A survey was commissioned in 2015 to obtain general population figures for practitioner-led CAM use in England, and to discover people’s views and experiences regarding access.
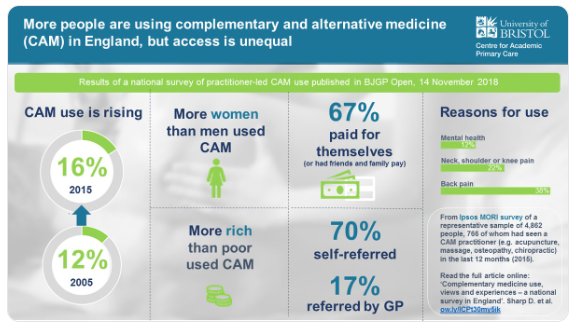
Of 4862 adults surveyed, 766 (16%) had seen a CAM practitioner. People most commonly visited CAM practitioners for manual therapies (massage, osteopathy, chiropractic) and acupuncture, as well as yoga, pilates, reflexology, and mindfulness or meditation. Women, people with higher socioeconomic status (SES) and those in south England were more likely to access CAM. Musculoskeletal conditions (mainly back pain) accounted for 68% of use, and mental health 12%. Most was through self-referral (70%) and self-financing. GPs (17%) or NHS professionals (4%) referred and/or recommended CAM to users. These CAM users were more often unemployed, with lower income and social grade, and receiving NHS-funded CAM. Responders were willing to pay varying amounts for CAM; 22% would not pay anything. Almost two in five responders felt NHS funding and GP referral and/or endorsement would increase their CAM use.
The authors concluded that CAM use in England is common for musculoskeletal and mental health problems, but varies by sex, geography, and SES. It is mainly self-referred and self-financed; some is GP-endorsed and/or referred, especially for individuals of lower SES. Researchers, patients, and commissioners should collaborate to research the effectiveness and cost-effectiveness of CAM and consider its availability on the NHS.
The table below shows the percentage figures for specific CAMs (right column).
| Type of CAM practitioner | n | % |
| Massage practitioner | 143 | 19 |
| Osteopath | 91 | 12 |
| Acupuncturist | 88 | 11 |
| Chiropractor | 87 | 11 |
| Yoga teacher | 52 | 7 |
| Physiotherapist-delivered CAM | 41 | 5 |
| Pilates teacher | 28 | 4 |
| Reflexologist | 22 | 3 |
| Meditation and/or mindfulness teacher | 20 | 3 |
| Homeopath | 20 | 3 |
| Reiki practitioner | 17 | 2 |
| Hypnotherapist | 15 | 2 |
| Herbalist | 14 | 2 |
| Chinese herbal medical practitioner | 12 | 2 |
| Other | 74 | 10 |
Our own survey suggested that, in 2005, the 1-year prevalence of CAM-use in England was 26.3 % and the practitioner-led CAM-use was 12.1 %. The two surveys are, however, not comparable because they did use different methodologies; for instance, they included different types of CAM. I therefore think that any conclusion of an increase in practitioner-led CAM-use between 2005 and 2015 is not warranted. It also follows that the graphic below is misleading.
In the discussion, the authors of the new survey make the following point: Ability to pay may be a factor in accessing CAM (indicated by the association of CAM use with higher SES; lower SES responders being more likely to be GP-referred to CAM; and responders stating that they may use more CAM if the NHS provided services, and GPs endorsed and/or referred them). Integration of CAM into the NHS through primary care could promote continuity of care, safety, and balance of power. An integrative medicine approach includes many of the values recently included in UK health policy documents; for example, Five Year Forward View. It is patient-centred, as discussed in 2010, focuses on prevention, and emphasises patient self-management and person- and community-centred approaches to health and wellbeing. Many of these values underpin social prescribing, which is an increasingly popular model of health care. There seems to be significant patient demand for CAM and more holistic approaches, and a view that CAM may improve patient satisfaction.
I have in a previous post commented on prevalence surveys: the argument that is all too often spun around such survey data goes roughly as follows: a large percentage of the population uses alternative medicine; people pay out of their own pocket for these treatments; they are satisfied with them (if not, they would not pay for them). BUT THIS IS GROSSLY UNFAIR! Why should only those individuals who are rich enough to afford alternative medicine benefit from it? ALTERNATIVE MEDICINE SHOULD BE MADE AVAILABLE FOR ALL.
To me, it is obvious that this line of argument is dangerously wrong. It lends itself to the promotion of unproven therapies to the detriment of good healthcare and progress. Sadly, I fear that the new survey is going to be misused in this way.
As is nearly always the case with this type of article, the authors conflate some modalities which probably do provide benefit for some patients, with those which certainly do not (other than non-specific placebo effects).
This skews their results from the get go, and the publication of such an article merely serves to strengthen the widely held opinion that this journal promotes quackery. Sigh.
Massage can help some musculo-skeletal conditions; some osteopaths do massage, but unless it can be shown that manipulating the skeleton has an effect on tissue vascularity, that ain’t osteopathy; likewise, unless adjustments can be shown to have released ‘innate intelligence’, that ain’t chiropractic; yoga and meditation, shorn of their esoteric elements and fake rationales, do help many folks, as does hypnosis.
(Indeed, I contend that placebo effects generated by CAM modalities result from auto-hypnosis, facilitated by an empathic practitioner.)
The modalities in above paragraph should not be regarded as ‘CAM’ as they do have support from a reasonable evidence base. The others listed do not.
To conflate them is mischievous (and unethical) – as the authors must well know.
Why do they have yoga and Pilates on this list? Yoga as practiced in the US (and probably the UK) has little in common with the ascetic and meditation practices of the the original. The exercises most people think of are actually gymnastics borrowed from Europe.
There’s no woo in real Pilates. It’s a series of exercises designed to work smaller muscles which most people, especially athletes, don’t use much in ordinary life It’s somewhat outdated so not necessarily the best possible way to correct muscle imbalances and prevent injury.
Agreed.
People are more likely to try something if they don’t have to pay for it. Who knew that?
CAM proponents – for that is what this group of “researchers” are – think we should consider making it available on the NHS.
Well, I’ll be damned!
I would like to suggest an alternative conclusion: “It is concerning that as many as 16% of the population have used CAM within the last 12 months as most CAM doesn’t have evidence of effectiveness for any health condition and there are also risks associated with CAM treatments. Policy makers should consider the following two actions to address this issue: a) better education of members of the public about the lack of evidence and scientific rationale behind most CAM treatments and the potential risks b) gaining a better understanding of the gaps in current NHS services that result in people undertaking CAM, with the longer-term aim of addressing these gaps with science- and evidence-based treatments”.