charlatan
I have written about Bioscan before; for instance here. Now there is more news about the device. In Germany, the manufacturers of Bioscan have been sued and found guilty of fraud.
The two managing directors of the company were sentenced to imprisonment for two and three years respectively and together they have to pay a fine of over 2.5 million euros. The presiding judge considered it proven that the manufacturers had sold useless devices. He said, “A measuring device that measures nothing is about as useful as a car that does not drive.” In addition, a former sales director was sentenced to a fine of 90 daily rates.
The three leading employees of the company were charged with commercial fraud and violations of the Therapeutic Products Advertising Act. The company from Pliezhausen had claimed that their device would measure blood and nutrient values in the body in an uncomplicated way and thus replace a time-consuming laboratory diagnosis.
The Bioscan device consists of two metal rods. You have to take them in your hand, according to the company’s instructions. They would then measure magnetic waves and produce a result. More than 200 medically important health data could allegedly be recorded, for example, cholesterol or testosterone levels. The court had summoned several experts to assess the device. However, they found that the device measured nothing except the current flowing through the cables.
The manufacturers had been doing a huge business with the device for years. The company is said to have earned almost 6 million euros. The devices are still being sold today, for instance, in Austria and Switzerland, among other countries. Despite all the criticism and the court case, the two managing directors had not stopped sales.
________________________
When I googled ‘Bioscan’ yesterday (30/5), the website informed me that:
The BioScan system is an FDA cleared, state of the art testing machine that scans the body’s organs and functions for imbalances using electrodermal screening (EDS).
BioScan SRT
What Is Stress Reduction Testing?
SRT is a remarkable new procedure that combines the disciplines of Acupuncture, Biofeedback and Homeopathy with Laser Light technology. A computerized scan or test is done to see what your body is sensitive to, and how it is out of balance, then help it learn not to be.
Are there any side effects?
No. A small percentage of clients report slight flushing or congestion for a short time (an hour or so) after their session, but this is actually a sign that the body is detoxifying (a good thing)! This process is safe, fast, non-invasive and painless. Unlike skin tests the actual substance is not used, so the body perceives its presence, it as if it were there, but does not act upon it.
What does the BioScan SRT treat?
The BioScan SRT Wellness System does not diagnose or treat any specific condition. Through the use of our FDA-cleared biofeedback technology, the BioScan SRT is able to assess with a very high degree of specificity which substances create increased levels of stress to the body.These specific stress inducing substances are often times what trigger the nervous systems fight or flight reactions which are expressed in a myriad of symptoms that have been scientifically proven to be associated with high levels of stress.
What substances can the BioScan SRT identify as stressors?
The BioScan SRT contains tens of thousands of substances in the main procedure libraries and up to an additional 50,000 substances in the advanced procedure libraries. This technology can identify almost every known substance that could possibly cause a stress reaction.
_________________________
And on the Internet, it takes just a minute to find a Bioscan device for sale. It would set you back by 119.98 Euros.
_________________________
Say no more!
Osteopathic visceral manipulation (VM) is a bizarre so-called alternative medicine (SCAM) that has been featured on this blog with some regularity, e.g.:
- Osteopathic visceral manipulation: a new study fails to convince anyone
- Visceral manipulation…you couldn’t make it up
- Intravaginal manipulations by (German) osteopaths: a new low point for clinical research into alternative medicine?
- Visceral osteopathy is implausible and does not work … SO, LET’S FORGET ABOUT IT ONCE AND FOR ALL
Rigorous trials fail to show that it works for anything. So, the obvious solution to this dilemma is to conduct dodgy trials!
This study tested the effects of VM on dysmenorrhea, irregular, delayed, and/or absent menses, and premenstrual symptoms in PCOS patients.
Thirty Egyptian women with polycystic ovary syndrome (PCOS), with menstruation-related complaints and free from systematic diseases and/or adrenal gland abnormalities, participated in a single-blinded, randomized controlled trial. They were recruited from the women’s health outpatient clinic in the faculty of physical therapy at Cairo University, with an age of 20-34 years, and a body mass index (BMI) ≥25, <30 kg/m2. Patients were randomly allocated into two equal groups (15 patients); the control group received a low-calorie diet for 3 months, and the study group that received the same hypocaloric diet added to VM to the pelvic organs and their related structures for eight sessions over 3 months. Evaluations for body weight, BMI, and menstrual problems were done by weight-height scale, and menstruation-domain of Polycystic Ovary Syndrome Health-Related Quality of Life Questionnaire (PCOSQ), respectively, at baseline and after 3 months from interventions. Data were described as mean, standard deviation, range, and percentage whenever applicable.
Of 60 Egyptian women with PCOS, 30 patients were included, with baseline mean age, weight, BMI, and a menstruation domain score of 27.5 ± 2.2 years, 77.7 ± 4.3 kg, 28.6 ± 0.7 kg/m2, and 3.4 ± 1.0, respectively, for the control group, and 26.2 ± 4.7 years, 74.6 ± 3.5 kg, 28.2 ± 1.1 kg/m2, and 2.9 ± 1.0, respectively, for the study group. Out of the 15 patients in the study group, uterine adhesions were found in 14 patients (93.3%), followed by restricted uterine mobility in 13 patients (86.7%), restricted ovarian/broad ligament mobility (9, 60%), and restricted motility (6, 40%). At baseline, there was no significant difference (p>0.05) in any of the demographics (age, height), or dependent variables (weight, BMI, menstruation domain score) among both groups. Post-study, there was a statistically significant reduction (p=0.000) in weight, and BMI mean values for the diet group (71.2 ± 4.2 kg, and 26.4 ± 0.8 kg/m2, respectively) and the diet + VM group (69.2 ± 3.7 kg; 26.1 ± 0.9 kg/m2, respectively). For the improvement in the menstrual complaints, a significant increase (p<0.05) in the menstruation domain mean score was shown in the diet group (3.9 ± 1.0), and the diet + VM group (4.6 ± 0.5). On comparing both groups post-study, there was a statistically significant improvement (p=0.024) in the severity of menstruation-related problems in favor of the diet + VM group.
The authors concluded that VM yielded greater improvement in menstrual pain, irregularities, and premenstrual symptoms in PCOS patients when added to caloric restriction than utilizing the low-calorie diet alone in treating that condition.
WHERE TO START?
- Tiny sample size.
- A trail design (A+B vs B) which will inevitably generate a positive result.
- Questionable ethics.
VM is a relatively invasive and potentially embarrassing intervention for any woman; I imagine that this is all the more true in Egypt. In such circumstances, it is mandatory to ask whether a planned study is ethically justifiable. I would answer this question related to an implausible treatment like VM with a straight NO!
I realize that there may be people who disagree with me. But even those guys should accept that, at the very minimum, such a study must be designed such that it leads to a clear answer – is VM effective or not? The present trial merely suggests that the placebo effect associated with VM is powerful (which is hardly surprising for a therapy like VM).
I have previously reported about the ‘Havelhöhe Community Hospital’ in Berlin and its medical director, Prof Harald Matthes. He made headlines two years ago when he claimed that anthroposophical remedies were effective for treating COVID. More recently, Matthes made headlines again when he went on TV claiming that serious adverse effects of COVID vaccinations were 40 times more frequent than generally accepted.
Now a German newspaper reports more about the ‘Havelhöhe Community Hospital’ and its medical director. Here are a few (translated) passages from this remarkable article:
At the Havelhöhe Community Hospital in Berlin, there are considerable shortcomings in the handling of the Corona pandemic … basic protective measures are in part neither adhered to nor monitored. In addition, employees of the anthroposophical clinic are recommended a vaccination regimen for which there is no approval, i.e. the option of “dose splitting with frequency increase,” in which the vaccine usually administered at one time is to be divided among several injections.
However, there is no official basis for this vaccination scheme. “There is no vaccine approved for it, and it does not correspond in any way to the Stiko recommendation,” said Gudrun Widders, the public health officer responsible. “My hair stands on end when I hear that,” says the head of the Berlin-Spandau health department, who is also a member of the Standing Commission on Vaccination.
Visitors of the hospital Havelhöhe can enter buildings and wards without control of the inoculation status or a daily updated test result which is against current regulations in Germany. While other Berlin hospitals such as the Charité imposed bans on visitors, a public concert took place at Havelhöhe Hospital, where the audience did not wear a mask, contrary to the valid Corona protection regulation. Employees of the hospital also report to the taz that many of the hospital staff are lax about wearing masks, even when on duty.
“I can only say something when I see someone,” said hospital director Harald Matthes. “And I don’t see anyone with me in the hospital who walks around without a mask.” Matthes had publicly criticized corona measures as excessive on several occasions.
________________________________
I have said it before and I say it again: in my view, Matthes’ behavior amounts to serious professional misconduct. I, therefore, suggest that his professional body, the Aerztekammer, look into it with a view of preventing further harm.
I was alerted to the following conference announcement:
The MEP Interest Group on Integrative Medicine and Health is delighted to invite you to the event ‘Integrative Medicine and Health in prevention and management of COVID-19 and long COVID’ on Thursday 2 June 16.00–18.00 CEST.
This event will give you in-depth information about:
Expert speakers will share their knowledge and insights about how:
• Complementary and Integrative Medicine and Health interventions can improve resilience to COVID-19 infection.
• Promoting resilience and health restoration can reduce the risk of severe COVID-19 or development of Long COVID.
• These interventions can improve the recovery from Long COVID.
Key speakers and topics:
Therapeutic strategies of complementary medicines in the COVID 19 pandemic and Long COVID in addition to conventional medicine
Dr Joanna Dietzel, MD Neurologist, Acupuncturist. Department for integrative & complementary medicine, Institute of social medicine, epidemiology and health economics, Charité – Universitätsmedizin Berlin, Germany.
Chinese herbal medicine treatment in cases of infections with SARS-CoV-2 – therapeutic strategies for COVID-19 and Long COVID
Dr Christian Thede, MD, General practitioner, specialised in Acupuncture and Chinese Medicine. Former lecturer in Chinese medicine, University of Witten-Herdecke, Germany
Instructor for Acupuncture and Chinese Medicine at International Society of Chinese Medicine (SMS).
Traditional and Complementary Medicine contributions to health system resilience during COVID-19 – the WHO perspective
Dr Geetha Kopalakrishna, MD, Bachelor of Ayurvedic Medicine & Surgery
Technical Officer at Traditional, Complementary & Integrative Medicine, Department of Service Delivery and Safety, World Health Organization, Geneva, Switzerland
Key member of the AYUSH-based COVID-19 response Task Force for the Government of India.
Research programme into integrative medicine’s contribution to improving resilience to COVID-19 infection and reducing the risk of severe COVID-19 or development of Long COVID
Dr Helene M. Langevin, Director at National Center for Complementary and Integrative Health, National Institutes of Health, Bethesda, Maryland (MD), USA. Previously, Director of the Harvard Osher Center for Integrative Medicine and professor of medicine at Harvard Medical School, Boston (MA) and professor of neurological sciences at the Larner College of Medicine at the University of Vermont (VT).
Q&A sessions after the presentations.
Resilience to infections: a solution for COVID-19 and other infectious illnesses
Studies show that certain common medical conditions put people at higher risk for severe illness and death from COVID-19. Nearly two-thirds of COVID-19 hospitalizations could be attributed to obesity, diabetes, hypertension, and heart failure. There is increasing awareness that a health system that focuses on improving health could prevent all these conditions to a large extent.
Long COVID
More than 40% of people who have or had COVID-19 get long COVID, and among people who needed hospitalization, the statistics go up to 57%. The recovery from such post viral syndromes will be greatly helped by offering patients access to complementary and integrative medicine interventions that aim at restoring their health balance.
MEP Interest Group on Integrative Medicine and Health
The event is hosted by the members of the MEP Interest Group on Integrative Medicine & Health:
Michèle Rivasi, Greens/EFA, France
Sirpa Pietikäinen, EPP, Finland
Tilly Metz, Greens/EFA, Luxembourg
Margrete Auken, Greens/EFA, Denmark
Romana Jerković, S&D, Croatia
Manuela Ripa, Greens/EFA, Germany
I had not been aware of the ‘MEP Interest Group on Integrative Medicine & Health‘. Therefore, I looked it up and found this:
The newly established Interest Group on Integrative Medicine & Health continues the work of the former MEP Interest Group on CAM. This group brings together MEPs who work collectively to promote the inclusion of CAM as part of Integrative Medicine & Health in all possible European Parliament public health policy.
Why an Interest Group in the European Parliament?
One in two EU citizens uses complementary medicine either alongside or as an alternative to conventional biomedical care. This high demand is not yet reflected in EU or national health policy or provision. In addition, there is diversity in complementary medicine regulation across the EU. There are differences in who can practice complementary medicine, what qualifications are required and how services are offered and financed. These discrepancies mean that citizens experience practical and attitudinal barriers that limit their access to and use of TCIM.
The health sector in the EU Member States is facing considerable challenges, such as antimicrobial resistance (AMR), increasing prevalence of Non-Communicable Diseases (NCDs) and soaring costs. Complementary medicine can offer a significant contribution to meet these challenges. These modalities are “integrative”, offering patient-centered healthcare, based on evidence-informed integration of conventional biomedicine and complementary medicine. Integrative Medicine and Health focuses on the whole person and considers the individual in its physical, psychological, spiritual, social and environmental context. It is inclusive of all professions and practices that use this approach and meets the demand of EU citizens for a more holistic, patient-centered approach in medicine. At the same time, TCIM is at the center of political and scientific debate. In this context, a forum for discussion on Integrative and Complementary Medicine’s contribution to EU health systems will bring clarity and rationality to this debate.
Aims and objectives of the Interest Group on Integrative Medicine & Health
- Establish and maintain a forum for discussion and action with all stakeholders regarding Integrative Medicine and Health.
- Raise awareness of Integrative Medicine and its contribution to more sustainable healthcare systems in the EU and a more holistic approach to health.
- Focus on the integration of complementary modalities into the health systems of the EU Member States.
- Protect and promote citizens’ right to choose their own healthcare while providing access to Integrative Medicine and Health information.
- Advocate for EU involvement in setting unified standards to regulation of Integrative Medicine and Health.
__________________________________
Unified standards? But what about high or perhaps just scientific standards? What about first doing the research and then making claims about CAM or TCIM or however you decide to call it? Has common sense gone out of fashion?
Yes, you guessed it: I am seriously underwhelmed by all this. To show you why, let me list just a few claims from the above two statements that are based purely on wishful thinking:
- Complementary and Integrative Medicine and Health interventions can improve resilience to COVID-19 infection.
- These interventions can improve the recovery from Long COVID.
- Studies show that certain common medical conditions put people at higher risk for severe illness and death from COVID-19.
- The recovery from such post viral syndromes will be greatly helped by offering patients access to complementary and integrative medicine interventions that aim at restoring their health balance.
- One in two EU citizens uses complementary medicine either alongside or as an alternative to conventional biomedical care.
- The health sector in the EU Member States is facing considerable challenges, such as antimicrobial resistance (AMR), increasing prevalence of Non-Communicable Diseases (NCDs) and soaring costs. Complementary medicine can offer a significant contribution to meet these challenges.
- These modalities are “integrative”, offering patient-centered healthcare, based on evidence-informed integration of conventional biomedicine and complementary medicine.
- Integrative medicine … meets the demand of EU citizens for a more holistic, patient-centered approach in medicine.
I find all this confusing and concerning in equal measure. I also seriously doubt that the forum for discussion on Integrative and Complementary Medicine will bring clarity and rationality to this debate. If they really wanted a debate, they would need to include a few critical thinkers; can anyone recognize one on the list of speakers? I cannot!
I fear the aim of the group and their meeting is to mislead us all into thinking that CAM, TCIM, etc. generate more good than harm without ever delivering the evidence for that assumption. Therefore, I suggest they rename both the conference as well as their group:
‘Wishful thinking in prevention and management of COVID-19 and long COVID’
and
MEP Interest Group on Wishful Thinking and Promotion of Quackery
PS
As an antidote to wishful thinking, I recommend reading some proper science papers on the subject. Here are the conclusions of an up-to-date and wishful-thinking-free review on the subject of post-acute infection syndrome:
Unexplained post-acute infection syndromes (PAISs) appear to be an under-recognized feature of a spectrum of infectious diseases in a minority of patients. At present, our understanding of the underlying pathophysiologic mechanisms and etiologic factors is poor and there are no known objective markers or effective therapeutic options. More basic biomedical research is needed. The overlap of symptoms, signs, and general features of the individual PAISs suggests the involvement of shared pathological pathways and the possibility that common diagnostic markers, or even a unified etiological model, might be established.
However, some symptoms or clinical characteristics seem to be trigger-specific or more prevalent in one PAIS than in others, emphasizing the need for cohorts with a well-documented infectious trigger. The overall clinical picture of many PAISs often overlaps with the presentation of post-infectious ME/CFS or fibromyalgia, or resembles other fatiguing, neurological, or rheumatic disorders. Exploiting existing knowledge of these conditions might help guide future scientific discovery and progress in clinical care.
The SARS-CoV-2 pandemic uncovered a significant gap in knowledge about post-acute sequelae of infectious diseases and identified the need for better diagnostic care and clinical infrastructure for patients experiencing these long-term effects. In addition to basic biomedical research, more needs to be done to refine diagnostic criteria and obtain more reliable estimates of the prevalence and societal burden of these disorders to help shape health-policy decisions. Moreover, we call for unified nomenclature and better conceptualization of post-acute infection symptoms.
There is much to be done, but the unprecedented amount of attention and resources that have recently been allocated to the study of COVID-19-related pathology brings a promise of much-needed progress in the wider field of unexplained infection-associated chronic disability.
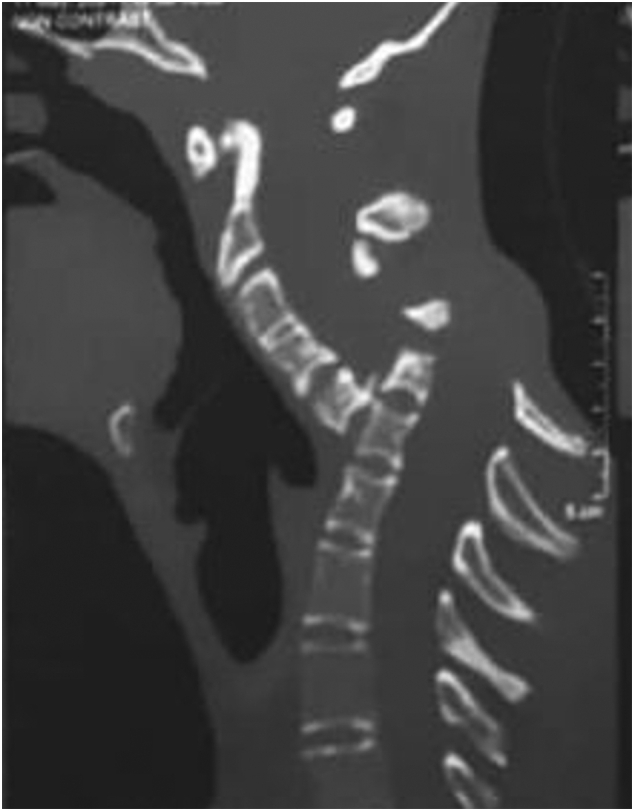
Spondyloptosis is a grade V spondylolisthesis – a vertebra having slipped so far with respect to the vertebra below that the two endplates are no longer congruent. It is usually seen in the lower lumbar spine but rarely can be seen in other spinal regions as well. Spondyloptosis is most commonly caused by trauma. It is defined as the dislocation of the spinal column in which the spondyloptotic vertebral body is either anteriorly or posteriorly displaced (>100%) on the adjacent vertebral body. Only a few cases of cervical spondyloptosis have been reported. The cervical cord injury in most patients is complete and irreversible. In most cases of cervical spondyloptosis, regardless of whether there is a neurologic deficit or not, reduction and stabilization of the fracture-dislocation is the management of choice
The case of a 16-year-old boy was reported who had been diagnosed with spondyloptosis of the cervical spine at the C5-6 level with a neurologic deficit following cervical manipulation by a traditional massage therapist. He could not move his upper and lower extremities, but the sensory and autonomic function was spared. The pre-operative American Spinal Cord Injury Association (ASIA) Score was B with SF-36 at 25%, and Karnofsky’s score was 40%. The patient was disabled and required special care and assistance.

The surgeons performed anterior decompression, cervical corpectomy at the level of C6 and lower part of C5, deformity correction, cage insertion, bone grafting, and stabilization with an anterior cervical plate. The patient’s objective functional score had increased after six months of follow-up and assessed objectively with the ASIA Impairment Scale (AIS) E or (excellent), an SF-36 score of 94%, and a Karnofsky score of 90%. The patient could carry on his regular activity with only minor signs or symptoms of the condition.
The authors concluded that this case report highlights severe complications following cervical manipulation, a summary of the clinical presentation, surgical treatment choices, and a review of the relevant literature. In addition, the sequential improvement of the patient’s functional outcome after surgical correction will be discussed.
This is a dramatic and interesting case. Looking at the above pre-operative CT scan, I am not sure how the patient could have survived. I am also not aware of previous similar cases. This does, however, not mean they don’t exist. Perhaps most affected patients simply died without being diagnosed. So, do we need to add spondyloptosis to the (hopefully) rare but severe complications of spinal manipulation?
A recent article in LE PARISIEN entitled “L’homéopathie vétérinaire, c’est sans effet… mais pas sans risque” – Veterinary homeopathy is without effect … but not without risk, tells it like it is. Here are a few excerpts that I translated for you.
More than 77% of French people have tried homeopathy in their lifetime. But have you ever given it to your pet? Harmless in most cases, its use can be dangerous when it replaces a treatment whose effectiveness is scientifically proven … from a safety point of view, the tiny granules are indeed irreproachable: their use does not induce any drug interaction or undesirable side effects, nor does it run the risk of overdosing or addiction … homeopathic preparations owe their harmlessness to their lack of proper effects. “Neither in human medicine nor in veterinary medicine, at the current stage, clinical studies of all levels do not provide sufficient scientific evidence to support the therapeutic efficacy of homeopathic preparations”, stated the French Veterinary Academy in May 2021. These conclusions are in line with those of the French Academies of Medicine and Pharmacy, the British Royal College of Veterinary Surgeons, and all the international scientific bodies that have given their opinion on the subject.
Therefore, when homeopathy delays diagnosis or is used in place of proven effective treatments, its use represents a “loss of opportunity” for your pet. The greatest danger of homeopathy is not that the remedies are ineffective, but that some homeopaths believe that their therapies can be used as a substitute for genuine medical treatment,” summarizes a petition to the UK veterinary regulatory body signed by more than 1,000 British veterinarians. At best, this claim is misleading and, at worst, it can lead to unnecessary suffering and death.”
But how can we explain the number of testimonies from pet owners who say that “it works”? “I am very satisfied with the Kalium Bichromicum granules for my cat with an eye ulcer, which is healing very well”… These improvements, real or supposed, can be explained by “contextual effects”, among which the famous placebo effect (which is not specific to humans), your subjective interpretation of his symptoms, or the natural history of the disease.
When these contextual effects are ignored or misunderstood, the spontaneous resolution or reduction of the disease can be wrongly attributed to homeopathy, and thus maintain the illusion of its effectiveness. This confusion is all the more likely because homeopathy owes much of its popularity to its use to treat “everyday ailments”: nausea, allergies, fatigue, bruises, nervousness, etc., which tend to get better on their own with time, or which have a fluctuating expression…
In April 2019, the association published an open letter addressed to the National Council of the Order of Veterinarians, calling on it to take a position on the compatibility of homeopathy with the “ethical and scientific requirements” of the profession. The organization, whose official function is to guarantee the quality of the service rendered to the public by the 20,000 veterinarians practicing in France, issued its conclusions last October. It invited veterinary training centers to remove homeopathy from their curricula, under penalty of having their accreditation withdrawn, and thus their ability to deliver training credits.
In my view, this is a remarkably good and informative text. How often do homeopathy fans claim IT WORKS FOR ANIMALS AND THUS CANNOT BE A PLACEBO! The truth is that, as we have so often discussed on this blog, homeopathy does not work beyond placebo for animals. This renders veterinary homeopathy:
- a waste of money,
- potentially dangerous,
- in the worst cases a form of animal abuse.
My advice is that, as soon as a vet recommends homeopathy, you look for the exit.
I was alerted to the following short article from ‘The Blackpool Gazette‘:
Criminals have been using the brand name Pfizer to sell fake homeopathic vaccines to residents, according to police. The white tablets are sold under the pretence that they are an alternative to traditional vaccines, but actually contain no active ingredient. Analysis conducted by Lancashire Police revealed the tablets were nothing more than sugar pills. “Please note Pfizer do not produce any tablets as a cure or prophylactic for COVID-19,” a spokesman for the force added.
Homeopathy is a “treatment” based on the use of highly diluted substances, which practitioners claim can help the body heal itself, according to the NHS. A 2010 House of Commons Science and Technology Committee report on homeopathy said that homeopathic remedies perform no better than placebos. In 2017, NHS England said it would no longer fund homeopathy on the NHS as the lack of any evidence for its effectiveness did not justify the cost. This was backed by a High Court judgement in 2018.
I think there might be a slight misunderstanding here. The homeopathic remedy might not be fake, as it was produced according to the concepts of homeopathy. It is homeopathy itself that is fake. To me, it looks as though we are dealing with the German product I mentioned a while ago. Let me remind you:
Many people believe that homeopathy is essentially plant-based – but they are mistaken! Homeopathic remedies can be made from anything: Berlin wall, X-ray, pus, excrement, dental plaque, mobile phone rays, poisons … anything you can possibly think of. So, why not from vaccines?
This is exactly what a pharmacist specialized in homeopathy thought.
It has been reported that the ‘Schloss-Apotheke’ in Koblenz, Germany offered for sale a homeopathic remedy made from the Pfizer vaccine. This has since prompted not only the Chamber of Pharmacists but also the Paul Ehrlich Institute and Pfizer to issue statements. On Friday (30/4/2021) morning, the pharmacy had advertised homeopathic remedies based on the Pfizer/Biontech vaccine. The Westphalia-Lippe Chamber of Pharmacists then issued an explicit warning against it. “We are stunned by this,” said a spokesman. The offer has since disappeared from the pharmacy’s website.
Pfizer vaccine. This has since prompted not only the Chamber of Pharmacists but also the Paul Ehrlich Institute and Pfizer to issue statements. On Friday (30/4/2021) morning, the pharmacy had advertised homeopathic remedies based on the Pfizer/Biontech vaccine. The Westphalia-Lippe Chamber of Pharmacists then issued an explicit warning against it. “We are stunned by this,” said a spokesman. The offer has since disappeared from the pharmacy’s website.
On Friday afternoon, the manufacturer of the original vaccine also intervened. The Paul Ehrlich Institute released a statement making it clear that a vaccine is only safe “if it is administered in accordance with the marketing authorization.”
The Schloss-Apotheke had advertised the product in question with the following words:
“We have Pfizer/BioNTech Covid-19-Vaccine in potentized form up to D30 as globules or dilution (for discharge) in stock.”
The chamber of pharmacists countered with a warming under the heading “Facts instead of Fake News” on Facebook and Instagram:
“Whatever they might contain: These remedies are no effective protection against Covid-19.”
Pharmacy manager, Annette Eichele, of the Schloss-Apotheke claimed she had not sold homeopathic Corona vaccines and stressed that effective vaccines of this kind do not exist. According to Eichele, only an additional “mini drop” of the original Biontech vaccine had been used and “highly potentized” and prepared homeopathically. According to Eichele, Corona vaccinations that had already been administered were thus to have a “better and more correct effect with this supplementary product, possibly without causing side effects … but this is not scientifically proven”. The homeopathic product had been produced only on customer request and had been sold less than a dozen times in the past weeks. Ten grams of the remedy were sold for about 15 Euros. On Twitter, Eichele stated: „Wir haben nichts Böses getan, wir wollten nur Menschen helfen!“ (We have done nothing evil, we only wanted to help people). I am reminded yet again of Bert Brecht who observed:
“The opposite of good is not evil but good intentions”.
_______________________
If I am right, the remedy is not truly fake but a genuine product of a fake concept, namely homeopathy. In that case, the term ‘criminal’ might need to be applied to homeopathy itself – an interesting thought!
The cardiothoracic surgeon and famous US woo merchant, Dr. Mehmet Oz, is probably known to most readers. I have previously mentioned him several times, for instance, here and here. His institution, Columbia University in New York City, has had many (I’d say too many) years of patience with his relentless promotion of outright and often dangerous quackery. Now it has been reported that the university has finally cut ties with Dr. Oz:
“It took Columbia far too long to remove Oz from its otherwise distinguished medical faculty,” Henry Miller, MD, of the Pacific Research Institute in California, told MedPage Today via email. Miller stressed that “the ‘Oz controversy’ was never about free speech. It was about an unethical grifter whose claims and pronouncements were not supported by science and were injurious to consumers — in the interest of financial benefit to Oz himself. That constitutes professional misconduct.”
The university’s Irving Medical Center quietly ended its relationship with Oz at the end of April, according to The Daily Beast. He had been removed from several pages of the medical center’s website in mid-January. In 2018, Oz’s title had been changed to professor emeritus and special lecturer, according to reports. A spokesperson for Columbia University confirmed the 2018 change in an email to MedPage Today.
In 2015, Miller and colleagues sent a letter to Lee Goldman, MD, MPH, dean of the Faculties of Health Sciences and Medicine at the university, calling for Oz’s expulsion. Oz had “repeatedly shown disdain for science and for evidence-based medicine” and “manifested an egregious lack of integrity by promoting quack treatments and cures in the interest of personal financial gain,” according to Miller’s group…
In 2014, Oz was called to testify before the Senate Subcommittee on Consumer Protection, Product Safety, and Insurance during a hearing on false advertising in the diet and weight-loss industry. Senators grilled Oz regarding statements he made on “The Dr. Oz Show” that promoted green coffee bean extract as a “miracle pill” for weight loss.
But long before that hearing, tensions had built between Oz and the medical community because of his penchant for spouting dubious medical claims on his TV show and in the media. For example, in a 2011 segment, ABC News‘ chief health and medical editor Richard Besser, MD, called out a purported “study” of arsenic in apple juice that Oz conducted for an episode of his show.
Besser charged that Oz’s science was shoddy because he reported total arsenic rather than the breakdown between organic and inorganic arsenic — only the latter of which is known to be toxic. Even the FDA sent the show a letter before the segment aired saying it would be “irresponsible and misleading” to report the results.
Oz again broke with medical science during the pandemic when he touted hydroxychloroquine as a cure for COVID-19, even as evidence mounted that it had no effect on disease course.
Oz is currently running for a U.S. Senate seat in Pennsylvania as a Republican candidate. Former President Trump endorsed Oz, touting Oz’s medical and academic credentials in a statement, according to NPR: “He even said that I was in extraordinary health, which made me like him even more (although he also said I should lose a couple of pounds!).”
__________________________
I have to admit that I find these reports somewhat puzzling. Don’t get me wrong: it’s not that I don’t think Oz deserves to be dismissed. In fact, he had already richly deserved it many years ago. What I find, however, odd is that giving someone the title ’emeritus professor’ can hardly be called ‘cutting ties’ with him. In some ways, it is even the opposite (I should know because I currently have this status).
When I looked up Oz, Columbia listed him as:
Oz, Mehmet C. (MD)
Special Lecturer in the Department of Surgery
Phone: 212.305.4434 · Fax: 212.342.3520
Location: MHB, Rm. 435-62
Similarly, the website of the Irving Medical Center is full of entries about Oz. Confusion is therefore more than justified, I think.
What is needed, I feel, is a clear statement from Columbia University about its relationship with Dr. Oz. Are they still proud of his considerable fame/notoriety, or did they in fact have the integrity to cut ties with one of the most self-aggrandizing woo merchants of all times?
Harad Matthes, the boss of the anthroposophical Krankenhaus Havelhoehe and professor for Integrative and Anthroposophical Medicine at the Charite in Berlin, has featured on my blog before (see here and here). Now he is making headlines again.
‘Die Zeit‘ reported that Matthes went on German TV to claim that the rate of severe adverse effects of COVID-19 vaccinations is about 40 times higher than the official figures indicate. In the MDR broadcast ‘Umschau’ Matthes said that his unpublished data show a rate of 0,8% of severe adverse effects. In an interview, he later confirmed this notion. Yet, the official figures in Germany indicate that the rate is 0,02%.
How can this be?
Die ZEIT ONLINE did some research and found that Matthes’ data are based on extremely shoddy science and mistakes. The Carite also distanced themselves from Matthes’ evaluation: “The investigation is an open survey and not really a scientific study. The data are not suitable for drawing definitive conclusions regarding incidence figures in the population that can be generalized” The problems with Matthes’ ‘study’ seem to be sevenfold:
- The data are not published and can thus not be scrutinized.
- Matthes’ definition of a severe adverse effect is not in keeping with the generally accepted definition.
- Matthes did not verify the adverse effects but relied on the information volunteered by people over the Internet.
- Matthes’ survey is based on an online questionnaire accessible to anyone. Thus it is wide open to selection bias.
- The sample size of the survey is around 10 000 which is far too small for generalizable conclusions.
- There is no control group which makes it impossible to differentiate a meaningful signal from mere background noise.
- The data contradict those from numerous other studies that were considerably more rigorous.
Despite these obvious flaws Matthes insisted in a conversation with ZEIT ONLINE that the German official incidence figures are incorrect. As Germany already has its fair share of anti-vaxxers, Matthes’ unfounded and irresponsible claims contribute significantly to the public sentiments against COVID vaccinations. They thus endangering public health.
In my view, such behavior amounts to serious professional misconduct. I, therefore, feel that his professional body, the Aerztekammer, should look into it and prevent further harm.
I just stumbled over a paper we published way back in 1997. It reports a questionnaire survey of all primary care physicians working in the health service in Devon and Cornwall. Here is an excerpt:
Replies were received from 461 GPs, a response rate of 47%. A total of 314 GPs (68%, range 32-85%) had been involved in complementary medicine in some way during the previous week. One or other form of complementary medicine was practised by 74 of the respondents (16%), the two most common being homoeopathy (5.9%) and acupuncture (4.3%). In addition, 115 of the respondents (25%) had referred at least one patient to a complementary therapist in the previous week, and 253 (55%) had endorsed or recommended treatment with complementary medicine. Chiropractic, acupuncture and osteopathy were rated as the three most effective therapies, and the majority of respondents believed that these three therapies should be funded by the health service. A total of 176 (38%) respondents reported adverse effects, most commonly after manipulation.
What I found particularly interesting (and had totally forgotten about) were the details of these adverse effects: Serious adverse effects of spinal manipulation included the following:
- paraplegia,
- spinal cord transection,
- fractured vertebra,
- unspecified bone fractures,
- fractured neck of femur,
- severe pain for years after manipulation.
Adverse effects not related to manipulation included:
- death after a coffee enema,
- liver toxicity,
- anaphylaxis,
- 17 cases of delay of adequate medical attention,
- 11 cases of adverse psychological effects,
- 14 cases of feeling to have wasted money.
If I remember correctly, none of the adverse effects had been reported anywhere which would make the incidence of underreporting 100% (exactly the same as in a survey we published in 2001 of adverse effects after spinal manipulations).