Monthly Archives: June 2018
The HRI is an innovative international charity created to address the need for high quality scientific research in homeopathy… HRI is dedicated to promoting cutting research in homeopathy, using the most rigorous methods available, and communicating the results of such work beyond the usual academic circles… HRI aims to bring academically reliable information to a wide international audience, in an easy to understand form. This audience includes the general public, scientists, healthcare providers, healthcare policy makers, government and the media.
This sounds absolutely brilliant!
I should be a member of the HRI!
For years, I have pursued similar aims!
Hold on, perhaps not?
This article makes me wonder:
START OF QUOTE
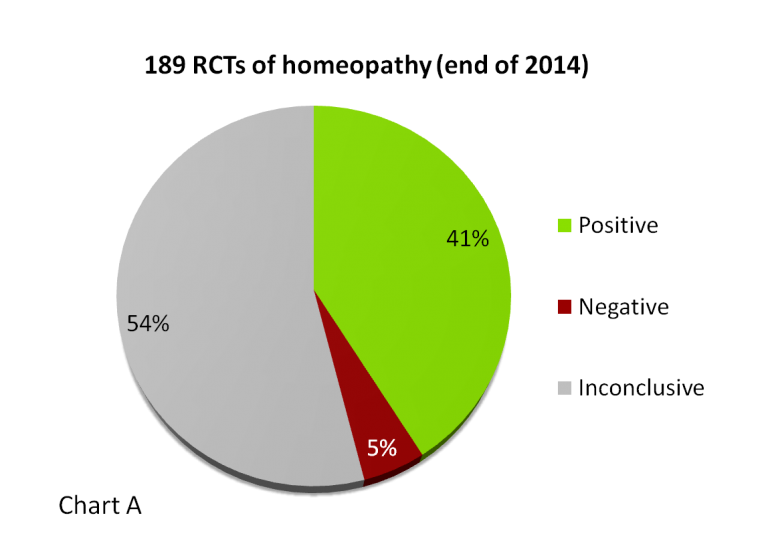
… By the end of 2014, 189 randomised controlled trials of homeopathy on 100 different medical conditions had been published in peer-reviewed journals. Of these, 104 papers were placebo-controlled and were eligible for detailed review:
41% were positive (43 trials) – finding that homeopathy was effective
5% were negative (5 trials) – finding that homeopathy was ineffective
54% were inconclusive (56 trials)
How does this compare with evidence for conventional medicine?

An analysis of 1016 systematic reviews of RCTs of conventional medicine had strikingly similar findings2:
44% were positive – the treatments were likely to be beneficial
7% were negative – the treatments were likely to be harmful
49% were inconclusive – the evidence did not support either benefit or harm.
END OF QUOTE
The implication here is that the evidence base for homeopathy is strikingly similar to that of real medicine.
Nice try! But sadly it has nothing to do with ‘reliable information’!!!
In fact, it is grossly (and I suspect deliberately) misleading.
Regular readers of this blog will have spotted the reason, because we discussed (part of) it before. Let me remind you:
_______________________________________________________________________________
A clinical trial is a research tool for testing hypotheses; strictly speaking, it tests the ‘null-hypothesis’: “the experimental treatment generates the same outcomes as the treatment of the control group”. If the trial shows no difference between the outcomes of the two groups, the null-hypothesis is confirmed. In this case, we commonly speak of a negative result. If the experimental treatment was better than the control treatment, the null-hypothesis is rejected, and we commonly speak of a positive result. In other words, clinical trials can only generate positive or negative results, because the null-hypothesis must either be confirmed or rejected – there are no grey tones between the black of a negative and the white of a positive study.
For enthusiasts of alternative medicine, this can create a dilemma, particularly if there are lots of published studies with negative results. In this case, the totality of the available trial evidence is negative which means the treatment in question cannot be characterised as effective. It goes without saying that such an overall conclusion rubs the proponents of that therapy the wrong way. Consequently, they might look for ways to avoid this scenario.
One fairly obvious way of achieving this aim is to simply re-categorise the results. What, if we invented a new category? What, if we called some of the negative studies by a different name? What about INCONCLUSIVE?
That would be brilliant, wouldn’t it. We might end up with a simple statistic where the majority of the evidence is, after all, positive. And this, of course, would give the impression that the ineffective treatment in question is effective!
How exactly do we do this? We continue to call positive studies POSITIVE; we then call studies where the experimental treatment generated worst results than the control treatment (usually a placebo) NEGATIVE; and finally we call those studies where the experimental treatment created outcomes which were not different from placebo INCONCLUSIVE.
In the realm of alternative medicine, this ‘non-conclusive result’ method has recently become incredibly popular . Take homeopathy, for instance. The Faculty of Homeopathy proudly claim the following about clinical trials of homeopathy: Up to the end of 2011, there have been 164 peer-reviewed papers reporting randomised controlled trials (RCTs) in homeopathy. This represents research in 89 different medical conditions. Of those 164 RCT papers, 71 (43%) were positive, 9 (6%) negative and 80 (49%) non-conclusive.
This misleading nonsense was, of course, warmly received by homeopaths. The British Homeopathic Association, like many other organisations and individuals with an axe to grind lapped up the message and promptly repeated it: The body of evidence that exists shows that much more investigation is required – 43% of all the randomised controlled trials carried out have been positive, 6% negative and 49% inconclusive.
Let’s be clear what has happened here: the true percentage figures seem to show that 43% of studies (mostly of poor quality) suggest a positive result for homeopathy, while 57% of them (on average the ones of better quality) were negative. In other words, the majority of this evidence is negative. If we conducted a proper systematic review of this body of evidence, we would, of course, have to account for the quality of each study, and in this case we would have to conclude that homeopathy is not supported by sound evidence of effectiveness.
The little trick of applying the ‘INCONCLUSIVE’ method has thus turned this overall result upside down: black has become white! No wonder that it is so popular with proponents of all sorts of bogus treatments.
__________________________________________________________________________________
But one trick is not enough for the HRI! For thoroughly misinforming the public they have a second one up their sleeve.
And that is ‘comparing apples with pears’ – RCTs with systematic reviews, in their case.
In contrast to RCTs, systematic reviews can be (and often are) INCONCLUSIVE. As they evaluate the totality of all RCTs on a given subject, it is possible that some RCTs are positive, while others are negative. When, for example, the number of high-quality, positive studies included in a systematic review is similar to the number of high-quality, negative trials, the overall result of that review would be INCONCLUSIVE. And this is one of the reasons why the findings of systematic reviews cannot be compared in this way to those of RCTs.
I suspect that the people at the HRI know all this. They are not daft! In fact, they are quite clever. But unfortunately, they seem to employ their cleverness not for informing but for misleading their ‘wide international audience’.
In 2005, I published a systematic review of ophthalmic adverse effects after spinal manipulations. At the time, I found 14 case reports. Clinical symptoms and signs were diverse and included loss of vision, ophthalmoplegia, diplopia and Horner’s syndrome. The underlying mechanism was arterial wall dissection in most cases. The eventual outcome varied and often included permanent deficits. Causality was frequently deemed likely or certain.
I concluded that upper spinal manipulation is associated with ophthalmological adverse effects of unknown frequency. Ophthalmologists should be aware of its risks. Rigorous investigations must be conducted to establish reliable incidence figures.
Now a new article has emerged that throws more light on this issue:
A 46-year-old healthy male with a history of chronic musculoskeletal neck pain presented to the emergency department with left sided weakness after a syncopal episode. The patient had been treated with frequent chiropractic neck manipulations over the past seven years, with his last session one month prior to presentation. One week prior to presentation, the patient developed a new headache, anisocoria, and ptosis of his right upper eyelid. Computed tomography angiography (CTA) of the head and neck showed an internal carotid occlusion with right middle cerebral artery zone of ischemia, and tissue plasminogen activator (tPA) was administered. Subsequently, the patient experienced vision loss in his right eye. MRI and CTA were repeated, revealing a right ICA dissection from below the ophthalmic artery to the posterior communicating artery. On examination, vision in the right eye was no light perception (NLP) and the pupil was amaurotic. Fundus exam showed vascular attenuation, severe pallor of the optic nerve and retina, without a cherry red spot. A diagnosis of ophthalmic artery occlusion was made.
Inpatient workup revealed no stroke risk factors, and he was discharged on aspirin and clopidogrel therapy. Follow up imaging showed re-cannulation of the ICA, although vision remained NLP at outpatient evaluation the following month. Macular spectral domain optical coherence tomography (SDOCT) showed hyperreflectivity of the inner retina diffusely and of the outer retina and retinal pigment epithelium (RPE) centrally. Fluorescein angiography revealed patchy choroidal filling, delayed arterial filling, and macular nonperfusion. Three months after presentation, vision had improved to light perception, and remains stable at one year after the dissection.
Central retinal artery occlusion (CRAO) has been previously described after neck manipulation; however, these cases have been attributed to a dislodged embolic plaque rather than arterial dissection as in this case. Carotid artery dissection after neck manipulation is rare, although the exact incidence is unknown, and may be fatal.
The authors of this case report concluded that internal carotid artery dissection in this case was permanently devastating to the vision of a previously healthy young patient.
What follows is simple:
- upper spinal manipulations have no or very little proven benefit;
- they are associated with a finite risk;
- thus, their risk/benefit balance fails to be positive;
- consequently, upper spinal manipulations cannot be recommended as a treatment of any condition.
When NHS England announced several months ago that they plan to stop the reimbursement of homeopathy, UK homeopaths were understandably upset and decided to launch a legal challenge to this decision. Yesterday, the result of this challenge has been published in a NHS press-release:
START OF QUOTE
NHS chief Simon Stevens has today welcomed the High Court’s decisive rejection of a legal challenge by the British Homeopathic Association to overturn plans to no longer routinely fund homeopathy on the NHS.
As part of action to clamp down on waste, over the last two years NHS England has taken action to curb prescriptions for medicines that can be bought over the counter or are of low value.
At the end of last year NHS England published guidance to curb prescriptions for 18 ineffective, unsafe or low clinical priority treatments, such as coproxamol, some dietary supplements, herbal treatments and homeopathy, saving up to £141 million a year. Earlier this year NHS England published a further list of 35 minor, short-term conditions for which over the counter medicines should not routinely be prescribed, saving around a further £100 million a year.
Savings form a key building block of the NHS’s 10 point efficiency plan contained in the Next Steps on the NHS Five Year Forward View, published in March 2017.
NHS chief, Simon Stevens said: “There is no robust evidence to support homeopathy which is at best a placebo and a misuse of scarce NHS funds.
“So we strongly welcome the High Court’s clear cut decision to kick out this costly and spurious legal challenge.”
Guidance on items which should not be routinely prescribed in primary care is available on the NHS England website.
END OF QUOTE
The reaction of UK homeopaths was as swift and deluded as it was predictable. The British Homeopathy Association, for instance, commented thus:
… The charity’s main claims against NHS England were that the consultation misrepresented homeopathy and therefore was unfair; and a report used in the consultation to inform the public was so complicated it would deter rather than encourage people to respond. Although the judge found there were sufficient grounds for a judicial review, after four days of lengthy legal arguments he dismissed the claims. Margaret Wyllie, BHA Chair, said the case highlighted how health bosses were unfairly manipulating the consultation process and making decisions about healthcare services without genuine patient engagement. “That NHS England attracted fewer than 3,000 responses from patients to a national consultation that ran for three months highlights its failure to genuinely engage with the public on important decisions about healthcare provision. Although 18 medicines were under review the only negative statement in NHS England’s press release promoting its public consultation was about homeopathy. The statement was so prejudicial it was widely reported in the media that the decision to deny patients homeopathic medicines had already been taken. How the judge failed to recognise that this was a deliberate attempt by NHS England to unfairly influence the public is astonishing,” said Mrs Wyllie.
In The Telegraph, Wyllie is quoted saying: “It appears NHS England can fail to engage with patients properly on removing services and get away with it. That is not good enough, for it is important to remember that the real losers in this case are the patients who are now being refused a treatment on which they have come to depend.”
One can only marvel at the lack of insight and self-criticism. I should to add that the BHA is a charity; with this court case, they have wasted significant amounts of public money for their own, hopelessly misguided interests. To me, this indicates that they no longer deserve a charitable status.
Personally, I had very little doubt that the court would decide as it did. The evidence was simply overwhelming and indisputable. In the written judgement, the judge stated that “I am satisfied that NHSE was rigorous in the discharge of the duty to have “due regard” to relevant matters, and that it was entitled, on the evidence before it, to conclude that the Guidance would not have an adverse impact on the statutory equality objectives, but rather, as the Analysis found, “would [enable] patients to have access to the most effective medications to achieve the best outcomes”.
In all this, the open questions, in my view, were whether
- Prince Charles, the prime defender of quackery in the UK, would intervene,
- and whether his intervention might change anything.
So, did he try to intervene?
I do not know. It could be that, after all the hoo-ha about his spider memos, he now is a little more cautions about meddling in health politics. It could also be that, as he is getting ready to become king, he wants to keep a low profile about his more bizarre ideas. Lastly, it could be that his opinion does not weigh as heavily as I had feared.
In any case, The High Court ruling is most welcome and unquestionably just, progressive, and long-overdue. I applaud all who have worked hard to bring it about, and am sure that (most of) my readers agree.
Personally, I find our good friend Dana Ullman truly priceless. There are several reasons for that; one is that he is often so exemplarily wrong that it helps me to explain fundamental things more clearly. With a bit of luck, this might enable me to better inform people who might be thinking a bit like Dana. In this sense, our good friend Dana has significant educational value.
Recently, he made this comment:
According to present and former editors of THE LANCET and the NEW ENGLAND JOURNAL OF MEDICINE, “evidence based medicine” can no longer be trusted. There is obviously no irony in Ernst and his ilk “banking” on “evidence” that has no firm footing except their personal belief systems: https://medium.com/@drjasonfung/the-corruption-of-evidence-based-medicine-killing-for-profit-41f2812b8704
Ernst is a fundamentalist whose God is reductionistic science, a 20th century model that has little real meaning today…but this won’t stop the new attacks on me personally…
END OF COMMENT
Where to begin?
Let’s start with some definitions.
- Evidence is the body of facts that leads to a given conclusion. Because the outcomes of treatments such as homeopathy depend on a multitude of factors, the evidence for or against their effectiveness is best based not on experience but on clinical trials and systematic reviews of clinical trials (this is copied from my book).
- EBM is the integration of best research evidence with clinical expertise and patient values. It thus rests on three pillars: external evidence, ideally from systematic reviews, the clinician’s experience, and the patient’s preferences (and this is from another book).
Few people would argue that EBM, as it is applied currently, is without fault. Certainly I would not suggest that; I even used to give lectures about the limitations of EBM, and many experts (who are much wiser than I) have written about the many problems with EBM. It is important to note that such criticism demonstrates the strength of modern medicine and not its weakness, as Dana seems to think: it is a sign of a healthy debate aimed at generating progress. And it is noteworthy that internal criticism of this nature is largely absent in alternative medicine.
The criticism of EBM is often focussed on the unreliability of the what I called above the ‘best research evidence’. Let me therefore repeat what I wrote about it on this blog in 2012:
… The multifactorial nature of any clinical response requires controlling for all the factors that might determine the outcome other than the treatment per se. Ideally, we would need to create a situation or an experiment where two groups of patients are exposed to the full range of factors, and the only difference is that one group does receive the treatment, while the other one does not. And this is precisely the model of a controlled clinical trial.
Such studies are designed to minimise all possible sources of bias and confounding. By definition, they have a control group which means that we can, at the end of the treatment period, compare the effects of the treatment in question with those of another intervention, a placebo or no treatment at all.
Many different variations of the controlled trial exist so that the exact design can be adapted to the requirements of the particular treatment and the specific research question at hand. The over-riding principle is, however, always the same: we want to make sure that we can reliably determine whether or not the treatment was the cause of the clinical outcome.
Causality is the key in all of this; and here lies the crucial difference between clinical experience and scientific evidence. What clinician witness in their routine practice can have a myriad of causes; what scientists observe in a well-designed efficacy trial is, in all likelihood, caused by the treatment. The latter is evidence, while the former is not.
Don’t get me wrong; clinical trials are not perfect. They can have many flaws and have rightly been criticised for a myriad of inherent limitations. But it is important to realise that, despite all their short-comings, they are far superior than any other method for determining the efficacy of medical interventions.
There are lots of reasons why a trial can generate an incorrect, i.e. a false positive or a false negative result. We therefore should avoid relying on the findings of a single study. Independent replications are usually required before we can be reasonably sure.
Unfortunately, the findings of these replications do not always confirm the results of the previous study. Whenever we are faced with conflicting results, it is tempting to cherry-pick those studies which seem to confirm our prior belief – tempting but very wrong. In order to arrive at the most reliable conclusion about the efficacy of any treatment, we need to consider the totality of the reliable evidence. This goal is best achieved by conducting a systematic review.
In a systematic review, we assess the quality and quantity of the available evidence, try to synthesise the findings and arrive at an overall verdict about the efficacy of the treatment in question. Technically speaking, this process minimises selection and random biases. Systematic reviews and meta-analyses [these are systematic reviews that pool the data of individual studies] therefore constitute, according to a consensus of most experts, the best available evidence for or against the efficacy of any treatment.
END OF QUOTE
Other criticism is aimed at the way EBM is currently used (and abused). This criticism is often justified and necessary, and it is again the expression of our efforts to generate progress. EBM is practised by humans; and humans are far from perfect. They can be corrupt, misguided, dishonest, sloppy, negligent, stupid, etc., etc. Sadly, that means that the practice of EBM can have all of these qualities as well. All we can do is to keep on criticising malpractice, educate people, and hope that this might prevent the worst abuses in future.
Dana and many of his fellow SCAMers have a different strategy; they claim that EBM “can no longer be trusted” (interestingly they never tell us what system might be better; eminence-based medicine? experience-based medicine? random-based medicine? Dana-based medicine?).
The claim that EBM can no longer be trusted is clearly not true, counter-productive and unethical; and I suspect they know it.
Why then do they make it?
Because they feel that it entitles them to argue that homeopathy (or any other form of SCAM) cannot be held to EBM-standards. If EBM is unreliable, surely, nobody can ask the ‘Danas of this world’ to provide anything like sound data!!! And that, of course, would be just dandy for business, wouldn’t it?
So, let’s not be deterred or misled by these deliberately destructive people. Their motives are transparent and their arguments are nonsensical. EBM is not flawless, but with our continued efforts it will improve. Or, to repeat something that I have said many times before: EBM is the worst form of healthcare, except for all other known options.
Nipah virus (NiV) infection is a zoonosis that causes severe disease in both animals and humans. The natural host of the virus are fruit bats of the Pteropodidae Family, Pteropus genus. Human-to-human transmission has also been documented, including in a hospital setting in India. Clinical presentations range from asymptomatic infection to acute respiratory syndrome and fatal encephalitis. There is no vaccine for either humans or animals. The primary treatment for human cases is intensive supportive care. In Kerala, India, several people have died of the deadly NiV. The infection has a mortality rate of around 70%.
It was predictable that such events would bring homeopaths to the fore. This article explains:
The Indian Homeopathic Medical Association’s Kerala unit has claimed to have the medicines to treat Nipah virus. B Unnikrishnan, an association official, said homeopathy has the appropriate medicines for all types of fever and hence they should be allowed to treat the infected patients. The association has requested the state Health Minister KK Shailaja to allow their professionals to examine the records of all those patients who have been tested positive for Nipah… So far, 16 people have died and two are recovering. Some 2,000 people who came in contact with the infected patients are also being monitored.
Knowing that an international delegation of homeopaths travelled to Liberia to treat Ebola (with the official support of their respective professional organisations), this news cannot surprise anyone.
Homeopaths dilute their remedies and delude themselves.
Sadly, the victims of their dilutions/delusions are:
- their patients,
- public health,
- progress,
- and rationality.
Our good friend Dana Ullman commented on my last post that doctors are being unethical by NOT prescribing homeopathic medicines because they are breaking one of the most important medical guidelines: “First, do no harm.” Here I do not want to discuss in-depth the nonsense about homeopathy in his sentence, rather I want to focus on the notion that doctors are obliged to foremost do no harm.
The sentence ‘first do no harm’ is supposed to originate from the Hippocratic oath which allegedly all doctors have to take when finishing medical school. This is twice wrong:
- we don’t take this oath – I have read it, and it is something utterly non-applicable to today;
- the famous sentence does not appear in the oath.
But never mind the history and all that! Doctors are nevertheless obliged to ‘first do no harm’ because it is an important principle of medical ethics.
This is also not true, I’m afraid.
If it were true, doctors would have to stop practicing much of medicine instantly. Clinicians do harm all the time. Their injections hurt, their diagnostic procedures can be unpleasant and painful, their medications cause adverse effects, their surgical interventions are full of risks, etc., etc. None of this would be remotely acceptable, if it did not also some good.
And that is why the ethical imperative of doing no harm has sensibly been changed to the imperative of doing more good than harm. Of course, doctors must be allowed to do even quite serious harm, as long as their actions can be expected to generate even more good. In more common medical terms, we speak of the risk/benefit balance of an intervention:
- if the known risks of a treatment are greater than the expected benefits, we cannot ethically prescribe it;
- if the benefits outweigh the risks, we can consider it as a reasonable option.
That is all very well, but it can only apply to treatments where both the risks and the benefits are well-understood. What about the many treatments where there is uncertainty regarding either or both of these factors? This question is impossible to answer in the abstract. We need to look at the best evidence we have for each specific case and, together with the patient, try to make an informed judgement.
Now, let’s please our good friend Dana and do such an evaluation for homeopathy, as one of many examples of an alternative therapy:
- The best evidence fails to show that highly diluted homeopathic remedies have any specific effects.
- As these remedies contain nothing, they also cannot cause any harm.
Therefore, one might argue that the balance of risk versus benefit might not look all that bad. Dana and his colleagues would thus feel that it ethically legitimate to routinely use homeopathy. But this line of thought would ignore an important issue: harm can be done not just by the remedy itself. The harm caused by applying an ineffective treatment for conditions that are otherwise effectively treatable (usually referred to as neglect) can be considerable, even fatal. So, for homeopathy the true situation presents itself as follows:
- no benefit beyond placebo;
- high risk of neglect.
This results in a negative risk/benefit balance which means, as outlined above, we cannot ethically use homeopathy.
… and, of course, Dana’s statement (doctors are being unethical by NOT prescribing homeopathic medicines because they are breaking one of the most important medical guidelines: “First, do no harm.” ) turns out to be wrong on several levels.
My previous post was about the question whether lay-homeopaths can practise homeopathy without breaking their code of ethics. The answer was NO, because they lack most of the skills needed to obtain informed consent.
What about doctor homeopaths?
Can they practice homeopathy ethically?
Doctors are, of course, also obliged to follow their ethical code, and that means they too must obtain informed consent from their patients before starting a therapy. This is, for instance, what the UK General Medical Council tells their members:
You must give patients the information they want or need about:
- the diagnosis and prognosis
- any uncertainties about the diagnosis or prognosis, including options for further investigations
- options for treating or managing the condition, including the option not to treat
- the purpose of any proposed investigation or treatment and what it will involve
- the potential benefits, risks and burdens, and the likelihood of success, for each option; this should include information, if available, about whether the benefits or risks are affected by which organisation or doctor is chosen to provide care
- whether a proposed investigation or treatment is part of a research programme or is an innovative treatment designed specifically for their benefit4
- the people who will be mainly responsible for and involved in their care, what their roles are, and to what extent students may be involved
- their right to refuse to take part in teaching or research
- their right to seek a second opinion
- any bills they will have to pay
- any conflicts of interest that you, or your organisation, may have
- any treatments that you believe have greater potential benefit for the patient than those you or your organisation can offer.
You should explore these matters with patients, listen to their concerns, ask for and respect their views, and encourage them to ask questions.
You should check whether patients have understood the information they have been given, and whether or not they would like more information before making a decision. You must make it clear that they can change their mind about a decision.
Following the 8 points from my previous post (I am trying to apply the same criteria to both types of homeopaths), a medical homeopath might tell her patient (whose stomach pain turns out to be caused, let’s assume, by a stomach ulcer) roughly this:
- The tests show that you are suffering from stomach ulcer.
- The natural history of this condition is usually benign, but it needs effective treatment; if not, the problem would become serious.
- Conventional medicine has several effective therapeutic options.
- I nevertheless propose to treat you with a homeopathic remedy.
- There is no good evidence that it will work beyond a placebo effect.
- The remedy is harmless, but not giving you an effective treatment might cause considerable harm.
- The cost of the consultation is £80, and the remedy will cost you around £15.
- I suggest you come again in a week or two; perhaps we need quite a few consultations altogether.
Again, as with the lay-homeopath from my previous post, any sensible patient would walk away without accepting the treatment. This means that our doctor homeopath can only practice homeopathy, if she does not inform her patient about points 5 and 6. In other words, doctors who practice homeopathy cannot obtain adequately informed consent. We have recently seen a real case of this happening and ending in the death of the patient.
Of course, the homeopath might send her patient to a specialist; or she might decide to administer a conventional therapy herself. Either way, she would not be practising homeopathy.
The dilemma is real, yet it is rarely considered. Here is a short passage from our book where we discuss the ethics of alternative medicine in full detail:
Genuine informed consent is unattainable for most CAM modalities. This presents a serious and intractable ethical problem for CAM practitioners. Attempts to square this circle by watering down or redefining the criteria for informed consent are ethically indefensible. The concept of informed consent and its centrality in medical ethics therefore renders most CAM practice unacceptable. Conventional healthcare subscribes to the ethical principle ‘no consent, no treatment’; we are not aware of the existence of any good reasons to excuse CAM from this dictum.
As I said, the ethical practice of homeopathy is a practical impossibility.
Or do you think I got this wrong?
Alternative medicine is riddled with a multitude of serious ethical problems. In our recent book, we made an attempt to look at them systematically and critically (I am not aware of anyone having done this before). Essentially, we arrive at the conclusion that, for many types of alternative medicine, it is not possible to practise them according to fundamental demands of healthcare.
Homeopathy is one of them. I recently had a look at the CODE OF ETHICS of the UK Society of Homeopaths (last updated 2015). There I almost instantly stumbled over perhaps the most significant hurdle of practising homeopathy ethically. Here is what the SoH demands of its members:
1) To ensure that the patient is always able to make informed choices with regard to their healthcare, registered and student clinical members must give full and clear information about their services when commencing homeopathic treatment. This will include written information about the nature of the treatment, charges, availability for advice, confidentiality and security of records.
2) To ensure that the patient or their authorised representative is able to give valid consent with regard to healthcare, registered and student clinical members must give clear and sufficient information about the nature of homeopathic treatment, its scope and its limitations, before treatment begins and as appropriate during treatment…
The SoH is absolutely correct, full, sufficient and clear information before commencing treatment and consent to that treatment are two preconditions for any type of healthcare. However, the SoH is a bit shy about explaining what ‘full information’ must entail. As I have mentioned before, full and sufficient information must include:
- the diagnosis,
- its natural history,
- the most effective treatment options available,
- the proposed therapy,
- its effectiveness,
- its risks,
- its cost,
- a rough treatment plan.
So, let’s imagine a patient who suffers from stomach pains consulting his homeopath. Following the above 8 points, here is what she would need to tell him:
- I don’t know what your diagnosis is; I am not medically trained.
- I therefore can tell you nothing about its natural history.
- And nothing about the most effective treatment for your condition.
- I nevertheless propose to treat you with a homeopathic remedy.
- There is no good evidence that it will work beyond a placebo effect.
- The remedy is harmless, but not giving you an effective treatment might, of course, cause considerable harm.
- The cost of the consultation is £80, and the remedy will cost you around £15.
- I suggest you come again in a week or two; perhaps we need quite a few consultations altogether.
After hearing this, almost any patient would get up, thank the homeopath for the full information and look for a clinician who is able to offer an effective therapy. In other words, the SoH is inhibiting its members from practising homeopathy (alright, they don’t spell it out in such clear terms, but that is what full and sufficient information amounts to).
Why do they do that?
Because they have to!
Not supplying full and sufficient information would simply be unethical. And unethical healthcare cannot be tolerated.