chiropractic
The McTimoney College of Chiropractic just announced that it has established a new four-year program in veterinary chiropractic for college students:
It means that those without a prior degree can undertake the training and education necessary to enter this coveted career. To date, animal chiropractors were required to have a prior qualification in human chiropractic or a degree in the relevant sciences.
Applications for the new program are being accepted from September 2023. Students will attend Abingdon-based University, Oxford, and a variety of practical locations, enabling the development of academic knowledge and the application of practical skills together . Modules include anatomy and physiology, veterinary science, practice and professionalism, and clinical skills, with a research dissertation running over the four-year course.
University director Christina Cunliffe said the new program was an exciting step in the development of chiropractic care for animals.
“Building on our decades of experience graduating confident, competent, and highly-skilled animal chiropractors, now is the time to open up this exciting career opportunity to college students.”
For the past 50 years, McTimoney College of Chiropractic has been training and educating human chiropractors to the highest regulatory standards. Over the past 20 years, animal chiropractic has developed to meet the requirements for this gentle, holistic treatment in the veterinary world.
Prospective students are invited to a Open House at McTimoney College of Chiropractic in Abingdon on February 16.
McTimoney Chiropractic for Animals identifies areas of stiffness, asymmetry, and poor range of motion within the skeletal system, particularly the spine and pelvis. This affects the muscles that surround these structures, as well as the nerve impulses that pass from the central nervous system to the periphery of the body. The adjustments are very light and fast, stimulating an instant response in the affected soft tissues and joints, promoting relaxation of muscle spasms, improving nerve function, and helping the skeletal structure regain better symmetry and movement again.
In many cases, animals suffer from underlying conditions such as arthritic changes or degenerative diseases that force them to compensate in their posture and movement in an attempt to remain comfortable. However, these offsets become increasingly entrenched and can be painful or uncomfortable, requiring chiropractic care to provide some relief. In other cases, the animals are working hard or competing and as such accumulate tension and asymmetries due to the demands of their work. Once again, chiropractic care helps relieve pain and promote performance, whether it’s faster speeds over hurdles for racehorses and events, better jumping style in showjumpers, or more extravagant movements for dressage stars.
Two recent graduates of the school’s Master of Animal Handling (Chiropractic) program did not hesitate to recommend the university. Natalie McQuiggan said that she had wanted to do McTimoney Chiropractic from a very young age, “but the process of doing it always seemed really daunting.
“But from the start, the staff and teachers were lovely and welcoming, and queries were answered promptly. I have really enjoyed my two years in the Master of Animal Handling (Chiropractic) program and would recommend anyone thinking of doing it to just do it.”
Pollyanna Fitzgerald said the university offered a supportive and welcoming learning environment, allowing her to grow and develop as a student and future professional. “There is always someone to talk to and offer encouragement when needed. As a student I have learned a lot and have been encouraged to believe in myself and it has been a wonderful place to learn.”
A free webinar, McTimoney’s Animal Chiropractic as a Careeron January 24 at 7:30 p.m. (GMT), is open to those who wish to learn more about the McTimoney technique and its application, and the training paths available to those interested in becoming a McTimoney Animal Chiropractor.
________________________
I think this announcement is puzzling on several levels:
- I was unable to find an ‘Abingdon-based University, Oxford’; could it be this institution that is a college and not a university?
- Christina Cunliffe seems to be (or has been?) affiliated with the McTimoney College of Chiropractic which is a bit odd, in my opinion.
- The college does not have ‘decades of experience’; it was founded only in 2001.
- Most importantly, I am unable to find a jot of good evidence that veterinary chiropractic is effective for any condition (see also here, here, and here). In case anyone is aware of any, please let me know. I’d be delighted to revise my judgment.
If I am right, the new course could be a fine example of quackademia where students are ripped off and taught to later rip off the owners of animals after the academically trained quacks have mistreated them.
In case you have categorized Harry Windsor as an ungrateful brat, you are entirely wrong! He did thank a lot of people – Ophra and Gwyneth Paltrow, for instance. No, I did not read Harry’s bestseller ‘SPARE’. But I did, of course, read the odd report about it simply because it is almost impossible to escape the current press hoo-ha about it.
Most of what I learned is of no interest to me. Some of it, I have to admit, made me concerned about Hary’s wellbeing – after all, we know that chronic drug-taking can severely affect one’s mental health! However, one recent article in Newsweek managed to reassure me on that score:
Among the “professionals, medical experts, and coaches” thanked by the prince for “keeping me physically and mentally strong over the years,” is John Amaral, a Los Angeles-based chiropractor, energy practitioner, author and educator. Amaral is known for his self-developed “energy flow formula,” which combines body and energy work to include mindfulness, meditation and breathing.
This sounded sufficiently relevant for me to look up Amaral. This is what we learn from one website:
Dr. John Amaral is a holistic chiropractor that practices Network Spinal (NSA). This technique helps people release stored tension in their muscles and joints through gentle force adjustments, also known as entrainments. Instead of the traditional cracking or popping of bones that you’re used to seeing at chiropractic offices, John Amaral leverages different energetic intelligences to help people heal physically and emotionally.
Another source tells us the following:
John Amaral is a chiropractor, energy healer and educator who works behind the scenes helping celebrities, entrepreneurs, pro athletes and influencers elevate their energy so they feel and perform their best. John has worked with thousands of people from over 50 countries. He is the Founder of Body Centered Leadership… How much do his sessions cost? According to the Wall Street Journal, a healing session with Amaral will run you $2,500.
And a third website informs us that:
Amaral works with what he calls the “subtle energy body”, which is the energy field around the body that can extend around 3 to 8 feet from the physical body. His work is primarily focused on shifting the tension state of the body and help in freeing up bound-up energy that’s held in different parts of the body. He accesses the energy around the body to achieve this.
In case you have not yet got the drift, take a look at this video; impressive isn’t it?
Yes, Amaral is not cheap but he must be worth it! And because he is such a genial healer, I am confident that we can all relax now knowing that Harry’s health is in such good hands. Personally, I am thrilled by Harry’s hint that there might be a second book in the offing – one with the really dirty linen. I think I might actually buy that one, now that I know how badly he needs the money for keeping healthy.
You, the readers of this blog, have spoken!
The WORST PAPER OF 2022 competition has concluded with a fairly clear winner.
To fill in those new to all this: over the last year, I selected articles that struck me as being of particularly poor quality. I then published them with my comments on this blog. In this way, we ended up with 10 papers, and you had the chance to nominate the one that, in your view, stood out as the worst. Votes came in via comments to my last post about the competition and via emails directly to me. A simple count identified the winner.
It is PAUL VARNAS, DC, a graduate of the National College of Chiropractic, US. He is the author of several books and has taught nutrition at the National University of Health Sciences. His award-winning paper is entitled “What is the goal of science? ‘Scientific’ has been co-opted, but science is on the side of chiropractic“. In my view, it is a worthy winner of the award (the runner-up was entry No 10). Here are a few memorable quotes directly from Paul’s article:
- Most of what chiropractors do in natural health care is scientific; it just has not been proven in a laboratory at the level we would like.
- In many ways we are more scientific than traditional medicine because we keep an open mind and study our observations.
- Traditional medicine fails to be scientific because it ignores clinical observations out of hand.
- When you think about it, in natural health care we are much better at utilizing the scientific process than traditional medicine.
But I am surely doing Paul an injustice. To appreciate his article, please read his article in full.
I am especially pleased that this award goes to a chiropractor who informs us about the value of science and research. The two research questions that undoubtedly need answering more urgently than any other in the realm of chiropractic relate to the therapeutic effectiveness and risks of chiropractic. I just had a quick look in Medline and found an almost complete absence of research from 2022 into these two issues. This, I believe, makes the award for the WORST PAPER OF 2022 all the more meaningful.
PS
Yesterday, I wrote to Paul informing him about the good news (as yet, no reply). Once he provides me with a postal address, I will send him a copy of my recent book on chiropractic as his well-earned prize. I have also invited him to contribute a guest post to this blog. Watch this space!
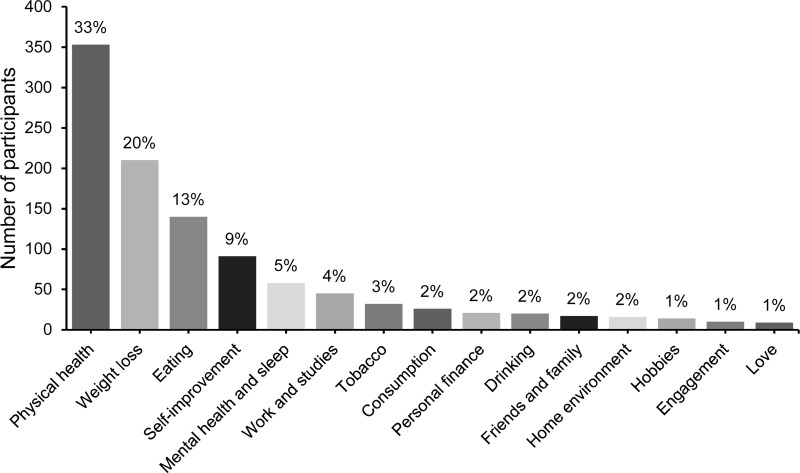
In 2020, a Swedish team published a study investigating what resolutions people make when they are free to formulate them, whether different resolutions reach differing success rates, and whether it is possible to increase the likelihood of a resolution’s success by administering information and exercises on effective goal setting. Participants (N = 1066) from the general public were randomized into three groups:
- active control,
- some support,
- and extended support.
The most popular resolutions regarded physical health, weight loss, and eating habits. At a one-year follow-up, 55% of responders considered themselves successful in sustaining their resolutions. Participants with approach-oriented goals were significantly more successful than those with avoidance-oriented goals (58.9% vs. 47.1%). The group that received some support was exclusively and significantly more successful compared to the other two.
The authors concluded that New Year’s resolutions can have lasting effects, even at a one-year follow-up.
This is a truly interesting study generating a lot of truly boring resolutions.
Boring is, however, something that we must avoid on this blog. In an attempt of doing just this, I decided to lodge my tongue in my cheek and formulate my very own resolutions for 2023 in relation to so-called alternative medicine (SCAM) and this blog. I shall:
- Never again call a comment or a commentator idiotic.
- Never state that chiropractors, homeopaths, osteopaths, naturopaths, or other SCAM practitioners are unethical charlatans.
- Never claim that subluxations, meridians, vital forces, etc. are pure fantasy.
- Never suggest that the assumptions of homeopathy fly in the face of science.
- Never imply that holism, integrative medicine, etc. are just sales gimmicks for crooks to boost their businesses.
- Never again demonstrate that a study is fraudulent just because its findings are too good to be true.
- Never again utter a critical word about our SCAM-loving sovereign, King Charles.
In case you are puzzled by my resolutions, please consider this: contrary to the above-cited evidence, it has been shown that only 12% of people who make new year’s resolutions will actually keep them. And this brings me to my last (and only realistic) resolution for 2023:
8. I shall not feel tempted to adhere to my New Year’s resolutions.
The purpose of this review was to
- identify and map the available evidence regarding the effectiveness and harms of spinal manipulation and mobilisation for infants, children and adolescents with a broad range of conditions;
- identify and synthesise policies, regulations, position statements and practice guidelines informing their clinical use.
Two reviewers independently screened and selected the studies, extracted key findings and assessed the methodological quality of included papers. A descriptive synthesis of reported findings was undertaken using a level-of-evidence approach.
Eighty-seven articles were included. Their methodological quality varied. Spinal manipulation and mobilisation are being utilised clinically by a variety of health professionals to manage paediatric populations with 
- adolescent idiopathic scoliosis (AIS),
- asthma,
- attention deficit hyperactivity disorder (ADHD),
- autism spectrum disorder (ASD),
- back/neck pain,
- breastfeeding difficulties,
- cerebral palsy (CP),
- dysfunctional voiding,
- excessive crying,
- headaches,
- infantile colic,
- kinetic imbalances due to suboccipital strain (KISS),
- nocturnal enuresis,
- otitis media,
- torticollis,
- plagiocephaly.
The descriptive synthesis revealed: no evidence to explicitly support the effectiveness of spinal manipulation or mobilisation for any condition in paediatric populations. Mild transient symptoms were commonly described in randomised controlled trials and on occasion, moderate-to-severe adverse events were reported in systematic reviews of randomised controlled trials and other lower-quality studies. There was strong to very strong evidence for ‘no significant effect’ of spinal manipulation for managing
- asthma (pulmonary function),
- headache,
- nocturnal enuresis.
There was inconclusive or insufficient evidence for all other conditions explored. There is insufficient evidence to draw conclusions regarding spinal mobilisation to treat paediatric populations with any condition.
The authors concluded that, whilst some individual high-quality studies demonstrate positive results for some conditions, our descriptive synthesis of the collective findings does not provide support for spinal manipulation or mobilisation in paediatric populations for any condition. Increased reporting of adverse events is required to determine true risks. Randomised controlled trials examining effectiveness of spinal manipulation and mobilisation in paediatric populations are warranted.
Perhaps the most important findings of this review relate to safety. They confirm (yet again) that there is only limited reporting of adverse events in this body of research. Six reviews, eight RCTs and five other studies made no mention of adverse events or harms associated with spinal manipulation. This, in my view, amounts to scientific misconduct. Four systematic reviews focused specifically on adverse events and harms. They revealed that adverse events ranged from mild to severe and even death.
In terms of therapeutic benefit, the review confirms the findings from the previous research, e.g.:
- Green et al (Green S, McDonald S, Murano M, Miyoung C, Brennan S. Systematic review of spinal manipulation in children: review prepared by Cochrane Australia for Safer Care Victoria. Melbourne, Victoria: Victorian Government 2019. p. 1–67.) explored the effectiveness and safety of spinal manipulation and showed that spinal manipulation should – due to a lack of evidence and potential risk of harm – be recommended as a treatment of headache, asthma, otitis media, cerebral palsy, hyperactivity disorders or torticollis.
- Cote et al showed that evidence is lacking to support the use of spinal manipulation to treat non-musculoskeletal disorders.
In terms of risk/benefit balance, the conclusion could thus not be clearer: no matter whether chiropractors, osteopaths, physiotherapists, or any other healthcare professionals propose to manipulate the spine of your child, DON’T LET THEM DO IT!
This double-blind, randomized study assessed the effectiveness of physiotherapy instrument mobilization (PIM) in patients with low back pain (LBP) and compared it with the effectiveness of manual mobilization.
Thirty-two participants with LBP were randomly assigned to one of two groups:
- The PIM group received lumbar mobilization using an activator instrument, stabilization exercises, and education.
- The manual group received lumbar mobilization using a pisiform grip, stabilization exercises, and education.
Both groups had 4 treatment sessions over 2-3 weeks. The following outcomes were measured before the intervention, and after the first and fourth sessions:
- Numeric Pain Rating Scale (NPRS),
- Oswestry Disability Index (ODI) scale,
- Pressure pain threshold (PPT),
- lumbar spine range of motion (ROM),
- lumbar multifidus muscle activation.
There were no differences between the PIM and manual groups in any outcome measures. However, over the period of study, there were improvements in both groups in NPRS (PIM: 3.23, Manual: 3.64 points), ODI (PIM: 17.34%, Manual: 14.23%), PPT (PIM: ⩽ 1.25, Manual: ⩽ 0.85 kg.cm2), lumbar spine ROM (PIM: ⩽ 9.49∘, Manual: ⩽ 0.88∘), and/or lumbar multifidus muscle activation (percentage thickness change: PIM: ⩽ 4.71, Manual: ⩽ 4.74 cm; activation ratio: PIM: ⩽ 1.17, Manual: ⩽ 1.15 cm).
The authors concluded that both methods of lumbar spine mobilization demonstrated comparable improvements in pain and disability in patients with LBP, with neither method exhibiting superiority over the other.
If this conclusion is meant to tell us that both treatments were equally effective, I beg to differ. The improvements documented here are consistent with improvements caused by the natural history of the condition, regression towards the mean, and placebo effects. The data do not prove that they are due to the treatments. On the contrary, they seem to imply that patients get better no matter what therapy is used. Thus, I feel that the results are entirely in keeping with the hypothesis that spinal mobilization is a placebo treatment.
So, allow me to re-phrase the authors’ conclusion as follows:
Lumbar mobilizations do not seem to have specific therapeutic effects and might therefore be considered to be ineffective for LBP.
The aim of this evaluator-blinded randomized clinical trial was to determine if manual therapy added to a therapeutic exercise program produced greater improvements than a sham manual therapy added to the same exercise program in patients with non-specific shoulder pain. 
Forty-five subjects were randomly allocated into one of three groups:
- manual therapy (glenohumeral mobilization technique and rib-cage technique);
- thoracic sham manual therapy (glenohumeral mobilization technique and rib-cage sham technique);
- sham manual therapy (sham glenohumeral mobilization technique and rib-cage sham technique).
All groups also received a therapeutic exercise program. Pain intensity, disability, and pain-free active shoulder range of motion were measured post-treatment and at 4-week and 12-week follow-ups. Mixed-model analyses of variance and post hoc pairwise comparisons with Bonferroni corrections were constructed for the analysis of the outcome measures.
All groups reported improved pain intensity, disability, and pain-free active shoulder range of motion. However, there were no between-group differences in these outcome measures.
The authors concluded that the addition of the manual therapy techniques applied in the present study to a therapeutic exercise protocol did not seem to add benefits to the management of subjects with non-specific shoulder pain.
What does that mean?
I think it means that the improvements observed in this study were due to 1) exercise and 2) a range of non-specific effects, and that they were not due to the manual techniques tested.
I cannot say that I find this enormously surprising. But I would also find it unsurprising if fans of these methods would claim that the results show that the physios applied the techniques not correctly.
In any case, I feel this is an interesting study, not least because of its use of sham therapy. But I somehow doubt that the patients were unable to distinguish sham from verum. If so, the study was not patient-blind which obviously is difficult to achieve with manual treatments.
This systematic review, meta-analysis, and meta-regression investigated the effects of individualized interventions, based on exercise alone or combined with psychological treatment, on pain intensity and disability in patients with chronic non-specific low-back pain.
Databases were searched up to January 31, 2022, to retrieve respective randomized clinical trials of individualized and/or personalized and/or stratified exercise interventions with or without psychological treatment compared to any control.
The findings show:
- Fifty-eight studies (n = 10084) were included. At short-term follow-up (12 weeks), low-certainty evidence for pain intensity (SMD -0.28 [95%CI -0.42 to -0.14]) and very low-certainty evidence for disability (-0.17 [-0.31 to -0.02]) indicates superior effects of individualized versus active exercises, and very low-certainty evidence for pain intensity (-0.40; [-0.58 to -0.22])), but not (low-certainty evidence) for disability (-0.18; [-0.22 to 0.01]) compared to passive controls.
- At long-term follow-up (1 year), moderate-certainty evidence for pain intensity (-0.14 [-0.22 to -0.07]) and disability (-0.20 [-0.30 to -0.10]) indicates effects versus passive controls.
Sensitivity analyses indicate that the effects on pain, but not on disability (always short-term and versus active treatments) were robust. Pain reduction caused by individualized exercise treatments in combination with psychological interventions (in particular behavioral-cognitive therapies) (-0.28 [-0.42 to -0.14], low certainty) is of clinical importance.
The certainty of the evidence was downgraded mainly due to evidence of risk of bias, publication bias, and inconsistency that could not be explained. Individualized exercise can treat pain and disability in chronic non-specific low-back pain. The effects in the short term are of clinical importance (relative differences versus active 38% and versus passive interventions 77%), especially in regard to the little extra effort to individualize exercise. Sub-group analysis suggests a combination of individualized exercise (especially motor-control-based treatments) with behavioral therapy interventions to boost effects.
The authors concluded that the relative benefit of individualized exercise therapy on chronic low back pain compared to other active treatments is approximately 38% which is of clinical importance. Still, sustainability of effects (> 12 months) is doubtable. As individualization in exercise therapies is easy to implement, its use should be considered.
Johannes Fleckenstein, the 1st author from the Goethe-University Frankfurt, Institute of Sports Sciences, Department of Sports Medicine and Exercise Physiology, sees in the study “an urgent health policy appeal” to strengthen combined services in care and remuneration. “Compared to other countries, such as the USA, we are in a relatively good position in Germany. For example, we have a lower prescription of strong narcotics such as opiates. But the rate of unnecessary X-ray examinations, which incidentally can also contribute to the chronicity of pain, or inaccurate surgical indications is still very high.”
Personally, I find the findings of this paper rather unsurprising. As a clinician, many years ago, prescribing exercise therapy for low back pain was my daily bread. None of my team would have ever conceived the idea that exercise does not need to be individualized according to the needs and capabilities of each patient. Therefore, I suggest rephrasing the last sentence of the conclusion: As individualization in exercise therapies is easy to implement, its use should be standard procedure.
I was fascinated to find a chiropractor who proudly listed ‘the most common conditions chiropractors help kids with‘:
- Vision problems
- Skin conditions
- Bedwetting
- Sinus problems
- ADD/ADHD
- Stomachaches
- Asthma
- Allergies
- Loss of hearing
- Ear Infections
- Hip, leg, or foot pain
- Constipation
- Poor coordination
- Breastfeeding difficulties
- Arm, hand, or shoulder pain
- Anxiety and nervousness
- Colic
- Scoliosis
The birth process, even under normal conditions, is frequently the first cause of spinal stress. After the head of the child appears, the physician grabs the baby’s head and twists it around in a figure eight motion, lifting it up to receive the lower shoulder and then down to receive the upper shoulder. This creates significant stress on the spine of the baby.
“Spinal cord and brain stem traumas often occur during the process of birth but frequently escape diagnosis. Infants often experience lasting neurological defects. Spinal trauma at birth is essentially attributed to longitudinal traction, especially when this force is combined with flexion and torsion of the spinal axis during delivery.” ~Abraham Towbin, MD
Growth patterns suggest the potential for neurological disorders is most critical from birth to two years of age, as this time is the most dynamic and important phase of postnatal brain development. Over sixty percent of all neurological development occurs after birth in the child’s first year of life. This is why it is so important to bring your child to a local pediatric chiropractor to have them checked and for your child to get a chiropractic adjustment during the first year of their life. Lee Hadley MD states “Subluxation alone is a rational reason for Pediatric Chiropractic care throughout a lifetime from birth.”
As our children continue to grow, the daily stresses can have a negative impact on an ever growing body. During the first few years of life, an infant often falls while learning to walk or can fall while tumbling off a bed or other piece of furniture. Even the seemingly innocent act of playfully tossing babies up in the air and catching them often results in a whiplash-like trauma to the spine, making it essential to get your baby checked by a pediatric chiropractor every stage of his/her development as minor injuries can present as major health concerns down the road if gone uncorrected.
______________________________
On the Internet, similar texts can be found by the hundreds. I am sure that many new parents are sufficiently impressed by them to take their kids to a chiropractor. I have yet to hear of a single case where the chiropractor then checked out the child and concluded: “there is nothing wrong; your baby does not need any therapy.” Chiropractors always find something – not something truly pathological, but something to mislead the parent and to earn some money.
Often the treatment that follows turns out to be a prolonged and thus expensive series of sessions that almost invariably involve manipulating the infant’s fragile and developing spine. There is no compelling evidence that this approach is effective for anything. In addition, there is evidence that it can do harm, sometimes even serious harm.
And that’s the reason why I have mentioned this topic before and intend to continue doing so in the future:
- There is hardly a good reason for adults to consult a chiropractor.
- There is no reason to take a child to a chiropractor.
- There are good reasons for chiropractors to stop treating children.
But let’s be a bit more specific. Let’s deal with the above list of indications on the basis of the reliable evidence:
- Vision problems – no sound evidence that chiropractic manipulations are effective.
- Skin conditions – no sound evidence that chiropractic manipulations are effective.
- Bedwetting – some evidence that chiropractic manipulations are ineffective.
- Sinus problems – no sound evidence that chiropractic manipulations are effective.
- ADD/ADHD – some evidence that chiropractic manipulations are ineffective.
- Stomachaches – no sound evidence that chiropractic manipulations are effective.
- Asthma – some evidence that chiropractic manipulations are ineffective.
- Allergies – no sound evidence that chiropractic manipulations are effective.
- Loss of hearing – no sound evidence that chiropractic manipulations are effective.
- Ear Infections – some evidence that chiropractic manipulations are ineffective.
- Hip, leg, or foot pain – no sound evidence that chiropractic manipulations are effective.
- Constipation – no sound evidence that chiropractic manipulations are effective.
- Poor coordination – no sound evidence that chiropractic manipulations are effective.
- Breastfeeding difficulties – no good evidence that chiropractic manipulations are effective.
- Arm, hand, or shoulder pain – no sound evidence that chiropractic manipulations are effective.
- Anxiety and nervousness – no sound evidence that chiropractic manipulations are effective.
- Colic – some evidence that chiropractic manipulations are ineffective.
- Scoliosis – no sound evidence that chiropractic manipulations are effective.
I rest my case.
One of the numerous conditions chiropractors, osteopaths, and other manual therapists claim to treat effectively is tension-type headache (TTH). For this purpose, they (in particular, chiropractors) often use high-velocity, low-amplitude manipulations of the neck. They do so despite the fact that the evidence for these techniques is less than convincing.
This systematic review evaluated the evidence about the effectiveness of manual therapy (MT) on pain intensity, frequency, and impact of pain in individuals with tension-type headache (TTH).
Medline, Embase, Scopus, Web of Science, CENTRAL, and PEDro were searched in June 2020. Randomized clinical trials that applied MT not associated with other interventions for TTH were selected. The level of evidence was synthesized using GRADE, and Standardized Mean Differences (SMD) were calculated for meta-analysis.
Fifteen studies were included with a total sample of 1131 individuals. The analyses show that high-velocity, low-amplitude techniques were not superior to no treatment in reducing pain intensity (SMD = 0.01, low evidence) and frequency (SMD = -0.27, moderate evidence). Soft tissue interventions were superior to no treatment in reducing pain intensity (SMD = -0.86, low evidence) and frequency of pain (SMD = -1.45, low evidence). Dry needling was superior to no treatment in reducing pain intensity (SMD = -5.16, moderate evidence) and frequency (SMD = -2.14, moderate evidence). Soft tissue interventions were not superior to no treatment and other treatments on the impact of headache.
The authors concluded that manual therapy may have positive effects on pain intensity and frequency, but more studies are necessary to strengthen the evidence of the effects of manual therapy on subjects with tension-type headache. Implications for rehabilitation soft tissue interventions and dry needling can be used to improve pain intensity and frequency in patients with tension type headache. High velocity and low amplitude thrust manipulations were not effective for improving pain intensity and frequency in patients with tension type headache. Manual therapy was not effective for improving the impact of headache in patients with tension type headache.
So, this review shows that:
- soft tissue interventions are better than no treatment,
- dry needling is better than no treatment.
These two results fail to impress me. Due to a placebo effect, almost any treatment should be better than no therapy at all.
ALMOST, because high-velocity, low-amplitude techniques were not superior to no treatment in reducing the intensity and frequency of pain. This, I feel, is an important finding that needs an explanation.
As it is only logical that high-velocity, low-amplitude techniques must also produce a positive placebo effect, the finding can only mean that these manipulations also generate a negative effect that is strong enough to cancel the positive response to placebo. (In addition, they can also cause severe complications via arterial dissections, as discussed often on this blog.)
Too complicated?
Perhaps; let me, therefore, put it simply and use the blunt words of a neurologist who once was quoted saying this:
DON’T LET THE BUGGARS TOUCH YOUR NECK!