
Updated Edition!
 for Cancer")





")









![]()

Well-conducted systematic reviews (SRs) should in principle provide the most reliable evidence on the effectiveness of acupuncture. However, limitations on the methodological rigour of SRs may impact the trustworthiness of their conclusions. This cross-sectional study was aimed at evaluating the methodological quality of recent SRs of acupuncture.
The Cochrane Database of Systematic Reviews, MEDLINE, and EMBASE were searched for SRs focusing on manual acupuncture or electro-acupuncture published during January 2018 and March 2020. Eligible SRs needed to contain at least one meta-analysis and be published in the English language. Two independent reviewers extracted the bibliographical characteristics of the included SRs with a pre-designed questionnaire and appraised the methodological quality of the reviews with the validated AMSTAR 2 (A MeaSurement Tool to Assess systematic Reviews 2). The associations between bibliographical characteristics and methodological quality ratings were explored using Kruskal-Wallis rank tests and Spearman’s rank correlation coefficients.
A total of 106 SRs were appraised. The results were as follows:
- one (0.9%) SR was of high methodological quality,
- no review (0%) was of moderate quality,
- six (5.7%) were of low quality,
- 99 (93.4%) were of critically low quality.
Only ten (9.4%) provided an a priori protocol, only four (3.8%) conducted a comprehensive literature search, only five (4.7%) provided a list of excluded studies, and only six (5.7%) performed a meta-analysis appropriately. Cochrane SRs, updated SRs, and SRs that did not search non-English databases had relatively higher overall quality. The vast majority (87.7%) of the 106 reviews included in this analysis originated from Asia. Conflicts of interest of the review authors were declared in only 2 of the 106 reviews.
The authors concluded that the methodological quality of SRs on acupuncture is unsatisfactory. Future reviewers should improve critical methodological aspects of publishing protocols, performing comprehensive search, providing a list of excluded studies with justifications for exclusion, and conducting appropriate meta-analyses. These recommendations can be implemented via enhancing the technical competency of reviewers in SR methodology through established education approaches as well as quality gatekeeping by journal editors and reviewers. Finally, for evidence users, skills in SR critical appraisal remain to be essential as relevant evidence may not be available in pre-appraised formats.
On this blog, I have often complained about the lack of critical input and the poor quality of systematic reviews of so-called alternative medicine (SCAM), particularly of acupuncture, and especially of Chinese reviews, and even more especially Chinese reviews of (mostly) Chinese studies. This new paper is a valuable confirmation of this fast-growing deficit.
One does not need to be a prophet to predict that this pollution of the literature with complete rubbish will have detrimental effects. Because poor reviews almost always draw an over-optimistic picture of the value of acupuncture, this phenomenon must seriously mislead the public. The end result will be that the public believes acupuncture to be effective.
I cannot help thinking that this is, in fact, the intended aim of the authors of such poor, false-positive reviews. Moreover, a glance at the subject areas of the reviews in the list below gives the impression that China is heavily promoting the idea that acupuncture is a panacea. Yet there is good evidence to show that acupuncture is little more than placebo therapy.
In my last post, I have reported that I am an author of many of the frequently-cited systematic acupuncture reviews. You might thus assume that I am a significant part of this pollution by rubbish reviews. This would, however, be an entirely wrong conclusion. The above analysis covers a period when my unit had already been closed, and I am thus not responsible for a single of the papers included in the above analysis.
List of included systematic reviews
| ID | Included systematic reviews |
| 1 | Acupuncture for primary insomnia: An updated systematic review of randomized controlled trials |
| 2 | Efficacy and safety of acupuncture for essential hypertension: A meta-analysis |
| 3 | Acupuncture for the treatment of sudden sensorineural hearing loss: A systematic review and meta-analysis: Acupuncture for SSNHL |
| 4 | Effectiveness of Acupuncturing at the Sphenopalatine Ganglion Acupoint Alone for Treatment of Allergic Rhinitis: A Systematic Review and Meta-Analysis |
| 5 | Acupuncture and clomiphene citrate for anovulatory infertility: a systematic review and meta-analysis |
| 6 | Acupuncture for primary trigeminal neuralgia: A systematic review and PRISMA-compliant meta-analysis |
| 7 | Acupuncture as an adjunctive treatment for angina due to coronary artery disease: A meta-analysis |
| 8 | Conventional treatments plus acupuncture for asthma in adults and adolescent: A systematic review and meta-analysis |
| 9 | Optimizing acupuncture treatment for dry eye syndrome: A systematic review |
| 10 | Acupuncture using pattern-identification for the treatment of insomnia disorder: a systematic review and meta-analysis of randomized controlled trials |
| 11 | Efficacy and Safety of Auricular Acupuncture for Cognitive Impairment and Dementia: A Systematic Review |
| 12 | Acupuncture for cognitive impairment in vascular dementia, alzheimer’s disease and mild cognitive impairment: A systematic review and meta-analysis |
| 13 | Effectiveness of pharmacopuncture for cervical spondylosis: A systematic review and meta-analysis |
| 14 | Acupuncture combined with swallowing training for poststroke dysphagia: a meta-analysis of randomised controlled trials |
| 15 | Scalp acupuncture treatment for children’s autism spectrum disorders: A systematic review and meta-analysis |
| 16 | Acupuncture for Post-stroke Shoulder-Hand Syndrome: A systematic review and meta-analysis |
| 17 | Systematic review of acupuncture for the treatment of alcohol withdrawal syndrome |
| 18 | Acupuncture for hip osteoarthritis |
| 19 | Clinical Benefits of Acupuncture for the Reduction of Hormone Therapy-Related Side Effects in Breast Cancer Patients: A Systematic Review |
| 20 | Combination therapy of scalp electro-acupuncture and medication for the treatment of Parkinson’s disease: A systematic review and meta-analysis |
| 21 | Acupuncture for migraine: A systematic review and meta-analysis |
| 22 | Acupuncture to Promote Recovery of Disorder of Consciousness after Traumatic Brain Injury: A Systematic Review and Meta-Analysis |
| 23 | Acupuncture Compared with Intramuscular Injection of Neostigmine for Postpartum Urinary Retention: A Systematic Review and Meta-Analysis of Randomized Controlled Trials |
| 24 | Acupuncture for the relief of hot flashes in breast cancer patients: A systematic review and meta-analysis of randomized controlled trials and observational studies |
| 25 | Effectiveness and Safety of Acupuncture for Perimenopausal Depression: A Systematic Review and Meta-Analysis of Randomized Controlled Trials |
| 26 | Acupuncture plus Chinese Herbal Medicine for Irritable Bowel Syndrome with Diarrhea: A Systematic Review and Meta-Analysis |
| 27 | Electroacupuncture as an adjunctive therapy for motor dysfunction in acute stroke survivors: A systematic review and meta-analyses |
| 28 | Acupuncture for Acute Pancreatitis: A Systematic Review and Meta-analysis |
| 29 | Acupuncture for chronic fatigue syndrome: a systematic review and meta-analysis |
| 30 | Compare the efficacy of acupuncture with drugs in the treatment of Bell’s palsy: A systematic review and meta-analysis of RCTs |
| 31 | The effectiveness and safety of acupuncture for the treatment of myasthenia gravis: a systematic review and meta-analysis of randomized controlled trials |
| 32 | Acupuncture therapy for fibromyalgia: A systematic review and meta-analysis of randomized controlled trials |
| 33 | The effectiveness of acupuncture therapy in patients with post-stroke depression: An updated meta-analysis of randomized controlled trials |
| 34 | Fire needling for herpes zoster: A systematic review and meta-analysis of randomized clinical trials |
| 35 | Comparison between the Effects of Acupuncture Relative to Other Controls on Irritable Bowel Syndrome: A Meta-Analysis |
| 36 | Manual Acupuncture for Optic Atrophy: A Systematic Review and Meta-Analysis |
| 37 | Effect of warm needling therapy and acupuncture in the treatment of peripheral facial paralysis: A systematic review and meta-analysis |
| 38 | The Effect of Acupuncture in Breast Cancer-Related Lymphoedema (BCRL): A Systematic Review and Meta-Analysis |
| 39 | The Efficacy of Acupuncture in Chemotherapy-Induced Peripheral Neuropathy: Systematic Review and Meta-Analysis |
| 40 | The maintenance effect of acupuncture on breast cancer-related menopause symptoms: a systematic review |
| 41 | The effectiveness of acupuncture in the management of persistent regional myofascial head and neck pain: A systematic review and meta-analysis |
| 42 | Acupuncture for the Treatment of Adults with Posttraumatic Stress Disorder: A Systematic Review and Meta-Analysis |
| 43 | The effectiveness of superficial versus deep dry needling or acupuncture for reducing pain and disability in individuals with spine-related painful conditions: a systematic review with meta-analysis |
| 44 | Effects of dry needling trigger point therapy in the shoulder region on patients with upper extremity pain and dysfunction: a systematic review with meta-analysis |
| 45 | Is dry needling effective for low back pain?: A systematic review and PRISMA-compliant meta-analysis |
| 46 | The effectiveness and safety of acupuncture for patients with atopic eczema: a systematic review and meta-analysis |
| 47 | Comparing verum and sham acupuncture in fibromyalgia syndrome: a systematic review and meta-analysis |
| 48 | Acupuncture for symptomatic gastroparesis |
| 49 | The Efficacy and Safety of Acupuncture for the Treatment of Children with Autism Spectrum Disorder: A Systematic Review and Meta-Analysis |
| 50 | Acupuncture Versus Sham-acupuncture: A Meta-analysis on Evidence for Non-immediate Effects of Acupuncture in Musculoskeletal Disorders |
| 51 | Acupuncture Treatment for Post-Stroke Dysphagia: An Update Meta-Analysis of Randomized Controlled Trials |
| 52 | Effectiveness of Acupuncture Used for the Management of Postpartum Depression: A Systematic Review and Meta-Analysis |
| 53 | Clinical effects and safety of electroacupuncture for the treatment of post-stroke depression: a systematic review and meta-analysis of randomised controlled trials |
| 54 | Placebo effect of acupuncture on insomnia: a systematic review and meta-analysis |
| 55 | Acupuncture for Chronic Pain-Related Insomnia: A Systematic Review and Meta-Analysis |
| 56 | Evidence for Dry Needling in the Management of Myofascial Trigger Points Associated With Low Back Pain: A Systematic Review and Meta-Analysis |
| 57 | Warm needle acupuncture in primary osteoporosis management: a systematic review and meta-analysis |
| 58 | Acupuncture for overactive bladder in adults: a systematic review and meta-analysis |
| 59 | Traditional acupuncture for menopausal hot flashes: A systematic review and meta-analysis of randomized controlled trials |
| 60 | The effectiveness of acupuncture for osteoporosis: A systematic review and meta-analysis |
| 61 | Long-term effects of acupuncture for chronic prostatitis/chronic pelvic pain syndrome: Systematic review and single-Arm meta-Analyses |
| 62 | Does acupuncture the day of embryo transfer affect the clinical pregnancy rate? Systematic review and meta-analysis |
| 63 | Acupuncture treatments for infantile colic: a systematic review and individual patient data meta-analysis of blinding test validated randomised controlled trials |
| 64 | Acupuncture performed around the time of embryo transfer: a systematic review and meta-analysis |
| 65 | Is Acupuncture Effective for Improving Insulin Resistance? A Systematic Review and Meta-analysis |
| 66 | Efficacy of acupuncture in the management of post-apoplectic aphasia: A systematic review and meta-analysis of randomized controlled trials |
| 67 | Acupuncture for lumbar disc herniation: a systematic review and meta-analysis |
| 68 | Traditional Chinese acupuncture and postpartum depression: A systematic review and meta-analysis |
| 69 | Acupuncture for Chronic Pain: Update of an Individual Patient Data Meta-Analysis |
| 70 | Acupuncture Therapy for Functional Effects and Quality of Life in COPD Patients: A Systematic Review and Meta-Analysis |
| 71 | Electroacupuncture for Reflex Sympathetic Dystrophy after Stroke: A Meta-Analysis |
| 72 | The Effect of Patient Characteristics on Acupuncture Treatment Outcomes |
| 73 | The efficacy and safety of acupuncture in women with primary dysmenorrhea: A systematic review and meta-analysis |
| 74 | Role of acupuncture in the treatment of insulin resistance: A systematic review and meta-analysis |
| 75 | Appropriateness of sham or placebo acupuncture for randomized controlled trials of acupuncture for nonspecific low back pain: A systematic review and meta-analysis |
| 76 | Evidence of efficacy of acupuncture in the management of low back pain: a systematic review and meta-analysis of randomised placebo- or sham-controlled trials |
| 77 | The effects of acupuncture on pregnancy outcomes of in vitro fertilization: A systematic review and meta-analysis |
| 78 | Acupuncture for migraine without aura: a systematic review and meta-analysis |
| 79 | Acupuncture for acute stroke |
| 80 | Acupuncture at Tiaokou (ST38) for Shoulder Adhesive Capsulitis: What Strengths Does It Have? A Systematic Review and Meta-Analysis of Randomized Controlled Trials |
| 81 | Acupuncture for hypertension |
| 82 | The effect of acupuncture on Bell’s palsy: An overall and cumulative meta-analysis of randomized controlled trials |
| 83 | Effects of acupuncture on cancer-related fatigue: a meta-analysis |
| 84 | Acupuncture for adults with overactive bladder |
| 85 | Electroacupuncture for Postoperative Urinary Retention: A Systematic Review and Meta-Analysis |
| 86 | Meta-Analysis of Electroacupuncture in Cardiac Anesthesia and Intensive Care |
| 87 | Acupuncture therapy improves health-related quality of life in patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis |
| 88 | The effect of acupuncture on the quality of life in patients with migraine: A systematic review and meta-analysis |
| 89 | Cognitive improvement effects of electro-acupuncture for the treatment of MCI compared with Western medications: A systematic review and Meta-analysis 11 Medical and Health Sciences 1103 Clinical Sciences |
| 90 | Oriental herbal medicine and moxibustion for polycystic ovary syndrome: A meta-analysis |
| 91 | The Effect of Acupuncture and Moxibustion on Heart Function in Heart Failure Patients: A Systematic Review and Meta-Analysis |
| 92 | Acupuncture therapy for the treatment of stable angina pectoris: An updated meta-analysis of randomized controlled trials |
| 93 | Traditional manual acupuncture combined with rehabilitation therapy for shoulder hand syndrome after stroke within the Chinese healthcare system: a systematic review and meta-analysis |
| 94 | Effects of moxibustion on pain behaviors in patients with rheumatoid arthritis: A meta-analysis |
| 95 | Acupuncture Treatment for Chronic Pelvic Pain in Women: A Systematic Review and Meta-Analysis of Randomized Controlled Trials |
| 96 | The effectiveness of dry needling for patients with orofacial pain associated with temporomandibular dysfunction: a systematic review and meta-analysis |
| 97 | Acupuncture for postherpetic neuralgia systematic review and meta-analysis |
| 98 | Acupoint selection for the treatment of dry eye: A systematic review and meta-analysis of randomized controlled trials |
| 99 | Warm-needle moxibustion for spasticity after stroke: A systematic review of randomized controlled trials |
| 100 | Acupuncture for menstrual migraine: a systematic review |
| 101 | The efficacy of acupuncture for stable angina pectoris: A systematic review and meta-analysis |
| 102 | Acupuncture and weight loss in Asians: A PRISMA-compliant systematic review and meta-analysis |
| 103 | Effects of Acupuncture on Breast Cancer-Related lymphoedema: A Systematic Review and Meta-Analysis |
| 104 | Acupuncture for infertile women without undergoing assisted reproductive techniques (ART): A systematic review and meta-analysis |
| 105 | Moxibustion for alleviating side effects of chemotherapy or radiotherapy in people with cancer |
| 106 | Acupuncture for stable angina pectoris: A systematic review and meta-analysis |
It was only when I came across this recent paper that I realized that, apparently, I am THE WORLD CHAMPION in acupuncture reviews. The aim of this paper was to analyze the 100 most-cited systematic reviews or meta-analyses in the field of acupuncture research. 
The Web of Science Core Collection was used to retrieve lists of 100 most-cited systematic reviews or meta-analyses in the field of acupuncture research. Two authors screened literature, extracted data, and analyzed the results.
The citation number of the 100 most-cited systematic reviews or meta-analyses varied from 65 to 577; they were published between 1989 and 2018. Fourteen authors published more than 1 study as the corresponding author and 10 authors published more than 1 study as the first author.
In terms of the corresponding authors, Edzard Ernst and Linde Klaus published the most systematic reviews/meta-analyses (n = 7). The USA published most of the systematic reviews or meta-analyses (n = 24), followed by England (n = 23) and China (n = 14). Most institutions with more than 1 study were from England (4/13). The institutions with the largest numbers of most-cited systematic reviews or meta-analyses were the Technical University of Munich in Germany, the University of Maryland School of Medicine in the USA (n = 8), the Universities of Exeter and Plymouth in England (n = 6), and the University of Exeter in England (n = 6). The journal with the largest number of most-cited systematic reviews or meta-analyses was the Cochrane Database of Systematic Reviews (n = 20), followed by Pain (n = 6). The majority of the 100 most-cited reviews are on pain or pain-related conditions. Only 4 of them focus on safety issues, and all of these are by my team.
The authors concluded that the 100 most-cited systematic reviews or meta-analyses in the acupuncture research field are mostly from high impact factor journals and developed countries. It will help researchers follow research hot spots, broaden their research scope, expand their academic horizons, and explore new research ideas, thereby improving the quality of acupuncture research.
The authors show that, both in the list of corresponding as well as first authors, I am in place number one! Not only that, they furthermore reveal that my department is also in place number 1 (as Universities of Exeter and Plymouth in England (n = 6), and the University of Exeter in England (n = 6) both refer to my unit [in the 19 years it existed the Exeter medical school changed affiliation twice]). This is remarkable, particularly because acupuncture was only one of several research foci of my team (the other 3 being herbal medicine, homeopathy, and spinal manipulation), and my department was closed almost 10 years ago.
When I write about acupuncture these days (mostly on this blog), I often get the impression that the true believers in this therapy don’t especially like what I have to say. I, therefore, fear that the concept of me being the WORLD CHAMPION of acupuncture reviews might cause some degree of displeasure to them.
What can I say?
Sorry guys!
The non-specific effects constitute part of the overall effect of acupuncture. It is unclear whether responders and non-responders of acupuncture experience non-specific effects differently. This analysis aimed to compare their experiences in a nested qualitative study embedded in an acupuncture trial on functional dyspepsia.
Purposive sampling was used to capture the experience of responders (n=15) and non-responders (n=15) to acupuncture via individual in-depth interviews. Design and analysis followed a framework analysis approach, with reference to an existing model on acupuncture non-specific effects. Themes emerging outside of this model were purposefully explored.
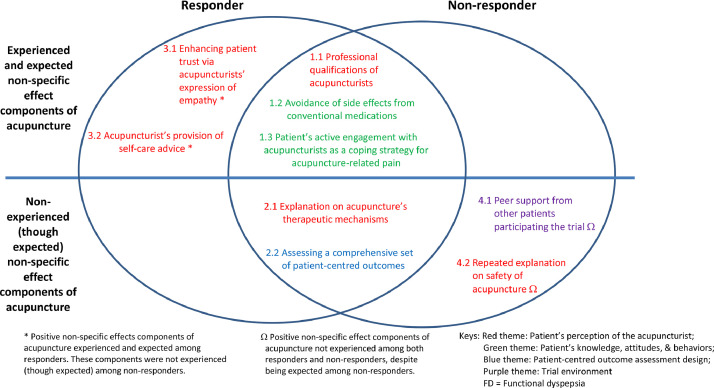
The findings suggest that responders had a more trusting relationship with the acupuncturist in response to their expression of empathy. In turn, they were more actively engaged in lifestyle modifications and dietary advice offered by acupuncturists. Non-responders were not satisfied with the level of reassurance regarding acupuncture safety. They were also expecting more peer support from fellow participants, regarded that as an empowerment process for initiating and sustaining lifestyle changes.
The authors concluded that our results highlighted key differences in acupuncture non-specific effect components experienced by responders and non-responders. Positive non-specific effects contributing to overall benefits could be enhanced by emphasizing on empathy expression from acupuncturists, trust-building, offering appropriate explanations on safety, and organizing patient support groups. Further research on the relative importance of each component is warranted.
I doubt that this tiny study lends itself to drawing any firm conclusions. However, what they seem to imply and what the authors (proponents of acupuncture) ignore totally is the following: acupuncture responders are those people who respond to the context of the treatment situation. Thus their positive result is not due to the specific effects of acupuncture itself but to non-specific effects. In other words, acupuncture operates predominantly or entirely via non-specific effects. Or, to put it bluntly: this analysis confirms what we have discussed many times before (see for instance here, here, and here), namely that
acupuncture is a placebo therapy.
The 13th European Congress for Integrative Medicine is about to take place online between 4 and 7 November 2021. It will host 125+ speakers presenting from around the world. The programme will cover the following topics.
- Anthroposophic Medicine
- Arts in Healthcare
- Acupuncture
- Antimicrobial Resistance
- Ayurveda
- Covid Research
- Diabetes
- Homeopathy
- Immunology
- Integrative Oncology
- Lifestyle Medicine
- Medical Education
- Mental Health & Stress Management
- Mind and Body Connection
- Mistletoe Therapy
- Nutrition, Gut Health & Microbiome
- Pain Management
- Patient Activation & Self-Management
- Planetary & Environmental Health
- Research and Evaluation
- Social Prescribing
- Traditional Health
- Yoga
Even looking at the more detailed list of lectures, I did not find a single contribution on conventional medicine (“Integrative medicine combines conventional medicine with…” [see below]) or a lecture that is remotely critical of integrative medicine. The definition of INTEGRATED MEDICINE (IM) adopted here seems similar to the US definition we recently discussed. Here is the European definition:
Integrative medicine combines conventional medicine with evidence-informed complementary medicine and therapies to achieve the optimum health and wellbeing of the patient. Focusing on a holistic, patient-centred approach to healthcare, it takes into consideration the patient’s physical and psychological wellbeing and treats the whole person rather than just the disease.
Allow me to do a quick analysis of this definition by looking at its key elements:
- Evidence-informed: While proper medicine is BASED on evidence, IM is merely INFORMED by it. The difference is fundamental. It allows IM clinicians to use any un- or disproven so-called alternative medicine (SCAM) they can think of or invent. The evidence for homeopathy fails to show that it is effective? Never mind, IM does not need to be evidence-based, it is evidence-informed. IM physicians know homeopathy is a placebo therapy (if not they would be ill-informed which would make them unethical), but they nevertheless use homeopathy (try to find an IM clinic that does not offer homeopathy!), because IM is not EBM. IM is evidence-informed!
- Therapies that achieve optimum health and wellbeing. This is odd because the website also states that “therapies can include anything from acupuncture, yoga, massage, aromatherapy, herbal medicine, nutrition, exercise along with many more approaches, tailored to the needs of the individual” indicating that virtually anything can be included. Anyway, “optimum health and wellbeing” seems a strange and unachievable criterion. In fact, it is nothing but a ‘bait and switch‘ salesmen’s trick.
- Holistic: This is a little trick that IM proponents love. With it, they imply that normal medicine is not holistic. However, this implication is demonstrably wrong. Any good medicine is holistic, and if a sector of healthcare fails to account for the whole person, we need to reform it. (Here are the conclusions of an editorial I published in 2007 entitled ‘Holistic heath care?‘: good health care is likely to be holistic but holistic health care, as it is marketed at present, is not necessarily good. The term ‘holistic’ may even be a ‘red herring’ which misleads patients. What matters most is whether or not any given approach optimally benefits the patient. This goal is best achieved with effective and safe interventions administered humanely — regardless of what label we put on them.) Creating a branch of medicine that, like IM, pretends to have a monopoly on holism is grossly misleading and can only hinder this process.
- Patient-centred: This is the same mean little trick in a different guise. They imply that conventional medicine is not patient-centred. Yet, all good medicine is, of course, patient-centred. To imply otherwise is just daft.
- Consideration of the patient’s physical and psychological wellbeing and treating the whole person rather than just the disease: Same trick yet again! The implication is that physical and psychological wellbeing and the whole person are not all that relevant in conventional medicine where only disease labels are being treated.
Altogether, this definition of IM is unworthy of anyone with the slightest ability to think critically. I find it much worse than the latest US definition (which already is fairly awful). In fact, it turns out to be a poorly disguised bonanza of strawman fallacies combined with ‘bait and switch’ deception.
How can this be?
How can a professional organisation engage in such mean trickery?
Perhaps a look at the list of speakers will go some way towards answering the question. Have a good look, you might recognize many individuals as members of our ALTERNATIVE MEDICINE HALL OF FAME.
PS
Registration costs £ 249 (standard rate)
PPS
Perhaps I should also mention at least 4 of the many commercial sponsors of the conference:
- Boiron
- Helixor
- Iscador
- Weleda
The British Royal Family have been proponents of homeopathy for generations. Homeopathy was originally introduced into the UK by Frederic Hervey Foster Quin who, as a young physician, had visited Hahnemann in Koethen, Germany. Quin was soon fully converted to homeopathy and returned to England. Being well-connected to the European aristocracy, he managed to attract many influential personalities to homeopathy. In 1844, he founded the British Homeopathic Society and, in 1850, he opened the predecessor of the Royal London Homeopathic Hospital which is today called the Royal London Hospital for Integrated Medicine.
Our Queen has many times been reported to swear by her homeopathic remedies. Some went as far as claiming her good health in old age must be due to her using homeopathy to keep well. Here is just one example from ‘THE OFFICIAL HOMEOPATHY RESOURCE’ of 2016:
On her 90th birthday, the London Weekly News reports that in spite of criticism the Queen has used homeopathy all her life and has remarkable good health. In fact, many generations of the Royal family have used homeopathy
For as The Queen marks her 90th birthday on April 21, that she has reached such an excellent age is largely due to her lifelong trust in homeopathy. Everywhere that Her Majesty goes she is accompanied by a small case of special cures and tinctures and, although doctors no not care to admit it, it is because of her herbal little helpers that she rarely gets a cold or any other sort of complaint.
Empiricists would argue that as both The Queen and the late Queen Mother have been avid fans of homeopathy and as The Queen Mum died at the age of 101, the glaring probability that it works seems to be rather evident.
Sadly, her good health cannot last forever, and we have all seen recent reports of her being unwell, spending one night in hospital, and announcing the cancellation of all her engagements during the next two weeks resting on doctors’ orders.
Which doctors?
Peter Fisher was her homeopath, but he tragically died three years ago. Did the Queen appoint another homeopath to look after her? Did she go into the Royal London Hospital for Integrated Medicine when she was ill? Was she reported to be taking homeopathic remedies during her recovery? The answer to all those questions seems to be NO.
What does that tell us?
I have often observed that our Royals use homeopathy while they are well and conventional medicine when they are ill. The Queen might have followed this strategy too. But not appointing a successor to Peter Fisher suggests something quite different. Does it indicate, I ask myself, that the Queen has recently had the occasion to look at the evidence and concluded – as most intelligent people did some time ago – that homeopathy does not work beyond placebo?
I certainly hope so, not least because refusing to rely on homeopathy would significantly increase her chances of remaining our Queen for some time to come.
The Austrian Health Insurance Fund is the largest social health insurance in Austria. Currently, about 82 percent of the people living in our country are insured with the ÖGK – that is 7.2 million insured persons. The ÖGK was created on 01.01.2020 through the merger of the nine former regional health insurance funds.
I was alerted to the following announcement by the Austrian Health Insurance Fund (my translation):
The Austrian Health Insurance Fund (ÖGK) ensures comprehensive medical care. However, medical services that do not treat an illness or contribute to preventive health care have to be paid for by the insured persons themselves
In the following cases, you have to pay for the services yourself, even if you use a panel doctor (Vertrauensarzt):
- Sports or driving licence examinations
- Exemptions from gym classes
- Vaccinations (if they are not medical treatment)
- Second medical opinions
- Requests for nursing leave
- Employment examinations on commencement of employment
- Treatments for which there is no scientific medical evidence of effectiveness (e.g. homeopathy)
- Purely cosmetic treatments
- Examinations for the clarification of claims for disability, occupational incapacity, incapacity to work.
The term HOMEOPATHY was not highlighted in the original. As it is, however, of particular interest to the discussions on this blog, I took the liberty of doing so.
The writing for homeopathy had been on the wall for some time in Austria- to be exact, since 1819!
This is when his majesty, the emperor Franz 2nd, issued the above decree strictly forbidding Hahnemann’s method.
My translation:
Prohibition of Hahnemann’s healing method
His Majesty, by the highest resolution of October 13, 1819, decreed: Doctor Hahnemann’s homeopathic method of treatment is to be generally and strictly prohibited.
Court Chancellery Decree of 21 October 1819, to all State Offices
I have reported about Lyma twice before (see here and here). So, why again? I know, it’s just a supplement, but it is still a special case because
- it is being marketed very aggressively,
- it is the “world’s 1st super supplement”,
- we have on this blog a long debate with one of the experts responsible for Lyma.
On 18 March 2019, Paul Clayton, a clinical pharmacologist employed by the firm, stated the following about Lyma: you will realise that all the actives bar one (the ashwagandha) are food derivates / extracts. I take this to mean that, except for ashwagandha, all the ingredients of Lyma ought to be inherently safe. If we accept this for a moment (even though I am not sure that it is entirely correct), it means that ashwagandha determines the safety of Lyma more than any of the other ingredients. Paul Clayton also assured us that Lyma is totally safe, meaning that no serious concerns about ashwagandha’s safety have been reported.
Sadly, this does not seem to be quite true. There have been several reports of liver injury after the consumption of the herbal remedy. Here is another article that is not Medline-listed: Inagaki K, Mori N, Honda Y, Takaki S, Tsuji K, Chayama K. A case of drug-induced liver injury with prolonged severe intrahepatic cholestasis induced by Ashwagandha. Kanzo 2017; 58: 448-54. (20 year old man developed jaundice a month after increasing the dose of ashwagandha [bilirubin 20.7 mg/dL, ALT 94 U/L, Alk P 343 U/L, INR 1.02], jaundice persisting for more than 2 months, but ultimately resolving).
Perhaps the most concerning paper is this latest article:
Background & aims: Ashwagandha (Withania somnifera) is widely used in Indian Ayurvedic medicine. Several dietary supplements containing ashwagandha are marketed in the US and Europe, but only one case of drug-induced liver injury (DILI) due to ashwagandha has been published. The aim of this case series was to describe the clinical phenotype of suspected ashwagandha-induced liver injury.
Methods: Five cases of liver injury attributed to ashwagandha-containing supplements were identified; three were collected in Iceland during 2017-2018 and two from the Drug-Induced Liver Injury Network (DILIN) in 2016. Other causes for liver injury were excluded. Causality was assessed using the DILIN structured expert opinion causality approach.
Results: Among the five patients, three were males; mean age was 43 years (range 21-62). All patients developed jaundice and symptoms such as nausea, lethargy, pruritus and abdominal discomfort after a latency of 2-12 weeks. Liver injury was cholestatic or mixed (R ratios 1.4-3.3). Pruritus and hyperbilirubinaemia were prolonged (5-20 weeks). No patient developed hepatic failure. Liver tests normalized within 1-5 months in four patients. One patient was lost to follow-up. One biopsy was performed, showing acute cholestatic hepatitis. Chemical analysis confirmed ashwagandha in available supplements; no other toxic compounds were identified. No patient was taking potentially hepatotoxic prescription medications, although four were consuming additional supplements, and in one case, rhodiola was a possible causative agent along with ashwagandha.
Conclusions: These cases illustrate the hepatotoxic potential of ashwagandha. Liver injury is typically cholestatic or mixed with severe jaundice and pruritus, but self-limited with liver tests normalizing in 1-5 months.
In the lengthy exchanges between Paul Clayton and others on my blog – truly worth reading! – Paul assured us all that he is a serious scientist who would not mislead the consumer. At the time, he might not have been aware of the above-mentioned reports (the most recent of the above-mentioned papers was published in April 2020). Today, however, he must know of these concerns. Therefore, we can soon expect some serious measures from him and his employers, the firm that manufactures/sells Lyma.
I wonder what they will do. As far as I can see, it will have to be the voluntary withdrawal of Lyma from the market or, at the very least, the inclusion of a warning in all their materials:
“This product may cause severe liver damage”.
In so-called alternative medicine (SCAM), vitamin D is often recommended for a range of indications, including cancer prevention. Observational studies did indeed suggest that low vitamin D status may be a risk factor for cancer. On the basis of such evidence, a team of researchers sought to determine if vitamin D supplementation lowers the risk of cancer and precancers.
The Vitamin D and type 2 diabetes (D2d) cancer outcomes study (D2dCA) is an ancillary study to the D2d study, which was conducted at 22 academic medical centers in the United States. Participants had prediabetes and overweight/obesity and were free of cancer for the previous 5 years. Participants were randomized to receive vitamin D3 4000 IU daily or placebo. At scheduled study visits (4 times/year), cancer and precancer events were identified by questionnaires. Clinical data were collected and adjudicated for all reported events. Cox proportional hazard models compared the hazard ratio (HR) of incident cancers and precancers between groups.
Over a median follow-up period of 2.9 years, among 2385 participants (mean age 60 years and 25-hydroxyvitamin D 28 ng/mL), there were 89 cases of cancer. The hazard ratio (HR) of incident cancer for vitamin D vs placebo was 1.07 (95% CI 0.70, 1.62). Of 241 participants with incident precancers, 239 had colorectal adenomatous polyps. The HR for colorectal polyps for vitamin D vs placebo was 0.83 (95% CI 0.64, 1.07).
The authors concluded that, in the D2d population of participants with prediabetes and overweight/obesity, not selected for vitamin D insufficiency, vitamin D supplementation did not have a significant effect on risk of incident cancer or colorectal polyps.
For some reason, the discussions about the value of vitamin D for any condition tend to be dominated by emotion rather than evidence. This is particularly true in the realm of SCAM. The trial is a significant step forward. It is rigorous and generates clear findings. Let’s hope it will contribute to a more rational debate about the value of vitamin D in cancer prevention.
The secret is simple, and it is for sale. The advertising could not be clearer:
“Get ready for some good lovin’ because more blood to your bits means better stimulation to your love organ, which may improve fertility and give you a boost to your libido.”
The supplement that can achieve all this for you is called ‘Nitro Wood‘. It contains the following ingredients:
PINE BARK + BEETROOT + CINNAMON + GRAPE SEED EXTRACT + GARLIC EXTRACT + CAYENNE PEPPER
And these herbal remedies are claimed to have the following effects:
- Promotes Nitric Oxide Production Studies suggest that almost half the cases of sexual dysfunction in men are from lack of nitric oxide. This explosive blend naturally triggers the best kind of nitric oxide production — your own body’s.
- Lowers Blood Pressure Healthy blood vessels significantly lower your risks of heart disease and stroke. This combination of superfood extracts is high in nitrates, which is nature’s way of keeping your blood pressure in check.
Improves Physical Performance You’ll notice a vast improvement in your physical activity and endurance, whether at the gym or in the bedroom. Whatever the playground, you’ll be knocking it out of the park!
And it comes with an authoritative endorsement:
Nitro Wood contains key nutrients that are proven to support healthy blood flow, improving your overall wellness, energy levels and performance in the gym — and in the bedroom (if you know what we mean 😉
Cedars-Sinai Cardiologist Dr. David M. Filsoof, M.D.
And at an ‘auto subscription’ prize of US$ 34.39 for 30 servings, this seems a bargain too good to miss. There is, as far as I can see, just one tiny little snag: I failed to find anything that looks remotely like evidence to suggest that ‘Nitro Wood’ has any effect whatsoever.
So, in case you are disappointed by this product and also prefer something that is ‘super safe’, how about this gadget? 
Doubting your capability in bed? We got you! We are happy to offer you a product that can make you last long in bed while providing the maximum performance! Introducing the 4000ions HardSteel AlphaMaleMagnetic Bracelet
This STYLISH BRACELET is POWERED by a BUILT-IN INFRARED that has a BIO-ACT TECHNOLOGY that DELIVERS the fir (far-infrared) energy into a nano structure that PENETRATES DEEPLY in to the human skin and provides the following benefits: Reduces Inflammation, Strengthens Heart Health, Aids Digestion, Lowers Blood Pressure, Detoxify Body, Relieves Stress and Boosts Immune System.
Please note how almost all the buzz-words of so-called alternative medicine are elegantly put to their strongest advantage:
- bio
- energy
- nano
- detox
- stress
- immune system
The ‘4000ions HardSteel AlphaMaleMagnetic Bracelet’ has the additional advantage of being more economical. It costs just Euro 10.26!
Alas, the gadget has the same drawback as the ‘Nitro Wood’ supplement: there is not a jot of evidence to suggest that it helps anyone else than the manufacturer.
Increased intestinal permeability, also often called leaky gut syndrome, has been popularized by some health practitioners, mainly those of so-called alternative medicine (SCAM). There is insufficient evidence to support its existence and the claim that SCAMs are effective treatments of it is unsubstantiated.
This study aims to describe the health-seeking behavior of Australian adults with suspected increased intestinal permeability (IP). A cross-sectional survey was conducted of 589 Australian adults who have been diagnosed with IP or have suspected (undiagnosed) IP.
The majority (56.2%) of participants with suspected IP reported self-diagnosing their condition, with the majority (56.7%) of these participants preferring to be assessed using an accurate method by a general practitioner or naturopath. On average, Australian adults with suspected IP spent 11.1 (95% CI: 9.5, 12.8) years between first suspecting IP and receiving a formal diagnosis. Over the previous 12 months, participants spent an average of $699 on consultation fees, $2176 on dietary supplements for the treatment of IP, and an average of $287 on the assessment of IP. Furthermore, participants who find it difficult to live on their available household income spent significantly more (mean=$2963) on dietary supplements compared to participants who find it easy to live on their available household income ($1918) (p=0.015).
In terms of the preferred method of treating IP, participants ‘strongly prefer’ the use of dietary products (n=392, 82.2%), followed by lifestyle habits (n=357, 76.5%), and dietary supplements (n=324, 68.6%). On the contrary, 82.8% (n=351) of participants ‘slightly prefer’ the use of medications to treat IP, representing the least preferred method of IP treatment.
The authors concluded that the majority of participants experienced a considerable length of time between first suspecting IP and receiving a diagnosis of IP. The out-of-pocket expenditure associated with the management of IP suggests a financial burden for people with suspected IP. The results of this study provide novel patient-centred considerations that can be used to inform a clinical practice guideline for the management of IP.
I would, however, draw a very different conclusion from these data: patients who think they suffer from IP often fall into the hands of SCAM practitioners who assure them to have a non-existing disease and relieve them of their money by treating them with bogus SCAM.