panacea
If you assumed that the best management of a child by chiropractors is not to treat this patient and refer to a proper doctor, think again. This paper was aimed at building upon existing recommendations on best practices for chiropractic management of children by conducting a formal consensus process and best evidence synthesis. Its authors composed a best practice guide based on recommendations from current best available evidence and formal consensus of a panel of experienced practitioners, consumers, and experts for chiropractic management of pediatric patients. They thus syntheized results of a literature search to inform the development of recommendations from a multidisciplinary steering committee, including experts in pediatrics, followed by a formal Delphi panel consensus process.
The consensus process was conducted June to August 2022. All 60 panelists completed the process and reached at least 80% consensus on all recommendations after three Delphi rounds. Recommendations for best practices for chiropractic care for children addressed the following aspects of the clinical encounter:
- patient communication, including informed consent;
- appropriate clinical history, including health habits;
- appropriate physical examination procedures;
- red flags/contraindications to chiropractic care and/or spinal manipulation;
- aspects of chiropractic management of pediatric patients, including infants;
- modifications of spinal manipulation and other manual procedures for pediatric patients;
- appropriate referral and comanagement;
- appropriate health promotion and disease prevention practices.
The authors concluded that this set of recommendations represents a general framework for an evidence-informed and reasonable approach to the management of pediatric patients by chiropractors.
Whenever I read the term ‘evidence-informed’ I need to giggle. Why not evidence-based? Evidence-informed might mean that chiros are informed that their treatments are useless or even dangerous for children … but, on reflection and taking their own need for earning a living, they subsequently ignore these facts. And sure enough, the authors of the present paper do mention that a Cochrane review concluded that spinal manipulation is not recommended for children under 12, for a number of conditions, or for general wellness … only to then go on and ignore the very fact.
In doing so, the authors issue a string of self-evident platitudes which occasionally border on the irresponsible. For instance, under the heading of ‘primary prevention’, vaccinations are mentioned as the very last item with the following words:
If parents ask for advice or information about childhood vaccinations, explain that they have the right to make their own health decisions. They should be adequately informed about the benefits and risks to both their child and the broader community associated with these decisions. Consider referral to a health professional whose scope of practice includes vaccinations to address patient questions or concerns.
What that really means in practice, I fear, might be summarized like this: If parents ask for advice or information about childhood vaccinations, explain that they are dangerous, and that even D. D. Palmer recognized as early as 1894 that vaccination is ‘…the monstrous delusion … fastened on us by the medical profession, enforced by the state boards, and supported by the mass of unthinking people …’
Altogether, the ‘Clinical Practice Guideline for Best Practice Management of Pediatric Patients by Chiropractors’ is a thoroughly disreputable document. It was constructed in the way all charlatans tend to construct their consensus documents:
- convene a few people who are all in favour of a certain motion,
- discuss the motion,
- agree with it,
- write up the process
- publish your paper in a third class journal,
- boast that there is a consensus,
- stress that the motion must thereefore be ethical, correct and valuable.
Do chiropractors know that, using this methodology, the ‘flat earth society’ can easily pass a consensus that the earth is indeed flat?
I am sure they do!
Many of you will be familiar with the ‘ALTERNATIVE MEDICINE HALL OF FAME’. It is my creation and meant to honour reserchers who have dedicated much of their professional career to investigating a form of so-called alternative medicine (SCAM) without ever publishing negative conclusions about it. Obviously, if anyone studies any therapy, he/she will occasionally produce a negative finding. This would be the case, even if he/she tests an effective treatment. However, if the treatment in question comes from the realm of SCAM, one would expect negative results fairly regularly. No therapy works well under all conditions, and to the best of my knowledge, no SCAM is a panacea!
This is why researchers who defy this inevitability are remarkable. If someone tests a treatment that is at best dubious and at worst bogus, we are bound to see some studies that are not positive. He/she would thus have a high or normal ‘TRUSTWORTHINESS INDEX‘ (another creation of mine which, I think, is fairly self-explanatory). Conversely, any researcher who does manage to publish nothing but positive results of a SCAM is bound to have a very low ‘TRUSTWORTHINESS INDEX‘. In other words, these people are special, so much so that I decided to honour such ‘geniuses’ by admitting them to my ALTERNATIVE MEDICINE OF FAME.
So far, this elite group of people comprises the following individuals:
- Helge Franke (osteopathy, Germany)
- Tery Oleson (acupressure , US)
- Jorge Vas (acupuncture, Spain)
- Wane Jonas (homeopathy, US)
- Harald Walach (various SCAMs, Germany)
- Andreas Michalsen ( various SCAMs, Germany)
- Jennifer Jacobs (homeopath, US)
- Jenise Pellow (homeopath, South Africa)
- Adrian White (acupuncturist, UK)
- Michael Frass (homeopath, Austria)
- Jens Behnke (research officer, Germany)
- John Weeks (editor of JCAM, US)
- Deepak Chopra (entrepreneur, US)
- Cheryl Hawk (chiropractor, US)
- David Peters (osteopathy, homeopathy, UK)
- Nicola Robinson (TCM, UK)
- Peter Fisher (homeopathy, UK)
- Simon Mills (herbal medicine, UK)
- Gustav Dobos (various SCAMs, Germany)
- Claudia Witt (homeopathy, Germany/Switzerland)
- George Lewith (acupuncture, UK)
- John Licciardone (osteopathy, US)
You will notice that the group does not yet contain a representative of anthroposophic medicine. Today, I intend to rectify this oversight by admitting Helmut Kiene (1952-). He has published plenty of studies and reviews on his pet subject; here are the ones that I found on Medline:
- Anthroposophic therapies in chronic disease: the Anthroposophic Medicine Outcomes Study (AMOS). Eur J Med Res. 2004 Jul 30;9(7):351-60.
- Anthroposophic medical therapy in chronic disease: a four-year prospective cohort study. Hamre HJ, Witt CM, Glockmann A, Ziegler R, Willich SN, Kiene H.BMC Complement Altern Med. 2007 Apr 23;7:10. doi: 10.1186/1472-6882-7-10.
- Anthroposophic art therapy in chronic disease: a four-year prospective cohort study. Hamre HJ, Witt CM, Glockmann A, Ziegler R, Willich SN, Kiene H.Explore (NY). 2007 Jul-Aug;3(4):365-71. doi: 10.1016/j.explore.2007.04.008.
- Rhythmical massage therapy in chronic disease: a 4-year prospective cohort study. Hamre HJ, Witt CM, Glockmann A, Ziegler R, Willich SN, Kiene H.J Altern Complement Med. 2007 Jul-Aug;13(6):635-42. doi: 10.1089/acm.2006.6345
- Anthroposophic vs. conventional therapy for chronic low back pain: a prospective comparative study. Hamre HJ, Witt CM, Glockmann A, Wegscheider K, Ziegler R, Willich SN, Kiene H.Eur J Med Res. 2007 Jul 26;12(7):302-10.
- Viscum album L. extracts in breast and gynaecological cancers: a systematic review of clinical and preclinical research. Kienle GS, Glockmann A, Schink M, Kiene H.J Exp Clin Cancer Res. 2009 Jun 11;28(1):79. doi: 10.1186/1756-9966-28-79.
- Anthroposophic therapy for children with chronic disease: a two-year prospective cohort study in routine outpatient settings. Hamre HJ, Witt CM, Kienle GS, Meinecke C, Glockmann A, Willich SN, Kiene H.BMC Pediatr. 2009 Jun 19;9:39. doi: 10.1186/1471-2431-9-39
- Predictors of outcome after 6 and 12 months following anthroposophic therapy for adult outpatients with chronic disease: a secondary analysis from a prospective observational study. Hamre HJ, Witt CM, Kienle GS, Glockmann A, Willich SN, Kiene H.BMC Res Notes. 2010 Aug 3;3:218. doi: 10.1186/1756-0500-3-218.
- Pulpa dentis D30 for acute reversible pulpitis: A prospective cohort study in routine dental practice. Hamre HJ, Mittag I, Glockmann A, Kiene H, Tröger W.Altern Ther Health Med. 2011 Jan-Feb;17(1):16-21.
- Use and safety of anthroposophic medications for acute respiratory and ear infections: a prospective cohort study. Hamre HJ, Glockmann A, Fischer M, Riley DS, Baars E, Kiene H.
- [Clinical research on anthroposophic medicine:update of a health technology assessment report and status quo]. Kienle GS, Glockmann A, Grugel R, Hamre HJ, Kiene H.Forsch Komplementmed. 2011;18(5):269-82. doi: 10.1159/000331812. Epub 2011 Oct 4.
- Anthroposophical medicine: a systematic review of randomised clinical trials. Kienle GS, Hamre HJ, Kiene H.Wien Klin Wochenschr. 2004 Jun 30;116(11-12):407-8; author reply 408. doi: 10.1007/BF03040923.
- Eurythmy therapy in chronic disease: a four-year prospective cohort study. Hamre HJ, Witt CM, Glockmann A, Ziegler R, Willich SN, Kiene H.BMC Public Health. 2007 Apr 23;7:61. doi: 10.1186/1471-2458-7-61.
- Long-term outcomes of anthroposophic therapy for chronic low back pain: A two-year follow-up analysis. Hamre HJ, Witt CM, Kienle GS, Glockmann A, Ziegler R, Willich SN, Kiene H.J Pain Res. 2009 Jun 25;2:75-85. doi: 10.2147/jpr.s5922.
- Health costs in anthroposophic therapy users: a two-year prospective cohort study. Hamre HJ, Witt CM, Glockmann A, Ziegler R, Willich SN, Kiene H.BMC Health Serv Res. 2006 Jun 2;6:65. doi: 10.1186/1472-6963-6-65.
- Use and safety of anthroposophic medications in chronic disease: a 2-year prospective analysis. Hamre HJ, Witt CM, Glockmann A, Tröger W, Willich SN, Kiene H.Drug Saf. 2006;29(12):1173-89. doi: 10.2165/00002018-200629120-00008.
- Anthroposophic therapy for chronic depression: a four-year prospective cohort study. Hamre HJ, Witt CM, Glockmann A, Ziegler R, Willich SN, Kiene H.BMC Psychiatry. 2006 Dec 15;6:57. doi: 10.1186/1471-244X-6-57.
- Health costs in patients treated for depression, in patients with depressive symptoms treated for another chronic disorder, and in non-depressed patients: a two-year prospective cohort study in anthroposophic outpatient settings. Hamre HJ, Witt CM, Glockmann A, Ziegler R, Kienle GS, Willich SN, Kiene H.Eur J Health Econ. 2010 Feb;11(1):77-94. doi: 10.1007/s10198-009-0203-0.
- Outcome of anthroposophic medication therapy in chronic disease: a 12-month prospective cohort study. Hamre HJ, Witt CM, Glockmann A, Ziegler R, Kienle GS, Willich SN, Kiene H.Drug Des Devel Ther. 2009 Feb 6;2:25-37.
- Clinical research in anthroposophic medicine. Hamre HJ, Kiene H, Kienle GS.Altern Ther Health Med. 2009 Nov-Dec;15(6):52-5.
- Anthroposophic therapy for attention deficit hyperactivity: a two-year prospective study in outpatients. Hamre HJ, Witt CM, Kienle GS, Meinecke C, Glockmann A, Ziegler R, Willich SN, Kiene H.Int J Gen Med. 2010 Aug 30;3:239-53. doi: 10.2147/ijgm.s11725.
- Anthroposophic therapy for asthma: A two-year prospective cohort study in routine outpatient settings. Hamre HJ, Witt CM, Kienle GS, Schnürer C, Glockmann A, Ziegler R, Willich SN, Kiene H.J Asthma Allergy. 2009 Nov 24;2:111-28.
- Anthroposophic therapy for migraine: a two-year prospective cohort study in routine outpatient settings. Hamre HJ, Witt CM, Kienle GS, Glockmann A, Ziegler R, Rivoir A, Willich SN, Kiene H.Open Neurol J. 2010;4:100-10.
- Antibiotic Use in Children with Acute Respiratory or Ear Infections: Prospective Observational Comparison of Anthroposophic and Conventional Treatment under Routine Primary Care Conditions. Hamre HJ, Glockmann A, Schwarz R, Riley DS, Baars EW, Kiene H, Kienle GS.Evid Based Complement Alternat Med. 2014;2014:243801.
- An assessment of the scientific status of anthroposophic medicine, applying criteria from the philosophy of science. Baars EW, Kiene H, Kienle GS, Heusser P, Hamre HJ.Complement Ther Med. 2018 Oct;40:145-150.
- Anthroposophic vs. conventional therapy of acute respiratory and ear infections: a prospective outcomes study. Hamre HJ, Fischer M, Heger M, Riley D, Haidvogl M, Baars E, Bristol E, Evans M, Schwarz R, Kiene H.Wien Klin Wochenschr. 2005 Apr;117(7-8):256-68. doi: 10.1007/s00508-005-0344-9.
- Long-term outcomes of anthroposophic treatment for chronic disease: a four-year follow-up analysis of 1510 patients from a prospective observational study in routine outpatient settings. Hamre HJ, Kiene H, Glockmann A, Ziegler R, Kienle GS.BMC Res Notes. 2013 Jul 13;6:269. doi: 10.1186/1756-0500-6-269
- Eurythmy Therapy in anxiety. Kienle GS, Hampton Schwab J, Murphy JB, Andersson P, Lunde G, Kiene H, Hamre HJ.Altern Ther Health Med. 2011 Jul-Aug;17(4):56-63
- Mistletoe in cancer – a systematic review on controlled clinical trials. Kienle GS, Berrino F, Büssing A, Portalupi E, Rosenzweig S, Kiene H.Eur J Med Res. 2003 Mar 27;8(3):109-19.
- Anthroposophic therapy of respiratory and ear infections. Hamre HJ, Fischer M, Heger M, Riley D, Haidvogl M, Baars E, Bristol E, Evans M, Schwarz R, Kiene H.Wien Klin Wochenschr. 2005 Jul;117(13-14):500-1. doi: 10.1007/s00508-005-0389-9
- Complementary cancer therapy: a systematic review of prospective clinical trials on anthroposophic mistletoe extracts.
Eur J Med Res. 2007 Mar 26;12(3):103-19.
- Review article: Influence of Viscum album L (European mistletoe) extracts on quality of life in cancer patients: a systematic review of controlled clinical studies. Kienle GS, Kiene H.Integr Cancer Ther. 2010 Jun;9(2):142-57.
- [Anthroposophic medicine: health technology assessment report – short version].
Forsch Komplementmed. 2006;13 Suppl 2:7-18. doi: 10.1159/000093481. Epub 2006 Jun 26.
- Bilateral Asynchronous Renal Cell Carcinoma With Lung Metastases: A Case Report of a Patient Treated Solely With High-dose Intravenous and Subcutaneous Viscum album Extract for a Second Renal Lesion. Reynel M, Villegas Y, Kiene H, Werthmann PG, Kienle GS.Anticancer Res. 2019 Oct;39(10):5597-5604. doi: 10.21873/anticanres.13754.
- Long-term survival of a patient with an inoperable thymic neuroendocrine tumor stage IIIa under sole treatment with Viscum album extract: A CARE compliant clinical case report. Reynel M, Villegas Y, Werthmann PG, Kiene H, Kienle GS.Medicine (Baltimore). 2020 Jan;99(5):e18990. doi: 10.1097/MD.0000000000018990
- Long-Term Survival of a Patient with Recurrent Dedifferentiated High-Grade Liposarcoma of the Retroperitoneum Under Adjuvant Treatment with Viscum album L. Extract: A Case Report. Reynel M, Villegas Y, Werthmann PG, Kiene H, Kienle GS.Integr Cancer Ther. 2021 Jan-Dec;20:1534735421995258. doi: 10.1177/1534735421995258.
- Intralesional and subcutaneous application of Viscum album L. (European mistletoe) extract in cervical carcinoma in situ: A CARE compliant case report. Reynel M, Villegas Y, Kiene H, Werthmann PG, Kienle GS.Medicine (Baltimore). 2018 Nov;97(48):e13420.
- High-Dose Viscum album Extract Treatment in the Prevention of Recurrent Bladder Cancer: A Retrospective Case Series.
Perm J. 2015 Fall;19(4):76-83. doi: 10.7812/TPP/15-018.
- Disappearance of an advanced adenomatous colon polyp after intratumoural injection with Viscum album (European mistletoe) extract: a case report. von Schoen-Angerer T, Goyert A, Vagedes J, Kiene H, Merckens H, Kienle GS.J Gastrointestin Liver Dis. 2014 Dec;23(4):449-52. doi: 10.15403/jgld.2014.1121.234.acpy.
- Viscum Album in the Treatment of a Girl With Refractory Childhood Absence Epilepsy. von Schoen-Angerer T, Madeleyn R, Kienle G, Kiene H, Vagedes J.J Child Neurol. 2015 Jul;30(8):1048-52. doi: 10.1177/0883073814541473. Epub 2014 Jul 17.
- Improvement of Asthma and Gastroesophageal Reflux Disease With Oral Pulvis stomachicus cum Belladonna, a Combination of Matricaria recutita, Atropa belladonna, Bismuth, and Antimonite: A Pediatric Case Report. von Schoen-Angerer T, Madeleyn R, Kiene H, Kienle GS, Vagedes J.Glob Adv Health Med. 2016 Jan;5(1):107-11. doi: 10.7453/gahmj.2015.019. Epub 2016 Jan 1.
- Use of Iscador, an extract of European mistletoe (Viscum album), in cancer treatment: prospective nonrandomized and randomized matched-pair studies nested within a cohort study. Grossarth-Maticek R, Kiene H, Baumgartner SM, Ziegler R.Altern Ther Health Med. 2001 May-Jun;7(3):57-66, 68-72, 74-6 passim
WHAT A LIST!
It makes several things very clear to me:
- Kiene is a productive researcher
- He likes observational studies and case reports
- He dislikes the idea of rigorously testing a hypothesis
- He never publishes a negative finding about anthroposophical medicine
- He certainly deserves to be admitted to the ALTERNATIVE MEDICINE HALL OF FAME!
Welcome Helmut
The ‘University College of Osteopathy’ announced a proposal to merge with the AECC University College (AECC UC). Both institutions will seek to bring together the two specialist providers to offer a “unique inter-disciplinary environment for education, clinical practice and research in osteopathy, chiropractic, and across a wide range of allied health and related disciplines”.
The partnership is allegedly set to unlock significant opportunities for growth and development by bringing together the two specialist institutions’ expertise and resources across two locations – in Dorset and central London.
As a joint statement, Chair of the Board of Governors at AECC UC, Jeni Bremner and Chair of the Board of Governors at UCO, Professor Jo Price commented:
“We believe the proposed merger would further the institutional ambitions for both of our organisations and the related professional groups, by allowing us to expand our educational offering, grow student numbers and provide a unique inter-disciplinary training environment, providing students the opportunity to be immersed in multi-professional practice and research, with exposure to and participation in multi-disciplinary teams.
“There is also an exciting and compelling opportunity to expedite the development of a nationally unique, and internationally-leading MSK Centre of Excellence for Education and Research, developed and delivered across our two sites.”
The announcement is accompanied by further uncritical and promotional language:
Established as the first chiropractic training provider in Europe, AECC UC has been at the forefront of evidence-based chiropractic education, practice and research for more than 50 years. The institution is on an exciting journey of growth and development, having expanded and diversified its academic portfolio and activity beyond its traditional core offering of chiropractic across a broad range of allied health courses and apprenticeships, working closely with NHS, local authority and other system partners across Dorset and the south-west. The proposed merger with UCO would allow AECC UC to enhance the breadth and depth of its offer to support the expansion and development of the health and care workforce across a wider range of partners.
Now in its 106th year, UCO is one of the UK’s leading providers of osteopathic education and research with an established reputation for creating highly-skilled, evidence-informed graduates. UCO research is recognised as world-leading, delivering value to the osteopathic and wider health care community.
Sharon Potter, Acting Vice-Chancellor of UCO, said:
“As an institution that has long been at the forefront of osteopathic education and research, we are committed to ensuring further growth and development of the osteopathic profession.
“UCO has been proactively considering options to future-proof the institution. Following a review of strategic options, UCO is delighted by the proposed merger, working closely with AECC UC to ensure that UCO and osteopathy thrives as part of the inter-professional health sciences landscape, both academically and clinically. There is significant congruence between UCO and AECC UC in our strong aligned values, commitment to and delivery of excellent osteopathic education, clinical care and research, and opinion leadership.
“AECC UC has a strong track record of respecting the differences in professions, evidenced by the autonomy across the 10 different professional groups supported by the institution. The merger will not only mean we are protecting UCO through preserving its osteopathic heritage and creating a sustainable future, but that our staff and students can collaborate with other professional groups such as physiotherapy, chiropractic, sport rehabilitation, podiatry and diagnostic imaging, in a multidisciplinary MSK and rehabilitation environment unlike anywhere else in the UK.”
Professor Lesley Haig, Vice-Chancellor of AECC UC, commented:
“Preserving the heritage of UCO and safeguarding its future status as the flagship osteopathy training provider in the UK will be critical, just as it has been to protect the chiropractic heritage of the AECC brand. UCO is seen as synonymous with, and reflective of, the success of the osteopathy profession and we fully recognise and respect the important role that UCO plays not only as a sector-leading provider of osteopathic education, research and clinical care, but as the UK’s flagship osteopathy educational provider.
“Overall it is clear that UCO and AECC UC already have a common values base, similar understanding of approaches to academic and clinical delivery, and positive relationships upon which a future organisational structure and opportunities can be developed. It’s an exciting time for both institutions as we move forward in partnership to create something unique and become recognised nationally and internationally as a centre of excellence.”
The proposed merger would continue the already founded positive relations between the institutions, where regular visits, sharing of good practice, and collaborative research work are already taking place. Heads of terms for the potential merger have now been agreed and both institutions are entering into the next phase of discussions, which will include wide consultation with staff, students and other stakeholders to produce a comprehensive implementation plan.
__________________________________
In case this bonanza of platitudes and half-truths has not yet overwhelmed you, I might be so bold as to ask 10 critical questions:
- What is an “evidence-based chiropractic education”? Does it include the messages that 1) subluxation is nonsense, 2) chiropractic manipulations can cause harm, 3) there is little evidence that they do more good than harm?
- How an an “expansion and development of the health and care workforce” be anticipated on the basis of the 3 points I just made?
- What does the term “evidence-informed graduates” mean? Does it mean they are informed that you teach them nonsense but instruct them to practice this nonsense anyway?
- Do “options to future-proof the institution” include the continuation of misleading the public about the value of chiropractic/osteopathy?
- Does the”delivery of excellent osteopathic education, clinical care and research, and opinion leadership” account for the fact that the evidence for osteopathy is weak at best and for most conditions negative?
- By “preserving its osteopathic heritage”, do you intend to preserve also the reputation of your founding father, Andrew Taylor Still, who did many dubious things. In 1874, for instance, he was excommunicated by the Methodist Church because of his “laying on of hands”; specifically, he was accused of trying to emulate Jesus Christ, labelled an agent of the Devil, and condemned as practicing voodoo. Or do you prefer to white-wash the osteopathic heritage?
- You also want “to protect the chiropractic heritage”; does that mean you aim at white-washing the juicy biography of the charlatan who created chiropractic, DD Palmer, as well?
- “UCO and AECC UC already have a common values base” – what are they? As far as I can see, they mainly consist in hiding the truth about the uselessness of your activities from the public.
- How do you want to “recognised nationally and internationally as a centre of excellence”? Might it be a good idea to begin by critically assessing your interventions and ask whether they do more good than harm?
- Crucially, what is really behing the merger that you are trying to sell us with such concentrated BS?
Blood electrification? If you had not heard about it, you are in good company. What is it? The Internet has many columns on it. Here is an article that I abbreviated a bit for the purpose of this blog:
Dr. Robert C. Beck is the inventor of blood electrification, which can be traced back to the work of Dr. Hulda Clark and Dr. Robert J. Thiel. The method is based on the assumption that parasites, bacteria, viruses and fungi are paralyzed by a low current pulse of 50 to 100 microamperes. As a result, the pathogens are no longer able to infect the body and the immune system can readily eliminate.
Dr. Beck found that the current flow, i.e., blood electrification, is more important than the frequency. Unlike previous ‘zappers’, the “Beck-Zapper” works only with a frequency of 3.920 Hz. Beck believes that the lower the frequency, the greater the current absorption, i.e. the more effective the therapy. Moreover, the Beck zapper is in harmony with the body’s own rhythm and is therefore not a stress trigger. Since the Beck zapper works with a higher voltage (27 volts) than the Clark zapper (9 volts), it is attached directly to the pulse vein and not held in the hands. Here’s how the Beckzapper works:
- The “enemy in the blood,” as Beck called parasites, viruses and bacteria, is fought with mild electricity between 50 and 100 microamperes at half the Schumann frequency of 3.92 Hz, he said.
- During blood electrification, colloidal silver is added to prevent secondary infection. Colloidal silver is extremely small silver particles dissolved in water, which are held in suspension by the water molecules. Although collodial silver enjoyed great importance in medicine hundreds of years ago, it fell into oblivion due to the introduction of antiobiotics and has only been gradually rediscovered in recent years.
- Powerful magnetic pulses are said to carry pathogens from the lymphatic system back into the bloodstream, where they can then be eliminated by the immune system.
Beck was able to prove that his patients became virus-free and symptom-free after the exact application of the blood electrification device. However, he also found that some of his patients became ill again with the same virus after a few months. After further study, he realized that the repeated infections were due to lingering viruses in the lymph fluid. Starting from the lymph fluid, the viruses returned to the bloodstream, where they re-infected cells and multiplied, causing the repeated symptoms of the disease. Beck then invented another device, the so-called magnetic pulser.
This generated an electrical flow by means of a magnetic pulse, which triggered contractions in the lymphatic channels. This forced movement of the lymph, causing the microbes to be forced back into the bloodstream where they could be electrified. Beck applied the Magnetpluser to some patients in combination with the blood electrifier and obtained surprisingly positive results.
Dr. Beck assumed that parasites were responsible for the development of diseases. Beck also believed that parasites in the blood would limit human life expectancy to 70 to 80 years. Dr. Beck himself was convinced of the effectiveness of his zapper and lost 60 kg through it. He explained this weight loss by the fact that the parasites had previously consumed a large part of the nutrients, causing him to experience constant ravenous hunger. In addition, Beck’s blood pressure dropped significantly, as did his blood sugar. He also regained a full head of hair as an almost 70-year-old bald man. Beck attributed all these benefits to his zapper, which he was able to prove after a three-week treatment by means of a blood test using the dark field method: His blood count was perfect.
The blood zapper also helps with herpes diseases, AIDS, chicken pox, lung ulcers, leukemia and other types of cancer, as well as chronic fatigue syndrome, diabetes, flu-like infections, asthma and gastritis. In short, the blood zapper has been able to treat many diseases that are usually considered incurable.
Beck recommends performing blood electrification for two hours daily for 3 to 6 weeks, or longer if necessary.
- The Beckzapper can be carried in the breast pocket or on the belt.
- The cathode and anode are to be placed where on the one hand the blood flows and on the other hand the pulse beat can be felt.
- This can be, for example, on the wrist or feet.
- For the greatest possible freedom of movement during treatment, the “miniZAP” is recommended.
- This is a matchbox-sized zapper that can be worn comfortably on the wrist.
- The method of blood electrification can be performed by anyone. There are no known side effects when using the blood zapper.
Dr. Alfons Weber has presented research according to which most cancers are caused by excessive microbial infestation of blood cells. According to the findings of Prof. Pappa, this circumstance, in turn, can be attributed to a too low energy status. The use of electrotherapy can therefore achieve considerable success in the treatment of parasitic and energy-related cancers in particular.
- The use of the Beckzapper in cancer patients should be continuous
- According to Dr. Weber, the carcinoma protozoa are located in the blood cells and eat the hemoglobin here.
- The carcinoma protozoa located in the blood cells are first hardly affected by the increased current flow in the blood plasma.
- Only when the respective blood cell has been eaten empty do the carcinoma protozoa leave the blood cell in search of a new one.
- Once the carcinoma protozoa are outside the plasma, they can be eliminated by the continuous surge of the Beckzapper.
- In this way, new blood cells cannot be attacked in the first place.
The continuous application of the Beckzapper, possibly in combination with a magnetic pulse generator with collodial silver, can significantly reduce the number of protozoa.
Vis a vis so much nonsense, I am almost speechless. I did try to find any credible publications that might back up the multityde of claims made above. Neddless to say, I was not successful.
And what makes that anyone who promotes ‘blood electrification’ as a cure of anything?
The answer is easy:
A DANGEROUS CHARLATAN
It has been reported that a UK Conservative candidate for the next general election reportedly claimed she healed a man’s hearing through the power of prayer. Kristy Adams has been chosen to represent the Conservatives in Mid Sussex at the next general UK election, which is expected to take place in May or the autumn of next year. Mrs Adams previously stood as the Tory candidate in Hove in 2017, placing a distant second behind Labour MP Peter Kyle.
In a recording from 2010, the Conservative hopeful reportedly told the King’s Arms Church in Bedford how she healed a deaf man by placing her hands over his ears and saying: “Be healed in Jesus’s name”. Mrs Adams is reported to have said: “He had hearing aids in both ears and I just thought that wasn’t right. It just annoyed me. I said ‘can I pray for you?’ and his eyes lit up, which is unusual when you offer to pray for someone’s healing.” After removing her hands, she claims the man could hear without his hearing aids. “I don’t know if he was more surprised or me,” she reportedly said.
Speaking to The Argus during her 2017 election campaign, Mrs Adams said she had asked the Daily Mirror to remove a story about the alleged recording but refused to answer whether she believed non-scientific medical miracles can happen. She said: “Millions of Christians around the world pray every day to help people.”
- Daily prayer against severe COVID – an update of a study started two years ago
- Resolution of blindness after prayer?
- Prayer as a therapy: a new randomised study
- Prayer as a medical therapy? Time to stop this nonsense!
- When an undercover journalist tests alternative cancer healers
- Biblical Naturopathy, another SCAM that is new to me
- The ‘Association of Catholic Doctors’ and homeopathic conversion therapy
- Prof Harald Walach’s new ground breaking study of praying the Rosary
- Higher religiousness/spirituality is associated with a more frequent use of so-called alternative medicine (SCAM)
- ‘The power of all religions’ is being tested in a study with severely ill corona-virus patients
- Does religiosity influence post-operative survival?
- Daniel P Wirth, his dubious research, and the remarkable apathy of some medical journals
Suffice to say, perhaps, that the evidence for prayer as a therapy is not positive.
The ‘ALTERNATIVE MEDICINE HALL OF FAME’ is my creation amd is meant to honour reserchers who have dedicated much of their professional career to investigating a form of so-called alternative medicine (SCAM) without ever publishing negative conclusions about it. Obviously, if anyone studies any therapy, he/she will occasionally produce a negative finding. This would be the case, even if he/she tests an effective treatment. However, if the treatment in question comes from the realm of SCAM, one would expect negative results fairly regularly. No therapy works well under all conditions, and to the best of my knowledge, no SCAM is a panacea!
This is why researchers who defy this inevitability must be remarkable. If someone tests a treatment that is at best dubious and at worst bogus, we are bound to see some studies that are not positive. He/she would thus have a high or norma ‘TRUSTWORTHINESS INDEX‘ (another creation of mine which, I think, is fairly self-explanatory). Conversely, any researcher who does manage to publish nothing but positive results of a SCAM is bound to have a very low ‘TRUSTWORTHINESS INDEX‘. In other words, these people are special, so much so that I decided to honour such ‘geniuses’ by admitting them to my ALTERNATIVE MEDICINE OF FAME.
So far, this elite group of people comprises the following individuals:
- Tery Oleson (acupressure , US)
- Jorge Vas (acupuncture, Spain)
- Wane Jonas (homeopathy, US)
- Harald Walach (various SCAMs, Germany)
- Andreas Michalsen ( various SCAMs, Germany)
- Jennifer Jacobs (homeopath, US)
- Jenise Pellow (homeopath, South Africa)
- Adrian White (acupuncturist, UK)
- Michael Frass (homeopath, Austria)
- Jens Behnke (research officer, Germany)
- John Weeks (editor of JCAM, US)
- Deepak Chopra (entrepreneur, US)
- Cheryl Hawk (chiropractor, US)
- David Peters (osteopathy, homeopathy, UK)
- Nicola Robinson (TCM, UK)
- Peter Fisher (homeopathy, UK)
- Simon Mills (herbal medicine, UK)
- Gustav Dobos (various SCAMs, Germany)
- Claudia Witt (homeopathy, Germany/Switzerland)
- George Lewith (acupuncture, UK)
- John Licciardone (osteopathy, US)
Today, it is my great pleasure to admit another osteopath to the HALL OF FAME:
Helge Franke
Helge is a German Heilpraktiker and Osteopath. On his website, he lists his publications (kindly saving me the effort of doing a Medline search):
- Osteopathic manipulative treatment for nonspecific low back pain: a systematic review and meta-analysis. BMC Muskuloskeletal Disorders, 2014
- Effectiveness of osteopathc manipulative therapy for managing symptoms of irritable bowel syndrome: a systematic review. Journal of the American Osteopathic Association, 2014
- Why reservations remain: A critical reflection about the systematic review and meta-analysis “Osteopathic manipulative treatment for low back pain” by Licciardone et al. Journal of Bodywork & Movement Therapies, 2012, Elsevier
- Osteopathic Manipulative Treatment (OMT) for Lower Urinary Tract Symptoms (LUTS) in Women. A Systematic Review and Meta-analyses. Journal of Bodywork & Movement Therapies, 2012, Elsevier
- Comment: Is a postural-structural-biomechanical model, within manual therapy, viable? A JBMT debate. Journal of Bodywork & Movement Therapies (2011) 15, 259-261, Elsevier
- Die manuelle Behandlung des Kniegelenks – veraltetes Verfahren oder alternative Option? Naturheilpraxis mit Naturmedizin 9-2010, 1019-1026, Pflaum Verlag
- CRPS und Osteopathie – Grenzen und Möglichkeiten DO – Deutsche Zeitschrift für Osteopathie 3-2010, 6-8, Hippokrates Verlag
- Research and osteopathy: An interview with Dr Gary Fryer by Journal of Bodywork & Movement Therapies. 14, 304-308, Elsevier
- „…there is not much we can say without any doubt“ DO Life about Gary Fryer DO – Deutsche Zeitschrift für Osteopathie 1-2010, 4-5, Hippokrates Verlag
- Fred Mitchell und die Entwicklung der Muskel-Energie-Techniken DO – Deutsche Zeitschrift für Osteopathie 2-2009, 4-5, Hippokrates Verlag
- A randomized trial of arthroscopic surgery for osteoarthritis of the knee. Commentary Forschende Komplementärmedizin 2008 Dec 15(6), 354-5, Karger
- Evidence-informed management of chronic low back pain with spinal manipulation and mobilization. Commentary Forschende Komplementärmedizin 2008 Dec 15(6), 353-4, Karger
- Interview mit Prof. Eyal Lederman Teil 1 Osteopathische Medizin, 2/2007, S.15-21, Elsevier
- Interview mit Prof. Eyal Lederman Teil 2 Osteopathische Medizin, 3/2007, S.22-27, Elsevier
- Artikel über das 3. Internationale Symposium über die Fortschritte in der osteopathischen Forschung. Osteopathische Medizin, 1-2007, S.23-24, Elsevier
- Die richtige Haltung des Behandlers Osteopathische Medizin, 4-2006, S.8-10, Elsevier
- Interview mit Laurie Hartman Osteopathische Medizin, 4-2006, S. 11-16, Elsevier
- Herausgeber des Sonderheftes „Functional Technique” Osteopathische Medizin, 2-2006, Elsevier
- Harold Hoover, Charles Bowles, William Johnston und die Geschichte der Funktionellen Technik Osteopathische Medizin, 2-2006, S.4-12, Elsevier
- Interview mit Harry Friedman Osteopathische Medizin, 2-2006, S.25-30, Elsevier
- Funktionelle Technik – Praxis Osteopathische Medizin, 2-2006, S.17-23, Elsevier
- Osteopathische Diagnose und Behandlung des Hüftgelenks Naturheilpraxis mit Naturmedizin, 10-2006, S.1383-1393, Pflaum-Verlag
- Bericht über das 2-Tage Seminar von Prof. Laurie Hartman in München Naturheilpraxis mit Naturmedizin, 5-2006, S.754-755, Pflaum Verlag
- Bewusstsein für Bewegung. Die minimale Hebeltechnik und das Behandlungskonzept von Laurie Hartman Osteopathische Medizin, 4-2006, S.4-7, Elsevier
- ICAOR 6 / Interview mit Florian Schwerla Osteopathische Medizin, 3-2006, S.15-17, Elsevier
- Muscle Energy Technique – Geschichte, Modell und Wirksamkeit Teil 1 Geschichte Osteopathische Medizin 2-2005, S.4-10, Elsevier
- Muscle Energy Technique – Geschichte, Modell und Wirksamkeit Teil 2 Modell Osteopathische Medizin 3-2005, S.4-10, Elsevier
- Muscle Energy Technique – Geschichte, Modell und Wirksamkeit Teil 3 Wirksamkeit Osteopathische Medizin 4-2005, S.4-10, Elsevier
- Die Behandlung der Rippen mit Muskel-Energie-Techniken Naturheilpraxis mit Naturmedizin, 10-2005, S. 1353-1359, Pflaum Verlag
Yes, I agree! The list is confusing because it contains all sorts of papers, including even interviews. Let’s do a Medline search after all and find the actual studies published by Franke:
- Osteopathic manipulative treatment (OMT) for lower urinary tract symptoms (LUTS) in women. Franke H, Hoesele K.J Bodyw Mov Ther. 2013 Jan;17(1):11-8. doi: 10.1016/j.jbmt.2012.05.001. Epub 2012 Jun 17.
- Effectiveness of osteopathic manipulative treatment for pediatric conditions: A systematic review. Franke H, Franke JD, Fryer G.J Bodyw Mov Ther. 2022 Jul;31:113-133. doi: 10.1016/j.jbmt.2022.03.013. Epub 2022 Mar 24.
- Muscle energy technique for non-specific low-back pain. Franke H, Fryer G, Ostelo RW, Kamper SJ. Cochrane Database Syst Rev. 2015 Feb 27;(2):CD009852. doi: 10.1002/14651858.CD009852.pub2.
-
Osteopathic manipulative treatment for nonspecific low back pain: a systematic review and meta-analysis. Franke H, Franke JD, Fryer G.BMC Musculoskelet Disord. 2014 Aug 30;15:286. doi: 10.1186/1471-2474-15-286.Effectiveness of osteopathic manipulative therapy for managing symptoms of irritable bowel syndrome: a systematic review. Müller A, Franke H, Resch KL, Fryer G.J Am Osteopath Assoc. 2014 Jun;114(6):470-9. doi: 10.7556/jaoa.2014.098.
- Osteopathic manipulative treatment for low back and pelvic girdle pain during and after pregnancy: A systematic review and meta-analysis. Franke H, Franke JD, Belz S, Fryer G.J Bodyw Mov Ther. 2017 Oct;21(4):752-762. doi: 10.1016/j.jbmt.2017.05.014. Epub 2017 May 31.
- Evidence-informed management of chronic low back pain with spinal manipulation and mobilization Franke H.Forsch Komplementmed. 2008 Dec;15(6):353-4
- Osteopathic manipulative treatment for chronic nonspecific neck pain: A systematic review and meta-analysis Helge Franke, Jan-David Franke, Gary Fryer, 2015 Int J Osteop Med.
Not a huge list, I agree. Yet it is respectable, particularly if we consider that Franke managed to squeeze out a little positive message even from cases where the data are fairly clearly negative. Another thing that I find noteworthy is the fact that Franke, as far as I can see, never published a clinical trial. He seems to specialize in reviews – and perhaps that is understandable: if one is compelled to spinning the message from fairly negative evidence to a positive conclusion, reviews might be better suited.
Altogether, I think Helge Franke deserves his place in the ALTERNATIVE MEDICINE HALL OF FAME!
Joe Dispenza is not all that well known in Europe but, in the US, he is all the rage as a health guru. Despite pretending to be a top (neuro)scientist and expert of quantum physics, Dispenza has, as far as I can see, just three Medline-listed papers to his credit. Here are their abstracts:
No 1 is entitled “Meditation-induced bloodborne factors as an adjuvant treatment to COVID-19 disease”
The COVID-19 pandemic has resulted in significant morbidity and mortality worldwide. Management of the pandemic has relied mainly on SARS-CoV-2 vaccines, while alternative approaches such as meditation, shown to improve immunity, have been largely unexplored. Here, we probe the relationship between meditation and COVID-19 disease and directly test the impact of meditation on the induction of a blood environment that modulates viral infection. We found a significant inverse correlation between length of meditation practice and SARS-CoV-2 infection as well as accelerated resolution of symptomology of those infected. A meditation “dosing” effect was also observed. In cultured human lung cells, blood from experienced meditators induced factors that prevented entry of pseudotyped viruses for SARS-CoV-2 spike protein of both the wild-type Wuhan-1 virus and the Delta variant. We identified and validated SERPINA5, a serine protease inhibitor, as one possible protein factor in the blood of meditators that is necessary and sufficient for limiting pseudovirus entry into cells. In summary, we conclude that meditation can enhance resiliency to viral infection and may serve as a possible adjuvant therapy in the management of the COVID-19 pandemic.
No 2 is entitled “The Mathematical Characterization of the Complexity Matching during a Healing Circle Meditation”
The aim of the study is to evaluate the complexity matching between the HRVs of the group of Healers and the Healee during the various stages of the meditation protocol by employing a novel mathematical approach based on the H-rank algorithm. The complexity matching of heart rate variability is assessed before and during a heart-focused meditation in a close non-contact healing exercise. The experiment was conducted on a group of individuals (eight Healers and one Healee) throughout the various phases of the protocol over a ~75-minute period. The HRV signal for the cohort of individuals was recorded using high resolution HRV recorders with internal clocks for time synchronization. The Hankel transform (H-rank) approach was employed to reconstruct the real-world complex time series in order to measure the algebraic complexity of the heart rate variability and to assess the complexity matching between the reconstructed H-rank of the Healers and Healee during the different phases of the protocol. The integration of the embedding attractor technique was used to aid in the visualization of reconstructed H-rank in state space across the various phases. The findings demonstrate the changes in the degree of reconstructed H-rank (between the Healers and the Healee) during the heart-focused meditation healing phase by employing mathematically anticipated and validated algorithms. It is natural and thought-provoking to contemplate the mechanisms causing the complexity of the reconstructed H-rank to come closer; it can be explicitly stated that the purpose of the study is to communicate a clear idea that the H-rank algorithm is capable of registering subtle changes in the healing process, and that there was no intention of delving deep to uncover the mechanisms involved in the HRV matching. Therefore, the latter might be a distinct goal of future research.
No 3 is entitled “Large effects of brief meditation intervention on EEG spectra in meditation novices”
This study investigated the impact of a brief meditation workshop on a sample of 223 novice meditators. Participants attended a three-day workshop comprising daily guided seated meditation sessions using music without vocals that focused on various emotional states and intentions (open focus). Based on the theory of integrative consciousness, it was hypothesized that altered states of consciousness would be experienced by participants during the meditation intervention as assessed using electroencephalogram (EEG). Brainwave power bands patterns were measured throughout the meditation training workshop, producing a total of 5616 EEG scans. Changes in conscious states were analysed using pre-meditation and post-meditation session measures of delta through to gamma oscillations. Results suggested the meditation intervention had large varying effects on EEG spectra (up to 50 % increase and 24 % decrease), and the speed of change from pre-meditation to post-meditation state of the EEG co-spectra was significant (with 0.76 probability of entering end-meditation state within the first minute). There was a main 5 % decrease in delta power (95 % HDI = [-0.07, -0.03]); a global increase in theta power of 29 % (95 % HDI = [0.27, 0.33]); a global increase of 16 % (95 % HDI = [0.13, 0.19]) in alpha power; a main effect of condition, with global beta power increasing by 17 % (95 % HDI = [0.15, 0.19]); and an 11 % increase (95 % HDI = [0.08, 0.14]) in gamma power from pre-meditation to end-meditation. Findings provided preliminary support for brief meditation in altering states of consciousness in novice meditators. Future clinical examination of meditation was recommended as an intervention for mental health conditions particularly associated with hippocampal impairments.
Unimpressed?
Me too!
It seems noteworthy that none of these articles support any of the many outlandish therapeutic claims Dispenza makes. In these papers, Dispenza give his affiliation as “Encephalon, LLC, Rainier, WA”. My seraches for this institution led me to the website of Dispenza’s company that tries to sell you all sorts of strange stuff and bombards you with irritating platitudes about spirituality and related subjects. Here you will also find several of Dispenza’s books. Naturally, they were big successes. The latest volume is called ‘Becoming Supernatural‘. Its topics include:
- Demystifying the body’s seven energy centers and how you can balance them to heal
- How to free yourself from the past by reconditioning your body to a new mind
- How you can create reality in the generous present moment by changing your energy
- The difference between third-dimension creation and fifth-dimension creation
- The secret science of the pineal gland and its role in accessing mystical realms of reality
- The distinction between space-time vs. time-space realities
By now, I am beginning to suspect that “Dr. Joe”, as he likes to wrongly depict himself, is an 18 carrat bullshitter, and I feel like learning more about him and his incredible popularity.
So, who is Joe Dispenza?
Dispenza trained as a chiropractor and, in 1986, he had a cycling accident that left him with six compressed vertebrae – at least that is what he likes to tell journalists. Allegedly, doctors told him he might never walk again and recommended spine surgery. But he knew better, checked himself out of the hospital, and reconstructed his vertebrae with his mind. Within 10 weeks he was walking again. “I made a deal with myself that if I was ever able to walk again I would spend the rest of my life studying the mind-body connection,” he claimed in a 2018 interview. If you don’t know about vertebral compression fractures, this sounds like an unusal recovery. If you, however, know about such injuries, the course of events is not abnormal.
Ever since, Dispenza uses his mind to heal others. His website contains ~40 testimonials of people claiming he cured their cancer or their multiple sclerosis or their infertility. Under the heading of “coherence healing,” the site boasts Dispenza and his disciples have “produced profound biological changes in multitudes of individuals around the world” and “observed hundreds of healings from a wide variety of health conditions.” In a 2020 interview Dispenza bragged about bringing children onstage at his retreats to cure them of “really serious health conditions.” He claimed to have cured a 76-year-old woman of Parkinson’s. He said his treatments cured illness faster than chemotherapy and that “profound and prestigious universities” in the United States wanted to study his methods. “[We’ve seen] tumors disappearing, people stepping out of wheelchairs, blind people seeing, deaf people hearing—crazy stuff,” he stated. “This is biblical proportions stuff.”
Dispenza likes to present himself as a scientist. “Learning” becomes “forging new synaptic connections” and changing one’s behavior becomes “reorganizing circuits.” He claims that meditating in the presence of others—combining “coherent fields,” as he calls this—opens up “interference patterns of fractal geometry that are doors to dimensions.” During performances, he occasionally brings followers on stage to share the “miracles” they experienced at the workshops that day, such as a woman who claimed she regained her depth perception after decades of encephalitis. “She got a biological upgrade … and all she did was make up her mind to do it,” he told the audience.
Back in 2012, I published a post entitled “How to become a charlatan” where I provide several practical instructions for all who intend to persue this career:
1. Find an attractive therapy and give it a fantastic name
Did I just say “straight forward”? Well, the first step isn’t that easy, after all. Most of the really loony ideas turn out to be taken: ear candles, homeopathy, aura massage, energy healing, urine-therapy, chiropractic etc. As a true charlatan, you want your very own quackery. So you will have to think of a new concept.
Something truly ‘far out’ would be ideal, like claiming the ear is a map of the human body which allows you to treat all diseases by doing something odd on specific areas of the ear – oops, this territory is already occupied by the ear acupuncture brigade. How about postulating that you have super-natural powers which enable you to send ‘healing energy’ into patients’ bodies so that they can repair themselves? No good either: Reiki-healers might accuse you of plagiarism.
But you get the gist, I am sure, and will be able to invent something. When you do, give it a memorable name, the name can make or break your new venture.
2. Invent a fascinating history
Having identified your treatment and a fantastic name for it, you now need a good story to explain how it all came about. This task is not all that tough and might even turn out to be fun; you could think of something touching like you cured your moribund little sister at the age of 6 with your intervention, or you received the inspiration in your dreams from an old aunt who had just died, or perhaps you want to create some religious connection [have you ever visited Lourdes?]. There are no limits to your imagination; just make sure the story is gripping – one day, they might make a movie of it.
3. Add a dash of pseudo-science
Like it or not, but we live in an age where we cannot entirely exclude science from our considerations. At the very minimum, I recommend a little smattering of sciency terminology. As you don’t want to be found out, select something that only few experts understand; quantum physics, entanglement, chaos-theory and Nano-technology are all excellent options.
It might also look more convincing to hint at the notion that top scientists adore your concepts, or that whole teams from universities in distant places are working on the underlying mechanisms, or that the Nobel committee has recently been alerted etc. If at all possible, add a bit of high tech to your new invention; some shiny new apparatus with flashing lights and digital displays might be just the ticket. The apparatus can be otherwise empty – as long as it looks impressive, all is fine.
4. Do not forget a dose of ancient wisdom
With all this science – sorry, pseudo-science – you must not forget to remain firmly grounded in tradition. Your treatment ought to be based on ancient wisdom which you have rediscovered, modified and perfected. I recommend mentioning that some of the oldest cultures of the planet have already been aware of the main pillars on which your invention today proudly stands. Anything that is that old has stood the test of time which is to say, your treatment is both effective and safe.
5. Claim to have a panacea
To maximise your income, you want to have as many customers as possible. It would therefore be unwise to focus your endeavours on just one or two conditions. Commercially, it is much better to affirm in no uncertain terms that your treatment is a cure for everything, a panacea. Do not worry about the implausibility of such a claim. In the realm of quackery, it is perfectly acceptable, even common behaviour to be outlandish.
6. Deal with the ‘evidence-problem’ and the nasty sceptics
It is depressing, I know, but even the most exceptionally gifted charlatan is bound to attract doubters. Sceptics will sooner or later ask you for evidence; in fact, they are obsessed by it. But do not panic – this is by no means as threatening as it appears. The obvious solution is to provide testimonial after testimonial.
You need a website where satisfied customers report impressive stories how your treatment saved their lives. In case you do not know such customers, invent them; in the realm of quackery, there is a time-honoured tradition of writing your own testimonials. Nobody will be able to tell!
7. Demonstrate that you master the fine art of cheating with statistics
Some of the sceptics might not be impressed, and when they start criticising your ‘evidence’, you might need to go the extra mile. Providing statistics is a very good way of keeping them at bay, at least for a while. The general consensus amongst charlatans is that about 70% of their patients experience remarkable benefit from whatever placebo they throw at them. So, my advice is to do a little better and cite a case series of at least 5000 patients of whom 76.5 % showed significant improvements.
What? You don’t have such case series? Don’t be daft, be inventive!
8. Score points with Big Pharma
You must be aware who your (future) customers are (will be): they are affluent, had a decent education (evidently without much success), and are middle-aged, gullible and deeply alternative. Think of Prince Charles! Once you have empathised with this mind-set, it is obvious that you can profitably plug into the persecution complex which haunts these people.
An easy way of achieving this is to claim that Big Pharma has got wind of your innovation, is positively frightened of losing millions, and is thus doing all they can to supress it. Not only will this give you street cred with the lunatic fringe of society, it also provides a perfect explanation why your ground-breaking discovery has not been published it the top journals of medicine: the editors are all in the pocket of Big Pharma, of course.
9. Ask for money, much money
I have left the most important bit for the end; remember: your aim is to get rich! So, charge high fees, even extravagantly high ones. If your treatment is a product that you can sell (e.g. via the internet, to escape the regulators), sell it dearly; if it is a hands-on therapy, charge heavy consultation fees and claim exclusivity; if it is a teachable technique, start training other therapists at high fees and ask a franchise-cut of their future earnings.
Over-charging is your best chance of getting famous – or have you ever heard of a charlatan famous for being reasonably priced? It will also get rid of the riff-raff you don’t want to see in your surgery. Poor people might be even ill! No, you don’t want them; you want the ‘worried rich and well’ who can afford to see a real doctor when things should go wrong. But most importantly, high fees will do a lot of good to your bank account.
Could it be that Joe Dispenza is the most successful pupil of my crash-course in charlatanism?
PS
I have been asked by the NY Post to answer a few questions about Dispenza. Allow me to present them to you here:
What makes Dispenza so dangerous (his advice, obsession with manifesting, etc.)?
Dispenza is at his most dangerous firstly when he implies that he can cure serious illness. In this way, he can cause the premature death of many patients. Secondly, he systematically undermines rational thinking which inevitably will cause significant harm to the already badly damaged US society. As Voltaire once pointed out: those who make you believe in absurdities can make you commit atrocities.
Why, in your opinion, has he amassed a cult-like following?
In 2012 I published a satirical piece entitled ‘How to become a charlatan’ (How to become a charlatan (edzardernst.com)). It seems to me that Dispenza followed my instructions to the letter providing a masterclass on fooling the public. He is a textbook example of a charismatic pseudoscientist (e.g.: I am a “researcher of epigenetics, quantum physics & neuroscience“) touting pure bullshit (e.g.: “new science is emerging that empowers all human beings to create the reality they choose”). He may be a charlatan but he is very good at it, runs a highly sophisticated campaign, and is laughing all the way to the bank.
For readers who find themselves enamored by Dispenza, what advice would you give them?
My advise is to take a step back and do a reality check: ‘Dr.Joe’ is not a medical doctor or neuroscientist but a chiropractor. He does not understand quantum physics. He has not published any meaningful scientific studies. His proclamations are nothing but platitudes or empty phrases. My advice also is to ask yourself: are you sure you are not the victim of your own gullibility?
We have discussed the Miracle Mineral Solution (MMS) before. Now it has been making headlines again. It has been reported that a Miami federal jury convicted a father and his three sons of selling a toxic bleach solution as a “miracle” medical cure out of a fake Florida church’s website to thousands of consumers across the US. Mark Grenon, 65, and sons Jonathan, 37, Joseph, 35, and Jordan, 29, chose to represent themselves in their two-day trial in Miami federal court. But they said nothing during the trial as if they were silently protesting the proceeding. Only after the 12-person jury hit them with a quick verdict did one of the Grenons speak up. “We will be appealing,” Joseph Grenon said.
During the trial and closing arguments, prosecutors portrayed the four defendants as con men who used a phony religious front on a website, the Genesis II Church of Health and Healing, to sell $1 million worth of their “Miracle Mineral Solution” a cure for 95% of the world’s known diseases, from AIDS to the coronavirus. “This whole Miracle Mineral Solution scheme was built on deception and dishonesty,” the prosecutor said during his closing argument, telling jurors that the Grenons “created a fake church to make it harder for the Food and Drug Administration and government to stop them from selling snake oil.” But, “this was no church,” he argued. “This was a scam for money — an old-fashioned scam.” The jury found the four defendants — all wearing beige inmate uniforms, ponytails, and flowing beards — guilty of conspiring to defraud the U.S. government and FDA, which regulates the food and drug industry, by distributing an unapproved and misbranded drug, Miracle Mineral Solution (MMS). That conviction carries up to five years in prison.
During the trial, the prosecutor said the Grenons called themselves “bishops” and peddled MMS as “sacraments” to consumers in South Florida and other parts of the US in exchange for a “donation” to the Genesis church, before the FDA cracked down on the family in 2020.
The Grenons were charged that April with conspiring to defraud the U.S. government after the outbreak of the COVID-19 pandemic when they defied FDA and court orders to stop distributing the toxic MMS substance. Their criminal case was the first pandemic-related enforcement action in Florida. In public warnings, FDA said it received several reports of hospitalizations and life-threatening conditions as people drank the dangerous substance.
MMS is a chemical solution containing sodium chlorite that, when mixed with water and a citric acid “activator,” turns into chlorine dioxide, a powerful bleach typically used for industrial water treatment or bleaching textiles, pulp, and paper. During the trial, a FDA agent testified about three Grenon-produced videos that pitched the solution as a cure for cancer, lung cancer, and COVID-19, among other deadly diseases. “We are trying to create a world without disease,” Mark Grenon said in one video, pitching the MMS substance. “It’s been proven to be tremendously effective in curing cancer.” Another video, dated March 8, 2020, was titled: “The coronavirus is curable. Do you believe it? You better!”
Prosecutors said the Grenon family’s religious front, the Genesis II Church of Health and Healing, sold tens of thousands of MMS orders in violation of federal law since 2010. It was in that year that Mark Grenon claims to have founded the organization with a man named Jim Humble in a plan to avoid governmental regulation and arrest as they promoted MMS as a miracle cure. Humble, a man who has dabbled in Scientology and professed to be a billion-year-old god, began promoting the substance as early as 2006 in self-published works after he claimed to have discovered its medical properties while on a gold-mining expedition in South America. After Humble supposedly stepped away from the organization in 2017, Grenon continued to manufacture, promote and sell MMS with his three sons.
The Grenons’ open defiance of a court order ultimately led to criminal charges and a federal raid on the family’s Bradenton home, where federal investigators say they found loaded guns, nearly 10,000 pounds of sodium chlorite powder, and thousands of bottles of MMS.
In response to yesterday’s post, I received a lengthy comment from ‘Stan’. Several readers have already commented on it. Therefore, I can make my arguments short. In this post, will repeat Stan’s points each followed by my comments (in bold). Here we go:
Seven Reasons Homœopathy is Not Placebo Effect
Sorry, Stan, but your heading is not proper English; I have therefore changed it for the title of this post.
1. Homeopathic remedies work on babies, animals, plants and people in a coma. Biodynamic farmers use homeopathic remedies to repel pests and treat plant diseases. Some organic ranchers rely on homeopathic remedies to treat their herds. Some “placebo by proxy” effect has been shown for children but its doubtful that it could be shown for a herd of cattle or crops in a field. Farmers can’t rely on wishful thinking to stay in business.
As discussed ad nauseam on this blog, homeopathic remedies do not work on babies or animals better than placebos. I don’t know of any studies with “people in a coma” (if you do, Stan, please let me know). The fact that ranchers rely on homeopathy is hilarious but does not prove anything.
2. The correct curative remedy will initially cause a worsening of the condition being cured if it is given in too strong (i.e. too dilute) a dose. A placebo might only cause a temporary improvement of the condition being treated; certainly not an aggravation.
The ‘homeopathic aggravation’ is a myth created by homeopaths. It disappears if we try to systematically research it; see here, for instance.
3. One can do a “proving” of an unknown homeopathic remedy by taking it repeatedly over several days and it will temporarily cause symptoms that one has never experienced previously – symptoms it will cure in a sick person. This is a repeatable scientific experiment used to determine the scope of a new remedy, or confirm the effects of an already proven remedy. A placebo might possibly have an effect if the individual taking it has been “prepared” by being told what they are taking but it likely wouldnt match previously recorded symptoms in the literature.
Homeopathic provings are rubbish and not reproducible when done rigorously; see here.
4. One can treat simple acute (self-limiting) conditions (e.g. minor burns, minor injuries, insect bites, etc.) and see unusually rapid cures with homeopathic remedies. A placebo might only cause a temporary improvement of the condition being treated while taken. Placebos have been found mostly effective in conditions with a strong psychological component like pain.
You mean like using Arnica for cuts and bruises? Sadly, it does not work.
5. One can get homeopathic treatment for long term chronic (non self-limiting) conditions and see a deep lasting cure, as has been documented clinically for a couple centuries. A placebo might only cause a temporary partial improvement of the condition being treated while the placebo is being taken.
You mean like asthma, eczema, or insomnia?
6. There is over 200 years worth of extensive documentation from around the world, of the clinical successes of homeopathy for both acute and chronic conditions of all types. As Dr Hahn has said you have throw out 90% of the evidence to conclude that homeopathy doesnt work. The Sheng et al meta-analysis in 2005 Lancet that was supposedly the death knell of homeopathy used only 8 studies, excluding hundreds of others. Unsurprisingly homeopathy was found wanting. So-called Skeptics see what they want to see in the science. There is relatively little documentation of placebo usage. A few recent studies have been done showing the limited temporary benefits of placebos.
What Hahn wrote is understandably liked by homeopaths but it nevertheless is BS. If you don’t trust me, please rely on independent bodies from across the world.
7. Homeopathic remedies have been shown to have a very weak electromagnetic signature and contain some nano-particles. Some believe this explains their mechanism. An exciting new potential field of research is the subtle cell signalling that has been found to direct the development of stem cells. Scientists have created double-headed planeria worms and this trait has been found to be inherited by their offspring without any change in the genes or epigenetics. Until now we had no idea how a single fertilized ovum could evolve into a complex creature that is bilateral and has multiple cell types. It is possible that the very subtle electromagnetic signature or some other unknown effect of homeopathic remedies is effecting this subtle cell signalling.
The homeopathic nano-myth is nonsense. And so is the rest of your assumptions.
Every conventional drug has “side effects” that match the symptoms for which it is indicated! Aspirin can cause headaches and fever, ritalin can cause hyperactive effects, radiation can cause cancer. Conventional doctors are just practicing bad homeopathy. They are prescribing Partially similar medicines. If their drugs were homeopathic (i.e. similar) to the patients symptoms on all levels they would be curative. Radiation sometimes does cure cancer instead of just suppressing it per usual.
Even if this were true, what would it prove? Certainly not that homeopathy works!
Dr Hahneman did forbid mixing homeopathy and conventional medicine. In his day doctors commonly used extensive blood letting and extreme doses of mercury. Its not Quite as bad now.
You evidently did not read Hahnemann’s writings.
Just because we dont know how extremely dilute homeopathic remedies work, doesn’t discount that they Do work. Homeopathy seems to fly in the face of Known science. In no way is it irrational or unscientific. There are lots of phenomena in the universe that cant be explained yet, like dark energy and dark matter effects and even consciousness!
Not knowing how a treatment works has not stopped science to test whether it works (e.g. Aspirin). In the case of homeopathy, the results of these endeavors were not positive.
The assumption that the moon is made of cheese also flies in the face of science; do you perhaps think that this makes it true?
The actions of homeopathy can and have been well-explained: they are due to placebo effects.
________________________
Stan, thank you for this entertaining exercise. But, next time, please remember to supply evidence for your statements.
There are debates in acupuncture-related systematic reviews and meta-analyses on whether searching Chinese databases to get more Chinese-language studies may increase the risk of bias and overestimate the effect size, and whether the treatment effects of acupuncture differ between Chinese and non-Chinese populations.
For this meta-epidemiological study, a team of investigators searched the Cochrane Library from its inception until December 2021, and identified systematic reviews and meta-analyses with acupuncture as one of the interventions. Paired reviewers independently screened the reviews and extracted the information. They repeated the meta-analysis of the selected outcomes to separately pool the results of Chinese- and non-Chinese-language acupuncture studies and presented the pooled estimates as odds ratios (OR) with 95% confidence interval (CI). They calculated the Ratio of ORs (ROR) by dividing the OR of the Chinese-language trials by the OR of the non-Chinese-language trials, and the ROR by dividing the OR of trials addressing Chinese population by the OR of trials addressing non-Chinese population. The researchers thus explored whether the impact of a high risk of bias on the effect size differed between studies published in Chinese- and in non-Chinese-language, and whether the treatment effects of acupuncture differed between Chinese and non-Chinese populations.
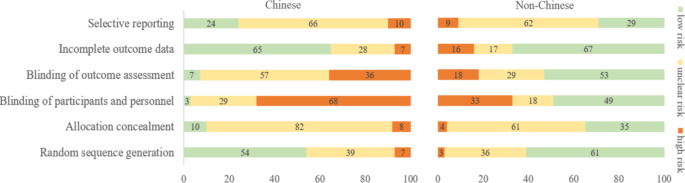
The researchers identified 84 Cochrane acupuncture reviews involving 33 Cochrane groups, of which 31 reviews (37%) searched Chinese databases. Searching versus not searching Chinese databases significantly increased the contribution of Chinese-language literature both to the total number of included trials (54% vs. 15%) and the sample size (40% vs. 15%). When compared with non-Chinese-language trials, Chinese-language trials were associated with a larger effect size (pooled ROR 0.51, 95% CI 0.29 to 0.91). The researchers also observed a higher risk of bias in Chinese-language trials in blinding of participants and personnel (97% vs. 51%) and blinding of outcome assessment (93% vs. 47%). The higher risk of bias was associated with a larger effect estimate in both Chinese language (allocation concealment: high/unclear risk vs. low risk, ROR 0.43, 95% CI 0.21 to 0.87) and non-Chinese-language studies (blinding of participants and personnel: high/unclear risk vs. low risk, ROR 0.41, 95% CI 0.23 to 0.74). However, the team found no evidence that the higher risk of bias would increase the effect size of acupuncture in Chinese-language studies more often than in non-Chinese-language studies (the confidence intervals of all ROR in the high-risk group included 1, Table 3). The researchers further found acupuncture appeared to be more effective in Chinese than in non-Chinese populations.

The authors concluded that the findings of this study suggest the higher risk of bias may lead to an overestimation of the treatment effects of acupuncture but would not increase the treatment effects in Chinese-language studies more often than in other language studies. The difference in treatment effects of acupuncture was probably associated with differences in population characteristics.
The authors discuss that, although searching Chinese databases can substantially increase the number of eligible studies and sample size in acupuncture reviews, the potentially higher risk of bias is an argument that needs to be considered in the inclusion of Chinese-language studies. Patients, investigators, and guideline panels should be cautious when adopting evidence from acupuncture reviews where studies with a high risk of bias contributed with a high weight to the meta-analysis.
The authors observed larger treatment effects of acupuncture in Chinese-language studies than in studies published in other languages. Although the treatment effects of acupuncture tended to be greater in studies with a high risk of bias, this potential overestimation did not differ between studies published in Chinese and in other languages. In other words, the larger treatment effects in Chinese-language studies cannot be explained by a high risk of bias. Furthermore, our study found acupuncture to be more effective in Chinese populations than in other populations, which could at least partly explain the larger treatment effects observed in Chinese-language studies.
I feel that this analysis obfuscates more than it clarifies. As we have discussed often here, acupuncture studies by Chinese researchers (regardless of what language they are published in) hardly ever report negative results, and their findings are often fabricated. It, therefore, is not surprising that their effect sizes are larger than those of other trials.
The only sensible conclusion from this messy and regrettable situation, in my view, is to be very cautious and exclude them from systematic reviews.