Cancer
Prof Michael Frass is the undisputed star amongst researchers of homeopathy. Here are the awards and achievements that he mentions on his website:
- 1994 until 2019Head, Special Outpatient Clinic “Homeopathy in Malignant Diseases”, Department of Internal Medicine I, General Hospital of the City of Vienna
- 1992 until Feb. 2004Director, Intensivstation 13.i2, Klinik für Innere Medizin I
- 1994 until 1998 Medical Director Maimonides Center
- since May 1994Vice President of the “Medical Society for Classical Homeopathy” (ÄKH)
- since Oct. 1995Head of the Working Group for Homeopathy of the ÄKH in Vienna
- since Jan. 1998 Speaker of the ÄKH at training courses
- 1999 – 2012Training Officer of the Austrian Society for Internal and General Intensive Care Medicine (ÖGIAIM)
- 2001 until 2019 Coordinator of the lecture series “Selected chapters and scientific discussion of complementary medicine methods”, Med. Univ. Vienna, VO 560480
- May 2002 – Dec. 2005Director of the Ludwig Boltzmann Institute for Homeopathy
- since June 2003Member of the Scientific Advisory Board of the Vienna International Academy of Holistic Medicine
- 2004 until 2019Expert in Airway Management and Homeopathy in Intensive Care Medicine at the Center of Excellence in Internal Critical Care Medicine (CEMIC).
- 2005 until 2019Coordinator of the free elective “Homeopathy”, Med. Univ. Vienna, VO 562 923
- since June 2005Director, Institute for Homeopathy Research
- 2006 until 2019Member of the planning area + lecturer for the line element “Interdisciplinary Patient Management” (compulsory lecture for medical students)
- since June 2006President of the Austrian Umbrella Association for Medical Holistic Medicine.
- since Nov. 2010Chairman of the Scientific Society for Homeopathy (WissHom)
Many of my readers will remember the case of the Prof. Frass et al study of homeopathy for cancer. On this blog, we have seen several articles about it:
- Michael Frass’ research into homeopathy for cancer: “numerous breaches of scientific integrity”
- An update on the dubious cancer study by Prof Michael Frass et al
- A thorough analysis of Prof M. Frass’ recent homeopathy trial casts serious doubts on its reliability
- Homeopathy prolongs survival of lung cancer patients … Can it be true?
The study and the suspicion of scientific misconduct it raised eventually resulted in an official complaint by the Viennese Medical School to the authority that deals with suspicions of publication fraud, the ‘Austrian Agency for Scientific Integrity’. It took a very long time, but recently they have published their final on-line summary of their assessment of the case; here is my translation:
Enquiry A 2021/10:
After an Austrian university was informed externally and by name of possible scientific misconduct in a study and the resulting publication, the institution concerned submitted the already publicised suspected case in the field of applied natural sciences to the OeAWI with a request for examination by the Commission.
After establishing sufficient suspicion of various violations of good scientific practice, the Commission declared itself responsible and initiated proceedings. In the course of this, the principal investigator was given the opportunity to submit a written statement and to provide the Commission for Research Integrity Annual Report 2022 material that would help to clarify the facts of the case, which the accused submitted in large quantities.
In a very complex, comprehensive investigation, which required, among other things, the on-site inspection of original documents, the Commission was able to substantiate the suspicion of data falsification, fabrication and manipulation. In a final statement, the study director, who no longer works for the university in question, and the numerous co-authors were informed in detail about the course and results of the commission’s investigation and informed of the recommendations to the university and journal. The Commission recommended that the university concerned should consider investigating its own responsibilities and act accordingly, and that the publication should be withdrawn as a matter of urgency. The journal responsible for the publication was asked to withdraw the publication on the basis of the findings of the investigation.
Nobody who has studied the Frass paper in some detail can be surprised by the verdict. I do applaud the ‘Austrian Agency for Scientific Integrity’ for their work. Yet, I do also have some criticism: health fraud on the scale of Frass can easily costs lives. I find it therefore unacceptable that the verdict took so long to get published.
Even worse is, in my view, the fact that the journal, ‘Oncologist’, is still offering this paper today, albeit with this ‘expression of concern’:
This is an Expression of Concern regarding: Michael Frass, Peter Lechleitner, Christa Gründling, Claudia Pirker, Erwin Grasmuk-Siegl, Julian Domayer, Maximilian Hochmair, Katharina Gaertner, Cornelia Duscheck, Ilse Muchitsch, Christine Marosi, Michael Schumacher, Sabine Zöchbauer-Müller, Raj K. Manchanda, Andrea Schrott, Otto Burghuber, Homeopathic Treatment as an Add-On Therapy May Improve Quality of Life and Prolong Survival in Patients with Non-Small Cell Lung Cancer: A Prospective, Randomized, Placebo-Controlled, Double-Blind, Three-Arm, Multicenter Study, The Oncologist, Volume 25, Issue 12, December 2020, Pages e1930–e1955, https://doi.org/10.1002/onco.13548
In August 2022, the journal editors received credible information from the Austrian Agency for Research Integrity about potential data falsification and data manipulation in this article.*** While The Oncologist editorial team investigates and communicates with the corresponding author, the editors are publishing this Expression of Concern to alert readers that, pending the outcome and review of a full investigation, the research results presented may not be reliable.
Cancer patients will thus still read the dangerously misleading conclusions of the Frass fabrication: “Quality of life (QoL) improved significantly in the homeopathy group compared with placebo. In addition, survival was significantly longer in the homeopathy group versus placebo and control. A higher QoL might have contributed to the prolonged survival. The study suggests that homeopathy positively influences not only QoL but also survival. Further studies including other tumor entities are warranted.” And lives of cancer patients remain needlessly at risk. In my view, this is seriously unethical.
***As far as I know, they received credible information from others long before that!
Yestderday, it was announced that King Charles has cancer. He had been in hospital for surgery for his enlarged prostate. Initially, the news was positive, as it was confirmed not to be prostate cancer. However, during the investigations, a cancer was discovered that apparently is unrelated to the prostate. Since the announcement, many journalists and other people have written to me asking what I think about it and what treatment Charles is likely to receive. I therefore decided to write a short post about the matter.
As a physician and human being I am very sorry whenever I hear that anyone has fallen ill, particularly if the condition is serious and potentially life-threatening. That this includes Charles goes without saying. Equally it is self-evident that I wish that all goes well for him, that the treatment he reportedly has already started is not too arduous, that he keeps in good spirit, that he has empathetic support from all his family and recovers quickly and fully.
Charles will, I am sure, have the best treatment anyone could wish for. Will he use so-called alternative medicine (SCAM), for example, the Gerson therapy, one of the SCAMs he once promoted as a cure of cancer? Of course not! He will receive the most effective, evidence-based care that is currently available. Will he thus not try any SCAM at all? I am confident that he will use SCAM wisely, namely not as a cure but as a supportive measure. In my book on this very subject, I go through all the relevant evidence and conclude that, while SCAM is most certainly not a cancer cure, it can have a place in supportive cancer care. Depending on the symptoms that develop during and after the conventional treatments, certain SCAMs can, according to fairly sound evidence, be helpful in improving wellness and quality of life.
Going through a battle against cancer is often a most humbling experience. Therefore, I am hopeful that, as he recovers from his ordeal, Charles will see that modern medicine – he once described it as being out of balance like the leaning tower of Pisa – is not just effective, empathetic and caring but also not nearly as unbalanced and unholistic as he often proclaimed it to be. In that sense, the experience might reform our king, and – who knows? – he might, after all, turn out to be not the self-proclaimed enemy but a true friend of the Enlightenment.
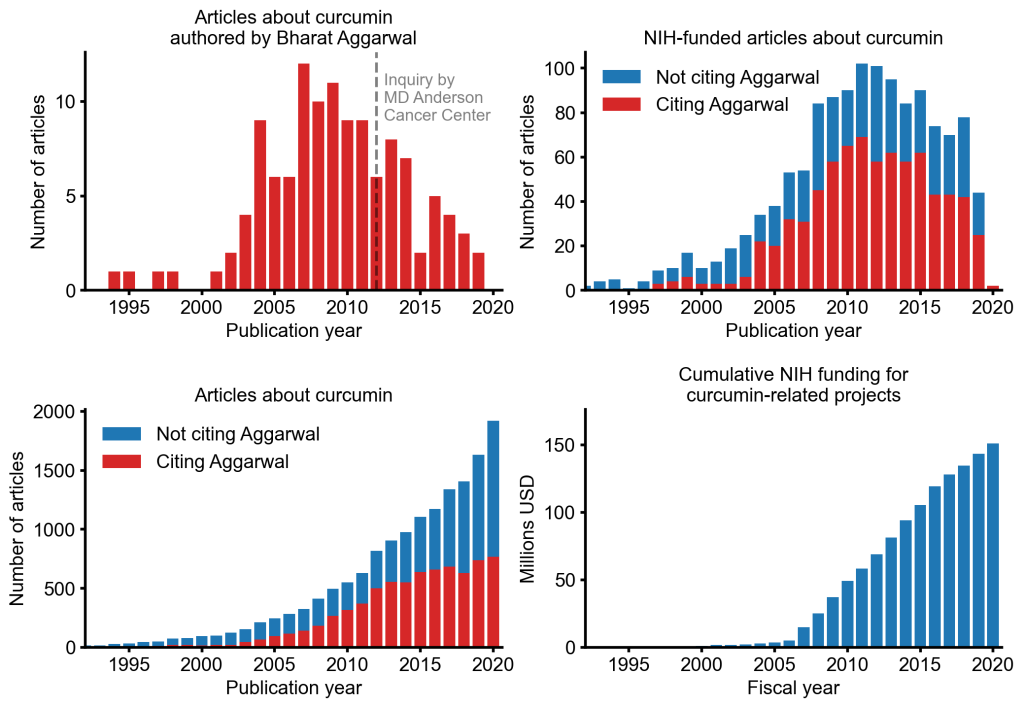
An alarming story of research fraud in the area of so-called alternative medicine (SCAM) is unfolding: Bharat B. Aggarwal, the Indian-American biochemist who worked at MD Anderson Cancer Center, focused his research on curcumin, a compound found in turmeric, and authored more than 125 Medline-listed articles about it. They reported that curcumin had therapeutic potential for a variety of diseases, including various cancers, Alzheimer’s disease and, more recently, COVID-19.
The last of these papers, entitled “Curcumin, inflammation, and neurological disorders: How are they linked?”, was publiched only a few months ago. Here is its abstract:
Background: Despite the extensive research in recent years, the current treatment modalities for neurological disorders are suboptimal. Curcumin, a polyphenol found in Curcuma genus, has been shown to mitigate the pathophysiology and clinical sequalae involved in neuroinflammation and neurodegenerative diseases.
Methods: We searched PubMed database for relevant publications on curcumin and its uses in treating neurological diseases. We also reviewed relevant clinical trials which appeared on searching PubMed database using ‘Curcumin and clinical trials’.
Results: This review details the pleiotropic immunomodulatory functions and neuroprotective properties of curcumin, its derivatives and formulations in various preclinical and clinical investigations. The effects of curcumin on neurodegenerative diseases such as Alzheimer’s disease (AD), amyotrophic lateral sclerosis (ALS), brain tumors, epilepsy, Huntington’s disorder (HD), ischemia, Parkinson’s disease (PD), multiple sclerosis (MS), and traumatic brain injury (TBI) with a major focus on associated signalling pathways have been thoroughly discussed.
Conclusion: This review demonstrates curcumin can suppress spinal neuroinflammation by modulating diverse astroglia mediated cascades, ensuring the treatment of neurological disorders.
The Anderson Cancer Center initially appeared to approve of Aggarwal’s work. However, in 2012, following concerns about image manipulation raised by pseudonymous sleuth Juuichi Jigen, MD Anderson Cancer Center launched a research fraud probe against Aggarwal which eventually led to 30 of Aggarwal’s articles being retracted. Moreover, PubPeer commenters have noted irregularities in many publications beyond the 30 that have already been retracted. Aggarwal thus retired from M.D. Anderson in 2015.
Curcumin doesn’t work well as a therapeutic agent for any disease – see, for instance, the summary from Nelson et al. 2017:
“[No] form of curcumin, or its closely related analogues, appears to possess the properties required for a good drug candidate (chemical stability, high water solubility, potent and selective target activity, high bioavailability, broad tissue distribution, stable metabolism, and low toxicity). The in vitro interference properties of curcumin do, however, offer many traps that can trick unprepared researchers into misinterpreting the results of their investigations.”
Despite curcumin’s apparent lack of therapeutic promise, the volume of research produced on curcumin grows each year. More than 2,000 studies involving the compound are now published annually. Many of these studies bear signs of fraud and involvement of paper mills. As of 2020, the United States National Institutes of Health (NIH) has spent more than 150 million USD funding projects related to curcumin.
This proliferation of research has fueled curcumin’s popularity as a dietary supplement. It is estimated that the global market for curcumin as a supplement is around 30 million USD in 2020.
The damage done by this epic fraud is huge and far-reaching. Hundreds of millions of taxpayer dollars, countless hours spent toiling by junior scientists, thousands of laboratory animals sacrificed, thousands of cancer patients enrolled in clinical trials for ineffective treatments, and countless people who have eschewed effective cancer treatment in favor of curcumin, were encouraged by research steeped in lies.
In total, 404 respondents completed the survey, of which 254 (62.9%) treated cancer patients. Most practitioners were acupuncturists and herbalists (57.1%), had (16.8 ± 9.9) years of clinical experience and see a median of 2 (1, 4) cancer patients per week. Breast cancer (61.8%) is the most common cancer type seen in SCAM clinics. Adjunctive SCAM treatments are frequently concurrent with the patient’s cancer specific treatment (39.9%), which is also reflected by the main goal of a SCAM treatment to alleviate side effects (52.4%). However, only 28.0% of the respondents are in contact with the treating oncologist. According to the respondents, pain is most effectively treated using acupuncture, while herbal medicine is best for cancer-related fatigue. SCAM practitioners mostly use certified courses (33.1%) or online databases (28.3%) but often believe that experts are more reliable to inform their practice (37.0%) than research publications (32.7%).
The authors concluded that acupuncturists and herbalists commonly treat cancer patients. Most practitioners use SCAM as an adjunct to biomedicine as supportive care and use it largely in accordance with current oncological guidelines.
You would think that the combined expertise of these institutions are capable of producing a decent survey:
- Palliative Care Unit, Division of Oncology, Department of Internal Medicine, Medical University of Graz, 8036 Graz, Austria
- Northern College of Acupuncture, York YO1 6LJ, United Kingdom
- School of Health and Society, Faculty of Education, Health and Wellbeing, University of Wolverhampton, Wolverhampton WV1 1LY, United Kingdom
- National Institute of Complementary Medicine Health Research Institute, Western Sydney University, Penrith NSW 2751, Australia
- Translational Health Research Institute, Western Sydney University, Penrith NSW 2751, Australia
- Medical Research Institute of New Zealand, Wellington 6021, New Zealand
- Translational Oncology, University Hospital of Augsburg, 86156 Augsburg, Germany
Well, you would have been mistaken! This surely is one of the worst investigations I have seen for a while. Here are just three reasons why:
- The researchers designed an anonymous self-completion questionnaire collecting data about the participating practitioners’ demographics and clinical practice of integrative oncology. Someone should tell them that one ought to validate questionnairs before using them and that validated questionnairs exist. Unvalidated questionnairs cannot tell us much of value.
- The researchers invited SCAM practitioners in Austria, Germany, USA, Australia, and New Zealand to participate in this study. Invitations were distributed through social media and emails between October 2022 and December 2022 by professional organizations. Someone should tell them that research needs to be reproducible and surveys need to cover a representative population – both criteria that are not met here.
- The survey participants had to hold a valid license to perform acupuncture, herbal medicine, or both. That excludes all other SCAM practitioners.
Despite these serious flaws, the survey shows two findings that might be worth mentioning:
- only 28.0% of the SCAM practitioners were in contact with the treating oncologist;
- SCAM practitioners believe that “experts” are more reliable to inform their practice than research publications.
For me, these two points alone would be sufficient reason to run a mile!
He came to my attention via the sad story recently featured here about patients allegedly being harmed or killed in a Swiss hospital for so-called alternative medicine (SCAM). What I then learned about the doctor in charge of this place fascinated me:
Rau states about himself (my translation):
Early on, Dr Rau focused on natural therapies, in particular homeopathy and dietary changes. The healing success of his patients proved him right, so he studied alternative healing methods with leading practitioners. These included orthomolecular medicine, Chinese and Ayurvedic medicine and European holistic medicine. With his wealth of knowledge and over 30 years of experience, Dr Rau formed his own holistic theory of healing: Swiss Biological Medicine – Dr Rau’s Biological Medicine. It is based on the principles of detoxification, nutrition, digestion and sustainable strengthening of the immune system.
Career & studies:
- Medical studies at the University of Bern
- Final medical examinations in Switzerland and the USA
- Subsequent work in rheumatology, internal and general medicine
- Member of the Swiss Medical Association FMH since 1981
- 1981 to 1992 conventional physician & medical director of a Swiss spa centre for rheumatology and rehabilitation medicine
- 1983 to 1992 Doctor at a drug rehabilitation centre
- 1992 to 2019 Establishment of the Paracelsus Clinic Lustmühle as medical director and partner
- until 2020 Head of the academic network and training organisation “Paracelsus Academy”
Rau also states this:
- 2019 mit dem Honorarprofessoren-Titel von der Europäischen Universität in Wien ausgezeichnet (2019, he was awarded the title of homorary professor at the European University in Vienna)
This puzzles me because there is no such institution as the ‘Europäische Universität in Wien’. There is a Central European University but this can hadly be it?!
Now, I am intrigued and see what the ‘honorary professor’ might have published. Sadly, there seems to be nothing on Medline except 2 interviews. In one interview, Rau explains (amongst other things) ‘live blood analysis’, a method that we have repeatedly discussed before (for instance, here and here):
Darkfield microscopy shows a lot. We take 1 drop of blood and look at it under a very large-scale magnification. The blood is life under the glass. Once it’s on the glass, there isn’t oxygen or light or heat. This is a giant stress for the blood. So we see how, over a time, the blood reacts to this stress, and how the blood cells tolerate the stress. You can see the changes. So we take a drop of blood that represents the organism and put it under stress and look at how the cells react to the stress, and then we can see the tolerance and the resistiveness of these cells. Do they have a good cell-membrane face? Do they have good energetic behavior? Do they clot together? Is there a chance for degenerative diseases? Is there a cancerous tendency in this blood? We see tendencies. And that’s what we are interested in, tendencies.
Question: If you saw a cancerous tendency, what would that look like?
Rau: Cancerous tendency is a change in the cells. They get rigid, so to say. They don’t react very well.
Question: And how long does blood live outside the body?
Rau: It can live for several days. But after 1 hour, the blood is already seriously changed. For example, a leukemia patient came to my clinic for another disease. But when we did darkfield, I found the leukemia. We saw that his white blood cells were atypical. Look at this slide—the fact that there are so many white blood cells together is absolutely unusual, and the fact that there are atypical white blood cells. This shows me that the patient has myeloid leukemia. The patient had been diagnosed as having rheumatoid lung pain, but it was absolutely not true. The real cause of his pain was an infiltration of the spinal bone by these lymphocytes.
This is, of course, complete nonsense. As I explained in my blog post, live blood analysis (LBA) is not plausible and there is no evidence to support the claims made for it. It also is by no means new; using his lately developed microscope, Antony van Leeuwenhoek observed in 1686 that living blood cells changed shape during circulation. Ever since, doctors, scientists and others have studied blood samples in this and many other ways.
New, however, is what today’s SCAM practitioners claim to be able to do with LBA. Proponents believe that the method provides information about the state of the immune system, possible vitamin deficiencies, amount of toxicity, pH and mineral imbalance, areas of concern and weaknesses, fungus and yeast infections, as well as just about everything else you can imagine.
LBA is likely to produce false-positive and false-negative diagnoses. A false-positive diagnosis is a condition which the patient does not truly have. This means she will receive treatments that are not necessary, potentially harmful and financially wasteful. A false-negative diagnosis would mean that the patient is told she is healthy, while in fact she is not. This can cost valuable time to start an effective therapy and, in extreme cases, it would hasten the death of that patient. The conclusion is thus clear: LBA is an ineffective, potentially dangerous diagnostic method for exploiting gullible consumers. My advice is to avoid practitioners who employ this technique.
And what does that say about ‘honorary professor’ Rau?
I think I let you answer that question yourself.
Some articles are just too remarkable for me to alter them in any way. This one impresses already by its title: “Ameliorative effects of homeopathic medicines in the management of different cancers“. By way of a ‘Christmas treat’, here its summary:
Homeopathy is a commonly used complementary and alternative system of medicine for the treatment of various sorts of ailments throughout the world. Homeopathic medicines are made up of potential therapeutic natural products that are primarily acknowledged for their low doses as well as extended patient survival results. Homeopathic medicines are derived from plants such as arnica (mountain herb), red onion, poison ivy, stinging nettle, and belladonna (deadly nightshade); minerals including white arsenic as well as from animals such as crushed whole bees. Homeopathic medicines are synthesized as sugar pellets to be placed under the tongue and may also be used in the form of gels, ointments, drops, tablets, and creams. Homeopathic medicines can be used to treat various disorders including migraine, depression, gastrointestinal diseases, joint pain, inflammation, different sorts of injuries, flu, arthritis as well as sciatica.
Cancer is the 2nd major reason behind global mortalities. It is revealed that developing countries around the world shoulder most of the cancer burden. According to a survey conducted in 2020, low- and middle-income countries face 70% of the total mortalities worldwide which accounts for approximately 10 million people of these countries. Homeopathic medicines ensure low-cost cancer treatment with little or no side effects on the bodies of humans and animals. Besides, it is applied as a supportive and palliative therapy in a broad range of cancer patients to enhance the body’s fight against cancer, alleviate discomfort resulting from disease or conventional treatments as well as improve the general well-being of the patients. In this chapter, our primary focus will be on the anti-cancerous effects of homeopathic medicines against different cancerous conditions in the body along with their mechanism of action.
Let me just mention a few fairly obvious points:
- Homeopathic medicines are made up of potential therapeutic natural products … REALLY? Have a look at those remedies, for instance:
- Blue (colour)
- Eclipse Totality
- Electricitas (Electricity – 80,000 volts)
- Electricitas (High Voltage Pylon)
- Green (colour)
- Halogen light
- Indigo (colour)
- Laser – red (Diode Laser Red)
- Laser Beam (2940 nm)
- LED (white) (White L(ight) E(mitting) D(iode) Light)
- LIGHT (ENERGY SAVING BULB)
- Luna (Moonlight)
- Microwave 750 MHz
- Milky Way (Essence)
- Mobile phone (Eising)
- Mobile Phone 1800MHz
- Mobile Phone 900Mhz
- Mobile Phone Mast G3
- Polaris (North star)
- Purple (Colour)
- Radiation Combination (Guild Radiation Combination)
- Rainbow (Spectrum)
- Red (colour)
- Red ( A. Wauters)
- Sol Africana
- Sol Australis (Sunlight – Australia)
- Sol Britannic (Sunlight British)
- Stonehenge (Emanation)
- Sunlight Blue (Prismatic blue from sunlight)
- Sunlight Green (Prismatic green from sunlight)
- Sunlight Orange (Prismatic orange from sunlight)
- Sunlight Purple (Prismatic purple from sunlight)
- Sunlight Red (Prismatic Red from Sunlight)
- Sunlight Yellow (Prismatic yellow from sunlight)
- Ultrasound (General)
- Ultrasound (Vaginal)
- Ultraviolet Light
- Vacuum
- Wind (South-West)
- X-ray
- Homeopathic medicines are derived from plants such as arnica (mountain herb), red onion, poison ivy, stinging nettle, and belladonna (deadly nightshade); minerals including white arsenic as well as from animals such as crushed whole bees. REALLY? Consider these remedies, for example:
- Aqua Aurum (Gold and sea water)
- Aqua Fida Vetusta (Old Faithful Water)
- Aqua Hochstein (Spring Source water from the Bavarian Forest)
- Aqua marina (Sea Water)
- Aqua nova
- Aqua Odilien
- Aqua Pura Bottled Water
- Aqua Schuasta
- Aqua Sulis (Water from Bath, Roman Spa)
- Aqua Victoria Falls
- Aqua XwMuthkwium (Musqueam Creek Water)
- Chalice Well Water
- Dead Sea Water
- Double Helix Water
- Ganga water (water from the River Ganges)
- Ganga Water (Gaumuk)
- Ganga Water (Varanasi)
- Gastein (Gastein Aqua)
- Geum Rivale (Water Avens)
- Halltal Spring Water (Water from Solbadhall in Tirol)
- Levico water (from lake in N Italy)
- Lourdes Water
- Nadana Water
- Nigari (Concentrated Japanese seawater)
- Nordenau water
- Seven Spring Head Water
- Severn Water (Source)
- Water (Guild)
- Wiesbaden Aqua (Wiesbaden Water)
- Winchelsea Water
- Zamzam aqua (Zamzam spring water [Mecca])
- Homeopathic medicines are synthesized… No, they are manufactured.
- Homeopathic medicines can be used to treat various disorders… albeit without any effect beyond placebo!
- Homeopathic medicines ensure low-cost cancer treatment with little or no side effects… and no therapeutic effect beyond placebo!
- Besides, it is applied as a supportive and palliative therapy in a broad range of cancer patients to enhance the body’s fight against cancer, alleviate discomfort resulting from disease or conventional treatments as well as improve the general well-being of the patients. This, I’m afraid, is a dangerous lie.
- …the anti-cancerous effects of homeopathic medicines… do not exist.
My conclusion:
Those who advocate homeopathy don’t know what it is, while those who know what it is, don’t advocate it.
The NZZ recently published a long and horrific report about a natural health clinic and its doctors. Here is a version translated and shortened by me; perhaps it makes a few people think twice before they waste their money and risk their health:
It is a narrow mountain road that they are racing down on this spring evening. Over the green Appenzell hills, towards Herisau hospital. Kathrin Pfister* is fighting for her life in the car. At the wheel is Thomas Rau, internationally renowned practitioner of so-called alternative medicine (SCAM) and director of his own luxury clinic, the Biomed Centre Sonnenberg. Three days later, Kathrin Pfister is dead. The most likely finding according to the experts: Pfister was injected with a drug that was not authorised in Switzerland at the time, the side effects of which killed her.
Pfister is not the only woman to have lost her life following treatment at the Sonnenberg. Other experts accuse Rau of serious breaches of duty that led to the death of a patient. Rau and another doctor are thus being investigated for involuntary manslaughter.
The events remained hidden from the public for over two years. It’s not just about one doctor, not just about one clinic. The events are politically explosive for Appenzell Ausserrhoden. The canton is the centre of alternative medicine in Switzerland. SCAM doctors are an important economic factor in Ausserrhoden. Wealthy people from all over the world fly here for therapies that most conventional doctors just shake their heads at. Treatments lasting several weeks with a hotel stay cost five-figure sums.
The 73-year-old Dr Rau is the star among Swiss alternative medicine practitioners.He describes himself as the “Mozart of medicine”. The Biomed Centre Sonnenberg is “Mozart’s” last big project. The clinic has a hotel and gluten-free vegan restaurant from the Tibits chain. Even the feather pillows are replaced with bamboo ones. All for the “detox” that Rau praises.
Kathrin Pfister’s case began in mid-April 2021, just four months after the Sonnenberg centre opened. She is actually healthy and comes to the clinic anyway; because of some digestive problems and headaches. The hospital records show that Pfister received infusions. Initially only those containing vitamin C and homeopathic remedies. Then one with artesunate, a preparation against malaria. And finally, on a Friday, Pfister was injected with a solution of alpha-lipoic acid into his bloodstream. The infusion is used in Germany for long-term diabetics with nerve damage. It was not authorised as a medicinal product in Switzerland at the time. According to the forensic experts, it was this substance that was “ultimately causally linked to the death”.
A few hours later, Pfister had severe abdominal cramps. Then pain throughout the body. The number of platelets in her blood drops dramatically. Anxiety sets in at the clinic. The intensive care doctors in Herisau and later at the cantonal hospital in St. Gallen can do nothing more. Pfister had a massive blood clotting disorder. Her liver and kidneys were no longer functioning.
Mary Anne Hawrylak meets Thomas Rau by chance at the clinic that weekend. She too is a patient, recently flown in from the USA. Hawrylak had massive side effects after infusions that Friday. “When I told him about it, he turned white as a sheet, like a ghost,” says Hawrylak. “Doctor Rau told me in horror that I had received the same infusions as ‘Kathrin’ and that he had to test my blood.” The tests showed that her blood platelet count had also dropped, says Hawrylak.
The forensic experts point to a central fact: Alpha lipoic acid can cause blood clotting disorders. They come to the conclusion that this is “most likely a lethal side effect of a drug”. The use of drugs that are not authorised in Switzerland is legal if they are authorised in a country with a comparable procedure. However, there is no real reason to inject this medication into the bloodstream of healthy people. It was authorised in Germany for diabetes patients with nerve damage. So, Pfister did not have this authorisation.
Experts refer to such applications as “off-label use”. Off-label treatments should only be carried out “on the basis of valid guidelines, generally recognised recommendations or scientific literature”. The guidelines also require that patients are given comprehensive information about off-label use. This counselling session should be documented in writing. None of this can be found in the clinic’s files. No written consent, no documented risk-benefit assessment, no reference to the risk of blood clotting disorders. The forensic experts state: “The scant documentation from the Sonnenberg Biomed Centre does not contain any corresponding information document.” The question arises as to “whether the medical treatment at the Sonnenberg Biomed Centre was carried out with the necessary medical care”.
Patient Hawrylak also says: “I was not told exactly what was in the infusions. I was never told that the medication was not authorised in Switzerland or that its use was off-label. I spoke to Dr Rau about what had happened to ‘Kathrin’ because I was worried about myself,” says Hawrylak. “He said to me: ‘I don’t think it was the infusions. I think it was the Covid vaccinations.” He only justified this with his “intuition”.
The Pfister case triggered an investigation by the public prosecutor’s office. But what hardly anyone knew at the time was that it was not the first questionable death at the clinic – not even the first in a month. Ruth Schmid*, a 77-year-old Swiss woman, had died just three weeks earlier. In this case, the forensic pathologists accused Rau: He had made mistakes that not even a medical student should have made, thus causing Schmid’s death.
Schmid was also in the clinic for a kind of cure. When she was about to leave, she began to tremble violently and had extreme stomach pains. She screamed “like an animal”, her partner said during the interrogation. Ultrasound examinations were carried out at the clinic and Rau gave Schmid painkillers, including morphine. According to the partner’s statement to the public prosecutor’s office, he asked Rau whether Schmid needed to be taken to hospital. Rau said no. Schmid stayed in the hotel room overnight. The next day – according to Rau, she had been feeling better since the previous evening – she travelled home. According to Rau’s confiscated notes, “she was to report closely” and return in four days. At home, Ruth Schmid fell into a coma-like state overnight. Admitted to Zurich University Hospital in an emergency, Schmid died there of cardiovascular failure due to septic shock.
The Zurich forensic pathologists performed an autopsy on Schmid’s body. Their findings: Schmid had suffered from intestinal paralysis. As a result, bacteria entered her body and poisoned her blood, leading to a heart attack. “From a forensic medical point of view, it is incomprehensible why the attending physician, Dr Thomas Rau, did not carry out appropriate diagnostics.” The irritation of the forensic experts is evident in almost every line. There had been several warning signs of intestinal paralysis. The forensic experts wrote: “This knowledge is taught in medical school and is considered basic knowledge in human medicine.” Rau’s behaviour was “a breach of the doctor’s duty of care”. With timely treatment, the prognosis for intestinal paralysis is excellent. The sad conclusion: Ruth Schmid did not have to die.
During questioning by the public prosecutor’s office, Rau denied any guilt. Schmid had left in “good condition”. There was no causality between what happened in the clinic and the death. The findings and conclusions of the Zurich forensic pathologists were wrong. Schmid did not have intestinal paralysis or septicaemia. He had been able to rule out intestinal paralysis because intestinal noises had been audible in the morning. The dose of morphine had been very small, so that it had had no effect. There were no indications of a serious condition. Rau testified that he had acted professionally, as would be expected of an internal medicine doctor.
In the Kathrin Pfister case, the doctors treating her also deny any culpability and question the forensic medical report. The doctor’s lawyer writes that the criminal investigation will show that there was no breach of the doctor’s duty to provide information. Alpha-lipoic acid was not responsible for the death. The expert opinion is not convincing in terms of method or content: “When analysed in depth, it contains no justification that the use of alpha-lipoic acid was in any way causal for the patient’s death.”
During the hearing on the Pfister case, Rau said that restricting the use of alpha-lipoic acid to diabetics was “a joke” and far too narrowly defined. He claimed that Pfister had polyneuropathy, a complex nerve disease. However, there is no mention of this in the files of Rau’s clinic.
The criminal investigation is ongoing in both cases. But did more happen on the Sonnenberg? A former hospital employee, who independently reported to the police, told the public prosecutor about other hair-raising incidents. During the interrogation, she testified that she had seen a young woman being carried out of the clinic extremely weak after an infusion. Days later, she had overheard parts of a telephone conversation between Rau and the patient’s angry husband which made it clear that the woman had died. The former employee also recounted a conversation with Rau’s wife, who is a trained nurse. She said that she had driven a patient to a hospital in Zurich in a private car with Rau because Rau was determined to take her to a particular specialist. The patient was so unwell that she was afraid the woman would die on the way. If this is true, Rau would have travelled past several hospitals with a seriously ill patient.
Hawrylak has one last memory of Appenzell etched in his memory. The departure. She was just leaving the clinic when Rau wished her good luck: “I could only say to him: I wish you good luck too, Doctor Rau. I think you’re really going to need it.”
*Names were altered.
As promised, here is my translation of the article published yesterday in ‘Le Figaro’ arguing in favour of integrating so-called alternative medicine (SCAM) into the French healthcare system [the numbers in square brackets were inserted by me and refer to my comments listed at the bottom].
So-called unconventional healthcare practices (osteopathy, naturopathy, acupuncture, homeopathy and hypnosis, according to the Ministry of Health) are a cause for concern for the health authorities and Miviludes, which in June 2023 set up a committee to support the supervision of unconventional healthcare practices, with the task of informing consumers, patients and professionals about their benefits and risks, both in the community and in hospitals. At the time, various reports, surveys and press articles highlighted the risks associated with NHPs, without pointing to their potential benefits [1] in many indications, provided they are properly supervised. There was panic about the “booming” use of these practices, the “explosion” of aberrations, and the “boost effect” of the pandemic [2].
But what are the real figures? Apart from osteopathy, we lack reliable data in France to confirm a sharp increase in the use of these practices [3]. In Switzerland, where it has been decided to integrate them into university hospitals and to regulate the status of practitioners who are not health professionals, the use of NHPs has increased very slightly [4]. With regard to health-related sectarian aberrations, referrals to Miviludes have been stable since 2017 (around 1,000 per year), but it should be pointed out that they are a poor indicator of the “risk” associated with NHPs (unlike reports). The obvious contrast between the figures and the press reports raises questions [5]. Are we witnessing a drift in communication about the risks of ‘alternative’ therapies? [6] Is this distortion of reality [7] necessary in order to justify altering the informed information and freedom of therapeutic choice of patients, which are ethical and democratic imperatives [8]?
It is the inappropriate use of certain NHPs that constitutes a risk, more than the NHPs themselves! [9] Patients who hope to cure their cancer with acupuncture alone and refuse anti-cancer treatments are clearly using it in a dangerous alternative way [10]. However, acupuncture used to relieve nausea caused by chemotherapy, as a complement to the latter, is recommended by the French Association for Supportive Care [11]. The press is full of the dangers of alternative uses, but they are rare: less than 5% of patients treated for cancer according to a European study [12]. This is still too many. Supervision would reduce this risk even further [13].
Talking about risky use is therefore more relevant than listing “illusory therapies”, vaguely defined as “not scientifically validated” and which are by their very nature “risky” [14]. What’s more, it suggests that conventional treatments are always validated and risk-free [15]. But this is not true! In France, iatrogenic drug use is estimated to cause over 200,000 hospital admissions and 10,000 deaths a year [16]. Yes, some self-medication with phytotherapy or aromatherapy does carry risks… just like any self-medication with conventional medicines [17]. Yes, acupuncture can cause deep organ damage, but these accidents occur in fewer than 5 out of every 100,000 patients [18]. Yes, cervical manipulations by osteopaths can cause serious or even fatal injuries, but these exceptional situations are caused by practitioners who do not comply with the decree governing their practice.[19] Yes, patients can be swindled by charlatans, but there are also therapeutic and financial abuses in conventional medicine, such as those reported in dental and ophthalmology centres. [20]
Are patients really that naive? No. 56% are aware that “natural” remedies can have harmful side-effects, and 70% know that there is a risk of sectarian aberrations or of patients being taken in by a sect [21]. In view of the strong demand from patients, we believe that guaranteeing safe access to certain NHPs is an integral part of their supervision, based on regulation of the training and status of practitioners who are not health professionals, transparent communication, appropriate research, the development of hospital services and outpatient networks of so-called “integrative” medicine combining conventional practices and NHPs, structured care pathways with qualified professionals, precise indications and a safe context for treatment.[22] This pragmatic approach to reducing risky drug use [17] has demonstrated its effectiveness in addictionology [23]. It should inspire decision-makers in the use of NHPs”.
- Reports about things going wrong usually do not include benefits. For instance, for a report about rail strikes it would be silly to include a paragraph on the benefits of rail transport. Moreover, it is possible that the benefits were not well documented or even non-existent.
- No, there was no panic but some well-deserved criticism and concern.
- Would it not be the task of practitioners to provide reliable data of their growth or decline?
- The situation in Switzerland is often depicted by enthusiasts as speaking in favour of SCAM; however, the reality is very different.
- Even if reports were exaggerated, the fact is that the SCAM community does as good as nothing to prevent abuse.
- For decades, these therapies were depicted as gentle and harmless (medicines douces!). As they can cause harm, it is high time that there is a shift in reporting and consumers are informed responsibly.
- What seems a ‘distortion of reality’ to enthusiasts might merely be a shift to responsible reporting akin to that in conventional medicine where emerging risks are taken seriously.
- Are you saying that informing consumers about risks is not an ethical imperative? I’d argue it is an imperative that outweighs all others.
- What if both the inappropriate and the appropriate use involve risks?
- Sadly, there are practitioners who advocate this type of usage.
- The recommendation might be outdated; current evidence is far less certain that this treatment might be effective (“the certainty of evidence was generally low or very low“)
- The dangers depend on a range of factors, not least the nature of the therapy; in case of spinal manipulation, for instance, about 50% of all patients suffer adverse effects which can be severe, even fatal.
- Do you have any evidence showing that supervision would reduce this risk, or is this statement based on wishful thinking?
- As my previous comments demonstrate, this statement is erroneous.
- No, it does not.
- Even if this figure is correct, we need to look at the risk/benefit balance. How many lives were saved by conventional medicine?
- Again: please look at the risk/benefit balance.
- How can you be confident about these figures in the absence of any post-marketing surveillance system? The answer is, you cannot!
- No, they occur even with well-trained practitioners who comply with all the rules and regulations that exist – spoiler: there hardly are any rules and regulations!
- Correct! But this is a fallacious argument that has nothing to do with SCAM. Please read up about the ‘tu quoque’ and the strawman’ fallacies.
- If true, that is good news. Yet, it is impossible to deny that thousands of websites try to convince the consumer that SCAM is gentle and safe.
- Strong demand is not a substitute for reliable evidence. In any case, you stated above that demand is not increasing, didn’t you?
- Effectiveness in addictionology? Do you have any evidence for this or is that statement also based on wishful thinking?
My conclusion after analysing this article in detail is that it is poorly argued, based on misunderstandings, errors, and wishful thinking. It cannot possibly convince rational thinkers that SCAM should be integrated into conventional healthcare.
PS
The list of signatories can be found in the original paper.
Mushrooms are somewhat neglected in medical research, I often feel. This systematic review focused on clinical studies testing the effectiveness of mushrooms in cancer care. A total of 39 met the authors’ inclusion criteria. The studies included 12 different mushroom preparations. Some of the findings were encouraging:
- A survival benefit was reported using Huaier granules (Trametes robiniophila Murr) in 2 hepatocellular carcinoma studies and 1 breast cancer study.
- A survival benefit was also found in 4 gastric cancer studies using polysaccharide-K (polysaccharide-Kureha; PSK) as an adjuvant therapy.
- Eleven studies reported a positive immunological response.
- Quality-of-life (QoL) improvement and/or reduced symptom burden was reported in 14 studies using various mushroom supplements.
- Most studies reported adverse effects of grade 2 or lower, mainly nausea, vomiting, diarrhea, and muscle pain.
The authors caution that limitations included small sample size and not using randomized controlled trial design. Many of the reviewed studies were observational. Most showed favorable effects of mushroom supplements in reducing the toxicity of chemotherapy, improving QoL, favorable cytokine response, and possibly better clinical outcomes.
The authors concluded that the evidence is inconclusive to recommend the routine use of mushrooms for cancer patients. More trials are needed to explore mushroom use during and after cancer treatment.
The use of mushrooms for medicinal purposes has a long history in many cultures. Some mushrooms are known to be highly poisonous, some have hallucinogenic effects, and some are assumed to have pharmacological effects that have therapeutic potential. Some mushrooms possess pharmacologic properties such as anti-tumour, immunomodulating, antioxidant, cardiovascular, anti-hypercholesterolemic, anti-viral, anti-bacterial, anti-parasitic, anti-fungal, detoxification, hepatoprotective, and anti-diabetic effects.
Many modern medicines were derived from fungi. The best-known example is penicillin; others include several cancer drugs, statins and immunosuppressants. In Traditional Chinese Medicine, numerous herbal mixtures contain mushrooms; examples are reishi, maitake and shiitake which are all assumed to have anti-cancer properties.
As the review authors point out, there is a paucity of clinical trials testing the effectiveness of mushrooms, and the existing studies tend to be of poor quality. At present, most of our knowledge comes from traditional use or test-tube studies. The adverse effects depend on the specific mushroom in question and, can in some instances, be serious.
Considering the potential and the complexity of mycomedicine, I find it surprising to not see much more research into this subject.
Bioenergy therapies are among the popular so-called alternative medicine (SCAM) treatments. They are used for many diseases, including cancer. Many studies deal with the advantages and disadvantages of bioenergy therapies as an addition to established treatments such as chemotherapy, surgery, and radiation in the treatment of cancer. However, a systematic overview of this evidence is thus far lacking. For this reason, the available evidence was reviewed and critically examined in this paper.
A systematic search was conducted searching five electronic databases (Embase, Cochrane, PsychInfo, CINAHL and Medline) to find randomized clinical trials concerning the use, effectiveness and potential harm of bioenergy therapies including Reiki, Therapeutic Touch, Healing Touch and Polarity Therapy on cancer patients.
From all 2477 search results, 21 publications with 1375 patients were included in this systematic review. The patients treated with bioenergy therapies were mainly diagnosed with breast cancer. The main outcomes measured were anxiety, depression, mood, fatigue, quality of life (QoL), comfort, well-being, neurotoxicity, pain, and nausea. The studies were predominantly of moderate quality and for the most part found no effect. In terms of QoL, pain and nausea, there were improved short-term effects of the interventions, but no long-term differences were detectable. The risk of side effects from bioenergy therapies appears to be relatively small. Most studies only had a passive control group. Accordingly, in contrast to the active bioenergy therapies groups, attention effects may strongly affect the results. In the comparisons with an active control group, for example a sham group, no effects were detectable.
The authors concluded that, considering the methodical limitations of the included studies, studies with high study quality could not find any difference between bioenergy therapies and active (placebo, massage, RRT, yoga, meditation, relaxation training, companionship, friendly visit) and passive control groups (usual care, resting, education). Only studies with a low study quality were able to show significant effects.
This conclusion will not surprise anyone who is capable of rational thinking. Energy healing methods are implausible; further research into this area is a pure wast of money and arguably unethical.