clinical trial
Lian gong (LG), also called Lian Gong Shi Ba Fa, is a form of so-called alternative medicine (SCAM) from China. More specifically, it is a set of stretching, breathing exercises, and self-massaging techniques aimed at preventing and relieving stress as well as acute pains around the neck, shoulders, back, hips, legs, joints, and connective tissues. Even though it is relatively new, it is based on old Chinese stretching, breathing, and warm-up exercises dating back more than 1,000 years, including the Eight Silk Brocade (八段錦). Lian gong has spread rapidly from China to other countries, especially to Japan and Brazil.
Lian Gong was developed by Dr. Zhuang Yuan Ming (1919- ), a traditional Chinese medical doctor, who started conducting a series of clinical trials around 1974 in a Shanghai hospital on patients suffering from a variety of stress-related conditions. Lian Gong is now being promoted as “massage in motion”.
One of the few controlled clinical studies of Liam gong aimed to evaluate the effects of LG on the impact of dizziness on the quality of life and fear of falling in primary health care patients. It was designed as a randomized clinical trial with 36 patients with dizziness not caused by central changes. The participants were randomly assigned to 3 groups:
- the Liam gong (LG) group ( n = 11),
- the vestibular rehabilitation (VR) group ( n = 11),
- the control group ( n = 14).
The treatments were carried out over a period of 12 weeks.
Lian gong reduced the influence of dizziness on the quality of life in physical (1.8 points, 95% confidence interval [CI]: 0.2-3.4), functional (4.0 points, 95% CI: 2.1-5.9), and emotional domains of quality of life (4.4 points, 95% CI: 1.7-7.2), with no differences, compared with VR.
The authors concluded that Lian gong was shown to be an effective balance rehabilitation strategy to reduce the impact of dizziness on quality of life, with similar results to those of VR.
Unfortunately, this study has many flaws – not least its minute sample size. Therefore, the conclusions seem more than a little over-optimistic. I would not be all that surprised to learn that these exercises can have beneficial effects for a range of conditions. What seems doubtful in my view, however, is whether it is superior to more conventional exercise therapies.
Ovariohysterectomy (OH) is one of the most frequent elective surgical procedures in routine veterinary practice. The aim of this study was to evaluate analgesia with Arnica montana 30cH during the postoperative period after elective OH.
Thirty healthy female dogs, aged 1 to 3 years, weighing 7 to 14 kg, were selected at the Veterinary Hospital in Campo Mourão, Paraná, Brazil. The dogs underwent the surgical procedure with an anaesthetic protocol and analgesia that had the aim of maintaining the patient’s wellbeing. After the procedure, they were randomly divided into three groups of 10. One group received Arnica montana 30cH; another received 5% hydroalcoholic solution; and the third group, 0.9% NaCl saline solution. All animals received four drops of the respective solution sublingually and under blinded conditions, every 10 minutes for 1 hour, after the inhalational anaesthetic had been withdrawn. The Glasgow Composite Measure Pain Scale was used to analyse the effect of therapy. Analysis of variance (ANOVA) followed by the Tukey test was used to evaluate the test data. Statistical differences were deemed significant when p ≤0.05.
The results show that the Arnica montana 30cH group maintained analgesia on average for 17.8 ± 3.6 hours, whilst the hydroalcoholic solution group did so for 5.1 ± 1.2 hours and the saline solution group for 4.1 ± 0.9 hours (p ≤0.05).
The authors concluded that these data demonstrate that Arnica montana 30cH presented a more significant analgesic effect than the control groups, thus indicating its potential for postoperative analgesia in dogs undergoing OH.
I do not have access to the full article (I was fired by the late Peter Fisher from the editorial board of the journal ‘HOMEOPATHY’) which puts me in a somewhat difficult position:
- not reporting this study could be construed as an anti-homeopathy bias,
- and reporting it handicaps me as I cannot assess essential details.
So, if anyone has access, please send the full paper to me and I will then study it and revise this post accordingly.
Judging from the abstract, I have to say that the results seem far too good to be true. I doubt that any oral remedy can have the effect that is being described here – let alone one that has been diluted (sorry, potentised) at a rate of 1: 1000000000000000000000000000000000000000000000000000000000000. That fact alone reduces the plausibility of the finding to zero.
At this stage, I do wonder who peer-reviewed the study and ask myself whether the rough data have been checked for reliability.
Psychosocial distress, depression, or anxiety are frequent problems of women after a breast cancer diagnosis and treatment. Many try so-called alternative medicine (SCAM) in an attempt to deal with them. But is this effective?
The purpose of this study was to assess the potential benefit of lavender oil as a perioperative adjunct to improve anxiety, depression, pain, and sleep in women undergoing microvascular breast reconstruction.
This was a prospective, single-blinded, randomized, controlled trial of 49 patients undergoing microvascular breast reconstruction. Patients were randomized to receive lavender oil or a placebo (coconut oil) throughout their period of hospitalization. The effect of lavender oil on perioperative stress, anxiety, depression, sleep, and pain was measured using the hospital anxiety and depression scale, Richards-Campbell Sleep Questionnaire, and the visual analogue scale.
Twenty-seven patients were assigned to the lavender group and 22 patients were assigned to the control group. No significant differences were seen in the perioperative setting between the groups with regard to anxiety (p = 0.82), depression, sleep, or pain scores. No adverse events were noted, and no significant differences in surgery-related complications were observed. When evaluating the entire cohort, postoperative anxiety scores were significantly lower than preoperative scores, while depression scores were significantly higher postoperatively as compared with preoperatively.
The authors concluded that, in the setting of microvascular breast reconstruction, lavender oil and aromatherapy had no significant adverse events or complications; however, there were no measurable advantages pertaining to metrics of depression, anxiety, sleep, or pain as compared with the control group.
One could argue that the sample size of the trial was too low to pick up small differences in the outcome measures. Yet, even then, the findings do not suggest that the treatment did make a large enough difference to justify the effort and expense of the treatment.
One could also argue that – who cares? – if a patient wants aromatherapy (or another SCAM that is harmless), why not? The answer to this is the fact that researchers have the ethical duty to identify the most effective treatment, and clinicians have the ethical duty to employ not just any odd therapy but the one that works demonstrably best. Seen from this perspective, the place of SCAM in cancer care seems far less certain than many enthusiasts try to make us believe.
Neck pain affects a vast number of people and leads to reduced quality of life and high costs. Clinically, it is a difficult condition to manage, and the effect sizes of the currently available treatments are moderate at best. Activity and manual therapy are first-line treatment options in several guidelines. But how effective are they really?
This study investigated the combination of home stretching exercises and spinal manipulative therapy in a multicentre randomized controlled clinical trial, carried out in a multidiscipline range of primary care clinics.
The treatment modalities utilized were spinal manipulative therapy combined with home stretching exercises compared to home stretching exercises alone. Both groups received 4 treatments for 2 weeks. The primary outcome was pain, where the subjective pain experience was investigated by assessing pain intensity (NRS – 11) and the quality of pain (McGill Pain Questionnaire). Neck disability and health status were secondary outcomes, measured using the Neck Disability Indexthe EQ-5D, respectively.
One hundred thirty-one adult subjects were randomized to one of the two treatment groups. All subjects had experienced persistent or recurrent neck pain the previous 6 months and were blinded to the other group intervention. The clinicians provided treatment for subjects in both groups and could not be blinded. The researchers collecting data were blinded to treatment allocation, as was the statistician performing data analyses. An intention-to-treat analysis was used.
Sixty-six subjects were randomized to the intervention group, and 65 to the control group. For NRS – 11, a B-coefficient of – 0,01 was seen, indication a 0,01 improvement for the intervention group in relation to the control group at each time point with a p-value of 0,305. There were no statistically significant differences between groups for any of the outcome measures.
Four intense adverse events were reported in the study, three in the intervention group, and one in the control group. More adverse incidents were reported in the intervention group, with a mean pain intensity (NRS-11) of 2,75 compared to 1,22 in the control group. There were no statistically significant differences between the two groups.
The authors concluded that there is no additional treatment effect from adding spinal manipulative therapy to neck stretching exercises over 2 weeks for patients with persistent or recurrent neck pain.
This is a rigorous and well-reported study. It suggests that adjuvant manipulations are not just ineffective for neck pain, but also cause some adverse effects. This seems to confirm many previously discussed investigations concluding that chiropractors do not generate more good than harm for patients suffering from neck pain.
In so-called alternative medicine (SCAM), vitamin D is often recommended for a range of indications, including cancer prevention. Observational studies did indeed suggest that low vitamin D status may be a risk factor for cancer. On the basis of such evidence, a team of researchers sought to determine if vitamin D supplementation lowers the risk of cancer and precancers.
The Vitamin D and type 2 diabetes (D2d) cancer outcomes study (D2dCA) is an ancillary study to the D2d study, which was conducted at 22 academic medical centers in the United States. Participants had prediabetes and overweight/obesity and were free of cancer for the previous 5 years. Participants were randomized to receive vitamin D3 4000 IU daily or placebo. At scheduled study visits (4 times/year), cancer and precancer events were identified by questionnaires. Clinical data were collected and adjudicated for all reported events. Cox proportional hazard models compared the hazard ratio (HR) of incident cancers and precancers between groups.
Over a median follow-up period of 2.9 years, among 2385 participants (mean age 60 years and 25-hydroxyvitamin D 28 ng/mL), there were 89 cases of cancer. The hazard ratio (HR) of incident cancer for vitamin D vs placebo was 1.07 (95% CI 0.70, 1.62). Of 241 participants with incident precancers, 239 had colorectal adenomatous polyps. The HR for colorectal polyps for vitamin D vs placebo was 0.83 (95% CI 0.64, 1.07).
The authors concluded that, in the D2d population of participants with prediabetes and overweight/obesity, not selected for vitamin D insufficiency, vitamin D supplementation did not have a significant effect on risk of incident cancer or colorectal polyps.
For some reason, the discussions about the value of vitamin D for any condition tend to be dominated by emotion rather than evidence. This is particularly true in the realm of SCAM. The trial is a significant step forward. It is rigorous and generates clear findings. Let’s hope it will contribute to a more rational debate about the value of vitamin D in cancer prevention.
Gua sha, sometimes referred to as “scraping”, “spooning” or “coining”, is a traditional Chinese treatment that has also been adopted in several other Asian countries. It has long been popular in Vietnam and is now also becoming
well-known in the West. The treatment consists of scraping the skin with a smooth edge placed against the pre-oiled skin surface, pressed down firmly, and then moved downwards along muscles or meridians, the assumed ‘energy’ channels of traditional Chinese medicine. According to its proponents, gua sha stimulates the flow of the vital energy ‘chi’ and releases unhealthy bodily matter from blood stasis within sored, tired, stiff or injured areas.
An international team of authors has revisited gua sha, a therapy that we have discussed repeatedly on this blog (see here and here). The authors offer the following summary:
Gua sha is a traditional healing technique that aims to create petechiae on the skin for a believed therapeutic benefit. Natural healings are mostly based on repeated observations and anecdotal information. Hypothetical model for healing does not always fit the modern understanding. Yet, the mechanisms underlying Gua Sha have not been empirically established. Contemporary scientific research can now explain some events of traditional therapies that were once a mystery. It is assumed that Gua Sha therapy can serve as a mechanical signal to enhance the immune surveillance function of the skin during the natural resolving of the petechiae, through which scraping may result in therapeutic benefits. The current review, without judging the past hypothetical model, attempts to interpret the experience of the ancient healings in terms of contemporary views and concepts.
The authors conclude that this narrative review draws up a survey of scientific sources on an ancient healing, scraping therapy. It is hypothesized that the skin, the nervous system and immune system interact with one another to generate a cascade of physiological responses to the scraping, through which scraping may result in therapeutic benefits. Within the scope and limitations of this review, only a brief overview could be given of the potential relationship between the observed outcomes and scraping therapy. Implementing effective traditional healings within health systems will require appropriate knowledge translations and future prospective studies.
And they add the following ket points:
- The observed therapeutic effects following scraping therapy may be a physiological response to the minor bruising.
- Scraping is assumed to be a mechanical signal to elicit the immune function of the skin.
- Through natural resolving of the scraping marks (petechiae) a cascade of physiological responses are generated.
- Counterirritation and placebo effect can also contribute to positive effects for symptom relief.
I think that this paper is a good example for highlighting a common misunderstanding in so-called alternative medicine (SCAM): the confusion about how and whether any given therapy might work.
It is in my view utterly irrelevant, to consider or investigate the mechanisms of action of a SCAM that has not been proven to be an effective treatment of a disease or symptom. Such an approach can only lead to confusion about the value of the SCAM in question. In the present case, it makes gua sha look almost like a reasonable therapy, and consumers who read the paper might conclude that gua sha is worth trying.
A deliberately exaggerated example might make this clearer: If I fall down the staircase, a multitude of physiological effects of the fall could easily be verified on my body. Yet, nobody would claim that throwing patients down the stairs is of therapeutic value. Likewise, the forceful scratching of the skin is bound to have all sorts of physiological effects. These are, however, totally irrelevant until someone has shown that the procedure also has therapeutic value.
To put it bluntly: who cares how a SCAM works when it is unproven that it works?
Muscular dystrophies are a rare, severe, and genetically inherited disorders characterized by progressive loss of muscle fibers, leading to muscle weakness. The current treatment includes the use of steroids to slow muscle deterioration by dampening the inflammatory response. Chinese herbal medicine (CHM) has been offered as adjunctive therapy in Taiwan’s medical healthcare plan, making it possible to track CHM usage in patients with muscular dystrophies. This investigation explored the long-term effects of CHM use on the overall mortality of patients with muscular dystrophies.
A total of 581 patients with muscular dystrophies were identified from the database of Registry for Catastrophic Illness Patients in Taiwan. Among them, 80 and 201 patients were CHM users and non-CHM users, respectively. Compared to non-CHM users, there were more female patients, more comorbidities, including chronic pulmonary disease and peptic ulcer disease in the CHM user group. After adjusting for age, sex, use of CHM, and comorbidities, patients with prednisolone usage exhibited a lower risk of overall mortality than those who did not use prednisolone. CHM users showed a lower risk of overall mortality after adjusting for age, sex, prednisolone use, and comorbidities. The cumulative incidence of the overall survival was significantly higher in CHM users. One main CHM cluster was commonly used to treat patients with muscular dystrophies; it included Yin-Qiao-San, Ban-Xia-Bai-Zhu-Tian-Ma-Tang, Zhi-Ke (Citrus aurantium L.), Yu-Xing-Cao (Houttuynia cordata Thunb.), Che-Qian-Zi (Plantago asiatica L.), and Da-Huang (Rheum palmatum L.).
The authors concluded that the data suggest that adjunctive therapy with CHM may help to reduce the overall mortality among patients with muscular dystrophies. The identification of the CHM cluster allows us to narrow down the key active compounds and may enable future therapeutic developments and clinical trial designs to improve overall survival in these patients.
I disagree!
What the authors have shown is a CORRELATION, and from that, they draw conclusions implying CAUSATION. This is such a fundamental error that one has to wonder why a respected journal let it go past.
A likely causative explanation of the findings is that the CHM group of patients differed in respect to features that the statistical evaluations could not control for. Statisticians can never control for factors that have not been measured and are thus unknown. A possibility in the present case is that these patients had adopted a different lifestyle together with employing CHM which, in turn, resulted in a longer survival.
As we have discussed ad nauseam on this blog, spinal manipulation therapy (SMT) can cause serious adverse events, including spinal epidural hematoma (SEH), an emergency that can cause severe neurological dysfunction. Chinese surgeons have reported three cases of SEH after SMT.
- The first case was a 30-year-old woman who experienced neck pain and numbness in both upper limbs immediately after SMT. Her symptoms persisted after 3 d of conservative treatment, and she was admitted to our hospital. Magnetic resonance imaging (MRI) demonstrated an SEH, extending from C6 to C7.
- The second case was a 55-year-old man with sudden back pain 1 d after SMT, numbness in both lower limbs, an inability to stand or walk, and difficulty urinating. MRI revealed an SEH, extending from T1 to T3.
- The third case was a 28-year-old man who suddenly developed symptoms of numbness in both lower limbs 4 h after SMT. He was unable to stand or walk and experienced mild back pain. MRI revealed an SEH, extending from T1 to T2.
All three patients underwent surgery after failed conservative treatment. Blood clots were found during the operation in case 1 and case 2, and the postoperative pathology confirmed a hematoma. In case three, a vein ruptured during the operation, causing massive bleeding. The three patients recovered to ASIA grade E on day 5, 1 wk, and day 10 after surgery, respectively. All patients returned to normal after 3 mo of follow-up.
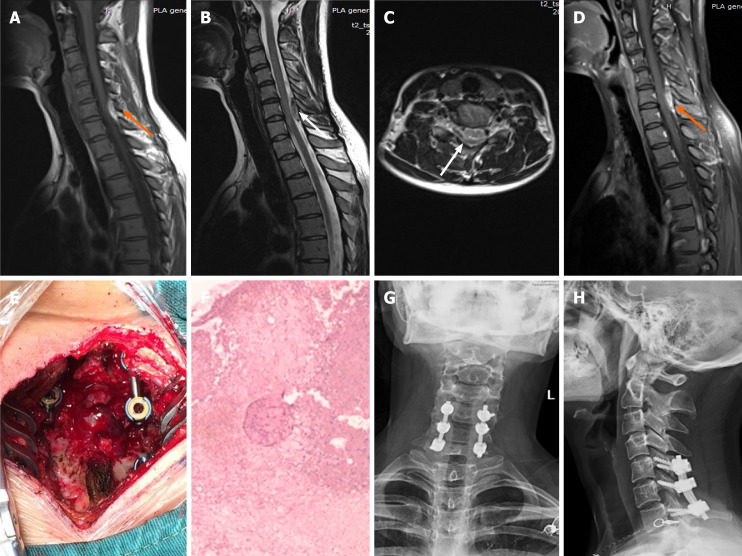
Imaging examinations of case 1. A: T1-weighted preoperative magnetic resonance imaging (MRI) image shows high signal intensity (orange arrow); B and C: Preoperative T2-weighted image shows low signal intensity, and an axial T2-weighted image demonstrates that the hematoma occurred in the posterior region (white arrow); D: Preoperative enhanced MRI suggests an enhanced hematoma signal (orange arrow); E: Intraoperative photograph shows that spinal cord compression has recovered; F: Postoperative pathology suggested a hematoma; G and H: X-ray at the 3-mo follow-up indicated intact internal fixation.
The authors concluded that before proceeding with SMT, each patient should be evaluated in detail and checked for risk factors. In cases where the physical condition changes rapidly, physicians should be alert to the danger and send the patient to the emergency department for a complete MRI examination. We recommend surgery if neurological symptoms appear.
In their paper, the authors also review 15 further cases of SEH that have been previously published. They stress several times in their article that this complication is rare. In my view, this begs the question: how do they know? As there is no post-marketing surveillance of chiropractors or other clinicians doing SMT, I would insist that nobody can be sure about the true incidence of SEH or any other complication after SMT.
Therapeutic touch (TT) is a form of paranormal or energy healing developed by Dora Kunz (1904-1999), a psychic and alternative practitioner, in collaboration with Dolores Krieger, a professor of nursing. TT is popular and practised predominantly by US nurses; it is currently being taught in more than 80 colleges and universities in the U.S., and in more than seventy countries. According to one TT-organisation, TT is a holistic, evidence-based therapy that incorporates the intentional and compassionate use of universal energy to promote balance and well-being. It is a consciously directed process of energy exchange during which the practitioner uses the hands as a focus to facilitate the process.
The question is: does TT work beyond a placebo effect?
This review synthesized recent (January 2009–June 2020) investigations on the effectiveness and safety of therapeutic touch (TT) as a therapy in clinical health applications. A rapid evidence assessment (REA) approach was used to review recent TT research adopting PRISMA 2009 guidelines. CINAHL, PubMed, MEDLINE, Cochrane databases, Web of Science, PsychINFO, and Google Scholar were screened between January 2009-March 2020 for studies exploring TT therapies as an intervention. The main outcome measures were for pain, anxiety, sleep, nausea, and functional improvement.
Twenty-one studies covering a range of clinical issues were identified, including 15 randomized controlled trials, four quasi-experimental studies, one chart review study, and one mixed-methods study including 1,302 patients. Eighteen of the studies reported positive outcomes. Only four exhibited a low risk of bias. All others had serious methodological flaws, bias issues, were statistically underpowered, and scored as low-quality studies. Over 70% of the included studies scored the lowest score possible on the GSRS weight of evidence scale. No high-quality evidence was found for any of the benefits claimed.
The authors drew the following conclusions:
After 45 years of study, scientific evidence of the value of TT as a complementary intervention in the management of any condition still remains immature and inconclusive:
- Given the mixed result, lack of replication, overall research quality and significant issues of bias identified, there currently exists no good quality evidence that supports the implementation of TT as an evidence‐based clinical intervention in any context.
- Research over the past decade exhibits the same issues as earlier work, with highly diverse poor quality unreplicated studies mainly published in alternative health media.
- As the nature of human biofield energy remains undemonstrated, and that no quality scientific work has established any clinically significant effect, more plausible explanations of the reported benefits are from wishful thinking and use of an elaborate theatrical placebo.
TT turns out to be a prime example of a so-called alternative medicine (SCAM) that enthusiastic amateurs, who wanted to prove TT’s effectiveness, have submitted to multiple trials. Thus the literature is littered with positive but unreliable studies. This phenomenon can create the impression – particularly to TT fans – that the treatment works.
This course of events shows in an exemplary fashion that research is not always something that creates progress. In fact, poor research often has the opposite effect. Eventually, a proper scientific analysis is required to put the record straight (the findings of which enthusiasts are unlikely to accept).
In view of all this, and considering the utter implausibility of TT, it seems an unethical waste of resources to continue researching the subject. Similarly, continuing to use TT in clinical settings is unethical and potentially dangerous.
A second look at old research suggested that the recommended dose for vitamin C is far too low. Here is the abstract of the recently published paper:
A double-blind controlled trial initiated in 1944 has led to the common narrative that a 10-mg daily vitamin C intake is adequate to prevent and treat impaired wound healing, and by inference, other collagen-related diseases such as heart disease or stroke. The WHO relies on this narrative to set the recommended nutrient intake for vitamin C. This narrative, however, is based on what is known as the eyeball method of data assessment. The 1944 trial published individual participant data on scar strength providing an opportunity to statistically probe the validity of the 10-mg narrative, something which has not yet been done. The findings show that a vitamin C intake that averages to 10 mg/d over a mean follow-up of 11.5 mo was associated with a 42% weakened scar strength when compared with 80 mg vitamin C intake/d (P < 0.001). The observed dose-response curve between scar strength and vitamin C intake suggests that the daily vitamin C intake needed to prevent collagen-related pathologies is in the range recommended by the National Academy of Medicine and the European Food Safety Authority (75 to 110 mg/d), not the WHO recommendation (45 mg/d). The findings also show that a vitamin C intake that averages to 65 mg/d over a mean follow-up of 6.5 mo failed to restore the normal wound-healing capacity of vitamin C-depleted tissues; such tissues had a 49% weaker scar strength when compared with nondepleted tissues (P < 0.05). Thus, average daily vitamin C intakes ∼50% higher than the WHO recommends may fail to treat existing collagen-related pathologies. It is concluded that the prior lack of statistical analyses of a landmark trial may have led to a misleading narrative on the vitamin C needs for the prevention and treatment of collagen-related pathologies.
The lead author of the recent re-analysis, Professor Philippe Hujoel from the Department of Epidemiology, School of Public Health, University of Washington, Seattle, said: “The vitamin C experiment is a shocking study. They depleted people’s vitamin C levels long-term and created life-threatening emergencies. It would never fly now. The findings of the re-analyses of the Sorby data suggest that the WHO’s recommendation is too low to prevent weak scar strength. Robust parametric analyses of the trial data reveal that an average daily vitamin C intake of 95mg is required to prevent weak scar strength for 97.5 percent of the population. Such a vitamin C intake is more than double the daily 45mg vitamin C intake recommended by the WHO but is consistent with the writing panels for the National Academy of Medicine and (other) countries.”
The original research of 1944 was headed by the British-German biologist and Nobel-prize winner Sir Hans Adolf Krebs. At the time, researchers conducted an experiment that controlled and monitored vitamin C consumption of just 20 volunteers. They were each given varying amounts of vitamin C, which helps the body to produce collagen – and given wounds to observe how quickly their scar tissue healed. The research aimed to ascertain how much vitamin C navy members living off rations is required in order to prevent them from developing scurvy, rather than how much is needed to boost health overall.
Prof Hujoel concluded that: “The failure to reevaluate the data of a landmark trial with novel statistical methods as they became available may have led to a misleading narrative on the vitamin C needs for the prevention and treatment of collagen-related pathologies.”