Many of you will know that JAMA is one of the most respected medical journals. It is therefore surprising that, within the period of a few days, they published not one but two dodgy RCTs of alternative treatments.
The new trial was aimed at determining whether the addition of chiropractic care to usual medical care results in better pain relief and pain-related function when compared with usual medical care alone.
The study was designed as a pragmatic comparative effectiveness clinical trial using adaptive allocation was conducted from September 28, 2012, to February 13, 2016, at three US military medical centres. Eligible participants were active-duty US service members aged 18 to 50 years with low back pain from a musculoskeletal source. The intervention period was 6 weeks. Usual medical care included self-care, medications, physical therapy, and pain clinic referral. Chiropractic care included spinal manipulative therapy in the low back and adjacent regions and additional therapeutic procedures such as rehabilitative exercise, cryotherapy, superficial heat, and other manual therapies.
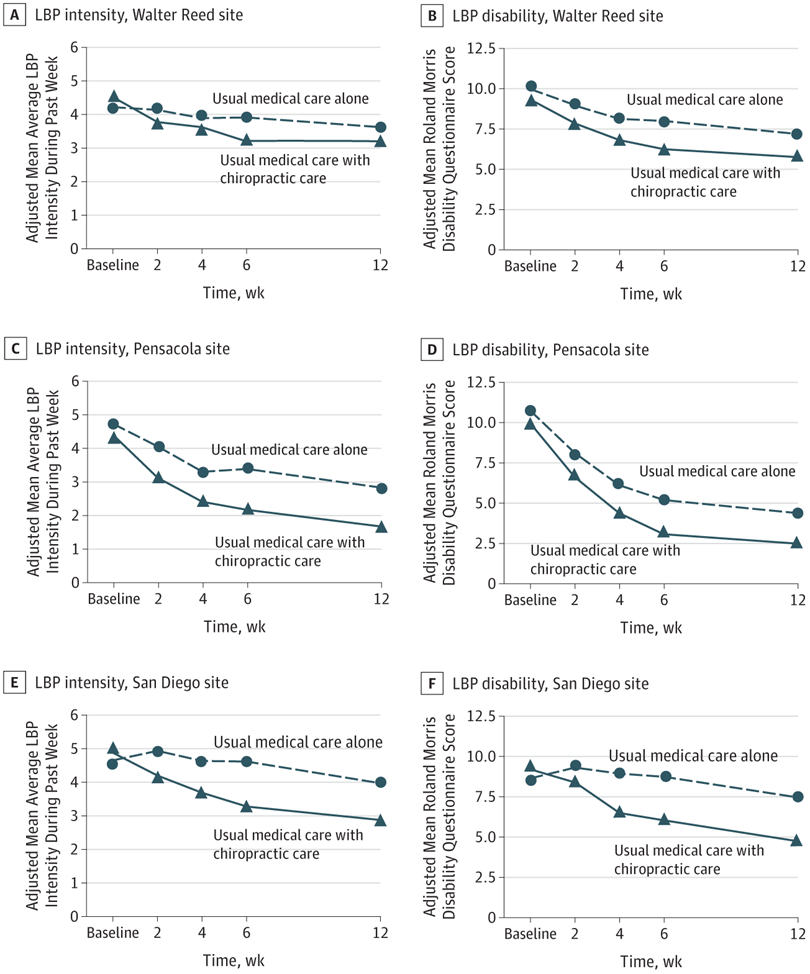
Primary outcomes were low back pain intensity (Numerical Rating Scale; scores ranging from 0 [no low back pain] to 10 [worst possible low back pain]) and disability (Roland Morris Disability Questionnaire; scores ranging from 0-24, with higher scores indicating greater disability) at 6 weeks. Secondary outcomes included perceived improvement, satisfaction (Numerical Rating Scale; scores ranging from 0 [not at all satisfied] to 10 [extremely satisfied]), and medication use.
In total, 750 patients were enrolled. Statistically significant site × time × group interactions were found in all models. Adjusted mean differences in scores at week 6 were statistically significant in favour of usual medical care plus chiropractic care compared with usual medical care alone overall for low back pain intensity (mean difference, −1.1; 95% CI, −1.4 to −0.7), disability (mean difference, −2.2; 95% CI, −3.1 to −1.2), and satisfaction (mean difference, 2.5; 95% CI, 2.1 to 2.8) as well as at each site. Adjusted odd ratios at week 6 were also statistically significant in favour of usual medical care plus chiropractic care overall for perceived improvement (odds ratio = 0.18; 95% CI, 0.13-0.25) and self-reported pain medication use (odds ratio = 0.73; 95% CI, 0.54-0.97). No serious adverse events were reported.
The authors concluded that chiropractic care, when added to usual medical care, resulted in moderate short-term improvements in low back pain intensity and disability in active-duty military personnel. This trial provides additional support for the inclusion of chiropractic care as a component of multidisciplinary health care for low back pain, as currently recommended in existing guidelines. However, study limitations illustrate that further research is needed to understand longer-term outcomes as well as how patient heterogeneity and intervention variations affect patient responses to chiropractic care.
Regular readers will have spotted it straight away: This trial follows the infamous ‘A+B versus B’ design. It will almost always generate a positive result – so much so that it is a waste of time to run the study because we know its findings before it has started. And if this is so, the trial is arguably even unethical.
The reason is, of course, that the study design does not control for placebo effects. And this means that even an utterly useless treatment will produce a (false-positive) result as long as it generates a placebo effect. Some of the authors of the present study are experienced researchers and clearly know all this. This is why they call their study a ‘pragmatic’ trial. But even with pragmatic trials, one cannot get away with murder!
As far as I can see, there are even two ‘murders’ here:
- The authors stated that their aim was to determine whether the addition of chiropractic care to usual medical care results in better pain relief and pain-related function when compared with usual medical care alone. I would argue that their study did not live up to this aim. As it did not control for placebo effects, it cannot possibly test the effectiveness of chiropractic care per se.
- The authors concluded that their trial provides additional support for the inclusion of chiropractic care as a component of multidisciplinary health care for low back pain. I would argue that this is quite simply wrong. The results are in perfect agreement with the assumption that chiropractic care is a placebo, and few would argue that the inclusion of a pure placebo can be recommended.
Compared to these major issues, my other concerns are mere trivialities:
- The trial tested spinal manipulation plus a whole bunch of physiotherapeutic intervention. I bet my last shirt that the chiro-community will claim that it demonstrated the effectiveness of chiropractic spinal manipulations. Already the very first sentence of the present paper’s discussion section goes into this direction: The changes in patient-reported pain intensity and disability as well as satisfaction with care and low risk of harms favoring UMC with chiropractic care found in this pragmatic clinical trial are consistent with the existing literature on spinal manipulative therapy…
- In their abstract, the authors (several of whom are chiropractors) state that there were no serious adverse effects (the paper is extremely thin on providing details about how adverse effects were assessed, verified, categorised etc.). What about non-serious adverse effects (arguably LBP is a minor condition, so minor adverse effects are relevant!)? In the paper, they enlighten us that of the 43 adverse effects reported by participants receiving UMC with chiropractic care, 38 were described as muscle or joint stiffness attributed to chiropractic care (37 events) or physical therapy (1 event), 1 was reported as indistinct symptoms following an epidural injection, 3 were described as pain, tingling, or sensitivity in an extremity without reference to a specific treatment, and 1 was a lower-extremity burning sensation for 20 minutes following spinal manipulative therapy. In my view, this is sufficiently important to be mentioned also in the abstract.
- The authors remain totally silent when it comes to the discussion of the effect sizes. To me, they seem to be moderate. Are they at all clinically relevant. I feel that the discussion of a PRAGMATIC trial must include this pragmatically important issue.
It is my strong opinion chiropractors now qualify to be integrated with all hospital based health practitioners. The Dutch have proven that it works for its citizens, the American Medical Association journal editor has now endorsed chiropractic management and therefore it is now time for Australia, the USA and the developed world to bring chiropractic into the public health care system. Out with Oxycontin and in with optimistic health outcomes. Time will tell if this decision is correct. As a chiropractor with 33 years experience and dedicated to the better health of the human race…..and domestic animals, I am sure my statement is correct!
whatever you have been smoking, can you send me some of it?
I never inhale. I recommend that you share your opinion also with JAMA Network Open.
“Dr” Epstein, you are not really a doctor at all, but rather you have a “doctorate” degree from a made up therapy taught at what can only be termed a fake college. Some links, please to the “proof” you claim for the Dutch.
Let’s see a study of the “added care” without the manipulation and see if we get the same result, eh? Subluxations don’t exist and any medical body that sanctions this nonsense based on them needs to see a neurologist to have his or her head examined. I include Medicare (US) and Medicaid in this as they now pay for these treatments. Placebos may be fine, but the taxpayer should not have to pay for them.
I need to correct the statement about the Dutch integrating chiropractic and medical care, as it is the Danes and not the Dutch.
You need to read up on a lot of things Mr. Epstein.
Judging from your previous performances I fear however, that you may not have the facilities necessary to assimilate much of it.
That some purported alternative to medicine is paid for by social funds is not the same as it being integrated into medicine or that its utility or benefit has been confirmed.
Chiropractic has been subsidized by the Danish social health care system since 1978. It is also subsidized by the social system in Norway.
Homeopathy, the mother of make-believe medicine, is subsidized by the social security systems of many countries, like the UK, France and Germany. That does not mean it works.
Like in the case of homeopathy the fact that a social security system pays partly or in full for chiropractic practice is not a guarantee that it is getting value for the money. By ‘chiropractic’ I am of course referring to the set of theatrical manipulations and unsubstantiated theories invented by DD Palmer and his congregation of subluxationists, not practices belonging to more credible and scientifically substantiated practices like modern physiotherapy.
Historically, chiropractors have gained this ground by active political lobbying, not through scientifically sound progress.
Also, in Scandinavia chiropractic practitioners have to a large extent adopted the more credible and proven arsenal of physiotherapy. Even if you see the odd quack chiropractor promising to strengthen the immune system by clicking your skull with a silly instrument or using applied kinesiology to detect food intolerances, cranial osteopathy to balance imaginary conditions or other similarly risible rubbish, the impression is that most Scandinavian chiropractors try their best to gain respectability by playing physiotherapists and keeping quiet about fairy-tale claims.
Chiropractors are good at activating their clients, giving sound lifestyle advice but they are exceptionally good at convincing customers of the qualities of their ministrations. That is what keeps them in business.
Like with other cultist following, a strong and loud, albeit small congregation of affectionate clients inevitably rises furiously to their defense whenever someone dares criticize their objects of admiration. Therefore health authorities choose to keep a status quo but do not encourage further ‘integration’.
No, chiropractic is not “integrated” into medical practice anywhere, not even in Scandinavia.
@Mr.Epstien: after 33 years in chiropractic you needn’t use the expression “strong opinion” since it’s a given that’s all you have at your disposal.
Goertz is a well-heeled apologist and chiroquaker. The oddest thing to me about this fraud is why pray-tell IF Physical Therapists were administering physical therapy couldn’t they have also administered spinal-manipulation? The frauds conducting the trial (Spine IQ of which the head fraud is CEO) could have then had the “insight” as to whether a dogmatic quack doing dogmatic-spinal-manipulation was any better than a less-dogmatic PT doing it. Manipulating the military should be illegal….who TF allows this shit to fester??
These SOBs want only confusion and obfuscation…..they abhor answers since they will topple the entire house of fraud.
Entrepreneurial theatrics masquerading as ‘health-care’ for 123 years….the whole lot should be Court marshaled.
I couldn’t agree more and thank you for your blunt language–it needs to be said. Chiros need to become properly trained Physical Therapists (physiotherapists, I believe, in UK) if they want to be taken seriously by anyone but the gullible.
For a chiropractor to become trained as a physiotherapist would involved serious down-skilling and resorting to a “shake, bake and fake” mode of therapies, divorced from scientific validity and lacking clinical base rigor. The Lancet outlined effective therapies for low back pain. None of the clinical offerings of Physios e.g. exercises, TENS, ultrasound, corsets, Pilates, biofeedback even rated a mention as being effective or clinically justified. What do physios have to offer in the treatment of neuro-musculo-skeletal disorders…………………nothing. Effective treatments were for patients to remain physically active, spinal manual therapy (expertise of chiropractors), and anti-inflammatories.
And of course they gaily skip over the fundamental matter: ‘chiropractic care’ involves adjusting subluxations, for which there is no plausible evidence; and releasing ‘innate intelligence’ for which there is also no evidence. Palmer stated “chiropractic is a different system from medicine.” He was right.
SMT may have a part to play, but that is not ‘chiropractic’.
There were other modalities used: “additional therapeutic procedures such as rehabilitative exercise, cryotherapy, superficial heat, and other manual therapies” – none of which are exclusive to or comprise ‘chiropractic’.
That having been said, these papers are useful additions to the literature which shows that there is no need to take time and trouble studying ‘chiropractic’. The days of that modality are over. Intending students of ‘musculo-skeletal care’ should train and qualify as physiotherapists, or doctors. The outcomes will be as good, and without a fake rationale.
The editors of JAMA need to read this critique and the comments, and reconsider their support for such false science and fraud. They must know better but apparently do not care. Could $$ have something to do with it?
“The Dutch have proven that it works for its citizens,”
I.m Dutch. Did I Miss anything?
Yet another example of something you have highlighted before in CAM: marketing masquerading as research
Some reviews.
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2680415
https://www.medscape.com/viewarticle/896946
@Michael Kenny
Christine Goetz has recently lost her research position after supporting the Choosing Wisely campaign. We are still to find out the full details. So your assertion that “Goertz is a well-heeled apologist and chiroquaker.” ??? Hmmmm, Your bias is showing just a tad.
@Richard Rawlins
“And of course they gaily skip over the fundamental matter: ‘chiropractic care’ involves adjusting subluxations,”
You employ similar arguments as the subluxationists I have to deal with. They call me a “medipractor” and you tell me I’m a physiotherapist if I follow best evidence. They also tell me that if its not subluxation then its not chiropractic.
https://www.ahpra.gov.au/Registration/Practitioner-Services/Practitioner-Home.aspx
AHPRA allows me to use the courtesy title Doctor.
“Your bias is showing a tad”? This in comparison to you having nothing but bias? I don’t pretend to be a “dr” of the worlds largest non-scientific health care delivery system…..and then perpetually try to defend it using the claim I can reform it….but can’t say into ‘what’.
Why don’t one of you jackwads for once simply tell us biased-skeptics WHAT Chiropractic-is…..if-not-just-an elaborate, 123 year old Health-care -scam???
It only morphed into a “musculoskeletal treatment” by default….after it became apparent to most that it had ZERO effect on human health (and not coincidentally it’s pretty much proven to have ZERO effect on MSK conditions as well). So WTF is chiropractic???? Micheal Menke DC PhD suggested there were 200 various Techniques….many so divergent as to share virtually no common ground.
So perhaps “chiropractic is as a chiropractor does”. Or more accurately fraud disguised as healthcare.
Anxiously awaiting your obfuscation and machinations.
@MK
Michael I have consistently posted my opposition to the abuse of the title ‘Dr” by chiropractors. Here in Australia I have actively lobbied against it. When registration was state based it was banned and inspectors would conduct random audits of clinics and hit the chiropractors with large fines. The vitalists lobbied heavily for the title to be given when we went to National registration for all health practitioners under a single body AHPRA. Unfortunately AHPRA decided to permit “Dr of Chiropractic” which annoyed many of us no end. Some states like NSW in the good old days were vigilant in fining chiropractors especially those trained in the US who were overly fond of the title.
I am also in agreement with you on “200 various Techniques….many so divergent as to share virtually no common ground.”
I have also been involved in lobbying here for the accrediting bodies that assign continuing professional development (CPD) hours to stop giving hours to all and sundry. There are two accrediting agencies here, CAA and COCA. COCA refuses to assign CPD hours and has rigorous criteria (the vitalists know this and don’t use COCA), CAA gives them to just about everyone. Under AHPRA all health professions need minimum CPD hours every year to re-register. CAA adopting COCA guidelines for CPD would send shock waves through the vitalist church which I would love to see. If you look at both physiotherapy and chiropractic these days to invent a technique all you need to do is add the word “functional” before the title and (TM) after it and your up and running. Clear enough?
So two points which we are in agreement.
“and not coincidentally it’s pretty much proven to have ZERO effect on MSK conditions as well”. I suggest you start reading the research. Starting with the 2008 supplement of The Spine Journal that compares 25 different approaches for the treatment of LBP. Chiropractic stacks up well compared to the alternatives.
“perpetually try to defend it using the claim I can reform it….but can’t say into ‘what’.”
Already there. Chiropractic Australia here is leading reform and advocacy. It was specifically set up by like minded chiropractors for that specific purpose. The chiropractors in Denmark, Norway and Ontario have been particularly effectively in banning/dumping Subluxation dogma. Utilization rates for chiropractic in those jurisdictions are at 22-25% of the population and they are struggling to keep up with demand. Elsewhere where subluxation rubbish persists utilization rates are stagnant at 10%.
So into what?
http://www.danskkiropraktorforening.dk/English/Chiropractic-in-Denmark/
The Danish chiropractors also all voted years ago that a % of every consultation goes into a research fund. They now have 15 researchers ranked in the top 60 MSK researchers in the world. Jan Hartvigsen was ranked #1 last year. He also deputy chaired the recent Low Back Pain Series in The Lancet.
So much of what is posted here in regards to chiropractic I am in agreement. But we are not all members of the high church of subluxation. That is why I have consistently said here:
Step 1. Point out the BS which I support.
Step 2. Point out whats right like the example of the Danes and support otherwise you are carpet bombing and look on the reformers and researchers like the Danes as acceptable collateral damage.
Critics like you Michael and Edzard are very important for reform and absolutely necessary. I just wish you were more targeted in your criticism AND support reform.
P.S. We are all biased towards what we do.
@C_C
Sorry, but your posts are increasingly tiresome. You answer MK’s “perpetually try to defend it using the claim I can reform it….but can’t say into ‘what’” with a link to Chiropractic in Denmark (where, by the way chiros use the ‘doctor’ title, to which you claim to object). What Michael Kenny was asking (and I have asked you in the past but you always respond with similar dissemblings as in the reply to MK) is exactly what does your ideal of reformed chiropractic consist?
If you ask someone what an obstetrician or an oncologist or a cardiologist or a neurologist does most people could provide fairly coherent answers and many could even name some of the procedures they use. The types of disease or condition these specialities handle is perfectly clear. So; a direct question for you: exactly what does a chiropractor do (no subluxations permitted) and what type of patient is appropriately referred to the speciality? What devices and medications does a chiropractor use? Your Danish link does at least provide a kind of halfway answer to my questions — “A chiropractor is an authorized healthcare practitioner who deals with the investigation, diagnosis, prevention and treatment of pain conditions and impairment of the musculoskeletal system.” Is that your definition?
Some more direct questions for you. What is your opinion of homeopathy? Of reiki? Of acupuncture? Of applied kinesiology? Do let us know whether you regard chiropractic as an exception among pseudo-medical ‘professions’ because it is not nonsense, regardless of its feeble evidence base. But you first have to spell out just what chiropractic IS, and how it differs from services offered by properly trained physicians.
@Cc: You don’t disappoint!! Obfuscation, machinations AND plenty of drivel for good measure!
Next time you are motion-palpating a ‘patient’ to determine the vector of your thrust….think hard and long how you ain’t just hunting a subluxation….irrespective of the name you ascribe to it and the reformist dogma you use to gain a semblance of rectitude.
Perhaps the bigger question is why did JAMA published a study which Ernst claims is “dodgy” and he also suggested the study was “unethical”?
that is a question you have to ask JAMA, not me.
They are probably more objective.
As far as your A + B…this was eluded to in the limitations of the study, so it’s a redundant point.
“Similarly, the use of hands-on, multimodal interventions commonly delivered by doctors of chiropractic makes it difficult to mask participants to treatment group or to control for the fact that those with chiropractic care received more time and attention from clinicians.”
alluding does not make it irrelevant.
I stated it was redundant.
Regardless, one can have a A+B study and have a negative outcome.
Also, the chiropractic model used in the study hasn’t been shown to be a placebo.
Thus, any suggestion of it being an unethical study is silly.
I disagree
I’m sure you do.
Toodles.
@GibletGiblet & MrDale: I recently experienced an electrocution while golfing rendering a loss of half of my IQ. However this has afforded me the ability to now understand and appreciate your blog entries!!
I’ve also decided to enroll in Chiropractic-clown college!! (I didn’t qualify previously with my normal IQ).
Perhaps when I graduate we can work together hunting subluxations with invalid and unreliable tests, manipulate hyper-mobile joints, stroke-out a few victims and get rich defrauding insurers? I’m sure you could use a new accomplice!
I’ll let you know if my IQ is restored and I’m thus disqualified…otherwise see you in 3.3 years!!
According to Ian Coulter the design of the study in the JAMA paper was set up by the Dept of Defense. The pragmatic non placbo design was because this is how chiropractic care is currently utilized within the military.
@ Dr Dale
See https://edzardernst.com/2018/06/malpractice-of-chiropractors-just-the-tip-of-an-iceberg/#comment-104062