
Updated Edition!
 for Cancer")





")









![]()

During the last few days, we were entertained by one of the more fanatical specimen of the lunatic fringe. From the outset, ‘ASTRO’ was out to provoke, insult, and foremost state utter nonsense. Within just a few hours ‘ASTRO’ posted dozens of comments, one more hilarious than the next.
As always, I let it pass for a while because this sort of thing usually is very amusing and mildly instructive. Then, when my fun was over, I told him or her that my conversation with him or her was finished, thereafter I sent ‘ASTRO’ my usual hint to indicate that my patience was wearing thin (an overdose of nonsense, fun, and hilarity might be toxic) and now I have blocked ‘ASTRO’.
This little incident is a mere triviality, of course. Yet, it is also a most welcome reminder to demonstrate what is needed to get blocked by me. Here are a few selected ‘bon mots’ posted by ‘ASTRO’ which all contributed to his or her dismissal from this blog:
- Lenny is an intellectual terrorist
- you manipulate data
- you are nobody in the scientific world
- I’m very sorry for your lack of education
- I don’t hate you for lying, I pity you
- With all sincerity, and seeing that you don’t have a single scientific publication, I recommend that mounts a business for atheists resentful and sell cheap products with the face of Carl Sagan or James Randi in a coffe cup or pins, I assure you that the media will make of your business, earn some money and you’ll be able to publish a book trash like Ben Goldacre, with his “Bad science” or the Steven Novella. Poor quality is a typical sign of skeptical pseudoscientists.
- your “letter to the editor” is based on manipulating data and making false accusations, everything
- you only have an opinion based on your belief and denial that may well be a projection of your lack of knowledge
- I’m disappointed that you have very superficial knowledge, no wonder Mathie will ignore you
- Your comments again reflect that you haven’t the slightest idea
- your lack of reading comprehension is evident
- You are very ignorant
- your aggressiveness and lack of empathy tell a lot about your profile of atheist resentful of life
- these” verdicts ” that Ernst quotes in his pamphlets are at best a fraud
- in reality you, Grams and the team of the anti-homeopathy propaganda network have no idea what you’re talking about
- Ernst,” friend, ” you’re still pretty aggressive, maybe you need some joy in your life. Now I understand why the pseudoscientific skeptical atheist community is so childish and so toxic
- anyone who questions Edzar’s sacred dogmas is a troll
- Thank you for confirming that you are a sectarian
- your obsessive behavior borders on harassment
- Magazines like Skepter are very popular with immature gentlemen who believe they are the world or with teenagers who are just out of college who believe that science is done with whims
- don’t be like Lenny and try to grow up
- real science is in the objective pursuit and not in harassment campaigns orchestrated by a few clowns who believe James Randi is unquestionable
- every time I read your entries I feel sorry that your level of logic is so low and lousy
- Your naivety and superficial knowledge in philosophy of science (and that of most of those who follow you) is very pitiful
- you are the example of a pseudo-sceptic, a rude and cowardly skeptic who can’t tolerate criticism
- your friends are a sect, possibly a group based on coertion
- it doesn’t look like “Lenny” has a single scientific article published, not to mention your colleagues in the “About” section that the few who look like scientists are mediocre in their fields, the rest are small-time activists. No wonder, so much envy, so much anger, so much hatred, that’s what leaves fanatical atheism. They’re talibans of science, not scientists
- you with your age presume a lot and I only see you being interviewed by mainstream media that talk nonsense against homeopathy
- You had to control that aggressiveness, you feel more nervous and angry, maybe you’re a relative of the troll Lenny
- The obsessive behavior of Aust trying to refute Frass already looks like that of a stalker, similar of the journalist Christian Kreil who invented a whole string of nonsense in a German public media trying to link Frass to a questionable company, the media does not even mention Frass’s refutation to Kreil
One thing we cannot accuse ‘ASTRO’ of is that he or she was not industrious. You might ask why I did not stop his aggressive stupidity earlier after it had stopped being funny. Perhaps I should have – but, to be honest, these trolls do amuse me a great deal. More importantly, they might teach us important lessons:
- The fun one can have with fanatics is usually short-lasted.
- Some weirdos are very well misinformed, i.e. they read a lot and misunderstand even more.
- The minds of heavily deluded people are beyond productive discussions.
- Any hope to educate them will be disappointed.
- If we allow them to, they swiftly make themselves ridiculous.
- Their pseudo-arguments are strikingly similar.
- Their aggressiveness can be considerable.
And finally, the little ‘ASTRO’ interlude tells you something else:
It really does need a lot to get banned from my blog.
By guest blogger Ken McLeod
RICHARD MICHAEL NILSSON is the owner of Colloidal Minerals Australia Pty Ltd, ACN 003 484 955, of Wyongah New South Wales (NSW), Australia. On August 13 he was convicted in the Wyong Court, after pleading guilty to offences including intimidation with intent to cause fear of physical or mental harm.
Nilsson is a prolific antivaxxer, deluging unlucky politicians, journalists, health officials, etc with emails containing misinformation about vaccines and warning of the dire consequences to come to anyone involved in vaccination programs. He has been known to harass and threaten. Usually recipients have better things to do than engage with a crank, but he has been known to go too far.
As the Sydney Daily Telegraph reported on 14 August 2021: “Anti-vaccine activist Richard Nilsson pleads guilty to sending death threats.”
“A Central Coast anti-vaccine campaigner who sent death threats to The Sunday Telegraph journalist Jane Hansen has pleaded guilty to the charge of using intimidation to unlawfully influence a person.
“Richard Nilsson, 66, from Wyongah, sent an email to Ms Hansen’s work email address on the evening of February 27.
“The subject of the email was “WHEN IS A MURDER WARRANTED? YOURS, YES?”
The contents of the email read: ‘I am proposing that your murder might well be a celebration of not life but death! And what a celebrated and glorious one at that!
‘I know ten thousand that would do it, but of course it only needs one and you will never know until it is too late!
‘I expect you might meet your maker, maybe in the near future … the sooner the better, yes?’
“Ms Hansen has reported widely on vaccination since 2013 when The Sunday Telegraph launched the No Jab No Play campaign, and more recently has reported on the vaccine rollout for Covid-19.
“On February 27, the evening the email was sent, Sky News re-ran a documentary made by Ms Hansen called Big Shots, which looked at anti-vaccine activity in relation to the pandemic and the vaccine rollout.
“Mr Nilsson followed up his email with another with the subject line: “WHEN IS SLUT NOT A SLUT AND IS A SELECTIVE SLUT STILL A SLUT?” before launching into a barrage of abuse.
“Mr Nilsson, who runs a business selling colloidal silver, faced Wyong Court on August 11 and pleaded guilty to a charge of use intimidation/violence to unlawfully influence a person.
“He received an 18-month Community Corrections Order to be of good behaviour.
“Ms Hansen said threats to journalists who write on the subject of vaccination were not unusual but Mr Nilsson’s emails were unsettling in their violence.
‘All journalists get abused on occasion, especially on the currently highly emotive topic of vaccination, and mostly it is best ignored but this email was next level and no one should have to put up with such vile abuse,’ she said.
“Mr Nilsson is well known by politicians, who have also received numerous emails from him suggesting all manner of conspiracies, including that Covid vaccination is a mass depopulation exercise.”
Nilsson appeared before His Honour Ian Guy in case number 2021/00159728, R V Richard Michael Nilsson. He was convicted of stalking or intimidation with intent to cause fear of physical or mental harm, an offence under section 13 of the Crimes (Domestic and Personal Violence) Act 2007 (NSW). This attracts a maximum penalty of 5 years imprisonment and/or $5,500. He could also have been convicted of using a carriage service to menace, harass or cause offence, an offence under section 474.17 of the Criminal Code Act 1995 (Commonwealth of Australia). That carries a maximum penalty of 3 years imprisonment.
He was sentenced to a Community Corrections Order requiring him to be of good behaviour.
A rational person would have thought themselves lucky that they had avoided years of a high-fibre low-calorie diet of porridge and baked beans, but we are not dealing with a rational person here.
Hardly was the ink dry on the Court file, than on the 15th, two days after he was found guilty, Nilsson pounded his foam-flecked keyboard and sent another rant in an email to 130 people and organisations, including politicians, Skeptics groups, a Radiation Oncologist, government departments, doctors, political parties, people in the horse-racing industry, scientists, journalists, lobby groups including climate and conservation organisations, mental health groups, the National Security Hotline, and a coal mining company.
It reads: “Subject: FW: The Hidden Victims of the Covid Vaccine and why I included you all in this email…
“When will it be that enough lives have been ruined and enough have been murdered? And when will the maiming and the killing end?
“My hope is that some of you here own up and confess (I know who among you are in this group and I suspect in time you will all pay a heavy price for your crimes and transgressions), while others it is incumbent upon you to inform all those you purport to represent that the maiming and killing that has transpired and of course is inevitably and scheduled to transpire will continue until such time we say: f_ ck you!
“I know, and some of you know too, who the traitors are. Scott Morrison is just one and Greg Hunt is another and of course Jane Halton, Brendan Murphy and Paul Kelly are other worthless humans and are included and we know they are just tools – plasticised and fake as they are.
“I have an incomplete list of those who need to answer for their crimes and it does not include all I have included in this email.
“Add a Mr Skerrit. His evilness is seen in his face and in his utterings and communications and his connection with Jane Halton and the WHO and the so-called, Australian Health (sickness proliferation) Dep’t and Event 201 should not be lost on anyone with brain cells that still operate and are able to coordinate.
“Wake the f_ _k up!”
All emphases and redactions above are as in Nilsson’s email. Scott Morrison is the Prime Minister, Greg Hunt the Commonwealth Minister for Health, Brendan Murphy is a former Chief Medical Officer (CMO) of Australia and now Secretary of the Department of Health. Paul Kelly is the current Chief Medical Officer, the “Mr Skerrit” he refers to is Adjunct Professor John Skerritt, Deputy Secretary, Health Products Regulation Group, Therapeutics Goods Administration. “Jane Halton” is a former Secretary of the Commonwealth Dept of Health, now Council Member of the Australian Strategic Policy Institute.
The “Event 201” that Nilsson refers to was a tabletop exercise conducted in October 2019 by the Johns Hopkins Center for Health Security (CHS), the World Economic Forum and the Bill and Melinda Gates Foundation in New York City. According to the CHS, “®he exercise illustrated areas where public/private partnerships will be necessary during the response to a severe pandemic in order to diminish large-scale economic and societal consequences”.
Event 201 simulated the effects of a fictional coronavirus originating in bats but passing to humans via pigs. Claims that Event 201 was a rehearsal for the COVID-19 pandemic have been debunked by fact-checking outlets such as USA Today and FullFact, but facts have never matter to antivax conspiracy theorists and other assorted cranks. All emergency response authorities and health bureaucracies conduct exercises to identify threats and to develop and improve response plans. There was nothing unusual in “Event 201” except in the fevered imaginations of nutters and fruitloops.
Does Nilsson, with no qualifications whatsoever, really think that he knows more about emergency response and immunology than those distinguished experts, and all the scientists researching Covid19 and vaccines? How does 20 minutes reading email conspiracy theories trump PhDs, professorships and Nobel Prizes? How conceited does someone have to be to imagine that? Where is the boundary between conceit and dementia? So does accusing honourable people of ‘crimes and transgressions,’ ‘maiming and killing,’ being ‘traitors,’ are evil tools, ‘who need to answer for their crimes’ constitute the good behaviour that the Court imposed? And coming within hours of the Court hearing?
Watch this space.
In their 2019 systematic review of spinal manipulative therapy (SMT) for chronic back pain, Rubinstein et al included 7 studies comparing the effect of SMT with sham SMT.
They defined SMT as any hands-on treatment of the spine, including both mobilization and manipulation. Mobilizations use low-grade velocity, small or large amplitude passive movement techniques within the patient’s range of motion and control. Manipulation uses a high-velocity impulse or thrust applied to a synovial joint over a short amplitude near or at the end of the passive or physiological range of motion. Even though there is overlap, it seems fair to say that mobilization is the domain of osteopaths, while manipulation is that of chiropractors.
The researchers found:
- low-quality evidence suggesting that SMT does not result in a statistically better effect than sham SMT at one month,
- very low-quality evidence suggesting that SMT does not result in a statistically better effect than sham SMT at six and 12 months.
- low-quality evidence suggesting that, in terms of function, SMT results in a moderate to strong statistically significant and clinically better effect than sham SMT at one month. Exclusion of an extreme outlier accounted for a large percentage of the statistical heterogeneity for this outcome at this time interval (SMD −0.27, 95% confidence interval −0.52 to −0.02; participants=698; studies=7; I2=39%), resulting in a small, clinically better effect in favor of SMT.
- very low-quality evidence suggesting that, in terms of function, SMT does not result in a statistically significant better effect than sham SMT at six and 12 months.
This means that SMT has effects that are very similar to placebo (the uncertain effects on function could be interpreted as the result of residual de-blinding due to a lack of an optimal placebo or sham intervention). In turn, this means that the effects patients experience are largely or completely due to a placebo response and that SMT has no or only a negligibly small specific effect on back pain. Considering the facts that SMT is by no means risk-free and that less risky treatments exist, the inescapable conclusion is that SMT cannot be recommended as a treatment of chronic back pain.
By guest blogger Wolfgang Denzer
Most pseudoscientific studies related to the explanation of the proposed mechanisms of homeopathy used tadpoles, wheat, or watercress as models. Results of these studies, e.g. those by Endler, Baumgartner & Co., were published in dedicated SCAM (So-Called Alternative Medicine) journals where the peers who review manuscripts have a clear tendency to support non-evidence-based studies in particular those that deal with homeopathy. In recent years several papers were published in reputable journals (see below) that purport the efficacy of ultrahigh dilution (UHD). None of these publications relates directly to homeopathy or even uses the term “homeopathy”. One thing the publications have in common is that they were either sponsored by the Russian OOO [sometimes LLC] “npf” Materia Medica Holding or co-authored by staff of that company. Materia Medica Holding produces and markets ultra-high diluted remedies that are called ‘release-active’ drugs (RA-drugs). The company founder rigorously states that their remedies are not homeopathy and that „homeopathy is doomed to have a marginal position in the modern system of therapy“. (see interview link at the end). Already a few years ago Panchin et al. (2018) analyzed several papers that involved Materia Medica Holding in one way or the other and published an article in BMJ Evidence-Based Medicine (Drug discovery today: no molecules required. http://dx.doi.org/10.1136/bmjebm-2018-111121). His remarkable conclusion was as follows: “Surprisingly, these innovative “drugs” contain no active molecules and can be considered a new brand of homeopathy. This indicates one of two possibilities: either we are at the brink of a revolution in medicine or that something went wrong with research published in numerous academic journals.” Of course, the latter assumption is correct.
The difficulty to uncover the use of an ultra-high diluted homeopathic (oops) remedy instead of proper medication published in a study is best shown by having a look at the following publication co-authored by the founder of Materia Medica Holding Oleg I. Epstein and two of his employees:
Pathogenetic approach to the treatment of functional disorders of the gastrointestinal tract and their intersection: results of the Russian observation retrospective program COMFORT (BMC Gastroenterol. 2020; 20: 2. Published online 2019 Dec 31. doi: 10.1186/s12876-019-1143-5).
The study deals with a retrospective analysis of the effectiveness of Kolofort, “a release-active drug” produced by Materia Medica Holding. The only statement regarding the composition of the drug reads as follows: “For the treatment of FGID [functional gastrointestinal disorders], the combination of released-active form of antibodies [RAF of Abs] to S-100 protein, TNF-α and histamine (RAF of Abs to S 100, Abs to TNF-α and Abs to H), a pathogenetically targeted drug Kolofort, was developed by the Research and Production Company Materia Medica Holding (LLC NPF” MATERIA MEDICA HOLDING”) Moscow, Russia and introduced into practical medicine. The RAF of Abs in the drug provides an anti-inflammatory, spasmolytic, and anxiolytic effect ” (notations in square brackets by me). The two following paragraphs provide information (and citations of two publications in Russian) related to the clinical trials of Kolofort. At no point in the publication are the concentrations of the active components of Kolofort mentioned! Only a web search provides further information about the composition of Kolofort (see screenshot). The three active ingredients, RAF of Abs to S-100 protein, TNF-α, and histamine, are only present at concentrations of C12, C30, and C200, respectively, i. e. they are absent. Perhaps a better notation for the remedy should be RAF in Abs of histamine, meaning release-active form in absence of histamine.
Judging from the composition of Kolofort no physiological or therapeutical reaction is to be expected. Still the authors claim that “The COMFORT program has demonstrated the positive effect of treatment [with Kolofort] in the majority of patients with IBS and FD and their combination in real clinical practice”. The authors arrived at these results by analyzing a questionnaire that had been specially developed for the assessment of gastrointestinal disorders. The questionnaire is called “7*7” [seven symptoms in seven days], but not further discussed or explained in the publication. Although there exists at least one publication from 2016 where the questionnaire was used to assess symptoms of gastrointestinal ailments (Ivashkin et al. RZHGGK. 2016;3(S):24-33. https://doi.org/10.22416/1382-4376-2016-26-3-24-33) the actual validation was not published until November 2018 (online, print June 2019) which is after the Kolofort study had already terminated (November 01, 2017, through March 30, 2018). Please note that the validation was done by one of the co-authors (V. Ivashkin) of the Kolofort study. There is certainly a good explanation for post-validating a tool used in earlier studies, but I just can’t think of one right now.
There exist several more (if not dozens) of publications by this group of authors that have already been investigated. It appears that the Materia Medica Holding director Oleg I. Epstein is heavily involved in a competition of who is capable of producing the highest number of retracted publications. Here are a few of them:
Retraction: Novel Approach to Activity Evaluation for Release-Active Forms of Anti-Interferon-Gamma Antibodies Based on Enzyme-Linked Immunoassay
The PLOS ONE Editors. Published: May 3, 2018
https://doi.org/10.1371/journal.pone.0197086
Retraction notice to “Efficacy of novel antibody-based drugs against rhinovirus infection: In vitro and in vivo results” [Antiviral Research 142 (2017) 185–192]
https://doi.org/10.1016/j.antiviral.2019.02.010
Retraction notice to “Activity of ultra-low doses of antibodies to gamma-interferon against lethal influenza A(H1N1)2009 virus infection in mice” [Antiviral Research 93 (2012) 219–224]
https://doi.org/10.1016/j.antiviral.2019.02.011
Retraction Note: Release-Active Dilutions of Diclofenac Enhance Anti-inflammatory Effect of Diclofenac in Carrageenan-Induced Rat Paw Edema Model
https://doi.org/10.1007/s10753-013-9705-0
Retraction: Activity of ergoferon against lethal influenza A (H3N2) virus infection in mice
https://www.intmedpress.com/journals/avt/article.cfm?id=3325&pid=48&sType=AVT
Retraction Note: Effects of chronic treatment with the eNOS stimulator Impaza on penis length and sexual behaviors in rats with a high baseline of sexual activity
https://www.nature.com/articles/s41443-020-0321-x
There are probably more retractions out there, but to make it onto the current Retraction Watch Leader Board (https://retractionwatch.com/the-retraction-watch-leaderboard/) a minimum of 25 retractions is required to take over rank 30. You have to work harder Dr. O. I. Epstein!
Last but not least there is an interview with Epstein available online (https://pharmaboardroom.com/interviews/interview-with-oleg-epstein-general-director-materia-medica/) where he claimed that „We proved that we [Materia Medica] are not a homeopathy company, and 1.5 years ago, the Ministry of Public Health decreed that our drugs will no longer be classified as homeopathic.“ Wow! How?
So, what does all this tell us? There exists a pool of authors, somehow connected to Materia Medica Holding, who manage to get articles, that are nothing else but homeopathy in disguise, past the peer review of reputable academic journals. It would be easy to blame the reviewers for their not soo stringent approach. But as the Kolofort paper shows, only in-depth research may actually reveal the truth. Let’s not forget, even the retracted papers made it through to publication and only a later review scrutinized their scientific merit.
It can be assumed that Materia Medica will not stop promoting their remedies through the publication of further studies. There are already publications out there that do not include any company staff as co-authors but were sponsored by the company. Judging from the rate of already retracted paper, reputation does not appear to matter. These authors possibly work along a submission-rejection-resubmission to a different journal approach until a paper gets published.
So far the homeopathy community hasn’t taken much notice of any of the beforementioned studies, most probably for two reasons: nowhere does the term “homeopathy” appear nor were the papers published in SCAM journals but rather in academic journals above the radar of homeopaths. But it can be assumed that in future, if it fits their purpose, such studies will feature among their usual dubious double blindfolded placebo trials.
Keep your eyes open for more of this stuff and please get in touch with the editorial team of the journal concerned if you discover yet another “UHD” or “RAF” publication!
This systematic review assessed the effect of spinal manipulative therapy (SMT), the hallmark therapy of chiropractors, on pain and function for chronic low back pain (LBP) using individual participant data (IPD) meta-analyses.
Of the 42 RCTs fulfilling the inclusion criteria, the authors obtained IPD from 21 (n=4223). Most trials (s=12, n=2249) compared SMT to recommended interventions. The analyses showed moderate-quality evidence that SMT vs recommended interventions resulted in similar outcomes on
- pain (MD -3.0, 95%CI: -6.9 to 0.9, 10 trials, 1922 participants)
- and functional status at one month (SMD: -0.2, 95% CI -0.4 to 0.0, 10 trials, 1939 participants).
Effects at other follow-up measurements were similar. Results for other comparisons (SMT vs non-recommended interventions; SMT as adjuvant therapy; mobilization vs manipulation) showed similar findings. SMT vs sham SMT analysis was not performed, because data from only one study were available. Sensitivity analyses confirmed these findings.
The authors concluded that sufficient evidence suggest that SMT provides similar outcomes to recommended interventions, for pain relief and improvement of functional status. SMT would appear to be a good option for the treatment of chronic LBP.
In 2019, this team of authors published a conventional meta-analysis of almost the same data. At this stage, they concluded as follows: SMT produces similar effects to recommended therapies for chronic low back pain, whereas SMT seems to be better than non-recommended interventions for improvement in function in the short term. Clinicians should inform their patients of the potential risks of adverse events associated with SMT.
Why was the warning about risks dropped in the new paper?
I have no idea.
But the risks are crucial here. If we are told that SMT is as good or as bad as recommended therapies, such as exercise, responsible clinicians need to decide which treatment they should recommend to their patients. If effectiveness is equal, other criteria come into play:
- cost,
- risk,
- availability.
Can any reasonable person seriously assume that SMT would do better than exercise when accounting for costs and risks?
I very much doubt it!
Guest post by Norbert Aust and Viktor Weisshäupl
Imagine you recently published an excellent and rigorous trial providing solid evidence that a certain therapy is able to help patients suffering from some inevitably fatal condition. You proved that your therapy is able to significantly prolong the patients’ lifetime, much longer than with the current state-of-the-art therapeutic approach. But the patients not only live considerably longer, but they also do so with a much better quality of life (QoL) and subjective well-being. In short: this therapy marks some progress that would otherwise take years or decades of scientific effort.
And then someone comes forward and points out your data apparently were manipulated. Essential parameters of this trial were modified sometime after data collection was completed, with the patients’ outcome and first analyses available. Thus the results were biased in a certain direction and the critics show that the results as published in your study show characteristics that such manipulations would evoke. After all, this holds an implication of scientific misconduct that could, if verified, ruin your academic reputation more or less completely.
What would you do?
Ignore the preposterous concerns because you know your methods and performance were rigorous and solid? After all, anytime some real academic criticism arises you are ready to prove your findings are well-founded results of accepted scientific methods. Or would you publish data or documents that your critics were too ignorant to find or to understand, and thus to stop such rumours once and for all? Maybe you could even clarify some of the issues raised by those critics, maybe add some follow-up information or data to ensure no more misunderstandings occur. Or would you try to find some clues for a libel lawsuit?
Well, we thought some of the above would happen after we contacted the authors of the recent study on adjunct homeopathy in non-small cell lung cancer. On that date, we forwarded our detailed analysis to the lead author and all the co-authors.
Of course, we even considered the possibility, not very likely though, that we would receive some explanation for the numerous exclusion criteria while other serious conditions that coincide with advanced age did not preclude enrollment. Or an updated CONSORT diagram accounting for the patients excluded. Or some explanation just why the numerous amendments to the protocol were necessary but not important enough to mention them in the published paper.
But nothing of this happened as yet (July 2021). Instead on June 14 and 16, 2021, not two weeks after our messages to the authors, the registration data at ClinicalTrials were updated once again and a new version of the protocol was uploaded [3]. And this update looks pretty much like it is meant to cover up and blur the former data that we based our analysis on. Of course, these data and the former version of the protocol are available still – just one layer further down, and you have to scroll to the bottom of the page to find the small link “history of changes”. Maybe not many visitors will do that.
In contrast to the versions before, now the uploaded data are in line with the study as published, namely, they include a full list of the exclusion criteria and the reduced observation time for QoL, which was the primary outcome. Note: throughout the trial until the end of data assessment those parameters were set with pregnancy as the only exclusion criterion and two years follow up time, only to be amended in the protocol uploaded two months after data collection was complete and analysis presumably was well underway.
In addition, there is a new version of the study protocol, this one dated Feb. 6, 2014. Of course, this protocol is fairly new, in spite of the date it carries. Why would the older version allegedly from January 2011 be uploaded to the register in September 2019, if this more actual version already had existed and was available?
Contrary to the prior version all the clues are removed that would indicate that this document was finished at a much later point in time than given in its date: References to some future software versions that were released years after the protocol was allegedly compiled are dropped. And this strange literature reference “25” that corresponds to the reference list in the final study as published but is pointless in the protocol without any reference list, is removed too. And of course, again contrary to the prior version, the exclusion criteria are identical with the final study as is the shortened follow-up time for QoL.
New to the protocol is a section “Bringing in the patient’s voice”, where the authors disclose how they want to “systematically research the ethical, legal, socio-political, and science theoretical dimensions of homeopathy as in the case of lung cancer (non-small-cell lung carcinoma) exemplified” in some “integral social scientific study”, where some “focus groups” of 4 to 10 participants together with their relatives, friends and caregivers included should be used to study “interactions between individuals, collectively shared and uncontested assumptions, and the emergence of collective meaning”.
But from all of this more or less meaningless but very sciency sounding socio-speak, not a single word found its way into the study. Nothing. So it is pointless to try to figure out what the content of this part of the investigation is all about.
Why then was this chapter added? This “integral social scientific study” was to start after the “third or fourth homeopathic treatment” (But why should patients not be included in this “research” from the very first beginning?). Is it perhaps to give some rationale why the follow-up time for QoL was to end after the third homeopathic treatment?
So what we see, when we look up the study at ClinicalTrials now, is a perfectly matching set of data and a protocol that corresponds to the study as published and looks as if it was published at a time where the trial was underway and the patients were still blinded. If you do not look very closely everything now appears to be perfect.
And here we would like to forward some critique to the register: The purpose of the study register is to prevent not only publication bias but misleading manipulation from happening as well. They do quite a good job in preserving former versions of data and documents and keeping them available to the public. Many national study registers do not offer this service. But you must be of a suspicious mind and of some persistence to actively search and find and check the history of modifications. Thus, a cover-up like the one we are witnessing here might well prove successful. We, therefore, propose to improve the presentation of the registration: If vital amendments occurred that may affect the outcomes – such as protocol changes, extensions of exclusion criteria, modifications of follow-up time – this should be indicated upfront in the study’s record instead of some small hint to “history of changes” at the very bottom of the page.
In conclusion, there appears to be no proof that the results of the study were produced using rigorous scientific methods. And the issues we raised in our report to the authors remain unresolved.
The objective of this systematic review was to assess the effects and reliability of sham procedures in manual therapy (MT) trials in the treatment of back pain (BP) in order to provide methodological guidance for clinical trial development. Different databases were screened up to 20 August 2020. Randomised clinical trials involving adults affected by BP (cervical and lumbar), acute or chronic, were included. Hand contact sham treatment (ST) was compared with different MT (physiotherapy, chiropractic, osteopathy, massage, kinesiology, and reflexology) and to no treatment. Primary outcomes were BP improvement, the success of blinding, and adverse effect (AE). Secondary outcomes were the number of drop-outs. Dichotomous outcomes were analysed using risk ratio (RR), continuous using mean difference (MD), 95% CIs. The minimal clinically important difference was 30 mm changes in pain score.
A total of 24 trials were included involving 2019 participants. Different manual treatments were provided:
- SM/chiropractic (7 studies, 567 participants).
- Osteopathy (5 trials, 645 participants).
- Kinesiology (1 trial, 58 participants).
- Articular mobilisations (6 trials, 445 participants).
- Muscular release (5 trials, 304 participants).
Very low evidence quality suggests clinically insignificant pain improvement in favour of MT compared with ST (MD 3.86, 95% CI 3.29 to 4.43) and no differences between ST and no treatment (MD -5.84, 95% CI -20.46 to 8.78).ST reliability shows a high percentage of correct detection by participants (ranged from 46.7% to 83.5%), spinal manipulation being the most recognised technique. Low quality of evidence suggests that AE and drop-out rates were similar between ST and MT (RR AE=0.84, 95% CI 0.55 to 1.28, RR drop-outs=0.98, 95% CI 0.77 to 1.25). A similar drop-out rate was reported for no treatment (RR=0.82, 95% 0.43 to 1.55).

Forest plot of comparison ST versus MT in back pain outcome at short term. MT, manual therapy; ST, sham treatment.
The authors concluded that MT does not seem to have clinically relevant effect compared with ST. Similar effects were found with no treatment. The heterogeneousness of sham MT studies and the very low quality of evidence render uncertain these review findings. Future trials should develop reliable kinds of ST, similar to active treatment, to ensure participant blinding and to guarantee a proper sample size for the reliable detection of clinically meaningful treatment effects.
Essentially these findings suggest that the effects patients experience after MT are not due to MT per see but to placebo effects. The review could be criticised because of the somewhat odd mix of MTs lumped together in one analysis. Yet, I think it is fair to point out that most of the studies were of chiropractic and osteopathy. Thus, this review implies that chiropractic and osteopathy are essentially placebo treatments.
The authors of the review also provide this further comment:
Similar findings were found in other reviews conducted on LBP. Ruddock et al included studies where SM was compared with what authors called ‘an effective ST’, namely a credible sham manipulation that physically mimics the SM. Pooled data from four trials showed a very small and not clinically meaningful effect in favour of MT.52
Rubinstein et al 53 compared SM and mobilisation techniques to recommended, non-recommended therapies and to ST. Their findings showed that 5/47 studies included attempted to blind patients to the assigned intervention by providing an ST. Of these five trials, two were judged at unclear risk of participants blinding. The authors also questioned the need for additional studies on this argument, as during the update of their review they found recent small pragmatic studies with high risk of bias. We agree with Rubinstein et al that recent studies included in this review did not show a higher quality of evidence. The development of RCT with similar characteristic will probably not add any proof of evidence on MT and ST effectiveness.53
If we agree that chiropractic and osteopathy are placebo therapies, we might ask whether they should have a place in the management of BP. Considering the considerable risks associated with them, I feel that the answer is obvious and simple:
NO!
Multiple sclerosis (MS) causes a range of different symptoms. Patients with MS have looked for alternative therapies to control their MS progress and treat their symptoms. Non-invasive therapeutic approaches such as massage can have benefits to mitigate some of these symptoms. However, there is no rigorous review of massage effectiveness for patients suffering from MS.
The present systematic review was aimed at examining the effectiveness of different massage approaches on common MS symptoms, including fatigue, pain, anxiety, depression, and spasticity.
A total of 12 studies met the inclusion criteria. The authors rated 5 studies as being of fair and 7 studies of good methodological quality. Fatigue was improved by different massage styles, such as reflexology, nonspecific therapeutic massage, and Swedish massage. Pain, anxiety, and depression were effectively improved by reflexology techniques. Spasticity was reduced by Swedish massage and reflexology techniques.
The authors concluded that different massage approaches effectively improved MS symptoms such as fatigue, pain, anxiety, depression, and spasticity.
Clinical trials of massage therapy face formidable obstacles including:
- difficulties in obtaining funding,
- difficulties in finding expert researchers who are interested in the subject,
- difficulties to control for placebo effects,
- difficulties in blinding patients,
- impossibility of blinding therapists,
- confusion about the plethora of different massage techniques.
Thus, the evidence is often less convincing than one would hope. This, however, does not mean that massage therapy does not have considerable potential for a range of indications. One could easily argue that this situation is similar to spinal manipulation. Yet, there are at least three important differences:
- massage therapy is not as heavily burdened with frequent adverse effects and potentially life-threatening complications,
- massage therapy has a rational basis,
- the existing evidence is more uniformly encouraging.
Consequently, massage therapy (particularly, classic or Swedish massage) is more readily being accepted even in the absence of solid evidence. In fact, in some countries, e.g. Germany and Austria, massage therapy is considered to be a conventional treatment.
This multicenter, randomized, sham-controlled trial was aimed at assessing the long-term efficacy of acupuncture for chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS). Men with moderate to severe CP/CPPS were recruited, regardless of prior exposure to acupuncture. They received sessions of acupuncture or sham acupuncture over 8 weeks, with a 24-week follow-up after treatment. Real acupuncture treatment was used to create the typical de qi sensation, whereas the sham acupuncture treatment (the authors state they used the Streitberger needle, but the drawing looks more as though they used our device) does not generate this feeling.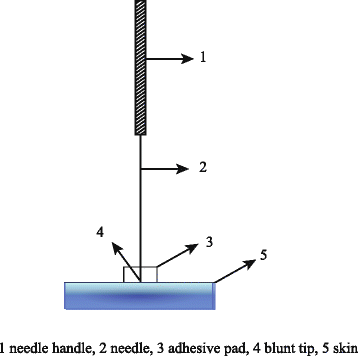
The primary outcome was the proportion of responders, defined as participants who achieved a clinically important reduction of at least 6 points from baseline on the National Institutes of Health Chronic Prostatitis Symptom Index at weeks 8 and 32. Ascertainment of sustained efficacy required the between-group difference to be statistically significant at both time points.
A total of 440 men (220 in each group) were recruited. At week 8, the proportions of responders were:
- 60.6% (95% CI, 53.7% to 67.1%) in the acupuncture group
- 36.8% (CI, 30.4% to 43.7%) in the sham acupuncture group (adjusted difference, 21.6 percentage points [CI, 12.8 to 30.4 percentage points]; adjusted odds ratio, 2.6 [CI, 1.8 to 4.0]; P < 0.001).
At week 32, the proportions were:
- 61.5% (CI, 54.5% to 68.1%) in the acupuncture group
- 38.3% (CI, 31.7% to 45.4%) in the sham acupuncture group (adjusted difference, 21.1 percentage points [CI, 12.2 to 30.1 percentage points]; adjusted odds ratio, 2.6 [CI, 1.7 to 3.9]; P < 0.001).
Twenty (9.1%) and 14 (6.4%) adverse events were reported in the acupuncture and sham acupuncture groups, respectively. No serious adverse events were reported. No significant difference was found in changes in the International Index of Erectile Function 5 score at all assessment time points or in peak and average urinary flow rates at week 8.
The authors concluded that, compared with sham therapy, 20 sessions of acupuncture over 8 weeks resulted in greater improvement in symptoms of moderate to severe CP/CPPS, with durable effects 24 weeks after treatment.
The study was sponsored by the China Academy of Chinese Medical Sciences and the National Administration of Traditional Chinese Medicine. The trialists originate from the following institutions:
- 1Guang’anmen Hospital, China Academy of Chinese Medical Sciences, Beijing, China (Y.S., B.L., Z.Q., J.Z., J.W., X.L., W.W., R.P., H.C., X.W., Z.L.).
- 2Key Laboratory of Chinese Internal Medicine of Ministry of Education, Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, China (Y.L.).
- 3ThedaCare Regional Medical Center – Appleton, Appleton, Wisconsin (K.Z.).
- 4Hengyang Hospital Affiliated to Hunan University of Chinese Medicine, Hengyang, China (Z.Y.).
- 5The First Hospital of Hunan University of Chinese Medicine, Changsha, China (W.Z.).
- 6Guangdong Provincial Hospital of Traditional Chinese Medicine, Guangzhou, China (W.F.).
- 7The First Affiliated Hospital of Anhui University of Chinese Medicine, Hefei, China (J.Y.).
- 8West China Hospital of Sichuan University, Chengdu, China (N.L.).
- 9China Academy of Chinese Medical Sciences, Beijing, China (L.H.).
- 10Yantai Hospital of Traditional Chinese Medicine, Yantai, China (Z.Z.).
- 11Shaanxi Provincial Hospital of Traditional Chinese Medicine, Xi’an, China (T.S.).
- 12The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, China (J.F.).
- 13Beijing Fengtai Hospital of Integrated Traditional and Western Medicine, Beijing, China (Y.D.).
- 14Xi’an TCM Brain Disease Hospital, Xi’an, China (H.S.).
- 15Dongfang Hospital Beijing University of Chinese Medicine, Beijing, China (H.H.).
- 16Luohu District Hospital of Traditional Chinese Medicine, Shenzhen, China (H.Z.).
- 17Guizhou University of Traditional Chinese Medicine, Guiyang, China (Q.M.).
These facts, together with the previously discussed notion that clinical trials from China are notoriously unreliable, do not inspire confidence. Moreover, one might well wonder about the authors’ claim that patients were blinded. As pointed out above, the real and sham acupuncture were fundamentally different: the former did generate de qi, while the latter did not! A slightly pedantic point is my suspicion that the trial did not test the efficacy but the effectiveness of acupuncture, if I am not mistaken. Finally, one might wonder what the rationale of acupuncture as a treatment of CP/CPPS might be. As far as I can see, there is no plausible mechanism (other than placebo) to explain the effects.
So, is the evidence that emerged from the new study convincing?
No, in my view, it is not!
In fact, I am surprised that a journal as reputable as the Annals of Internal Medicine published it.
A case report was published of a 35-year-old Chinese man with no risk factors for stroke. He presented with a 2-day history of expressive dysphasia and a 1-day history of right-sided weakness. The symptoms were preceded by multiple sessions of the neck, shoulder girdle, and upper back massage for pain relief in the prior 2 weeks. A CT-scan of the brain demonstrated an acute left middle cerebral artery infarct and left internal carotid artery dissection. The MRI cerebral angiogram confirmed left carotid arterial dissection and intimal oedema of bilateral vertebral arteries. In the absence of other vascular comorbidities and risk factors, massage-induced internal carotid arterial dissection was deemed to be the most likely cause of the near-fatal cerebrovascular event.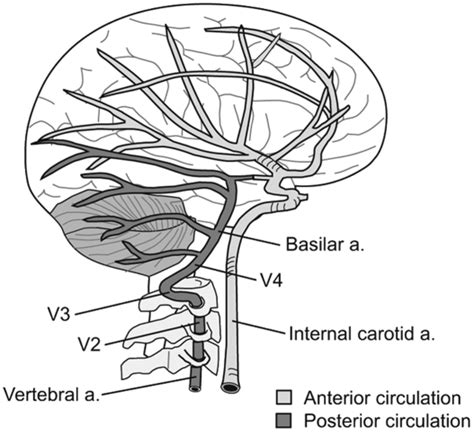
INSIDER reported further details of the case: the patient told the doctors who treated him that he had seen the chiropractor for two weeks before he experienced trouble reading, writing and talking. After experiencing those symptoms for two days and one day of pain on his right side, a friend convinced the patient to consult a neurologist. This led to the hospital admission, the above-named tests, and diagnosis. After three months of therapy and rehab, the patient showed “significant improvement,” according to the doctors.
What remains unclear is the exact nature of the neck treatment that is believed to have caused the arterial dissection. A massage is mentioned but massages have rarely been associated with such problems. Neck manipulations, on the other hand, are the hallmark therapy of chiropractors and have, as I have pointed out regularly, often been reported to cause arterial dissections.
Chiropractors usually deny this fact; alternatively, they claim that only poorly trained practitioners cause these adverse events or that their frequency is exceedingly small. However, without a proper post-marketing surveillance system, this argument is hardly convincing.