fallacy
After all these years, I am still fascinated by what proponents of homeopathy try to tell others about their trade. Recently I found a long article in this vein. It is aimed at an audience of HEILPRAKTIKER and their patients. It should therefore be responsible, thorough, and evidence-based (yes, I am an optimist).
“With this article”, the authors state, “we aim to provide a comprehensive overview of homeopathy and help people make informed decisions about their health. Whether you already have experience with homeopathy or simply want to inform yourself, we hope that this article will provide you with valuable insights and information” (my translation).
Here I present to you just the relatively short section dedicated to the ‘pros and cons’ of homeopathy. Here we go:
Advantages of homeopathy:
- Holistic approach: homeopathy considers the human being as a whole and takes into account both physical and emotional aspects. It aims to support individual balance and the body’s self-healing powers.
- Gentle and non-invasive treatment: Homeopathic remedies are usually taken as globules, drops, or tablets and are therefore easy and convenient to use. They rarely cause side effects and are generally well tolerated.
- Individualized treatment: In homeopathy, each patient is considered unique and treatment is based on individual symptoms and characteristics. There is no “one-size-fits-all” solution, but a personalized approach.
- Support for chronic diseases: Homeopathy can be an alternative or complementary treatment for chronic conditions where conventional medicines offer limited relief. It can help improve quality of life and promote overall well-being.
Limitations of homeopathy:
- Placebo effect: Much of the effect of homeopathy is attributed to the placebo effect. It is argued that the improvements patients experience occur because of belief in the efficacy of the remedies and positive expectations, rather than due to a specific effect of the diluted substances.
- Lack of scientific evidence: The scientific evidence for the efficacy of homeopathy is limited and controversial. Many studies have failed to demonstrate benefits beyond the placebo effect. There is a lack of well-conducted randomized controlled trials that clearly show the effectiveness of homeopathy.
- Delay or rejection of conventional treatments: In some cases, the choice of homeopathy as the sole method of treatment may lead to delays in the diagnosis and timely treatment of serious or acute illnesses. It is important that serious illnesses are examined by a doctor and treated appropriately.
- Difficulties in standardization: Homeopathy involves a variety of remedies used in different potencies and dilutions. This makes standardization and the conduct of reproducible studies difficult. There are also controversial debates about whether the dilutions go beyond the extent to which molecules of the original substance are still present.
__________________________
I am sure that you have heard the BS about the alleged advantages of homeopathy often enough. Therefore, I will here not bother to comment on them again. More interesting, in my view, are the limitations of homeopathy, as seen by its proponents. Please allow me, therefore, to discuss them briefly.
- The authors state that “it is argued that the improvements patients experience occur because of belief in the efficacy of the remedies and positive expectations”. This sounds as though this is a mere aberrant opinion or at least an ongoing debate amongst scientists. In fact, it is the scientific consensus supported by tons of evidence.
- This is the same point expressed differently.
- The admission that “the choice of homeopathy as the sole method of treatment may lead to delays in the diagnosis and timely treatment” is yet another way of stating that homeopathy is not effective. What is, however, not expressed clearly enough, in my view, is the fact that homeopathic treatment usually amounts to medical neglect which is unethical and can cause serious harm, in extreme cases even death.
- It is not true that the range of potencies renders “the conduct of reproducible studies difficult”. There are plenty of examples to demonstrate this, for instance, this study. “There are also controversial debates about whether the dilutions go beyond the extent to which molecules of the original substance are still present.” Yes, I did translate this correctly. I am sorry to say that this sentence does make no sense in German or in English.
What I find particularly interesting is that the authors do not mention disadvantages that non-homeopaths would rate as quite important, e.g.:
- The assumptions of homeopathy fly in the face of science.
- Hahnemann strictly forbade homeopathy to be combined with ‘allopathy’ (yet proponents now claim this option to be an advantage).
- Treating a patient with homeopathy violates even the most basic rules of medical ethics.
- Homeopaths have no choice but to lie to their patients on a daily basis.
- Many homeopaths have the nasty habit of advising their patients against using effective treatments, e.g. vaccinations.
- Homeopathy undermines rational thinking in a general way.
In summary, the authors’ “aim to provide a comprehensive overview of homeopathy and help people make informed decisions about their health” has not been reached.
The well-known Dr. Chris van Tulleken recently joined forces with Professor Michael Heinrich and Dr. Anthony Booker from the University College London School of Pharmacy to test a range of herbal products on sale in the UK. They bought over 70 herbal products from various high street stores and internet retailers. Some of the products were ‘THR’ (traditional herbal registration) herbal medicines, and some were marketed as food supplements. They then analyzed their chemistry to see whether each one really contained what the label says. The three popular herbal remedies we tested were:-
- Milk thistle (Silybum marianum),
- Ginkgo (Ginkgo biloba),
- Evening primrose (Oenothera).
The team at UCL used two different methods of analysis to verify the identity of these herbal products and extracts. High-performance thin-layer chromatography (HPTLC) is a sophisticated technique for the analysis of herbal products and is one of the most commonly used methods in the industry. HPTLC analysis creates a chemical fingerprint of the product which the researchers can then compare to an accepted reference standard for the herb. They look for a broad spectrum of ‘marker compounds’ these are the pharmacologically active and/or chemical constituents within a plant that can be used to verify its potency or identity. For complex samples or where additional confirmation is required, researchers often turn to ¹H nuclear magnetic resonance spectroscopy (¹H-NMR) which allows individual samples to be compared in detail against other samples or to the whole group.
In every THR product tested, the product contained what was claimed on the label. However, the food supplements showed a wide range of quality.
- Of the food supplement products labeled as Ginkgo, 8 out of 30 (27%) contained little or no ginkgo extract.
- 36% of the food supplement milk thistle products contained no detectable milk thistle. Although this is quite a small sample size it is still a startling result. Furthermore, in one case of milk thistle, unidentified adulterants suspected to be synthetic compounds were present in place of milk thistle.
- All of the evening primrose food products we tested did contain what the packet claimed.
The researchers concluded that their investigation shows that a regulatory system for herbal products, like the THR scheme, ensures that people have access to safe herbal medicine products. So, if you are considering buying herbal products then do look out for the THR mark– otherwise, you might not just be wasting your money, you might be consuming other, potentially dangerous, ingredients.
_______________________________
This is an interesting investigation. The researchers should be commended for it! However, I disagree with some of their conclusions. Here is why:
- The investigation merely tested the quality of the products and NOT THEIR SAFETY! To claim that the THR ensures access to safe herbal medicines is incorrect. A product might be of adequate quality but can still be unsafe. The THR only implies safety because the herbal has been used for years without problems being noted. This is not the same as ensuring that it is safe. A direct test of safety is usually not available.
- The recommendation to buy a product with a THR mark is also somewhat misleading. It implies that these products are effective. I fail to see convincing evidence that either MILK THISTLE, GINKGO, or EVENING PRIMROSE are effective for any disease or condition. Thus the responsible recommendation should, in my view, be to NOT buy them regardless of whether they are of good quality or not.
A ‘manifesto’ is not something that I come across often in my area of research, i.e. so-called alternative medicine (SCAM). This one is in German, I, therefore, translated it for you:
Manifesto for healthy medicine
With the Manifesto for healthy medicine, we, the citizens and patients alliance weil’s hilft! (‘BECAUSE IT HELPS’) demand a fundamental change in our healthcare system, towards a diverse medicine that focuses on people and health. Be part of it! Sign the manifesto and become part of the movement.
It’s of paramount importance, the Manifesto for healthy medicine. About the way we live. It’s about our health. It’s about you and it’s about me.
We want our healthcare system to actually focus on health.
We want a medicine that doesn’t ask what’s missing, but what is possible.
We want a medicine that cares about people, that takes care, gets to the bottom of things, and uses innovative technologies to do so.
We want more bio, so that the chemistry is right, and we want naturopathic procedures and naturally effective medicines to be recognized, promoted, and researched further.
We want research that creates knowledge because, in addition to studies, it also takes into account the experience of physicians and the needs of patients.
We want carers and doctors to be able to work in a way that is good for their patients and for themselves.
We want people from all healthcare professions to work together as equals.
We want a medicine that creates awareness for a good and healthy life because climate protection also begins in one’s own body.
We want an integrative medicine that puts people at the center and self-evidently combines conventional and natural healing methods.
And we want this medicine to be accessible and affordable for everyone.
We fight for a healthy medicine of the future.
Be part of it!
(sorry, if some of it might sound badly translated but the German original is in parts pure gibberish)
_____________________
Who writes such tosh composed of every thinkable platitude and then pompously calls it a MANIFESTO?
BECAUSE IT HELPS! (weil’s hilft!) is a citizens’ movement that demands a change in the health care system – towards the needs and preferences of patients, towards a holistic view of people, and a focus on health instead of disease. The sensible combination of natural medicine and conventional medicine, an integrative medicine, makes an indispensable contribution to this. This is because it relies fully on the patients and involves them as active partners in the treatment. Modern medicine of the future, therefore, needs the equal cooperation of natural medicine and conventional medicine – in the everyday life of physicians and patients, in the reimbursement by the health insurance companies as well as in research and teaching.
On the information platform www.weils-hilft.de weil’s hilft! informs about current developments in integrative medicine, provides background information, and publishes a podcast once a month. The movement is also active on social media at www.facebook.com/weilshilft and www.instagram.com/weilshilft.
weil’s hilft! is supported by the health and patient organizations GESUNDHEIT AKTIV, KNEIPP-BUND, and NATUR UND MEDIZIN. Together, the alliance represents the interests of more than 220,000 people.
_______________________
One could easily disclose the funny side of this, the utter stupidity of the arguments, the platitudes, fallacies, misunderstandings, ignorance, etc. Yes, that would hardly be difficult. But it would ignore how worrying this and similar movements are. They systematically misinform consumers with the sole aim of persuading them that the integration of unproven or disproven treatments into medical routine is in their interest. Yet, if we only scratch the surface of their arguments, we realize that it is exclusively in the interest of those who profit from this type of misinformation.
Imagine you have caught a cold. You think it is not necessary to see a doctor, but you want to take something that helps your body to get better. What is your choice of remedy? There are many options provided by conventional medicine as well as by so-called alternative medicine (SCAM).
Many people opt for SCAM to address health issues or prevent diseases. Yet, the evidence for SCAMs is either lacking or controversial due to methodological weaknesses. Thus, practitioners and patients primarily rely on subjective references rather than credible evidence from systematic research.
This study investigated whether cognitive and personality factors explain the differences in belief in SCAM and homeopathy. The researchers investigated the robustness of 21 predictors when examined together to obtain insights into some key determinants of such beliefs in a sample of 599 participants (60% female, 18-81 years). A combination of predictors explained 20% of the variance in SCAM belief. These predictors were:
- ontological confusions,
- spiritual epistemology,
- agreeableness,
- death anxiety,
- gender.
Approximately 21% of the variance in belief in homeopathy was explained by the following predictors:
- ontological confusions,
- illusory pattern perception,
- need for cognitive closure,
- need for cognition,
- honesty-humility,
- death anxiety,
- gender,
- age.
The authors concluded that some of the predictors from previous research replicated whereas others did not. Demographics and certain cognitive variables seem to be key determinants associated with beliefs in SCAM and homeopathy. Those individual differences and cognitive biases might result in a different perception of the world. However, variables related to abilities did not predict the beliefs. Thus, they might not be a result of inability but rather of ignorance.
Previous studies have shown that SCAM believers tend to believe in paranormal phenomena and conspiracies. I think that, in the discussion sections of this blog, we have ample evidence for this to be true. Paranormal beliefs are usually built on a magical worldview without reasoned review, which is shared by SCAM proponents. Such beliefs advocate emotional criteria for truth instead of data and logical considerations. Another belief, namely spirituality, is closely related to paranormal beliefs and religiosity and also associated with being a SCAM user. Lindeman found that SCAM belief could be best explained by intuitive reasoning, paranormal beliefs, and ontological confusions, defined as category mistakes in which properties of living and lifeless entities are mixed.
The authors point out that their results do not replicate previous findings that showed predictive value of certain cognitive variables such as cognitive style. An explanation could be that rather inattention to accuracy than the inability to consider empirical evidence fosters the beliefs. People might simply not be aware of the absence of evidence. Another possibility is that people are aware of the absence of evidence but are reluctant to engage with it. Practitioners and patients often claim “whatever works is good” or “the main thing is that it works”. Thus, it is ignorance rather than a lack of capacity to appropriately process the evidence.
The authors of this study are well aware of the limitations of their research:
“As with most cross-sectional studies using questionnaires, our results are based on self-reports. Additionally, single items were used for measuring belief strength. Even if multi-item measures often have advantages, single items can be advantageous in terms of practical benefits, e.g., adapting to subjects’ limited attention and time resources. There are several single item measures successfully used to measure diverse concepts including attitudes. Also, the variance on those items in our sample shows that participants were able to reflect their beliefs and rank them on the scale provided. Another limitation is that the findings are based on regression analyses, which do not provide insight into causality. Thus, the relationship remains correlational. Even if our sample was broader than in many other psychological studies—it was slightly unbalanced, especially in comparison to the German population. It over-represented educated individuals which may lead to an inadequate variation of the cognitive variables if we consider the relationship between cognition and education. However, education and the cognitive variables are only weakly correlated. Thus, it can be assumed that the unbalanced sample did not affect the distribution of cognitive variables to a great extent.”
I came across an article entitled “Consent for Paediatric Chiropractic Treatment (Ages 0-16)“. Naturally, it interested me. Here is the full paper; I have only inserted a few numbers in square brackets which refer to my comments below:
By law, all Chiropractors are required to inform you of the risks and benefits of chiropractic spinal manipulation and the other types of care we provide. Chiropractors use manual therapy alongside taking a thorough history, and doing a neurological, orthopaedic and chiropractic examination to both diagnose and to treat spinal, cranial and extremity dysfunction. This may include taking joints to the end range of function, palpating soft tissues (including inside the mouth and the abdomen), mobilisation, soft tissue therapy and very gentle manipulation [1]. Our Chiropractors have been educated to perform highly specific types of bony or soft tissue manipulation and we strive to follow a system of evidence-based care [2]. At the core of our belief system is “Do No Harm”. We recognise that infants and children are not tiny adults. The force of an adjustment used in a child is at least less than half of what we might use with a fully grown adult. Studies by Hawk et al (2016) and Marchand (2013) agreed that Chiropractors use 15 – 35 x less force in the under 3-month age group when compared to medical practitioners doing manipulation (Koch, 2002) [3]. We also use less force in all other paediatrics groups, especially when compared to adults (Marchand, 2013). In addition to using lower force, depth, amplitude and speed in our chiropractic adjustments [4], we utilise different techniques. We expect all children under the age of 16 years to be accompanied by a responsible adult during appointments unless prior permission to treat without a consenting adult e.g., over the age of 14 has been discussed with the treating chiropractor.
Risks
- Research into chiropractic care for children in the past 70 years has shown it to have a low risk of adverse effects (Miller, 2019) [5]. These effects tend to be mild and of short duration e.g., muscular or ligament irritation. Vorhra et al (2007) found the risk of severe of adverse effects (e.g. fracture, quadriplegia, paraplegia, and death) is very, very rare and was more likely to occur in individuals where there is already serious underlying pathology and missed diagnosis by other medical profession [6]. These particular cases occurred more than 25 years ago and is practically unheard of now since research and evidence-based care has become the norm [7].
- The most common side effect in infants following chiropractic treatment includes fussiness or irritability for the first 24 hours, and sleeping longer than usual or more soundly. (Miller and Benfield, 2008) [8]
- In older children, especially if presenting with pain e.g., in the neck or lower back, the greatest risk is that this pain may increase during examination due to increasing the length of involved muscles or ligaments [9]. Similarly, the child may also experience pain, stiffness or irritability after treatment (Miller & Benfield, 2008) [10]. Occasionally children may experience a headache.[11] We find that children experience side effects much less often than adults.[12]
Benefits
- Your child might get better with chiropractic care. [13] If they don’t, we will refer you on [14].
- Low risk of side effects and very rare risk of serious adverse effects [15].
- Drug-free health care. We are not against medication, but we do not prescribe [16].
- Compared with a medical practitioner, manual therapy carried out by a chiropractor is 20 x less likely to result in injury (Koch et al 2002, Miller 2009).[17]
- Children do not often require long courses of treatment (>3 weeks) unless complicating factors are present.[18]
- Studies have shown that parents have a high satisfaction rate with Chiropractic care [19].
- Physical therapies are much less likely to interfere with biomedical treatments. (McCann & Newell 2006) [20]
- You will have a better understanding of diagnosis of any complain and we will let you know what you can do to help.[21]
We invite you to have open discussions and communication with your treating chiropractor at all times. Should you need any further clarification please just ask.
References
- Hawk, C. Shneider, M.J., Vallone, S and Hewitt, E.G. (2016) – Best practises recommendations for chiropractic care of children: A consensus update. JMPT, 39 (3), 158-168.
- Marchand, A. (2013) – A Proposed model with possible implications for safety and technique adaptations for chiropractic spinal manipulative therapy for infants and children. JMPT, 5, 1-14
- Koch L. E., Koch, H, Graumann-Brunnt, S. Stolle, D. Ramirez, J.M., & Saternus, K.S. (2002) – Heart rate changes in response to mild mechanical irritation of the high cervical cord region in infants. Forensic Science International, 128, 168-176
- Miller J (2019) – Evidence-Based Chiropractic Care for Infants: Rational, Therapies and Outcomes. Chapter 11: Safety of Chiropractic care for Infants p111. Praeclarus Press
- Vohra, S. Johnston, B.C. Cramer, K, Humphreys, K. (2007) – Adverse events associated with paediatric spinal manipulation: A Systematic Review. Pediatrics, 119 (1) e275-283
- Miller, J and Benfield (2008) – Adverse effects of spinal manipulative therapy in children younger than 3 years: a retrospective study in a chiropractic teaching clinic. JMPT Jul-Aug;31(6):419-23.
- McCann, L.J. & Newell, S.J. (2006). Survey of paediatric complementary and alternative medicine in health and chronic disease. Archives of Diseases of Childhood, 91, 173-174
- Corso, M., Cancelliere, C. , Mior., Taylor-Vaise, A. Côté, P. (2020) – The safety of spinal manipulative therapy in children under 10 years: a rapid review. Chiropractic Manual therapy 25: 12
___________________________________
- “taking joints to the end range of function” (range of motion, more likely) is arguably not “very gently”;
- “we strive to follow a system of evidence-based care”; I do not think that this is possible because pediatric chiropractic care is hardy evidence-based;
- as a generalizable statement, this seems to be not true;
- ” lower force, depth, amplitude and speed”; I am not sure that there is good evidence for that;
- research has foremost shown that there might be significant under-reporting;
- to blame the medical profession for diagnoses missed by chiropractors seems odd;
- possibly because of under-reporting;
- possibly because of under-reporting;
- possibly because of under-reporting;
- possibly because of under-reporting;
- possibly because of under-reporting;
- your impressions are not evidence;
- your child might get even better without chiropractic care;
- referral rates of chiropractors tend to be low;
- possibly because of under-reporting;
- chiropractors have no prescription rights but some lobby hard for it;
- irrelevant if we consider the intervention useless and thus obsolete;
- any evidence for this statement?;
- satisfaction rates are no substitute for real evidence;
- that does not mean they are effective, safe, or value for money;
- this is perhaps the strangest statement of them all – do chiropractors think they are the optimal diagnosticians for all complaints?
_____________________________________
According to its title, the paper was supposed to deal with consent for chiropractic pediatric care. It almost totally avoided the subject and certainly did not list the information chiropractors must give to parents before commencing treatment.
Considering the arguments that the article did provide has brought me to the conclusion that chiropractors who treat children are out of touch with reality and seem in danger of committing child abuse.
This meta-analysis aimed “to provide better evidence of the efficacy of manual therapy (MT) on adolescent idiopathic scoliosis (AIS)”. 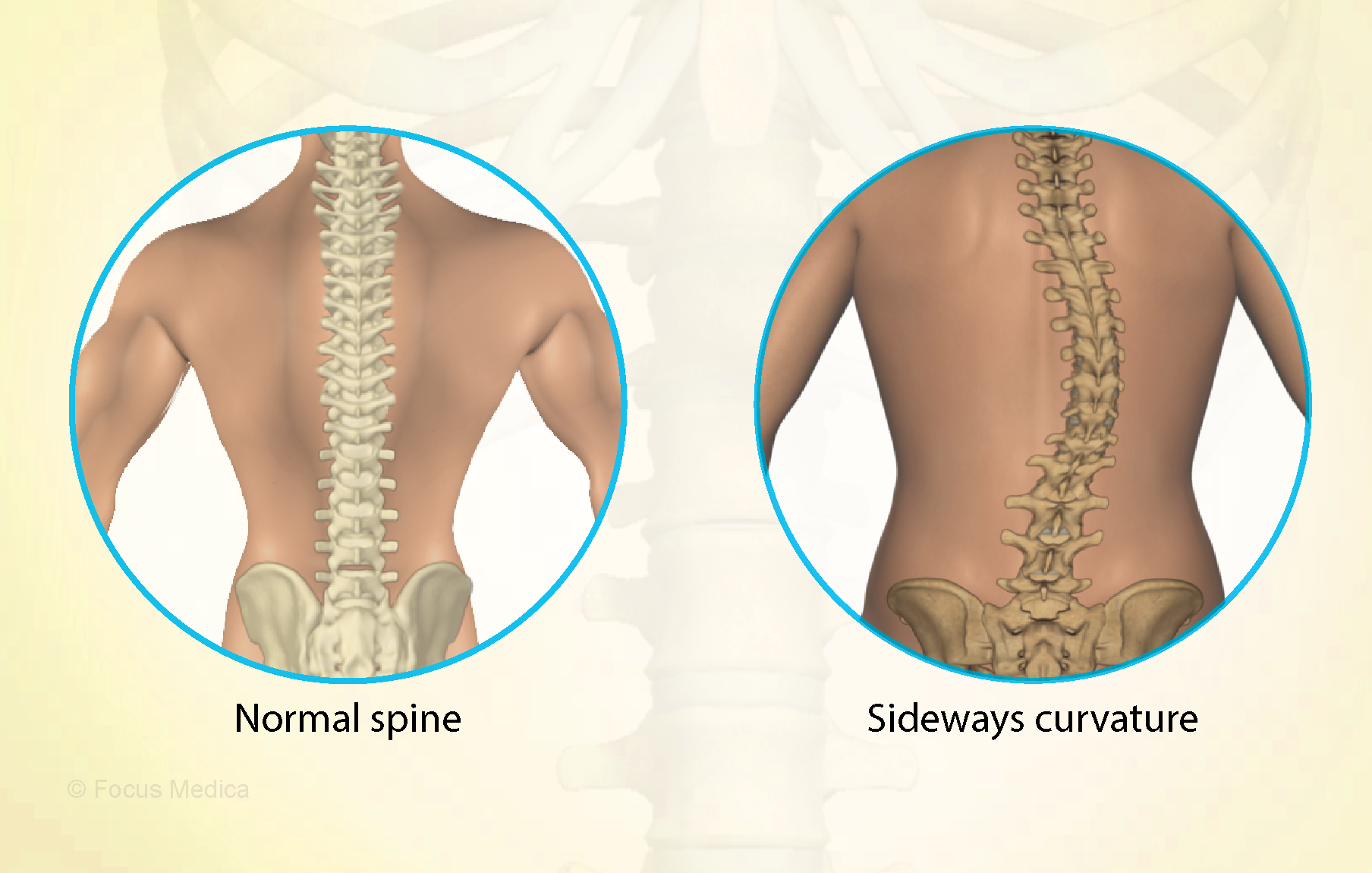
All RCTs of MT for the management of patients with AIS were included in the present study. The treatment difference between the experimental and control group was mainly MT. The outcomes consisted of the total effective rate, the Cobb angle, and Scoliosis Research Society-22 (SRS-22) questionnaire score. Electronic database searches were conducted from database inception to July 2022, including the Cochrane Library, PubMed, Web of Science, Embase, Wanfang Data, CNKI, and VIP. The pooled data were analyzed using RevMan 5.4 software.
Four RCTs with 213 patients in the experimental groups were finally included. There are 2 studies of standalone MT in the experimental group and 3 studies of MT with identical conservative treatments in the control group. Three trials reported the total effective rate and a statistically significant difference was found (P = 0.004). Three trials reported Cobb angle; a statistical difference was found (P = 0.01). Then, sensitivity analysis showed that there was a significant difference in the additional MT subgroup (P < 0.00001) while not in the standalone MT subgroup (P = 0.41). Three trials reported SRS-22 scores (P = 0.55) without significant differences.
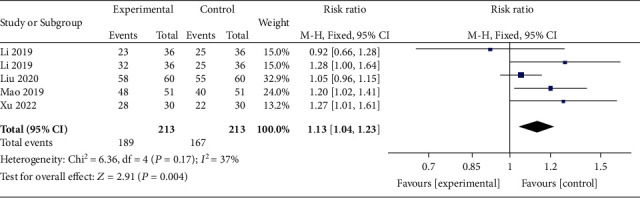
The authors concluded that there is insufficient data to determine the effectiveness of spinal manipulation limited by the very low quality of included studies. High-quality studies with appropriate design and follow-up periods are warranted to determine if MT may be beneficial as an adjunct therapy for AIS. Currently, there is no evidence to support spinal manipulation. 
The treatment of idiopathic scoliosis depends on the age, curve size, and progression of the condition. Therapeutic options include observation, bracing, physiotherapy, and surgery. They do NOT include MT because it is neither a plausible nor effective solution to this problem. It follows that further studies are not warranted and should be discouraged.
And, even if you disagree with me here and feel that further studies might be justified, let me remind you that proper research is never aimed at providing better evidence that a therapy works (as the authors of this odd paper seem to think); it must be aimed at testing whether it is effective!
Conspiracy beliefs have become a major issue and obstacle to progress. While holding conspiracy beliefs has been associated with several detrimental social, personal, and health consequences, little research has been dedicated to systematically reviewing the methods that could reduce conspiracy beliefs.
A team of researchers conducted a systematic review to identify and assess interventions that have sought to counter conspiracy beliefs. They included 25 studies (total N = 7179) and discovered that, while the majority of interventions were ineffective in terms of changing conspiracy beliefs, several interventions were particularly effective. Interventions that fostered an analytical mindset or taught critical thinking skills were found to be the most effective in terms of changing conspiracy beliefs.
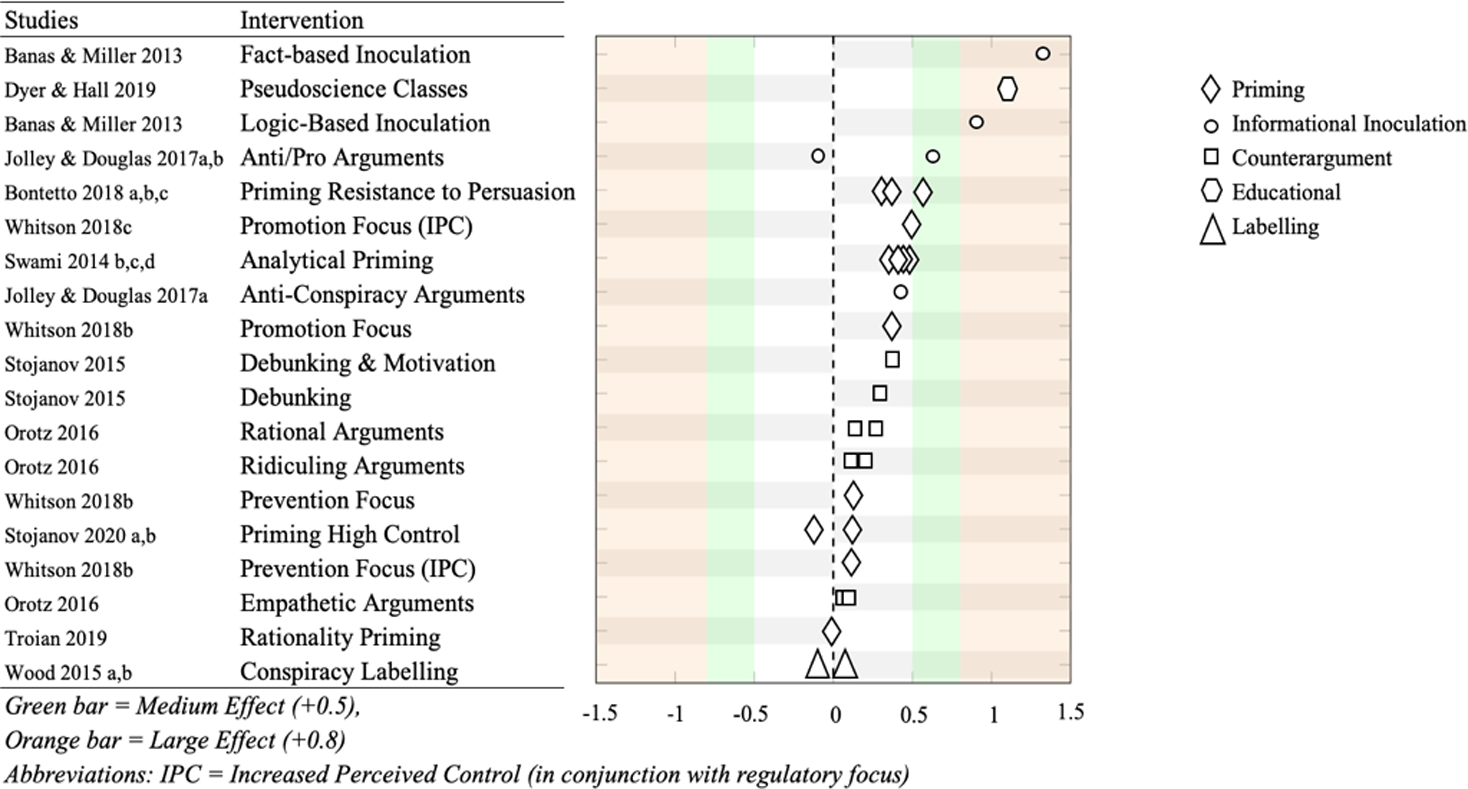
Approximately half of the examined interventions consisted of priming-based tasks. The majority of these interventions demonstrated a significant change in conspiracy beliefs. The effects were all either small or very small. Participants who were primed to be less susceptible to persuasion tactics showed significantly lower conspiracy beliefs when compared to controls among three experimental comparisons. These effects were shown to range from small to medium.
Interventions that primed participants to engage in analytical thinking resulted in primed participants having lower conspiracy beliefs than controls. However, the effects of these differences were small. Other priming interventions focused on manipulating participants’ sense of control. They had mixed results, either increasing or decreasing conspiracy beliefs with very small effects.
About a sixth of all interventions used inoculation methods. All successfully reduced conspiracy beliefs, relative to controls, all with either medium or large effects. Inoculations that identified the factual inaccuracies of conspiracy beliefs were found to be the most effective of all the interventions in the review. Inoculations that demonstrated the logical fallacies of conspiracy beliefs were found to be the second most effective intervention.
The authors concluded that their review found that overall, the majority of current conspiracy interventions are ineffective in terms of changing conspiracy beliefs. Despite this, we have identified several promising interventions that may be fruitful to pursue in future studies. We propose that a focus on inoculation-based and critical thinking interventions will bear more promising results for future research, though further efforts are needed to reduce participant burden and more easily implement these interventions in the real world.
The identification of the factual inaccuracies of conspiracy beliefs plus the stimulation of critical thinking are two aims I actively pursue with this blog. Thus, one might hope that I do make a small contribution to the reduction of conspiracy beliefs.
Yes, one might hope – but judging from many comments posted in the discussion sections, one could easily get a different impression.
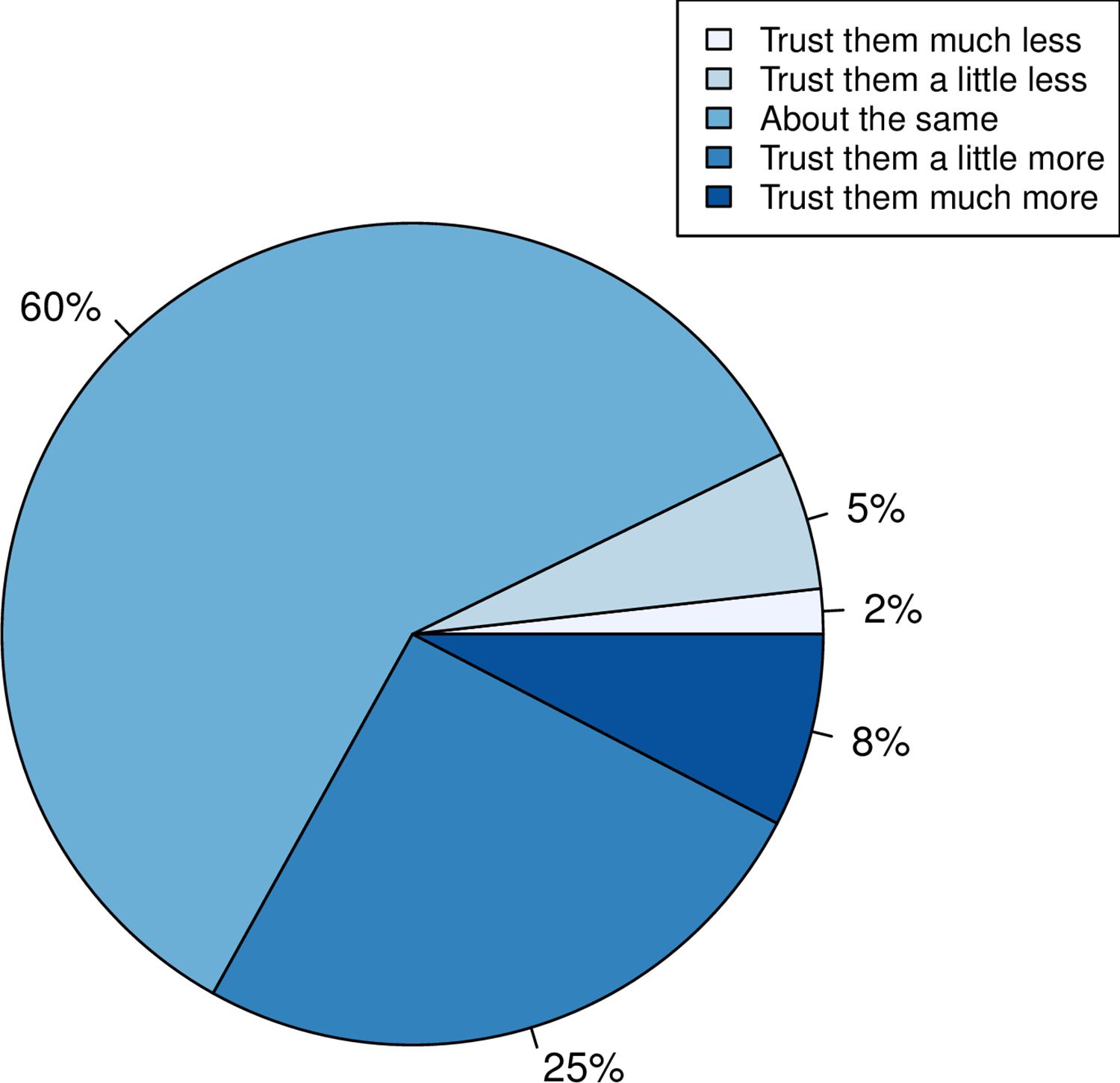
Research by the Milner Center for Evolution at the University of Bath, U.K., along with colleagues at the Universities of Oxford and Aberdeen, found that trust in scientists has hugely increased since the COVID-19 pandemic. The study also found that people were more likely to take the COVID-19 vaccine if their trust in the science had increased.
Using data from a survey of more than 2,000 U.K. adults commissioned by the Genetics Society, the team asked individuals whether their trust in scientists had gone up, down, or stayed the same.
- A third of people reported that their trust in scientists had gone up.
- When Pfizer, a company that made COVID-19 vaccines, was used as an example of the pharma industry, more people reported a positive response than when GlaxoSmithKline, a company not associated with the COVID-19 vaccine, was mentioned.
- The researchers also found that people who reported holding a negative view of science before the pandemic had become even more negative.
- People reporting increased trust were most likely to take the COVID-19 vaccine.
- Those preferring not to do so reported a decline in trust.
This is an interesting study with relevance to many discussions we had on this blog. I recommend reading it in full. Here are the abstract and link to the paper:
While attempts to promote acceptance of well-evidenced science have historically focused on increasing scientific knowledge, it is now thought that for acceptance of science, trust in, rather than simply knowledge of, science is foundational. Here we employ the COVID-19 pandemic as a natural experiment on trust modulation as it has enabled unprecedented exposure of science. We ask whether trust in science has on the average altered, whether trust has changed the same way for all and, if people have responded differently, what predicts these differences? We 1) categorize the nature of self-reported change in trust in “scientists” in a random sample of over 2000 UK adults after the introduction of the first COVID vaccines, 2) ask whether any reported change is likely to be real through consideration of both a negative control and through experiment, and 3) address what predicts change in trust considering sex, educational attainment, religiosity, political attitude, age and pre-pandemic reported trust. We find that many more (33%) report increased trust towards “scientists” than report decreased trust (7%), effects of this magnitude not being seen in negative controls. Only age and prior degree of trust predict change in trust, the older population increasing trust more. The prior degree of trust effect is such that those who say they did not trust science prior to the pandemic are more likely to report becoming less trusting, indicative of both trust polarization and a backfire effect. Since change in trust is predictive of willingness to have a COVID-19 vaccine, it is likely that these changes have public health consequences.
I had come across them so often that I had almost stopped noticing them: the ‘little extras‘ that make ineffective so-called alternative medicines (SCAMs) seem effective. Then, recently, during an interview about detox diets, the interviewer responded to my explanation of the ineffectiveness of these treatments by saying: “but these diets include stopping the consumption of alcohol, cigarettes, and other harmful stuff; therefore they must be good.” This seemingly convincing argument reminded me of a phenomenon – I call it here the ‘little extra‘ – that applies to so many (if not most) SCAMs.
Let me schematically summarise it as follows:
- A practitioner applies an ineffective SCAM to a patient.
- Because it is ineffective, it has little effect other than a small placebo response.
- The ineffective SCAM comes with a ‘little extra‘ which is unrelated to the SCAM.
- The ‘little extra‘ is effective.
- The end result is that the ineffective SCAM appears to be effective.
The above example makes it quite clear: the detox diet is utter nonsense but, as it goes hand in hand with effective lifestyle changes, it appears to be effective. A classic case. But SCAM offers no end of similar examples:
- Acupuncture is useless but it involves touch, time, attention, and empathy all of which are effective in making a patient feel better.
- Chiropractic is useless but it involves touch, time, attention, and empathy all of which are effective in making a patient feel better.
- Homeopathy is useless but it involves a long, empathic consultation and attention which are effective in making a patient feel better.
- Osteopathy is useless but it involves touch, time, attention, and empathy all of which are effective in making a patient feel better.
- Reflexology is useless but it involves touch, time, attention, and empathy all of which are effective in making a patient feel better.
Do I need to continue?
Probably not!
The ‘little extras‘ are often forgotten or subsumed under the heading ‘placebo’. Yet, they are not part of the placebo effect. Strictly speaking, they are concomitant treatments comparable to a pain patient using SCAM and also taking a few paracetamols. In the end, she forgets about the painkillers and thinks that her SCAM worked wonders.
Even ardent SCAM proponents have long realized this phenomenon. Here, for example, is a paper entitled ‘Acupuncture as a complex intervention: a holistic model’ by ex-colleagues of mine at Exeter looking at it but coming up with a very different perspective:
Objectives: Our understanding of acupuncture and Chinese medicine is limited by a lack of inquiry into the dynamics of the process. We used a longitudinal research design to investigate how the experience, and the effects, of a course of acupuncture evolved over time.
Design and outcome measures: This was a longitudinal qualitative study, using a constant comparative method, informed by grounded theory. Each person was interviewed three times over 6 months. Semistructured interviews explored people’s experiences of illness and treatment. Across-case and within-case analysis resulted in themes and individual vignettes.
Subjects and settings: Eight (8) professional acupuncturists in seven different settings informed their patients about the study. We interviewed a consecutive sample of 23 people with chronic illness, who were having acupuncture for the first time.
Results: People described their experience of acupuncture in terms of the acupuncturist’s diagnostic and needling skills; the therapeutic relationship; and a new understanding of the body and self as a whole being. All three of these components were imbued with holistic ideology. Treatment effects were perceived as changes in symptoms, changes in energy, and changes in personal and social identity. The vignettes showed the complexity and the individuality of the experience of acupuncture treatment. The process and outcome components were distinct but not divisible, because they were linked by complex connections. The paper depicts these results as a diagrammatic model that illustrates the components and their interconnections and the cyclical reinforcement, both positive and negative, that can occur over time.
Conclusions: The holistic model of acupuncture treatment, in which “the whole being greater than the sum of the parts,” has implications for service provision and for research trial design. Research trials that evaluate the needling technique, isolated from other aspects of process, will interfere with treatment outcomes. The model requires testing in different service and research settings.
I think the perspective of viewing SCAMs as complex interventions is needlessly confusing and deeply unhelpful. The truth is that there is no treatment that is not complex. Take a surgical treatment, for instance, it involves dozens of ‘little extras‘ that are known to be effective. Should we, therefore, try to use this fact for justifying useless surgical interventions? Or take a simple prescription of medication from a doctor. It involves time, empathy, attention, explanations, etc. all of which will affect the patient’s symptoms. Should we thus use this to justify a useless drug? Certainly not!
And for the same reason, it is nonsense to use the ‘little extras‘ that come with all the numerous ineffective SCAMs as a smokescreen that makes them look effective.
So-called alternative medicine (SCAM) is widely used in Arabia. One of the commonly used methods is camel urine alone or mixed with camel milk. Camel urine is a liquid by-product of camel metabolism. Urine from camels has been used as prophetic medicine for centuries, being a part of ancient Bedouin practices. Camel urine comes out as a concentrated, viscous syrup because the kidneys and intestines of a camel are very efficient at reabsorbing water. 
Camel urine is consumed and used for treating numerous ailments. Some employ it as a treatment for hair loss, for instance. The camel urine from a virgin camel is priced at twenty dollars per liter, with herders saying that it has curative powers.
A recent paper offers more information:
Camel is one of the important livestock species which plays a major role in the pastoral mode of life by fulfilling basic demands of livelihood. Traditionally, camel urine has been used in the treatment of human diseases. With regard to the health benefits of drinking the urine of camels, it has been proven by modern scientific researches. Camel urine has an unusual and unique biochemical composition that contributes to medicinal values. The chemical composition of camel urine showed the presence of purine bases, hypoxanthine, sodium, potassium, creatinine, urea, uric acid, and phosphates. The nano-particles in the camel’s urine can be used to fight cancer. Camel urine has antimicrobial activity against pathogenic bacteria. Its chemical and organic constituents have also inhibitory properties against fungal growth, human platelets, and parasitic diseases mainly fasciollosis in calves. The healthy status of the liver can be restored through ingestion of diet and minerals in camel urine. Camel urine is used by the camel owners and Bedouins as medicine in different ways. The Bedouin in the Arab desert used to mix camel urine with milk. Recently; the WHO has warned against drinking camel urine due to the modern attempt to limit Outbreaks of Respiratory Syndrome (MRS) in the Middle East. There is no scientific dosage for camel urine to be applied as medicine for different diseases and the ways of camel urine formulation and utilization for the care of patients varies from country to country. Therefore, the purposes of the present review describe the biochemical composition of camel urine will be scientifically extracted and formulated as a therapy rather than drinking raw urine and people’s health impact.
Researchers from the Medical Oncology Department, Comprehensive Cancer Center, King Fahad Medical City, Riyadh, Saudi Arabia wanted to determine whether camel urine shows promise in the treatment of cancer. The aim of their study was to observe cancer patients who insisted on using camel urine and to devise some clinically relevant recommendations.
The authors observed 20 cancer patients (15 male, 5 female) from September 2020 to January 2022 who insisted on using camel urine. They documented the demographics of each patient, the method of administering camel urine, the reasons for refusing conventional treatment, the period of follow-up, and the outcome and side effects.
All the patients had radiological investigations before and after finishing treatment with camel urine. All patients used a combination of camel urine and milk, and treatment ranged from a few days up to 6 months. The average amount of urine/milk consumed was 60 ml/day. No clinical benefit was observed and two patients developed brucellosis. Eleven patients changed their minds and eventually accepted conventional antineoplastic treatments but 7 were too weak to receive further treatment and died from their disease.
The authors concluded that camel urine had no clinical benefits in cancer patients, and may even have caused zoonotic infection. The promotion of camel urine as a traditional medicine should be stopped because there is no scientific evidence to support it.
I fear that, yet again, ‘ancient wisdom’ turns out to be just ‘old bullshit’.