Still anxiously waiting on the insights from those of you speaking on and dispensing the sempiternal Big Idea.
I am sorry professor… when a clinician tells me “I am never wrong” I tend to RUN…I hope and believe you are not serious
SO YOU ALSO DO NOT UNDERSTAND IRONY!
🙂 I am also not perfect…
This article demonstrates ignorance of the multiple approaches modern Chiropractic provides, from gentle therapy, exercise rehabilitation and other physical therapies, much less soft tissue, sports medicine, ergonomics and nutrition. A combination of these is obviously better than exercise rehabilitation alone.
Shame on you for being so one sided and printing negative, anti Chiropractic propaganda rather than doing real research.
Chiropractors are Doctors. Their scope of practice include judicious use of manipulation, but also nutrition, soft tissue techniques, exercise rehabilitation physical therapies, ergonomics and self help counselling. And the risk of Chiropractic care is so far less than with surgery and drugs.
One wonders why such a negative article was even written by an educated doctor who is ignorant of all the rats, muck less printed.
“Chiropractors are Doctors”
dream on!
EE: “Chiropractors are Doctors”
dream on!
Who decides the criteria for a profession to use the title Doctor?
What is the universally accepted definition of Doctor?
True, chiropractors are not:
Doctors of Medicine
Doctors of Osteopathy
Doctors of Physical Therapy
Doctors of Optometry
Doctors of Dentistry
So, is OK for all of those professions to use the title Doctor, but not chiropractors? If so, why?
@faux-doctor G: You may want to look up the definitions of those genuine-professions. They all have reputable, science based connotations and dennotations. Are you actually suggesting a made-up portmanteau like “Chiro-Practic” a.k.a chiroquackery….is analogous to DENTISTRY (Latin: of or pertaining to teeth)? Oh dear, a “doctorate” in a made up play thing. They really should add a few critical-thinking courses into clown college along with the applied kinesiology, leg-check, motion-palpation and insurance fraud classes.
You didnt answer my first two questions…try again.
@DC
It seems that, in North America, anyone wearing a clean white coat feels entitled to be called ‘doctor’. Other countries have tighter controls and barriers. Of course, in the USA Doctors of Osteopathy undergo virtually identical training to medical doctors, but osteopathy in Europe, for example, is a joke pseudo-medicine similar to chiropractic.
You didn’t answer my questions.
@DC
Fair enough. “Who decides the criteria for a profession to use the title Doctor?” There is no absolute
here. The fact that the answer varies between countries indicates that it’s more a question of culture, history and tradition than anything else. My own background (UK) means my intuitive feel for the answer will be different from someone in (e.g.) the USA.
However, there does seem to be a general rationale that the title ‘doctor’ should be reserved for someone who’s done something special; a long way above average. But the confusion (entirely thanks to to North America, as far as I can see) that anybody who diagnoses and treats any form of disease is entitled to be called ‘Doctor’ seriously muddies the waters. That results in even ‘professions’ that are based on unproven (and sometimes ludicrous) raisons d’etre having their practitioners styled ‘doctor’.
The public conception of a ‘doctor’ in most of the world appears to be ‘a person who can deal expertly with any medical condition’. But this can only result in confusion when someone who’s an expert on, say, medieval history is entitled to call themself ‘doctor’ because they have a PhD. Please note that my definition (a person who can deal expertly with any medical condition) would rule out the title of ‘doctor’ for dentists, optometrists and physical therapists.
I guess that the ultimate criterion could be that, when a call goes out on an aircraft in flight “is there a doctor on board” then only someone knowledgeable enough to deal with a genuine medical emergency would respond. No dentists, optometrists, physiotherapists, homeopaths, reiki masters, astrologers or ministers of religion — oh, or chiropractors — should be expected to respond to this call.
But, of course, you might want well qualified paramedics or nurses to respond. As ever, it’s a gray area.
So, DC, (as you knew perfectly well when you posed the question) the answer is a blur of expectations. One short response to “Who decides the criteria for a profession to use the title Doctor?” is “governments”. But all governments pass the problem on to ‘experts’, which — in practice — means those who lobby governments most successfully. That’s why, in some countries, chiropractors have pushed themselves into the position of ‘primary contact physicians’, while other, equally ridiculous pseudo-physicians (reiki masters, ear candlers, faith healers, iridologists, homeopaths, reflexologists and many more) have not.
Your second question: “What is the universally accepted definition of Doctor?” as you knew when you posed it and as is obvious from my response to your first question, is that there ain’t no such thing. The question is about as relevant as “what is the universally accepted definition of god?” or “what is the universally accepted definition of morality?” or “what is the universally accepted definition of a great movie?”. You’re trolling, DC, whether you realize it or not. You’re posing unanswerable riddles and taking pleasure in seeing the rest of us squirming on your hook.
So let me ask you a question. If you suffered a medical emergency on board an aeroplane that fell beyond the competence of the cabin crew to deal with, what kind of doctor would you most welcome coming forward to offer help?
Frank Odds
One a plane ?? Whats a doctor going to do for anybody other than take vital signs, or perform some CPR…. this does not require a “DOCTOR” …perhaps to advise to keep cool or warm, give oxygen…. nothing more.
… or administer one of the many injections that the stewards have on board.
The one most qualified to deal with the situation.
And yes, that may be a chiropractor or a dentist as we have more training than a computer salesperson or grandma on vacation.
Or should i just sit quietly while some fool does CPR for a head wound?
Frank,
Your “person who can deal expertly with any medical condition”, sadly, does not exist. Modern medical doctors refer patients to other practitioners all the time – to those better qualified, or with better experience, or if the condition doesn’t match their particular expertise.
And yet, I (and probably most people) still comfortably calling them ‘doctors’.
Again, our resident trolls reveal their total lack of knowledge and insight in medicine and health care.
EE…or administer one of the many injections that the stewards have on board.
If that is the best course of treatment for the condition, OK.
oh no, we doctors give intra-cardiac injections of adrenaline even for back pain and indigestion
Bjorn… Again, our resident trolls reveal their total lack of knowledge and insight in medicine and health care.
So Bjorn, taking the medical emergency on a plane scenario, is it your view that a chiropractor should not respond to “is there a doctor onboard?” even though all the other passengers on the plane barely passed high school biology?
@DC
“So Bjorn, taking the medical emergency on a plane scenario, is it your view that a chiropractor should not respond to “is there a doctor onboard?” even though all the other passengers on the plane barely passed high school biology?”
Obviously, I can’t speak for Bjorn, but since the scenario I raised seems to have attracted some attention, you might like to consider this: according to this 2013 article in the New England Journal of Medicine, the most common problems precipitating in-flight medical emergencies were “syncope or presyncope (37.4% of 11,920 cases analysed), respiratory symptoms (12.1%), and nausea or vomiting (9.5%).” Cardiac symptoms accounted for 7.7% and seizures for 5.5%.
From the same article: “On-board assistance was provided by physicians (48.1%), nurses (20.1%), EMS providers (4.4%), or other health care professionals (3.7%).” I presume chiropractors fall into that last category. (The article doesn’t state explicitly but I presume the cabin crew themselves accounted for the assistance given in the other 23.7% of cases.)
The article goes on to provide details for dealing with the in-flight emergencies. Interestingly, in the present context, none of these involve spinal manipulation.
For a more lighthearted treatment of the in-flight/doctor situation, you might turn to this piece from Reddit. It opens with “Plane emergency — ‘Are there any doctors on board?’ Would you want an MD or a Chiropractor to raise their hand?” The short piece goes on (satirically) to suggest that all an MD could do is call 911, while a chiro can “adjust the nervous system allowing the brain to better communicate with the body…”
The extensive comments that follow include many humorous digs at both MDs and chiros, but one serious comment (from a chiro) stood out for me: “One emergency procedures class does not prepare or qualify you to actually be able to help in an emergency. Your chiropractic education, at no point, prepared you to deal with a life threatening emergency.” I assume our resident set of chiropractic defenders will claim this is nonsense.
From a cardiolpgist friend of mine here: https://www.docsopinion.com/2017/10/23/in-flight-medical-emergencies/
I seriously doubt that more than perhaps a handful of chiropractors are competent to make a professional medical evaluation of any of these conditions. Flight attendants are trained to respond to most emergencies and they want professional up to date assistance (doctor, nurse or at least an EMT) when they call for a doctor, not a manual therapist with an overinflated ego.
correct!
I know a little bit about this because I have been assed to deal with in-flight emergencies on 2 occasions.
Mr. Edzard
“… or administer one of the many injections that the stewards have on board.”
The airlines don’t have a complete list of injections on board…. there are a couple or three. While it is true that the airlines employees won’t inject anybody unless directed to by a physician, it does not require a physician to inject anyone for anything. I inject my wife with B-complex from time to time. If I’m not available, she has injected herself many times. As stated on the forum previously many times in other threads, most injections are intended for muscle mass…. easy peasy.
you are talking a lot of nonsense!
why?
Bjorn…Flight attendants are trained to respond to most emergencies and they want professional up to date assistance (doctor, nurse or at least an EMT) when they call for a doctor, not a manual therapist with an overinflated ego.
My prior comment…The one most qualified to deal with the situation.
So the next time I come across a medical emergency I will stand amongst the crowd, watch and hope for a good outcome. Got it.
@DC
You can perhaps tell us how chiropractic schooling prepared you, or any chiropractor for a medical emergency aboard an airliner, let’s say an unconscious person.
Also, what are the requirements for maintenance training in medical emergency response and resuscitation for chiropractors?
Another thing, One of the roles of a doctor responding on board is to advise the captain on whether diversion is warranted. That can be a very costly decision either way. Do you think an insurance company would be happy to discover that a chiropractor had introduced himself as “doctor” and given advice of this sort?
Probably the main benefit of a doctor over a chiropractor in this situation is that the doctor will have spent time at some point in their career working with acutely sick patients in hospital and will recognise the signs of a pneumothorax, myocardial infarction, seizure, internal bleeding, anaphylaxis, hypoglycaemic coma or whatever and will have treated it previously. A paramedic, however, who is dealing with these problems on a daily basis and is used to being the first person on the scene of an emergency, might be a better bet.
Unfortunately the facilities, drugs and medical equipment available on a plane are limited, and also there is very little space, so there is only so much that you can due for somebody who is acutely sick. One important job is to make sure that when the plane lands the ambulance waiting on the tarmac is prepared for the specific problem they are going to have to deal with.
I have personally had to deal with emergencies twice. One was a young man who was unconscious and having multiple seizures, on the way from the Caribbean to Holland, and I suspect he may have been a drugs mole with a leak in one of his swallowed condoms, which is nearly always fatal. The other was a woman who was unconscious, white and pulseless, but who thankfully turned pink and started breathing when we laid her flat. The flight attendant had been a nurse and we found that we had worked in the same hospital, so she was keen to catch up on the gossip… But I did have to make the decision to continue to London rather than make an emergency landing in Bombay.
In neither case did I get any follow-up, so I never knew what had happened to these people.
Bjorn…You can perhaps tell us…
I already told you I would just stand back and watch along side the computer salesman and grandma. That’s apparently what you want us to do.
So the conclusion is that the word doctor in doctor of chiropractic does not mean that those advertising such a title are not competent to respond to a call for a doctor in a medical emergency.
That settles the question, I guess.
EE…So the conclusion is that the word doctor in doctor of chiropractic does not mean that those advertising such a title are not competent to respond to a call for a doctor in a medical emergency.
We are not medical doctors, so no. Plus I don’t think I ever said we were as competent as medical providers in an emergency situation.
Sorry to faux-doctor G….faux doctor DC. But you all need a lot more real philosophy and lot less Big Idea faux-philosophy.
If so how is it so much easier to have qualifications to train as chiropractor. It has always been 3 A level grade A ( for as long as we have hd A level- or at lest for a very long time). For Chiro it is much lower and you do not need 3 subjects in science.
@Jay: “a combination of these is better than exercise alone”. In regards your income-stream that would seem indubitable. As far as an evidence-based, research-proven claim it is undoubtedly dubious.
And since making a claim-of-efficacy keeps the burden-of-proof on the claim-maker (that would be YOU) asking the professor why HE isn’t doing YOUR research is a wee bit dopey? I say shame on Jay today, hey, hey.
Are they still carrying on about not being doctors???
Now, if anyone wants to actually address the OP paper and/or the general topic of chronic low back pain in the elderly and/or the options that are available to them and/or why, when and where spinal manipulation may or may not be a viable option and/or how to get them to safely exercise and/or which exercise are most appropriate for which condition, etc.
Enlighten me…
Its not even guessing is it? I know homeopaths like that
@DC: you need only look to the true scientific innovators in chiroquackery: those having discovered the “short-leg” analysis, the PI/AS, atlas-misalignments, AK muscle and stress-challenges, x-ray line drawing, subluxation-posture-patterns and of course intervertebral motion-palpation to deduce “fixations”. There’s your enlightenment.
But as has been asked a 1000 times before: what is it that YOU do? And WHAT is chiropractic really….if not all these gypsy tricks?
As I have explained before, what I do depends on the patient in front of me, their complaints, the findings of an exam, their goals, my experience, what the best research says…melded together to form a clinical plan for a short term trial of care.
woob