research
The KFF provides reliable, accurate, and non-partisan information to help inform health policy in the US. The KFF has just released its ‘Health Misinformation Tracking Poll Pilot‘ examining the public’s media use and trust in sources of health information and measuring the reach of specific false and inaccurate claims surrounding three health-related topics: COVID-19 and vaccines, reproductive health, and gun violence. It makes grimm reading indeed. Here are but a few excerpts pertaining to health/vaccination:
Health misinformation is widespread in the US with 96% of adults saying they have heard at least one of the ten items of health-related misinformation asked about in the survey. The most widespread misinformation items included in the survey were related to COVID-19 and vaccines, including that the COVID-19 vaccines have caused thousands of deaths in otherwise healthy people (65% say they have heard or read this) and that the MMR vaccines have been proven to cause autism in children (65%).
Regardless of whether they have heard or read specific items of misinformation, the survey also asked people whether they think each claim is definitely true, probably true, probably false, or definitely false. For most of the misinformation items included in the survey, between one-fifth and one-third of the public say they are “definitely” or “probably true.” The most frequently heard claims are related to COVID-19 and vaccines.
Uncertainty is high when it comes to health misinformation. While fewer than one in five adults say each of the misinformation claims examined in the survey are “definitely true,” larger shares are open to believing them, saying they are “probably true.” Many lean towards the correct answer but also express uncertainty, saying each claim is “probably false.” Fewer tend to be certain that each claim is false, with the exception of the claim that more people have died from the COVID-19 vaccines than from the virus itself, which nearly half the public (47%) recognizes as definitely false.
Across the five COVID-19 and vaccine related misinformation items, adults without a college degree are more likely than college graduates to say these claims are definitely or probably true. Notably, Black adults are at least ten percentage points more likely than White adults to believe some items of vaccine misinformation, including that the COVID-19 vaccines have caused thousands of sudden deaths in otherwise healthy people, and that the MMR vaccines have been proven to cause autism in children. Black (29%) and Hispanic (24%) adults are both more likely than White adults (17%) to say that the false claim that “more people have died from the COVID-19 vaccine than have died from the COVID-19 virus” is definitely or probably true. Those who identify as Republicans or lean towards the Republican Party and pure independents stand out as being more likely than Democratic leaning adults to say each of these items is probably or definitely true. Across community types, rural residents are more likely than their urban and suburban counterparts to say that some false claims related to COVID vaccines are probably or definitely true, including that the vaccines have been proven to cause infertility and that more people have died from the vaccine than from the virus.
Educational attainment appears to play a particularly important role when it comes to susceptibility to COVID-19 and vaccine misinformation. Six in ten adults with college degrees say none of the five false COVID-19 and vaccine claims are probably or definitely true, compared to less than four in ten adults without a degree. Concerningly, about one in five rural residents (19%), adults with a high school education or less (18%), Black adults (18%), Republicans (20%), and independents (18%) say four or five of the false COVID-19 and vaccine misinformation items included in the survey are probably or definitely true.
________________________________
If you have followed some of the comments on this blog, you might find it hard to be surprised!
I do encourage you to read the full article.
For about 40 years, the RMIT University in Australia had a Bachelor of Health Science/Bachelor of Applied Science (Chiropractic), probably the first official course of its kind in Australia. “Get qualified with a chiropractic degree: a solid grounding in anatomy, physiology and pathology and practise at the RMIT Health Clinic” was how the RMIT advertised it. But now the website states this: “from 2023, this degree is no longer offered.”
The Australian Chiropractors Association (ACA) is appalled!!!
- the main contribution of chiros to public health is that many of them advise AGAINST immunizations;
- a significant contribution by chiropractors to the health of the elderly is that they have put many of them in wheelchairs.
‘Chiropractic Economics‘ focuses on “bridging the gap between what doctors of chiropractic learn about healthcare and what they need to know as entrepreneurs who command successful, thriving practices. We are the top-rated resource for chiropractic news, marketing, consulting, financial planning, attracting and retaining patients, and motivating and managing employees. We provide information for practicing chiropractors, with a focus on office management, patient relations, personal development, financial planning, legal, clinical and research data, and wellness and nutrition.”
The magazine recently published an article that is so wonderfully overflowing with BS that I cannot resist showing you a few hilarious excerpts from it:
HOMEOPATHY IS A NATURAL FOR CHIROPRACTORS — because it works with innate intelligence. Each tiny pellet of a homeopathic remedy is like a flash drive full of information that “reinstalls the software,” i.e., it reminds the body that “you know how to have a healthy nervous system” or strong and healthy bones or muscles.
A remedy for patient malady
Homeopathic remedies have much to offer your patients:
- Fast-acting: Some patients will actually feel the effects as soon as they ingest the remedy; it works faster than herbs or vitamins
- Easily available in health food stores, some drug stores and online
- Inexpensive: pennies per dose
- No rebound or withdrawal: Your patient can discontinue it without symptoms recurring
- No drug interactions: It can work well alongside meds and supplements
- Safe: Reactions are rare and serious side effects are unknown.1
Practitioners will benefit as well from recommending homeopathy as this unusual modality will set the chiropractor apart and patients will be grateful for the relief they feel. Homeopathy is available as single remedies, plus more unusual ones are also blended into combination formulas which chiropractors may choose to stock in their office, just as they stock nutritional supplement and glandular formulas.
…
How does it work?
Homeopathy is totally safe because there is nothing in it — not even one molecule of its original starting substance — yet it is powerful and fast-acting. How can we make these contradictory claims? Because it is information technology.
The manufacturing process imprints the healing information onto water like recording onto a flash drive. The process takes the starting substance through many stages of dilution (making it safe) and potentizes or energizes it at each step (making it powerful). Water behaves differently at these very high dilutions, becoming coherent or structured, as explained by the newly emerging field of ultra-high dilution physics. Two Nobel laureates have testified that their studies explain how homeopathy works.2
Now let’s look at some specific remedies.
Hypericum for the nervous system
Hypericum is almost a universal remedy for nerve-related symptoms: tingling and numbness, pain shooting along a nerve, and trauma to nerve-rich areas (like hitting a finger with a hammer or slamming it in a car door):
- Arnica for soft tissue trauma: homeopathy’s best-known remedy, Arnica is good for sore muscles, pulled muscles, sports injuries, sprains and strains, and bruising.
- Symphytum for fractures: This is the well-known herbal remedy comfrey, known traditionally as “knit-bone,” used to speed the healing of fractures and reduce bone pain.
- Bryonia for joints that hurt to move. When your patient is splinting or guarding, think bryonia, for a bruised rib that makes it painful to laugh or cough or sneeze, or knees that hurt from walking that make the patient take cautious steps.
- Rhus tox for “rusty gate” joints: This is for your patient who needs to limber up when first getting out of bed, or who needs to swing their leg a few times to loosen it up before getting up from a chair.
- Ruta grav. for connective tissue, cartilage and joints in general: sprains and strains, cracking joints, torn tendons and ligaments, and fascia. It has a special affinity for the knee, like the knee that goes out from under someone and for Baker’s cysts.
Three homeopathically-energized minerals to strengthen and heal bone need to be given in a special 6x potency and are known as cell salts or tissue salts:
- Calcarea fluorica (Calc. fluor.) 6x to soften and dissolve: This remedy can help dissolve bone spurs and hardened or condensed tissues like cataracts.
- Calcarea phosphorica (Calc. phos.) 6x to deposit minerals in the bones: This provides the template to send calcium and other minerals to bones and not deposit them elsewhere in the body.
- Silicea 6x strengthens bone as well as hair, skin and nails; you know silica as a supplement, and as a homeopathic remedy it provides the instructions for silica the mineral to go where it is needed. However, Silica 30c (full strength) can push foreign objects out of the body and should not be given to patients with a rod or plate and screws.
…
What could possibly go wrong?
Not much — an “overdose” in homeopathy is not harmful in the long run — in fact, too much of a remedy is pushing the patient too fast in the direction of cure and the long-term result can be positive. It can be uncomfortable in the short run, though.
The body can only process so much of the remedy’s information at once, and if the body is presented with more than it can handle, it pushes back in the form of increased symptoms, the same symptoms the remedy was intended to treat. This is called an “aggravation” in homeopathy. It’s often said that “You have to get worse before you get better” in homeopathy and this is absolutely not true as long as mild to moderate doses are used (the typical 30c dose in health food stores) and the patient is told to stop if the remedy starts to feel too intense. When in doubt, it’s always safe to stop the remedy and start again later.
The bottom line
Start by recommending these few remedies and you are likely to get good feedback from your patients. Or consider stocking combination remedies that include even more unusual remedies.
They may give even better results and keep patients coming back to you for more, since they are only available through professionals. And if you’re feeling exhausted beyond repair, try some Sepia for yourself.
____________________________
END OF QUOTE
Yes, this is what a ‘top rated’ chiropractic resource mistakes for information on ‘clinical and research data, and wellness and nutrition’!
I didn’t promise too much, did I?
I was asked by NATURE to provide a comment on the WHO Traditional Medicine Global Summit: Towards health and well-being for all which is about to take place in India:
The First WHO Traditional Medicine Global Summit will take place on 17 and 18 August 2023 in Gandhinagar, Gujarat, India. It will be held alongside the G20 health ministerial meeting, to mobilize political commitment and evidence-based action on traditional medicine, which is a first port of call for millions of people worldwide to address their health and well-being needs.
The Global Summit will be co-hosted by WHO and the Government of India, which holds the presidency of the G20 in 2023. It will be a platform for all stakeholders, including traditional medicine workers, users and communities, national policymakers, international organizations, academics, private sector and civil society organizations, to share best practices and game-changing evidence, data and innovation on the contribution of traditional medicine to health and sustainable development.
For centuries, traditional and complementary medicine has been an integral resource for health in households and communities. It has been at the frontiers of medicine and science laying the foundation for conventional medical texts. Around 40% of pharmaceutical products today have a natural product basis, and landmark drugs derive from traditional medicine, including aspirin, artemisinin, and childhood cancer treatments. New research, including on genomics and artificial intelligence are entering the field, and there are growing industries for herbal medicines, natural products, health, wellness and related travel. Currently, 170 Member States reported to WHO on the use of traditional medicine and have requested evidence and data to inform policies, standards and regulation for its safe, cost-effective and equitable use.
In response to this increased global interest and demand, WHO, with the support of the Government of India, established in March 2022 the WHO Global Centre for Traditional Medicine as a knowledge hub with a mission to catalyse ancient wisdom and modern science for the health and well-being of people and the planet. The WHO Traditional Medicine Centre scales up WHO’s existing capacity in traditional medicine and supplements the core WHO functions of governance, norms and country support carried out across the six regional Offices and Headquarters.
The Centre focuses on partnership, evidence, data, biodiversity and innovation to optimize the contribution of traditional medicine to global health, universal health coverage, and sustainable development, and is also guided by respect for local heritages, resources and rights.
A cross-regional expert panel will advise on the Summit’s theme, format, topics and issues to address. All updates will be posted here and on the forthcoming webpages for the First WHO Traditional Medicine Global Summit.
In case you are interested, the programme can be seen here.
And my comment? I am afraid, it was not very encouraging. I doubt that Nature will publish it in full. So, allow me to show you my unabridged comment:
This article entitled: Keeping Medical Science Trustworthy: The Threat by Predatory Journals caught my attention.
Many scientific journals have started to ask article processes costs from authors. This development has created a new category of journals of which the business model is totally or predominantly based on financial contributions by its authors. Such journals have become known as predatory journals. The financial contributions that they ask are not necessarily lower than those asked by high-quality journals although they offer less:
- there is commonly no real review,
- texts are not edited,
- there are commonly no printed editions.
The lack of serious reviews might make predatory journals attractive particularly to authors of low-quality (or even fraudulent) manuscripts.
The authors of this paper suggest that numerous journals, some of which may predatory, attract manuscripts by approaching authors of articles in high-quality journals. They conclude that publication of articles in such journals contaminates the medical literature and undermines the trustworthiness of science and medicine. Any involvement in such journals (as an author, reviewer or editor) should therefore be discouraged.
The ironic thing here is that the paper was published by a journal that itelf is, in my view, borderline, to say the least. But let me nonetheless contribute a recent, personal experience on this issue.
About 2 weeks ago, I received an invitation to join the editorial board of a general medicine journal that I had never heard of. I looked it up and found that it had a decent impact factor and a long list of international members of the board. But then I found that the journal charged around $ 1 500 for each submission. I was told that this is to cover the cost of the review process.
I then decided to write to the editor thanking her for the kind invitation. I also asked her how much the journal would pay its reviewers for reviewing submissions. I received a polite answer explaining that the amount was $ 00.00. My response was to politely decline the invitation to join the editorial board and to urge the journal editor to make it clear from the outset that the fees charged to authors did NOT go to the reviewers.For many years now, I have taken a very dim view on predatory journals. Sadly, in the realm of so-called alternative medicine (SCAM), there currently are dozens of such publications. I believe their danger in polluting the medical literature is hard to over-estimate. I think they ought to be stopped. One way of doing this is refusing to co-operate with them in any way.
Charles has a well-documented weakness for so-called alternative medicine (SCAM) – not just any SCAM but predominantly the type of SCAM that is both implausible and ineffective. Therefore, nobody can be all that surprised to read in THE TIMES that he has decided to use SCAM for helping women who have difficulties getting pregnant.

If one really wanted to employ SCAM for this aim one is spoilt for choice. In fact, there are only few SCAMs that don’t claim to be useful for this purpose.
A recent review, for instance, suggested that some supplements might be helpful. Other authors advocate SCAMs such as acupuncture, moxibustion, Chinese herbal medicine, psychological intervention, biosimilar electrical stimulation, homeopathy, or hyperbaric oxygen therapy.
Yes, I know! The evidence for these treatments is lousy, and I would never issue a recommendation based on such flimsy evidence.
Yet, the SCAM project at Dumfries House, the Scottish stately home Charles restored in 2007, offers acupuncture, reflexology, massage, yoga, and hypnotherapy for infertile women.
REFLEXOLOGY for female infertility?
Reflexology, also called zone therapy, is a manual treatment where pressure is applied usually to the sole of the patient’s foot and sometimes also to other areas such as the hands or ears. According to its proponents, foot reflexology is more than a simple foot massage that makes no therapeutic claims beyond relaxation. It is based on the idea that the human body is divided into 10 zones each of which is represented on the sole of the foot. Reflexologists employ maps of the sole of the foot where the body’s organs are depicted. By massaging specific zones which are assumed to be connected to specific organs, reflexologists believe to positively influence the function of these organs. While reflexology is mostly used as a therapy, some therapists also claim they can diagnose health problems through feeling tender or gritty areas on the sole of the foot which, they claim, correspond to specific organs.
Reflexology is not merely implausible as a treatment for infertility, it also boasts of some fairly rigorous trial evidence. A clinical trial (perhaps even the most rigorous of all the trials of SCAM for female fertility problems) testing whether foot reflexology might have a positive effect on the induction of ovulation stated that “the results suggest that any effect on ovulation would not be clinically relevant”.
So, as so often before in the realm of SCAM, Charles has demonstrated that his lack of critical thinking leads him to the least promising options.
Well done, Your Majesty!
Like ultra-processed food (UPF) itself, the subject of UPF is everywhere – radio, TV, Twitter, you name it, the topic crops up. I too could not resist writing a post on it a few months ago. And now I am publishing another one but one in a slightly more irritated mood.
Why do these endless discussions on UPF irritate me?
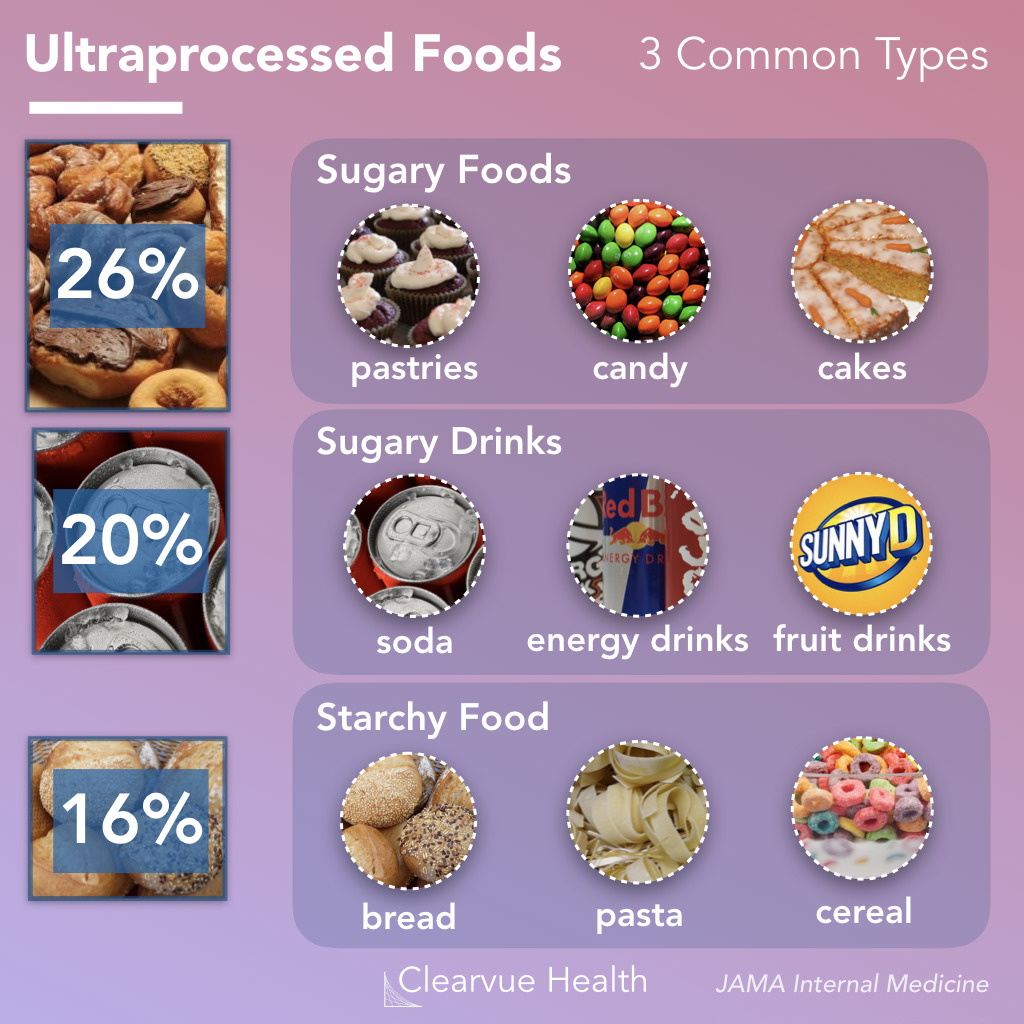
To start with, there is no uniform definition of UPF, and many commentators seem more than a little confused about what UPF actually is. One definition holds that Ultra-processed foods are foods that have been altered to include fats, starches, sugars, salts and hydrogenated oils extracted from other foods. They contain ingredients, additives, and preservatives that are not normally used in home cooking. It seems obvious that discussions on UPF without a clear and understandable definition of the term are merely generating confusion in the general public.
But there are, of course, lists of UPF that might render the subject a bit clearer. The trouble, however, is that these lists reveal disagreement among each other. Thus they are prone to generate even more confusion.
Next, there is the evidence – and there is lots of it. It suggests that the regular consumption of UPF is bad for virtually every aspect of health. And if there is no evidence that it is detrimental for a given condition, it probably is merely because nobody has yet bothered to do the analyses. The trouble is, however, that all the relevant research comes from either basic science or epidemiology. This means that causality is unproven.
A further problem is that even the experts don’t know what the alleged causal factors in UPF are.
- Is it the processing?
- The additives?
- The sugar?
- The fats?
- If so, which fats exactly?
- Is it perhaps a complex inter-play of some of these factors?
If we want to make progress, we need to know! If not, we cannot possibly begin to avoid the health-threatening effects of UPF.
The final and arguably biggest problem is that UPF is everywhere. Nobody living in an industrialized country and earning a regular living can avoid consuming UPF. This means, I fear, that all the current hype about UPF is not just irritating but possibly counter-productive.
Imagine an average person trying to make sense of these discussions. She would soon give up and conclude that all these ‘clever’ experts know nothing at all. Her foremost concern is to make ends meet. In the end, she will carry on as before. Alternatively, she might even conclude that, as the even experts do not make sense, UPF cannot be all that bad after all.
After reading about and listening to the arguments around UPF, I ask myself this: would it not be more productive to apply more common sense and focus on a few nutritional messages that are 1) solidly based on evidence and 2) an average person can actually follow?
This systematic review evaluated all available randomized controlled trials (RCTs) investigating the clinical effects of hydrotherapy according to Kneipp which is characterized by cold water applications. All RCTs on therapy and prevention with Kneipp hydrotherapy were included. Study participants were patients and healthy volunteers of all age groups. MEDLINE (via PubMed), Scopus, Central, CAMbase, and opengrey.eu were systematically searched through April 2021 without language restrictions and updated by searching PubMed until April 6th 2023. The risk of bias was assessed using the Cochrane tool version 1.
Twenty RCTs (N=4247) were included. Due to the high heterogeneity of the RCTs, no meta-analysis was performed. The risk of bias was rated as unclear in most of the domains. Of 132 comparisons, 46 showed significant positive effects in favor of hydrotherapy on chronic venous insufficiency, menopausal symptoms, fever, cognition, emotional function, and sickness absenteeism. However, 81 comparisons showed no differences between groups, and 5 were in favor of the respective control group. Only half of the studies reported safety issues.
The authors concluded that although RCTs on Kneipp hydrotherapy seem to show positive effects in some conditions and outcomes, it remains difficult to ascertain treatment effects due to the high risk of bias and heterogeneity of most of the considered studies. Further high-quality RCTs on Kneipp hydrotherapy are urgently warranted.
This is certainly the best review of the subject so far. It makes it very clear that the evidence for Kneipp hydrotherapy is weak, mostly because of the many flaws in the primary studies. One needs to add, I think, that 20 RCTs are an absurdly small amount considering that many indications this type of therapy is advocated for – many enthusiasts even consider it a panacea.
It follows, I fear, that Kneipp hydrotherapy is almost entirely not evidence-based. This should be bad news for the numerous institutions and Spa towns (mostly in Germany) that live on employing this treatment and telling patients that it is effective. They usually claim that experience shows this to be true. But this was the mantra of medicine ~100 years ago. Since then, we have learned that experience is a very poor guide that regularly leads us up the garden path.
Kneippians will counter that clinical trials are difficult to conduct and expensive to finance. Both arguments are of course true but, considering that an entire industry lives on telling patients something that essentially amounts to a lie (i.e. the claim that it works), it surely is obligatory to overcome these obstacles.
This review assessed the role of homoeopathy in the therapeutic management of substance use disorders (SUD) through a systematic web-based literature search. A comprehensive search was conducted online and manually to identify homoeopathic research studies published between 1993 and 2022 on SUD in international databases and the Central Council of Research in Homoeopathy library. Relevant studies were categorised and assessed in terms of study designs, number of participants, evidence grades and clinical outcome parameters. A total of 21 full-text studies were screened and evaluated. Risk of bias (RoB) was assessed for all studies and model validity was appraised for the included RCTs’.
10 studies were included:
- 3 Randomised Controlled Trials,
- 3 Observational studies,
- 1 Pilot study,
- 1 observational comparative study,
- 1 retrospective cohort study,
- 1 case series.
Three studies have a level of evidence of 1b with an ‘A’ grade of recommendation, which consists of the RCTs only. The most commonly prescribed medicines identified were:
- Arsenic album,
- Nux vomica,
- Lycopodium,
- Pulsatilla,
- Sulphur,
- Staphysagria,
- Belladonna,
- Ipecac,
- Chamomilla,
- Rhustox,
- Phosphorus,
- Lachesis.
A high risk of bias was elicited in most of the observational studies accentuating the need for more robust methodological studies.
The authors concluded that the majority of the studies have a small number of recruitments. Pragmatic studies with larger sample sizes and validated outcome measures may be designed further to validate the
promising role of homoeopathic medicines in SUDs and generate quality evidence.
The paper is surprising! Most of the studies are not RCTs and thus cannot come even near suggesting a causal effect of homeopathy. The three RCTs are the following:
- Manchanda RK, Janardanan Nair KR, Varanasi R, Oberai P, Bhuvaneswari R, Bhalerao R, et al. A randomised comparative trial in the management of alcohol dependence: Individualised homoeopathy versus standard allopathic treatment. Indian J Res Homoeopathy; 2016.
- Adler UC, Acorinte AC, Calzavara FO, et al. Double-blind evaluation of homeopathy on cocaine craving: A randomised controlled pilot study. J Integr Med. 2018; 16(3):178-184.
- Grover A, Bhushan B, Goel R. Double-blind placebo-controlled trial of homoeopathic medicines in the
management of withdrawal symptoms in opium addicts and its alkaloid derivatives dependents. Indian J Res Homoeopathy. 2009;3:41-4.
All of these 3 studies were assessed by the review authors as having major flaws. Only one is available on Medline:
Background: Brazil is among the nations with the greatest rates of annual cocaine usage. Pharmacological treatment of cocaine addiction is still limited, opening space for nonconventional interventions. Homeopathic Q-potencies of opium and Erythroxylum coca have been tested in the integrative treatment of cocaine craving among homeless addicts, but this setting had not proven feasible, due to insufficient recruitment.
Objective: This study investigates the effectiveness and tolerability of homeopathic Q-potencies of opium and E. coca in the integrative treatment of cocaine craving in a community-based psychosocial rehabilitation setting.
Design, setting, participants, and interventions: A randomized, double-blind, placebo-controlled, parallel-group, eight-week pilot trial was performed at the Psychosocial Attention Center for Alcohol and Other Drugs (CAPS-AD), Sao Carlos/SP, Brazil. Eligible subjects included CAPS-AD patients between 18 and 65 years of age, with an International Classification of Diseases-10 diagnosis of cocaine dependence (F14.2). The patients were randomly assigned to two treatment groups: psychosocial rehabilitation plus homeopathic Q-potencies of opium and E. coca (homeopathy group), and psychosocial rehabilitation plus indistinguishable placebo (placebo group).
Main outcome measures: The main outcome measure was the percentage of cocaine-using days. Secondary measures were the Minnesota Cocaine Craving Scale and 12-Item Short-Form Health Survey scores. Adverse events were reported in both groups.
Results: The study population comprised 54 patients who attended at least one post-baseline assessment, out of the 104 subjects initially enrolled. The mean percentage of cocaine-using days in the homeopathy group was 18.1% (standard deviation (SD): 22.3%), compared to 29.8% (SD: 30.6%) in the placebo group (P < 0.01). Analysis of the Minnesota Cocaine Craving Scale scores showed no between-group differences in the intensity of cravings, but results significantly favored homeopathy over placebo in the proportion of weeks without craving episodes and the patients’ appraisal of treatment efficacy for reduction of cravings. Analysis of 12-Item Short-Form Health Survey scores found no significant differences. Few adverse events were reported: 0.57 adverse events/patient in the homeopathy group compared to 0.69 adverse events/patient in the placebo group (P = 0.41).
Conclusions: A psychosocial rehabilitation setting improved recruitment but was not sufficient to decrease dropout frequency among Brazilian cocaine treatment seekers. Psychosocial rehabilitation plus homeopathic Q-potencies of opium and E. coca were more effective than psychosocial rehabilitation alone in reducing cocaine cravings. Due to high dropout rate and risk of bias, further research is required to confirm our findings, with specific focus on strategies to increase patient retention.
This study can hardly be said to show convincing evidence for homeopathy.
This paper is all the more surprising if we consider the affiliations of the authors:
- Clinical Research Unit (H), Aizawl under Central Council for Research in Homoeopathy, Ministry of AYUSH, Govt. of India, India.
- All India Institute of Ayurveda, New Delhi, India.
- Department of Materia Medica, Madhav Homoeopathic Medical College and Hospital, Madhav Hills,
Opposite Banas River, Abu Road, Rajasthan, India.
It is time, I think, that Indian officials and researchers learn some critical thinking and formulate the conclusions of reviews based on the evidence they produced. This would be a start:
Our review has not generated convincing evidence to suggest that homeopathy is effective in treating SUDs.
Guest post by Norbert Aust, Udo Endruscheit, and Edzard Ernst
How do we know whether a treatment is reasonable or just some so-called alternative medicine (SCAM) that is at best useless? A simple answer is that the former is evidence-based, while the latter is not. But how can we tell the difference? High-quality studies, with independent replications or even a systematic review, are the sort of things we are usually looking for. But there is an underlying assumption, namely that, in science, bogus studies are prevented from polluting the scientific database or, if such trials have emerged, there are ways to identify and eliminate them.
And what if this assumption is wrong?
What if respectable universities and research organizations venture into the realm of pseudoscience either knowingly or because it had slipped their attention?
What if the editorial board of a top journal passes bogus studies to peer review?
What if such a paper is eventually reviewed by a proponent of the implausible therapy?
What if the readers of the article, once it is published, are too lethargic to object and do not write letters to the editor in protest?
And what if skeptics do formulate a protest but the journal editor refuses to publish it?
Well, if all the checks that should prevent faulty results from entering the scientific knowledge fail, we have fake evidence: a study that looks like sound science but that, in fact, is invalid. It is not hard to imagine what would happen if SCAM therapies are supported by seemingly respectable studies published in top journals. The fake evidence would accumulate as part of the body of evidence and eventually enter mainstream clinical practice, education, politics, etc., etc. Thus the reputation of bogus therapies would grow unjustifiably.
If you think this cannot happen, you are in the wrong. After the infamous study by Frass et al about homeopathy as an add-on treatment for lung cancer, another homeopathy paper was published in 2022 by Gaertner et al. in Pediatric Research (PR), a Medline-indexed journal with a two-year impact factor of 3.95 belonging to the nature-group of journals. According to this meta-analysis ‘individualized homeopathy showed a clinically relevant and statistically robust effect in the treatment of ADHD’. Shortly after the publication of this paper, we sent a letter to the editor to point out the shortcomings of this study. Here it is:
Sir,
with this letter we like to comment on the systematic review and meta-analysis on childhood ADHD by Gaertner et al. recently published in your journal.
First off, we are surprised, that your journal that is connected to nature does publish a paper on a treatment that has no a-priory probability at all and thus can only contain false positives if any. And this review is no exception as will be seen presently.
Our concerns are:
Out of the six studies included three were mere pilot trials (Fibert_2019, Jacobs_2005, Oberai_2013, ) which cannot provide any evidence for the shortcomings involved in pilots. Three of the six trials show severe issues in blinding (Fibert_2016, Fibert_2019, Oberai_2013), with two of them concerning both of the participants and the test personnel. This usually leads to massive bias in favour of the treatment [Zitat Cochrane Handbook].
Then we compared data from two trials with the data reported in the review and found some major misrepresentations:
(1) Jacobs et al. report an improvement in the T-score of their main outcome (CGI-P) of 4.1 for homeopathy and 9.1 for controls, that is placebo outperformed the homeopathic intervention. But the authors give an effect size of 0.272 in favour of homeopathy which is the opposite of the findings in the trial.
(2) Oberai et al. report effect sizes for their three main outcomes of 0.22, 0.59 and 0.54 (CPRS-R, CGISS, CGIIS repectively). There is no way that this yields a pooled effect size of 1.436 as given in the review.
We conclude that the positive result obtained by the authors is due to a combination of the inclusion of biased trials unsuitable to build evidence together with some major misreporting of study outcomes.
Our recommendation would be that the authors reconsider their review and improve their report. Maybe the editors would like to add a caution-notice to the paper – if not to withdraw it completely.
In June 2023, a full year after our submission, we were informed that Pediatric Research would not publish our criticism because the priority given to it was not sufficient to justify publication. But we were assured, that the journal would take the matter seriously, that they will investigate this matter and take appropriate editorial action. But as of today (End of June 2023) no expression of concern has been published.
Did the journal receive other comments or criticisms related to the paper in question? No, apparently there were none, at least none was published and the paper remains unchallenged to this day. This means that it might be taken for reliable evidence on the effectiveness of homeopathy and mislead patients, carers, practitioners, decision-makers, etc.
We feel this is unacceptable and therefore again wrote to the editors asking to reconsider their decision. Here is our letter:
Dear …
together with my co-authors we would like to comment your decision about our letter to the editor about an extremely faulty and misleading paper that may well create harm to patients. In fact we find it very hard to accept your decision not to publish our comment.
We understand that Pediatric Research is a high impact journal with a 2-year IF of nearly 4. Your journal is member of COPE and is indexed with quite a few first rank institutions. By all standards, any reader will be convinced that a paper published in Pediatric Research is based on solid research and the results are derived by rigorous methodology and are as reliable as can be. Especially if this paper remains unchallenged by any reader’s comments for a full year after publication. This is your responsibility to the scientific community. And to the children that might receive treatment based on knowledge spread through your journal.
How then can it be, that an article about homeopathy, a thoroughly implausible lore, in the treatment of ADHD is published in Pediatric Research, where the authors come to the conclusion “that individualized homeopathy showed a clinically relevant and statistically robust effect in the treatment of ADHD”?
In our comment we point out that the authors made a lot of errors – to say it mildly. They deny the doubtful quality of the studies they included in their meta-analysis, they did not stick to their own exclusion criteria, the data the authors report do not resemble the findings of the studies they were allegedly taken from, the one study setting the results is a mere pilot study.
The reason you give for our letter not being published is that it was not given enough priority to justify publication. We would like to know: Which issues can conceivably receive higher priority than the fact that a paper in your journal is downright wrong and misleading?
What do you need to deem a comment important? Up to now the paper is unchallenged by any reader’s comments, so apparently there was no other letter to the editor that might be given higher priority than ours.
We ask you to review your decision, or better still, consider a retraction of the paper altogether. If so, an expression of concern should be issued at once. After all, the COPE-guidelines for retraction state “clear evidence, that the findings are unreliable, either as a result of major error (…), or as a result of fabrication (…) or faslification (…)’ as a reason to consider retraction.
Otherwise the malpractice of homeopathy will have a first class evidence that will be helpful to promote homeopathy to parents and their children.
Watch this space!