How often have we heard that chiropractic has moved on and has given up the concept of subluxation/malalignment? For sure there is no evidence for such nonsense, and it would be high time to give it up! But, as has been argued here and elsewhere, if chiros give it up, what is there left? What then would differentiate them from physios ? The answer is not a lot.
In any case, chiros have by no means given up subluxation. One can argue this point ad nauseam; yet, most chiros remain in denial.
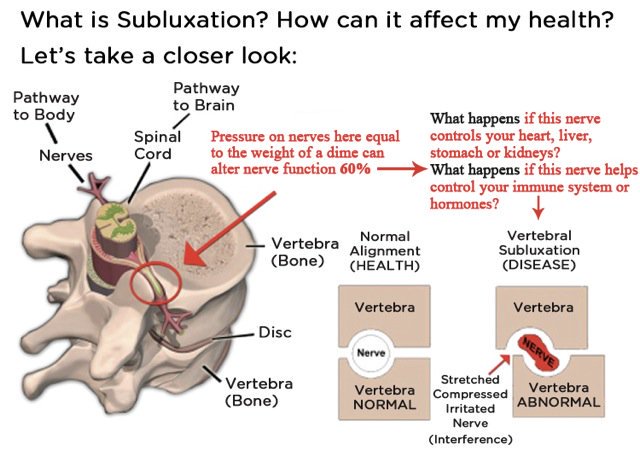
For this post, I have chosen a different approach to make my point. I simply went on twitter and had a look what messages chiros tweet. The impression I got is that the majority of chiros are totally immersed in subluxation. To provide some proof, I have copied a few images – if chiros do not listen to words, perhaps they understand pictures, I thought.
So, here we go – enjoy!
[please click to see them full size]



A very angry and aggressive post, all too typical of this site, as I’m sure Peter McAlpone will agree.
What then would differentiate them from physios ?
Umm, the fact that physios know what they are doing and provide positive treatment?
Also, most PT’s do not claim to cure or treat the multitude of unrelated symptoms and disorders that chiros advertise to help.
Yikes….thank you for this.
I recently was forced to sit through an hour long episode of ‘Ghost Hunters’ and was stuck by the overt similarities to things like Chiropractic (though I don’t believe Blue Cross or Medicare pay for ghost-expulsion, though I haven’t checked my policy).
Believers (or frauds) with capacious financial stakes willing (and enthusiastic) to set aside all logic, reason and historical data in pursuit of the fantasy of children and imbeciles.
There will NEVER be anything to come from any of it to help enlarge scientific understanding of the world or, in the case of subluxation-hunting, the spine or human health….however huge volumes may be deduced about human psychology and gullibility.
Abstract regarding DC students opinion of subluxation….it IS alive and well.
Chiropractic identity, role and future: a survey of North American chiropractic students
Chiro Man Ther 2015 23:4
Background
The literature pertaining to chiropractic students’ opinions with respect to the desired future status of the chiropractic physician is limited and is an appropriate topic worthy of study. A previous pilot study was performed at a single chiropractic college. This current study is an expansion of this pilot project to collect data from chiropractic students enrolled in colleges throughout North America.
Objective
The purpose of this study is to investigate North American chiropractic students’ opinions concerning professional identity, role and future.
Results
A total of 1,247 (16.7% response rate) questionnaires were electronically submitted. Most respondents agreed (34.8%) or strongly agreed (52.2%) that it is important for chiropractors to be educated in evidence-based practice. A majority agreed (35.6%) or strongly agreed (25.8%) the emphasis of chiropractic intervention is to eliminate vertebral subluxations/vertebral subluxation complexes. A large number of respondents (55.2%) were not in favor of expanding the scope of the chiropractic profession to include prescribing medications with appropriate advanced training. Most respondents estimated that chiropractors should be considered mainstream health care practitioners (69.1%). Several respondents (46.8%) think that chiropractic research should focus on the physiological mechanisms of chiropractic adjustments.
Conclusion
The chiropractic students in this study showed a preference for participating in mainstream health care, report an exposure to evidence-based practice, and desire to hold to traditional chiropractic theories and practices. The majority of students would like to see an emphasis on correction of vertebral subluxation, while a larger percent found it is important to learn about evidence-based practice. These two key points may seem contradictory, suggesting cognitive dissonance. Or perhaps some students want to hold on to traditional theory (e.g., subluxation-centered practice) while recognizing the need for further research to fully explore these theories. Further research on this topic is needed.
(doi:10.1186/s12998-014-0048-1)
I knew this paper.
what can one do with a response rate of 17%?
discard it?
the truth would probably be much more defaming for chiros.
@EE
“what can one do with a response rate of 17%?”
Marginalize the subluxationists and support the reformers, researchers and the reform process.
Step 1. Point out the BS.
Step 2. Point out what’s right and support.
If the critics do not take step 2 then they are entrenched carpet bombers who see reform and reformers as acceptable collateral damage. That makes them just as much a part of the problem when it comes to reform as the subbies. The two extremes.
It’s a shame I missed last months Vertebral Subluxation Summit in Kansas. Thanks for the posted advertisement. I assume that Dr Deed Harrisons lecture “Cervical Saggital Plane Subluxation and The Brain” was in relation to the following link that discusses the relationship between cervical lordosis remodelling(vertebral subluxation reduction) and long term improvement in patients who present with cervicogenic dizziness. A very well designed study performed by physiotherapists but supervised by Dr Harrison as he is the third author listed in the paper.
https://www.minervamedica.it/en/journals/europa-medicophysica/article.php?cod=R33Y2017N01A0057
Perfect! Dana Ullman in disguise! Let’s see what’s going on.
The fact that Dr. Harrison is the third author listed in the paper is NOT because he is some source of authority or expertise and acts as a supervisor. It is because he is affiliated with Denneroll™ and their device. Visit http://www.denneroll.com/about/ and scroll to the bottom to read the “testimony” of Mr. Deed Harrison:
“I personally use the Denneroll Orthotic device for my patients. Now, I have chosen to put the CBP name behind the Denneroll and recommend it to other Chiropractors.”
-Deed E. Harrison, D.C. Chiropractic BioPhysics Technique Director
And then there is https://idealspine.com/cervical-denneroll/ so this should be clear. They appear to be partners.
Good, so he is not a supervisor, he is a co-author because of vested interests. This is a textbook source of bias.
Still, I believe there is a fair chance that the study is relatively sound.
Check this out:
https://www.ncbi.nlm.nih.gov/pubmed/27576192.
https://www.ncbi.nlm.nih.gov/pubmed/22684211
https://www.ncbi.nlm.nih.gov/pubmed/23640324
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4161715/
It is the same two people, only without Deed Harrison as a co-author (except for the first one), trying various traction methods and getting positive results. This means only few things:
-Traction appears to help. However, I don’t see anything “chiropractic” in traction. Physical Therapists also use traction among other standard protocols.
-Indeed, Deed Harrison probably was only included as a co-author because of his affiliation with the device.
-Chiropractors cannot even make a comment without using the word “subluxation” in it, as is evident by the parenthesis in the earlier comment of Mr. Epstein.
-Interestingly, when I checked the text of the trial https://www.ncbi.nlm.nih.gov/pubmed/27576192 that used the Denneroll™ device, there is absolutely no mention of the words “subluxation” or “chiropractic” (which is only found in the references, mostly pertaining to journals).
The literature is a bit indecisive regarding traction. From what I found, the evidence are considered low-quality. I am amused to see that the two researchers in the studies cited above have put a lot of faith in it and are constantly carrying out trials. Maybe something good can come out of it in the end, so I will keep my fingers crossed for now.
However, the contention that cervical lordosis remodelling equates to vertebral subluxation reduction amounts to considering varying (abnormal) levels of kyphosis/lordosis to be subluxations. This is not in agreement to medical subluxation being a significant structural displacement. Maybe subluxation could be compared to spondylolisthesis. Osteopathy joined the evidence-based medicine club (and changed name to osteopathic medicine) in some countries. Why not chiropractic too?
James,
I agree that the use of the term Vertebral Subluxation creates confusion and clouds the facts that spinal displacements from average normal do exist and established Chiropractic Biophysics(CBP) evidence based protocols can guide clinicians in the reduction of abnormal spinal displacements. I prefer the use of spinal displacements over vertebral subluxation and use the term subluxation when the intersegmental translation of relative rotation angles between two individual vertebrae exists.
The authors of the paper mentioned in my previous comment, Moustafa and Diab have many more projects planned with the support and guidance of Chiropractic Biophysics Non Profit Inc. Since they have great influence and control of the university hospital’s clinic, much more long term RCT will be forth coming. so keep those fingers crossed!!
It would seem to me CBP is ‘practiced’ (properly?) by just a tiny, tiny fragment of DCs?
Though it has been vigorously promoted since the early 1980ish?
And (in all it’s science) has been unable to unseat “intervertebral subluxation” as the causa sui at any Chiropractic college? And likely in most practices is bastardized and it’s “physics propositions” simply used as one more scare tactic for upselling care volume. And wouldn’t it’s tactics be much, much, much better utilized in the hands of real kinesiologists and exercise physiologists?? Why propagate it’s ‘science’ to a profession of nuts?? Lip stick on a pig??
The “spinal adjustment” seems to add an utterly superfluous addition in CBP (as it is in all Chiropractic and Osteopathy) as “traction” is time-dependent and an “adjustment” is force-dependent. IF both are necessary, who has established the need or extent of each? And when are they co-treatment vs not? And wouldn’t a Chiropractor make more money billing ‘manipulation’ vs traction? And can’t traction be done at home…and in fact, according to Davis’s law of tissue remodeling be better done ALL day vs at an office visit of 15 mins or less??
The word ‘Chiropractic’ appearing in its moniker seems as just a plug-in to an established audience (Harrison was a DC, and like most held a probable dogmatic connection to his ‘profession’…). As always Chiropractic remains superfluous and adds unnecessary ‘goop’ to anything with a connection to real science.
Michael Kenny,
It should be noted that Dr Don Harrison, Chiropractor held degrees as a DC(Doctor of Chiropractic), MS(Mechanical Engineering) and a PhD(Applied Mathematics). He was an expert in the application of mechanical forces to the spine.
I did my post graduate internship for one year at his clinic in Sunnyvale, California and understand from observation why his son, Deed Harrison BS, DC is supporting his father’s legacy.
Michael Kenny,
Please do not be silly and think orthodontic bracing only needs to be performed for twenty minutes with a break in between before doing it all over again. Misaligned teeth in a child need constant loading because it is a deformity, like scoliosis or a hyper thoracic Scheuermann’s kyphosis present need bracing such as that developed by Australian chiropractors who developed Scoibrace and Kyphobrace. Please read the attached link.
https://www.scolicare.com/?s=Kyphosis+bracing.
At this time, I’m attending to a 12-year-old child three-four times a week($90 per visit paid weekly) and performing manipulations, exercises and traction “contortions” that already appear to be reducing his thoracic kyphotic posture but it is early days as I ‘ve been attending to him for only two weeks. Never the less I have discussed with his father and the son that bracing may be a needed option.
Remember spines move and teeth do not unless you have a severe periodontal disease from not performing regular dental hygiene habits and dental maintenance care.
Mr. Epstein
What are you talking about? Are you referring to spontaneous change in dental position or induced by traction/pressure as in orthodontic procedures?
Michael Kenny,
Part of my education as a chiropractor was a course in Rheology, a branch of physics that deals with the deformation and flow of matter. As such I can answer your question why traction for spinal remodelling purposes cannot be performed all day and why 15 minutes of traction in the office is ideal.
1. Ligaments need to experience plastic remodelling to create permanent change to their length and 10- 20 minutes of a constant load is required for ligament plasticity to occur. Viscoelasticity(1-10minutes load) is therapeutically beneficial but does not cause a permanent change to the length of ligaments.
2. The nature of many types of spinal remodelling traction requires specialised equipment and clinicians trained in the application and supervision of the procedure. In addition, even if the patient can perform the procedure at home, compliance is poor compared to supervised rehabilitation.
So should I remove my sons braces every 20 minutes? Will that remodel the soft tissue and straighten his teeth most effectively?
I did a search of the literature for ‘cervical curve restoration and it’s causal connection to human health’….and for decades only a thin veneer of value seems to pop through. Systematic reviews seem to share a common theme: it…don’t….seem….to….matter….much, if at all.
Additionally the metaphysics of pseudoscience Chiropractic biophysics is still hard at work building a bridge between the CNS, immune function and longevity etc etc And that has no piers i.e. Even IF you possess treatment acumen in such restoration and find gullible takers is it really worth the time and expense ?? It is to you as you are on the remuneration end…but what prey tell do you tell the patient? “Just ignore the systemic reviews I learned CBP from an authority….the guy that invented it”.
And since compliance is poor at home you force the patient (who apparently doesn’t really want the treatment…?) into contortions in office for THEIR benefit? And if it causes real damage and increased symptoms you simply say what? “Oops….well it’s not as bad as a stroke!”
Would that be “tractopractors”? Or perhaps “tractors”??
Mr Epstein. Your description involving the terms “plasticity” and “viscoelasticity”, seems to indicate you think of tissue remodelling as something that happens in the same way as a a child kneads Play-Doh?
Living tissue may have immediate characteristics and behaviour that can be described using terms of fluid dynamics when subjected to mechanical forces. But tissue remodelling is a process of rebuilding, not plasticity. Living tissue is broken down and rebuilt in response to long-term mechanical influence (https://en.m.wikipedia.org/wiki/Tissue_remodeling). You need to apply force continually for extended periods (ask any plastic or orthopedic surgeon, or a dentist doing orthodontics) in order to induce breakdown and rebuilding of tissue, not just temporary displacement.
Intermittent sessions of theatrical thumping (“chiropractic”) or intermittent sessions of short traction (“tractopractic”?) as this little congregation of DD Palmer’s disciples seems to have remarketed DD’s act with, are very unlikely (impossible with the former) to induce tissue remodelling of any degree.
Is it possible that you have a totally mistaken understanding of what happens in tissue remodelling?
a chiro being mistaken?
NEVER!!!
Please replace the link in my comment above with this one: https://en.m.wikipedia.org/wiki/Tissue_expansion
Note that I am familiar with using the term “tissue remodelling” in the context that we are discussing i.e. that of inducing permanent changein the configuration of tissue (skin, bone ligaments, etc.) by the application of mechanical force. The stub article on “tissue remodelling” I linked to in error, uses a more restrictive definition of the term even if it is describing part of the same physiological process that goes on when tissue is expanded/remodelled.
Note also that I have first hand experience of a variety of tissue remodelling techniques and the physiology involved. I have e.g. in my professional life* used tissue expanders and even worked with limb lengthening using the Ilizarow technique described in the above Wikipedia article. This involves protracted difficult traction over long periods. There is no possibility of lengthening a ligament or for that matter other tissues, with short sessions of traction like Mr Epstein is describing.
*I have not felt the need to use the “Dr.” prefix myself, even if I am an MD with surgery as specialty and several decades of hands on experience in manipulating human tissue. As the audience may have noticed, I resent the notion that practitioners of DD Palmer’s invention of fake tricks use such honorifics, even if they have sat on school benches for years and some of them happen to try their hand at physiotherapy, orthopedic techniques or other possibly useful services.
Dear Bjorn Geir MD,
The following link regarding the use of sustained cervical extension traction for 20 minutes three times a week resulted in a long standing increase in cervical lordosis. This was attributed to the ligament lengthening due to the visco-plasticity changes to the cervical ligaments. It is common knowledge that ligaments will permanently lengthen if under load for between 10- 20minutes. No further benefit will occur after 20 minutes in one session without some recovery time and less than 10 minutes will only have an elastic effect with no permanent lenghtening. That is why the dose response is low regarding ligament rehabilitation as only so much change can occur on a single consultation.
https://www.minervamedica.it/en/journals/europa-medicophysica/article.php?cod=R33Y2017N01A0057
Regarding the courtesy title, it is my understanding that the use of the title Dr is different in Europe than in Australia, other Commonwealth countries and the USA. I regret if my use of the title troubles you but I’m legally entitled to use it.
Yours sincerely,
Michael Epstein, DC
First of all, it is necessary to address this study once and for all, because it is getting tiresome. The link indicates that a multimodal program with added Denneroll traction 15-20 minutes, three times a week resulted in a long standing increase in cervical lordosis. The keyword here is “indicates”. It does not “prove” something. If this can be replicated without Mr. Deed Harrison, it would be nice. If this can be replicated with an object similar to the Denneroll device, all the better. 15-20 minutes it will be then…
https://www.ncbi.nlm.nih.gov/pubmed/28118272
This RCT here showed that cervical lordosis was restored just with an isometric neck extension home exercise program. The change in the intervention group amounted to over 9 degrees of change in 3 months, which is significant. Pain score also decreased. I would have reservations in attributing the changes in the study with the Denneroll device cited by Mr. Epstein solely to the Denneroll device.
Stretching, neck strengthening etc. are commonly known to restore cervical hypolordosis to an extent, often significant. Unless there is some significant underlying pathology, of course. However, in the study with the Denneroll device, cited by Mr. Epstein, even after 10 weeks of a multimodal program, that INCLUDES neck strengthening, the cervical angle from T2 to T7 did not change AT ALL. This is very strange. Could it be due to wrong measurements? Something does not seem right. I still hold my reservations anyway, mostly because of what I mention below.
Secondly, regarding chiropractic biophysics, remodelling, viscoelasticity, plasticity, etc. Applying solid and fluid mechanics IN-VIVO to biological materials is unsafe science, to say the least. It can provide a fair means for modelling, in order to study stresses, tensions, resistances and other physical measures, but it is mistaken to try to transfer the notions of plasticity and viscoelasticity directly, EVEN THOUGH identical macroscopic effects may be observable in a relatively long course of time. However, I think it is most enlightening to have Mr. Epstein let us know the nature of the misunderstandings. For one, I always found it difficult to discern what is actually wrong in the line of reasoning and it apparently always boils down to rather subtle points. I can now conceive why a man with much experience in applied mathematics, physics, engineering etc. would eventually wish to apply them in the biology of living matter (too bad they missed the “biology” part of it). I have such experience from more than one people with heavy expertise in mathematics. Unfortunately, mathematicians are very easy prey to alternative medicine practices, albeit I hope this is only my personal, coincidental, anecdotal experience.
I think one of the most important notions to get acquainted with is mechanotransduction. Inert solid and fluid materials differ strongly to living matter because they rearrange counter-intuitively in the microscopic level. This means that living matter has the ability to ignore the second law of thermodynamics (constantly increasing entropy) if compared directly to inert materials. Of course this is a grave misunderstanding, as living matter comprises open systems so there is a different correct perspective, in which entropy keeps increasing. When attempts are made to deform biological matter, it is sensed through (mostly) mechanotransduction pathways and an intricate process begins, which takes care of the restructuring, so that the END state will have the same properties, locally, as the initial state.
Deformation of inert materials alters the local properties in both the microscopic and macroscopic levels. The reason for that is that there is nothing to “restore” its properties. Glass with a crack breaks under lower external forces than glass without a crack, when forces are applied locally on the site of the crack (simple version). Exactly so, when you take a small mass of clay and lay it out to make a sheet, the larger the sheet, the lower its thickness (mass is conserved throughout deformations anyway). The more the sheet is expanded, the lower its local resistance to stress gets (as in “it gets thinner and punctures more easily”).
When biological “healthy” materials are deformed, such as skin, given that things are happening in the correct manner (enough stress to stimulate growth but not too high to cause material failure), new skin is deposited in the location of the stress, so that the new state will be under less stress eventually. Let’s give some very concise layman examples:
-As people get fat, skin is put under constant stress and its surface area expands. Through time, it can expand to twice its original area or more.
-Confer that with carrying a backpack for 15-20 minutes daily. There is HARDLY anyone who hasn’t done it in his life, I, for one, have had weeks or months carrying a backpack (~4-5 kg) in my shoulders day in, day out. My skin never increased its surface area due to these 15-20 (and much more) minutes of stress.
-Who has not carried relatively heavy grocery bags 3 times a week, for 15-20 minutes, systematically? Do their hands get longer? Do their ligaments around the shoulders get longer? No. I have been carrying grocery bags of about 6-7 kg in each hand for 15-20 minutes (~1.5 km. walk to the store) between 2-4 days a week. My hands have had the same length for the last… well, all years ever since adulthood. And people have carried such weights for even longer amounts of time quite often.
-Just walking or running puts a huge amount of stress to the ligaments of the knees and around the talocalcaneal joint (ankle). People going running for 15-20 minutes is an everyday practice (cf. marathon runners too). This is compressive stress. People don’t get shorter because of standing, not in the short-term that is. It takes YEARS (decades) for gravity to compress a body and, even so, height only decreases on the order of centimeters. However, proper strengthening can lead to avoidance of some of this loss of height.
-To talk about tensile stress, take as an example gymnasts hanging from bars. Experienced gymnasts hang for minutes on end, day after day… strong climbers can hold their bodies for more than a few minutes, time after time. Even if not 15-20 minutes, the loads applied on the ligaments are TREMENDOUS. EVEN these loads, provided the people have been adequately prehabilitated and trained, are not enough to induce plastic deformation, i.e. their hands do not get longer. Furthermore, such people, especially competitive athletes, train after adulthood and maturation, for many more years. If 15-20 minutes were enough for plastic deformation of ligaments, their hands would have to get perceptibly longer in those years.
Mr. Epstein
To clarify, you are not wrong in thinking that you can induce plastic deformation in ligaments. You are wrong in thinking that you can do it easily by modulating time RATHER than load, AND you are wrong on the time scale as well. To achieve plastic deformation in connective tissue, you need very high loads, and, just to make sure you understand it clearly, plastic deformation is a typical presentation of ligament failure, i.e. injuries.
In very simple words, the applied tractions need to persist on a time scale that is comparable to that of the corresponding tissue remodelling processes. Ligaments take a large amount of time to remodel appropriately (you don’t need peer-reviewed evidence for that, ask someone that had an ankle sprain, how long it took to get back to painless running). To contend that 15-20 minutes, a few times per week, of extremely moderate traction, is enough to elongate ligaments would mean that ligaments remodel so fast that sprains would heal in a matter of a few days to few weeks (or even less). Well, they don’t.
Dear James,
Thank you for sharing such an amazing article that is “hot off the press.” Putting aside its limitations such as knowing how stable the results are over a one year period and that the participant group is a decade younger than the Denneroll traction group. https://www.minervamedica.it/en/journals/europa-medicophysica/article.php?cod=R33Y2017N01A0057. If we go back to the beginning of this whole dissertation, reducing spinal misalignments strongly suggest better health outcomes for patients.
It should also be noted that that chiropractors were the most frequently cited authors in this most interesting paper. Again may I thank you for sharing.
The cervical lordosis is primarily governed by posture, not length of ligaments. Try nodding your head. That is an act of changing the lordosis back and forth. Anyone with experience of ER work knows how this postural aspect, as seen on an x-ray, changes after e.g. neck sprain or with headache and is normalised again when the patient has recovered, with or without any intervention. A change in measured lordosis (the natural curve of the spine) before vs. after such manipulations is very, very unlikely.
I admit that I do not have the time now to have a good look at your reference at this moment, but I dare guess that the change these people are measuring has nothing to do with tissue remodeling at all. Maybe I’ll come back to this but do not rely on it, I have better things to do than analyze unlikely research papers
With all respect Mr. Epstein, law is not medicine and can be in error as well. Your legal rights to use the honorific in question is I guess limited to the US? America is only a small, insignificant part of the medical world 😉
You can call yourself anything you like as far as I’m concerned. I am not aware of any law that says anyone is required to address you with this title. My not using the title when addressing or referring to you is not to belittle your person but to emphasize the fact that it is wrong to confuse chiropractic, a useless set o make-believe, with medicine and science. Chiropractic is the correct term for the set of theatrical tricks devised by DD Palmer and has nothing to do with efficacious health care. The fact that there are chiropractors who dabble in useful treatment techniques that may belong to real health care (i.e. have a real effect), that does not validate DD Palmer’s theatrical thumping or the fake phenomena he invented to fool his clients.
I accept your opinion but do not agree with anything you have stated in relation to your last reply. It is untenable for health care concepts that existed prior our understanding of human homeostasis and the discovery of antibiotics to be promoted today as representing the philosophy of chiropractic in 2017 as much as it is untenable for medicine to be currently represented based on the philosophy of the age of heroic medicine when purging and leaches were common practice.
Mr. Epstein.
You proudly decorate yourself with the “Dr.” title but your epistemic performance indicates there is hardly any (real) knowledge of medicine, biology or physiology behind it.
Whatever you learnt in chiro-school has not left a working understanding of how living tissue functions and reacts to external influence. The mentors and “researchers” you refer to, seem just as delusional.
You go on about tissue behaving like Play-Doh putty. That is plain and simply not how tissue behaves.
James has (on Thursday 17 August 2017 at 12:58) further elaborated in support of my explanation of this. I do not have to add anything to his thorough exposé.
James has, as I also tried to do, also explained that the normalisation of the cervical lordosis over time is to be expected as a result of physiological recovery from injury/dysfunction. It is not and cannot be a result of the silly theatricals resulting in imagined ligament lengthening through intermittent, minor mechanical influence.
I have alredy explained how and why I have the education and experience to say this. It has been my job for decades to know these things.
If you wish to distance yourself and your ailing dignity from what you call
and enter the era of rapid and effective medical progress, then you will have to not only stop calling yourself a chiropractor and forget the nonsense and fantasies you learned in chiro-school. You will also have to study and show genuine competence in a real science based health care field. Until then you are nothing more or less than a totally misinformed disciple of the charlatan magnet healer DD Palmer who invented his tricks without any backing in knowledge or experience and least of all in science. That is to say, you are only a ‘chiropractor’, which means in effect you are in the entertainment business, not medical.
Ligaments are not play-doe. They are serious physiological components of the human body that can break or make a person’s life!
Of course not Mr. Epstein. That is what I said. Why don’t you read my comment again. You do not seem to be comprehending what I am saying. Read it slowly this time and contemplate how it relates to your own claims of how ligaments can be affected by mechanical forces. Try looking up the terms you use in a dictionary and read up on how ligaments, bones and other tissues remodel under the influence of mechanical traction or pressure.
I live in Sydney Australia and can use the title, Dr throughout the whole Commonwealth of Australia and New Zealand. I’m a citizen of the USA, Australia and permitted permanent residency in New Zealand.
@Mick Epstein on Friday 18 August 2017 at 08:36
Mick,
it does not matter to what the law entitles, you are a quack practicing quackery. You aren’t even qualified to lance a boil and suture the wound, let alone operate on tumours or anything with a hint of seriousness. You faff around with the backs of the worried well, steal their money, pretend to provide health care, and massage your mighty ego, all the while doing sweet eff all in real health care.
I would like to see you confronted with a real medical problem, such as a ruptured appendix, and watch you poo your pants. Unfortunately, that would be unethical to place any human being in a position of requiring real medicine but sending them to a quack-meister.
Micky, you are delusional.
Dear Frank,
If I was confronted with a patient with acute abdominal pain, which I have and resolved very quickly after palpating its severity and determining that the pain was manageable after performing SMAT. Stay tuned to my publication of this procedure next month or in October in the Chiropractic Journal of Australia. It’s not a case report about abdominal pain management but the mechanism of the procedure itself. I look forward to your critique of this published paper. Remember, publish or perish.
Mr. Epstein
Today at 09:01 you stated:
Can you please confirm that in the above cited comment, you are stating that in your capacity as a licensed chiropractor in Australia, you have taken upon yourself to diagnose and treat patients with complaints of abdominal pain?
Do you have the qualifications and licensing to do so? I can not find any reference to such education and qualifications on your website.
Can you please also elaborate on the nature of the “procedure” you are alluding to?
@Mick Epstein on Sunday 20 August 2017 at 09:21
Micky,
What was the diagnosis? Did you perform this “palpation” in the hope of finding a diagnosis or was it the “cure”? You are very amusing, for all the wrong reasons.
@Mr. Epstein
You never responded to my questions as promised. Did you forget?
The paper you mentioned finally came out.
http://www.cjaonline.com.au/index.php/cja/article/view/168
I read through the opus and have to say I am flabbergasted. Primarily as to why it was accepted for publication. There is no way I am going to spend an entire day properly writing up the plethora of comments and concerns I have for this attempt at scientific writing. I will only ask a few of them for now. If I had been asked to review this paper for a medical journal (which would not be likely as this would not get past most proper medical editors at all) I would have asked these and many more questions and declared this work as not publishable. I would have suggested you might be welcome back when you had done a proper pilot study and a manuscript that conformed to accepted standards.
Anyway, for your benefit here are some of my concerns:
> Where do you declare and describe the scientific/ethical review board approval of this human experiment or was this omitted. Is that legal in your country or in Bali where at least part of the studies seem to have been made, even if only one human subject was involved?
> Why is there no mention of the characteristics of the single subject investigated. Sex, age, height and weight, previous medical history, ethnic background etc.? Such information is considered normal and even essential in medical reports and studies and usually supplied in a table.
> How was the effect of abdominal and spinal muscle guarding taken into account? Lying on one’s back with a heavy load on the belly induces a defensive muscle activity, which varies with physical fitness, tiredness and many other factors. There is nothing surprising about the aorta not being compressed, that is because it is protected by this guarding. Also the skeletal structure and its ligamentous connections are protected from abnormal loads by this muscular activity. I would have understood your concerns if you had put the subject under general, muscle relaxed anaesthesia for the experiment. The numerical differences in your multiple measurements seem generally to be very small in absolute terms and even relative terms so one wonders if they are not significantly confounded by the factors affecting muscular strength and endurance at different times between and within sessions.
> In the paper you say, at the end of the discussion section:
“It should also be noted that there was a significant reduction in frequency, severity and intensity of upper quadrant abdominal pain and bloating symptoms the participant was experiencing.”
You also mention this in the conclusions. How is this seemingly incidental, a-posteriori observation significant to the purpose and outcome of the experiment and what is your reason for including it?
Do you really believe this was not incidental??
> What was the time between first submission and final acceptance? This information is usually provided by the publisher but I am unable to find it.
I am sorry to be so harsh but this must be the longest, endpoint-inflated, over-interpreted, doubtfully useful, report of an N=1 experiment mislabelled as a “case report” in the whole history of health related publication?
Oh, my! 😀
I guessed wrong. Perhaps influenced by an american stereotype that has been so prominent lately? 😉
Well, you may have the right to decorate your letterhead, I never claimed otherwise, but that does not make the make-believe medicine DD Palmer invented any better and I am not aware of any law or regulation that requires me or anyone else to use this rather confusing title when referring to your person?
Bjorn, can you tell us where and when you obtained your licence as a medical surgeon? Also, can you tell us of any medical papers that you have published?
(The GMC reference number for a ‘Bjorn Geir Leifsson’ is 6086747, status: ‘temporary registration expired’)
I think Bjorn should only answer this once you have produced the equivalent data about yourself.
and even then it would be a monstrous ad hominem attack.
A tip or two for you, Greg:
Try to look up the meaning of the words “temporary” and the word “expired”. Then think hard about how they relate to each other. Maybe one day you will understand the GMC-riddle if you think hard enough 😉 I also had a license in another english speaking country, long ago. Can you find which and when?
I will give you another clue, to make your search more exiting: I am a currently licensed doctor and surgical specialist in more than one country. Can you find them all and perhaps the years they were issued? Can you also find my second medical specialty that I am certified in?
If you have problems finding information of this sort, maybe a librarian is willing to assist you. Let her or him show you how. You need to learn
There is a library in your village, right?
It is the 2nd time that I have asked the same questions and you are refusing to answer. Answer the questions Bjorn.
First time was on the blog: Death by homeopathy
‘Seeing that you were so interested in researching Dr. Mathie’s background; let’s have a look at yours:
Cand Med et Chir, 1983, University of Iceland. Did you obtain any specialist qualifications?
Last date on register of practitioners 2005?
Did you write a dissertation? What was the topic?
What scientific papers on medicine have you published (Edzard has done MANY)?
Do you have any training or qualifications in homeopathy?
Bjorn, are you bluffing the readers of edzardernst.com?
Greg, are you bluffing the readers of edzardernst.com pretending you have a functioning brain?
Dr. Ernst: Considering your background, and averring for several years to be ‘expert’ in all sorts of health practices that you are not qualified in is funny. Have you forgotten that you were fired from your post http://edzardernst.com/2013/03/ive-been-fired/) and that you were terminated in your post as ‘Professor of Complementary Medicine’?
As I have said before, the primary element of this blog is the humour that arises from reading stuff you and Bjorn write (Bjorn’s ‘sarcastic heckling’ is excessive in my view, his discussions with John are something to read), but there is an educational element as well: you are not educated in the topics you are discussing here.
Is Edzard a Walter Mitty type ‘professor’?
Edzard, is it taking your brain some time to think through my previous comment that you have not yet posted?
It is true though, isn’t it: that you have effectively been let go twice from jobs involving ‘complementary medicine’?
This one you called: fired
1. http://edzardernst.com/2013/03/ive-been-fired/
2. University of Exeter post as Professor of Complimentary Medicine, you called: RETIRED
https://www.timeshighereducation.com/news/research/research-intelligence-alternative-outcomes/416567.article?sectioncode=26&storycode=416567&c=1
What a sad way to go, after all the work you did.
If “Greg” had asked nicely I might have given a few more hints. When “Greg” has given its full confirmable credentials and CV, I promise I will provide the (easily found) link to my whole profile including publication list. ?
Waw Bjorn, you want to be asked ‘nicely’ but you have recently ‘apologised’ for your ‘sarcastic heckling’ of commenters that believe in alternative medicine. It fits the picture.
There is a limit to how much fun a cat can have from playing with a mouse, especially when that mouse has no talent for the game.
The title of this blog post is “Is chiropractic subluxation a notion of the past? SADLY NOT!”
I think Edzard has shown great patience by allowing you to rant and rave about unrelated topics, rather no topic at all.
I am guilty of encouraging this folly by playing the role of a cat 🙂 It is time to stop.
You grandiously demand respect but show little yourself.
You boastfully demand answers to your questions but answer close to none yourself.
You haughtily demand that I inform of my credentials but give none yourself.
My professional information is so easily found that it must take either lack of education above preschool or a significant mental handicap to avoid finding it. As I said before, you can ask the librarian in your village to help you with the search.
I am not going to humour you by revealing the one single link you need to find the information about me that you are asking for.
Let’s see if a last little hint will help you solve your embarrasing predicament:
On this very page you can find a feature that can click on and open a page to an outside resource. On the page that opens you will find this link to my profile 😉
Bjorn: See above:
‘Mr. Epstein.
You proudly decorate yourself with the “Dr.” title but your epistemic performance indicates there is hardly any (real) knowledge of medicine, biology or physiology behind it.
Whatever you learnt in chiro-school has not left a working understanding of how living tissue functions and reacts to external influence. The mentors and “researchers” you refer to, seem just as delusional.
You go on about tissue behaving like Play-Doh putty. That is plain and simply not how tissue behaves.
James has (on Thursday 17 August 2017 at 12:58) further elaborated in support of my explanation of this. I do not have to add anything to his thorough exposé.
James has, as I also tried to do, also explained that the normalisation of the cervical lordosis over time is to be expected as a result of physiological recovery from injury/dysfunction. It is not and cannot be a result of the silly theatricals resulting in imagined ligament lengthening through intermittent, minor mechanical influence.
I have alredy explained how and why I have the education and experience to say this. It has been my job for decades to know these things.’
Bjorn, you don’t answer a straightforward question: where did you train as a medical surgeon and on which register are/were you?
http://edzardernst.com/2017/05/a-method-of-ending-discussions-with-belligerent-twits/
Greg-
What would ‘training’ or “qualifications’ in homeopathy consist of?
What qualifications are needed to become an expert in mumbo jumbo?
A few years agoI stood behind a young woman in a newsagent’s who was holding such a ‘qualification'” which she was waiting to have photocopied( and, afterwards, framed, I expect).
It said ‘This is to certify that( (name) has successfully passed an examination in aromatherapy’.
Is that the type of thing you’re talking about?
In some countries (UK), you don’t need a qualification in homeopathy to be a homeopath (this has been discussed in the past with Alan and Simon). So, you can be a ‘homeopath’ if you live in the UK and you wanted to be one.
The question here is what are Bjorn’s medical qualifications as this is pertinent to his regular provision of medical commentary on this site (‘It has been my job for decades to do these things’).
It is an easy question for him to answer but he does not answer it.
no!
it is not the question at all – it is your question.
why don’t you look him up before you make a fuzz?
Oh, yes. How come it wasn’t obvious earlier… C’mon, spill it out… You like JAQing off right? (JAQ is short for Just-Asking-Questions)? You discovered this technique of rhetoric the other day and you are here to practice, huh?
So, the simple reason that he won’t answer to you (apart from the fact that it is utterly needless, as the stuff is available online), is that it is COMPLETELY out of the matter at hand. What is the reason you request it so persistently? Will it change your life? What is your course of reasoning on that matter? You are trying to make a point? You think that by not getting a direct answer, you will somehow prove that he has some special reason for not providing a straight answer? You believe he does not have medical qualifications? You believe you can trick people in here? Your tactic is that of question-flooding?
You think you can fool anyone into believing that there might be something fishy or catchy behind the fact that Björn does not answer straight away? Who are you? What are YOUR scientific qualifications? Did you finish high school? Where is your high school certificate? It is a straightforward and easy question. I will ask it for twenty consecutive posts, yet you will not be able to procure all the data I am requesting. This constitutes reasonable doubt that you have any credentials, doesn’t it?
Do you get +1 point for evoking every additional comment here responding to one of your answers? Do you make money out of this? Is there a bet we should be aware of? Are you intentionally getting on peoples’ nerves?
You already can find the data you are asking for. Why do you want them here posted by Björn? To be able to quote them afterwards as having been mentioned by Björn himself, so that you can keep trying to make void points? And, after that, what? You are going to find a different question, and keep posting that a million times? If you want to flood the comments section, be clear about it.
What was that again?
“It is the 2nd time that I have asked the same questions and you are refusing to answer. Answer the questions Bjorn.”
Who are you Greg? The Grand Jury? The Inquisition? A stooge for homeopathy? A shill for alternative medicine? An expert in anything, maybe? Where are your qualifications?
“Dr. Ernst: Considering your background, and averring for several years to be ‘expert’ in all sorts of health practices that you are not qualified in is funny. Have you forgotten that you were fired from your post http://edzardernst.com/2013/03/ive-been-fired/) and that you were terminated in your post as ‘Professor of Complementary Medicine’?”
Do you know of any job position that lasts forever? Who are you Greg? When was the last time you held any post? What post was that?
Wow, now you are going to accuse me of “ad hominem” attacks (how typical)? Not too complicated…this is just you looking in the Internet mirror. Welcome!
Let me end with your trademark signature…
…
You guys are so much fun.
Greg
In most real professions you do in fact need some kind of qualifications
In other areas- such as football for instance, or my previous profession of
illustration- qualifications may well be slightly mote abstract.. That is to say the abi
Ity to bang the ball into the net, or keep the ball out of the.net,Or to contribute to these ends.
No academic qualification needed in other words, but demonstrable proof that an argreed result had been achieved. In my case an example might be a photo realistic drawing for VW cars. A clear target set. a clear target achieved, with no hocus pocus to fool the client either needed or attempted.
Greg
There was a fashion among reggae singers a few years ago for calling themselves whatever they felt like sand so for a while there was a black Clint Eastwood and indeed a similarly tinted’Lautel and Hardy’.
‘Dr’ Gillian McKeith didn’t go quite so well however. at least among the more questioning.
Barrie
Dr Rawlins is a doctor of medicine – from 1969 and on the GMC register (although now retired) as a specialist – from 1996 (trauma and orthopaedic surgery). Bjorn refers me to his ‘profile’ link and James gives a long statement regarding Bjorn not answering straightforward questions.
Bjorn has stated his credentials before, what I am asking is for substantiation. Why? You can figure that one out Barrie.
we have all figured this out – it has nothing to do with Bjorn; the answer lies in your state of mind.
Edzard, how come you and James have to write comments on Bjorn’s behalf? In my view, Bjorn has subjected many people on this site to questioning of their background and ‘sarcastically heckled’ them, now he is not providing a simple answer.
So why are you jumping in here?
Also, who is WE? (you and James?), and what is THIS that you have FIGURED OUT?
I have always been intolerant of extreme stupidity
“So why are you jumping in here?”
I had a false sense of freedom of speech and thought I would make use of the right to exercise it for a few minutes.
Let’s, once again, in good faith, attempt to set straight some wildly pre-school type of reasoning that takes place.
Björn has subjected people to questioning of their background, when the matter at hand was their knowledge. They exhibited ignorance of basic knowledge on a subject. Then, their background was questionable, so it became the matter at hand. Thus, Björn’s asking was not an “ad hominem” argumentation, it was a question regarding the MATTER AT HAND (the knowledge of the people). Now, Björn himself has never shown ignorance of basic knowledge of any subject discussed herein. Thus, he has never ever given even a hint of a right to question his own qualifications and knowledge.
Reciprocating a behavior MIGHT be justified at times, but if you want to do it RIGHT, you have to carry it out on SIMILAR (or, even better, identical) terms. So, people exhibit blatant misunderstanding of some area of science and some others (Björn for example) may question them about where they obtained this mistaken knowledge of theirs. If you want to reciprocate this kind of behavior, you have to first make a case about some scientific statement of Björn that you believe is mistaken, and then, we can talk about whether Björn was indeed wrong on that. If reasonable doubt is substantiated, THEN you may go on asking about qualifications etc. As far as I am concerned, all I have seen of Björn’s expositions is a sound knowledge of multiple areas of science, a fact that substantiates the view that he is actually extremely well informed and knowledgeable as a scientist.
Needless to add that you have been wrong multiple times before, in terms of science. I don’t know about “we” (which is probably much more people than me and Edzard), but I, for one, have all the good faith and hope that you can understand the usefulness of learning the correct things, once you know that you are wrong with something. Why don’t you decide to improve?
And cut it out with Björn, you are hijacking these threads with irrelevancies all too often. Is chiropractic subluxation a notion of the past (sadly, not)? Talk about that, if you will.
Mr. Epstein
On Sunday 20 August 2017 at 12:18I asked you a very important question.
If you are still following this blog, or when you come back, will you please respond?
He became entangled in one of his ligament-traction-devices and developed his own acute abdominal pain.
Regrettably as the only Chiropractic in Australia that knows what he’s doing he has no one to help him.
I gather our friend Mr. Michael Epstein, an Australian chiropractor found it best to leave this blog when confronted with the question whether he was treating patients with abdominal pain. Despite his until then ardent commenting, he has not posted any comments since, that I have found.
I suggest, if there are any Australians reading this, especially from Sydney/New South Wales, that they send the health authorities in that region a “heads up” about this bombastic chiropractor and his stories that indicate he may not be fully respecting the limits of his licensure.
The pertinent comment of chiropractor Epstein (copied form further up in this thread), and my following question, which he has not seen fit to respond to:
It will be interesting to see if his (possibly revealing?) paper appears as promised in the October issue of The Chiropractic Journal of Australia, a publication mostly filled with boastful chiropractic anecdotes and wishful monologic attempts at substantiating the intangible “subluxation complex” (example)
I’ll reply over the weekend. Early days and late evenings with patients and a Bar Mitzvah in between does not make me a good correspondent.
Concocting science fiction and defending-the-indefensible does take one away from the pursuit of saving the human race from subluxation….and making lucrative bank deposits.
Mick,
Just to correct you on this, “Early days and late evenings with patients”, the word is “victims”.
Can anyone comment on Canadian chiropractic practices? I have met one in particular who thinks his education puts him on par with a family practitioner.
certainly a bogus and dangerous claim
I agree. He is particularly insistent; he was insistent that Canadian chiropractic is somehow different in curriculum from other chiropractic schools. Their education is superior he claims and this he is at the level of a family practitioner. hmm. I ask if he has ever worked in a hospital or managed a ward? Of course he hasn’t but still has no thought to pause for a second and wonder. Dangerous indeed.
I think Canadian (and worldwide) Chiropractic can best be summed up in the phrase:
“The gullible and their money are soon parted”.
M.K., your version of the physiotherapy profession can be described as “Fake, bake and shake, with a touch of Hands on Homeopathy.”
My “version” of the physiotherapy profession?
I mentioned elsewhere that studies show: “PT” (physiotherapy in your words) shows a negative-effect on (as an example) LBP when overall costs vs outcomes are factored in.
That is, “PT” (and Chiropractic as well) has scant little REAL benefit for people with LBP vs standard care (or NO care).
I recognize that “treating away” LBP with multiple “sessions” is financially motivated and an illusion in virtually all cases (how many DCs say or believe that??)…..80% of back pain is utterly self-limiting/self-healing, 5% surgical, 10% psychological and the last 5% in need of multi-factorial care. However for those who may benefit from care certainly any rationalist would want a PT or DPT (not a DC) on that team.
I don’t disagree that PT has its very real issues….however it is not a non-falsifiable religious dogma with net-work marketing business schemes and scams at it’s core.
That people get inappropriate or damaging surgeries doesn’t somehow lend credence to the development of another “surgery-like-but-based-on-nonsense” profession that has no idea what they are actually doing to fill-in when real surgery fails. Or am I missing something here?