big pharma
Practitioners of so-called alternative medicine (SCAM) often argue against treating back problems with drugs. They also frequently defend their own therapy by claiming it is backed by published guidelines. So, what should we think about guidelines for the management of back pain?
This systematic review was aimed at:
- systematically evaluating the literature for clinical practice guidelines (CPGs) that included the pharmaceutical management of non-specific LBP;
- appraising the methodological quality of the CPGs;
- qualitatively synthesizing the recommendations with the intent to inform non-prescribing providers who manage LBP.
The authors searched PubMed, Cochrane Database of Systematic Review, Index to Chiropractic Literature, AMED, CINAHL, and PEDro to identify CPGs that described the management of mechanical LBP in the prior five years. Two investigators independently screened titles and abstracts and potentially relevant full text were considered for eligibility. Four investigators independently applied the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument for critical appraisal. Data were extracted for pharmaceutical intervention, the strength of recommendation, and appropriateness for the duration of LBP.
Only nine guidelines with global representation met the eligibility criteria. These CPGs addressed pharmacological treatments with or without non-pharmacological treatments. All CPGs focused on the management of acute, chronic, or unspecified duration of LBP. The mean overall AGREE II score was 89.3% (SD 3.5%). The lowest domain mean score was for applicability, 80.4% (SD 5.2%), and the highest was Scope and Purpose, 94.0% (SD 2.4%). There were ten classifications of medications described in the included CPGs: acetaminophen, antibiotics, anticonvulsants, antidepressants, benzodiazepines, non-steroidal anti-inflammatory drugs (NSAIDs), opioids, oral corticosteroids, skeletal muscle relaxants (SMRs), and atypical opioids.
The authors concluded that nine CPGs, included ten medication classes for the management of LBP. NSAIDs were the most frequently recommended medication for the treatment of both acute and chronic LBP as a first line pharmacological therapy. Acetaminophen and SMRs were inconsistently recommended for acute LBP. Meanwhile, with less consensus among CPGs, acetaminophen and antidepressants were proposed as second-choice therapies for chronic LBP. There was significant heterogeneity of recommendations within many medication classes, although oral corticosteroids, benzodiazepines, anticonvulsants, and antibiotics were not recommended by any CPGs for acute or chronic LBP.
Oddly, this review was published by chiros in a chiro journal. The authors mention that nearly all guidelines the included CPGs recommended non-pharmacological treatments for non-specific LBP, however it was not always delineated as to precede or be used in conjunction with pharmacological intervention.
I find the review interesting because I think it suggests that:
- CPGs are not the most reliable form of evidence. Their guidance depends on how up-to-date they are and on the identity and purpose of the authors.
- Guidelines are therefore often contradictory.
- Back pain is a symptom for which currently no optimal treatment exists.
- The most reliable evidence will rarely come from CPGs but from rigorous, up-to-date, independent systematic reviews such as those from the Cochrane Collaboration.
So, the next time chiropractors osteopaths, acupuncturists, etc. tell you “BUT MY THERAPY IS RECOMMENDED IN THE GUIDELINES”, please take it with a pinch of salt.
Stress is associated with a multitude of physical and psychological health impairments. To tackle these health disorders, over-the-counter (OTC) products like Neurodoron® are popular since they are considered safe and tolerable. One tablet of this anthroposophic remedy contains the following active ingredients:
- 83.3 mg Aurum metallicum praeparatum trituration (trit.) D10,
- 83.3 mg Kalium phosphoricicum trit. D6,
- 8.3 mg Ferrum-Quarz trit. D2.
Experience reports and first studies indicate that Neurodoron® is efficient in the treatment of stress-associated health symptoms. “To confirm this” (!!!), a non-interventional study (NIS) with pharmacies was conducted.
The NIS was planned to enroll female and male patients who suffered from nervous exhaustion with symptoms caused by acute and/or chronic stress. The main outcome measures were characteristic stress symptoms, stress burden, and perceived stress. Further outcome measures included perceived efficacy and tolerability of the product as assessed by the patients and collection of adverse drug reactions (ADRs). A study duration of about 21 days with a recommended daily dose of 3–4 tablets was set.
In total, 279 patients were enrolled at 74 German pharmacies. The analyzed set (AS) included 272 patients (mean age 44.8 ± 14.4 years, 73.9% female). 175 patients of the AS completed the NIS. During the study, all stress symptoms declined significantly (total score 18.1 vs. 12.1 (of max. 39 points), < 0.0001). Furthermore, a reduction of stress burden (relative difference in stress burden, VAS = −29.1%, < 0.0001) was observed. For most patients, perceived stress was reduced at the study end (PSQ total score decreased in 70.9% of the patients). 75.9% of the study population rated the product efficacy as “good” or “very good” and 96.6% rated its tolerability as “good” or “very good.” One uncritical ADR was reported.
The authors concluded that this study adds information on the beneficial effects of Neurodoron® in self-medication. The results from this NIS showed a marked reduction in stress burden and perceived stress, along with an excellent safety profile of the medicinal product (MP) Neurodoron®. Further trials are required to confirm these results.
I beg to differ!
The study had no control group and therefore one cannot possibly attribute any of the observed changes to the anthroposophic remedy. They are more likely to be due to:
- the natural history of the condition,
- regression towards the mean,
- a placebo effects,
- other treatments administered during the trial period.
Sadly, the authors discuss none of these possibilities in their paper.
In view of this, I am tempted to rephrase their conclusions as follows:
This study adds no valuable information on the effects of Neurodoron® in self-medication. The results from this NIS showed what utter nonsense the Weleda marketing team is capable of producing in an attempt to boost sales.
PS
These declarations of the 4 study authors and the sponsorship are revealing, I thought:
RH and CS are employees of Weleda AG, Germany. JH and KS work for daacro GmbH & Co. KG, a clinical research organization, Germany. The authors declare that there are no conflicts of interest.
This study was financed by the pharmaceutical company Weleda AG, Arlesheim, the employer of RH and CS. Weleda commissioned the CRO daacro for their contribution to the manuscript.
Now that the first reviews of, and numerous comments on my new book are in, I thought I bring my readers up to date and perhaps contribute to some fun. My favorite quote comes from a comment on Harriett Hall’s review: “Nothing much new here about Chucky Windsor’s credulity…”
Perhaps I shouldn’t, but I think it is funny and thus I chose it as the title of this post. Apart from being funny, it also has a more serious background. Virtually everyone who contacted me and gave me feedback said that they knew about Charles’ advocacy of alternative medicine. So, the ‘nothing much new’ comment is apt. Yet, they all added that, before reading my book, they had no idea how deeply Charles was involved and how profoundly anti-scientific and irrational his thinking seems to be in this area. Jonathan Stea, for instance, tweeted: “I just finished reading it—review coming soon. Excellent book. I didn’t realize Prince Charles was so stubbornly in love with pseudoscience and trying to promote it for decades under the guise of alternative/integrative medicine.”
Another comment was made on my own blog: “I am an avid consumer of this and other science blogs, books, podcasts and any other media I encounter. One of my earliest exposures was your book Trick or Treat, which I credit with greatly expanding my knowledge of a subject I had dabbled in but had begun to question. I deplore the PoW’s promotion of quackery. I am American and have no dog in the value of Royalty debate. BUT, I don’t see the need to use such a deeply unflattering (and possibly photoshopped) photo of the PoW. I do not think that such a decision is in line with your list of “nots”, and I think it hinders the impact it might otherwise have on fence-sitters. It disappoints me and while I have purchased multiple copies of many of your books to pass on to friends, family, and believers, I will pass on this one.” The photo is perhaps not flattering but there a many out there that are even worse. In any case, it is the publisher who decides on the title page. In the present case, I merely asked them to make my name on the title page a little less prominent than it was on the draft.
And then there were people who emailed me directly, as this medical colleague:
Dear Dr Ernst,
as a GP and ex oral surgeon from a world famous medical school(Edinburgh), also an experienced alternative practitioner,with 51 years in NHS, more than your own clinical exposure, I’m saddened by sponsored? skewed assaults on healing modalities maybe also representing a threat to financial paradigms: I absolved myself of scientific trials “for profit only”, in deference to holistic patient care, & the Hippocratic Oath
In a similar vein, Dr. Larry Malerba, a US homeopath, posted this comment on a Medscape interview with me:
Fortunately, the book reviews were more intelligent. They confirm what I mentioned above: reviewers were amazed at the depth of Charles’ irrationality. Harriett Hall expressed it as follows: “Charles’ efforts to promote alternative medicine have been mentioned many times on SBM, but readers may not appreciate the depth of his folly. I know I didn’t, until I read this book. The full story has never been told until now.” And Paul Benedetti wrote: “In short, readable chapters, Ernst unblinkingly presents how Charles has written books and articles promoting alternative medicine and spearheaded organizations, colleges, and foundations, giving full-throated support to one unproven, often bizarre, alternative health cure after another.”
One of the nicest pieces of praise came from someone who posted this comment on Amazon:
This is a revelatory critique of where vague well-intentioned but ill-informed health ideas promoted by a powerful person do or don’t get us.
Professor Ernst’s explanations are admirably clear – and no-one is more qualified than he to write on this topic. It’s difficult to imagine a more devastating comment on the bad conseqeunces of ill-informed ideas and actions, than that found in the last two paragraphs on Page 88.
There is a great deal of valuable information here on ‘alternative medicine’ approaches, in addition to the explanations of HRH Prince Charles’ involvement with them. A most worthwhile book for anyone wanting to find out more about alternative/complementary treatment modalities.
Yes, publishing a book can be a mixed blessing. The author works tirelessly for many months (for next to no pay) only to get aggressed – not for factual errors (that would be perfectly alright) or unfounded arguments (that would be welcome) but for allegedly being in it for the money or producing ‘prejudicial propaganda’. In the case of the new book, this had to be expected. I hesitated for an entire decade writing it (hoping someone else would tackle the task) because I knew that it would be far from straightforward to criticize the future king of one’s own country.
All the more reason to take this occasion and thank those who stand by me, who find my book relevant, who agree that it is instructive, and who feel that it deserves a wide readership.
THANK YOU
On 27 January 2022, I conducted a very simple Medline search using the search term ‘Chinese Herbal Medicine, Review, 2022’. Its results were remarkable; here are the 30 reviews I found:
- Zhu, S. J., Wang, R. T., Yu, Z. Y., Zheng, R. X., Liang, C. H., Zheng, Y. Y., Fang, M., Han, M., & Liu, J. P. (2022). Chinese herbal medicine for myasthenia gravis: A systematic review and meta-analysis of randomized clinical trials. Integrative medicine research, 11(2), 100806.
- Lu, J., Li, W., Gao, T., Wang, S., Fu, C., & Wang, S. (2022). The association study of chemical compositions and their pharmacological effects of Cyperi Rhizoma (Xiangfu), a potential traditional Chinese medicine for treating depression. Journal of ethnopharmacology, 287, 114962.
- Su, F., Sun, Y., Zhu, W., Bai, C., Zhang, W., Luo, Y., Yang, B., Kuang, H., & Wang, Q. (2022). A comprehensive review of research progress on the genus Arisaema: Botany, uses, phytochemistry, pharmacology, toxicity and pharmacokinetics. Journal of ethnopharmacology, 285, 114798.
- Nanjala, C., Ren, J., Mutie, F. M., Waswa, E. N., Mutinda, E. S., Odago, W. O., Mutungi, M. M., & Hu, G. W. (2022). Ethnobotany, phytochemistry, pharmacology, and conservation of the genus Calanthe R. Br. (Orchidaceae). Journal of ethnopharmacology, 285, 114822.
- Li, M., Jiang, H., Hao, Y., Du, K., Du, H., Ma, C., Tu, H., & He, Y. (2022). A systematic review on botany, processing, application, phytochemistry and pharmacological action of Radix Rehmnniae. Journal of ethnopharmacology, 285, 114820.
- Mutinda, E. S., Mkala, E. M., Nanjala, C., Waswa, E. N., Odago, W. O., Kimutai, F., Tian, J., Gichua, M. K., Gituru, R. W., & Hu, G. W. (2022). Traditional medicinal uses, pharmacology, phytochemistry, and distribution of the Genus Fagaropsis (Rutaceae). Journal of ethnopharmacology, 284, 114781.
- Xu, Y., Liu, J., Zeng, Y., Jin, S., Liu, W., Li, Z., Qin, X., & Bai, Y. (2022). Traditional uses, phytochemistry, pharmacology, toxicity and quality control of medicinal genus Aralia: A review. Journal of ethnopharmacology, 284, 114671.
- Peng, Y., Chen, Z., Li, Y., Lu, Q., Li, H., Han, Y., Sun, D., & Li, X. (2022). Combined therapy of Xiaoer Feire Kechuan oral liquid and azithromycin for mycoplasma Pneumoniae pneumonia in children: A systematic review & meta-analysis. Phytomedicine : international journal of phytotherapy and phytopharmacology, 96, 153899.
- Xu, W., Li, B., Xu, M., Yang, T., & Hao, X. (2022). Traditional Chinese medicine for precancerous lesions of gastric cancer: A review. Biomedicine & pharmacotherapy = Biomedecine & pharmacotherapie, 146, 112542.
- Wang, Y., Greenhalgh, T., Wardle, J., & Oxford TCM Rapid Review Team (2022). Chinese herbal medicine (“3 medicines and 3 formulations”) for COVID-19: rapid systematic review and meta-analysis. Journal of evaluation in clinical practice, 28(1), 13–32.
- Chen, X., Lei, Z., Cao, J., Zhang, W., Wu, R., Cao, F., Guo, Q., & Wang, J. (2022). Traditional uses, phytochemistry, pharmacology and current uses of underutilized Xanthoceras sorbifolium bunge: A review. Journal of ethnopharmacology, 283, 114747.
- Liu, X., Li, Y., Bai, N., Yu, C., Xiao, Y., Li, C., & Liu, Z. (2022). Updated evidence of Dengzhan Shengmai capsule against ischemic stroke: A systematic review and meta-analysis. Journal of ethnopharmacology, 283, 114675.
- Chen, J., Zhu, Z., Gao, T., Chen, Y., Yang, Q., Fu, C., Zhu, Y., Wang, F., & Liao, W. (2022). Isatidis Radix and Isatidis Folium: A systematic review on ethnopharmacology, phytochemistry and pharmacology. Journal of ethnopharmacology, 283, 114648.
- Tian, J., Shasha, Q., Han, J., Meng, J., & Liang, A. (2022). A review of the ethnopharmacology, phytochemistry, pharmacology and toxicology of Fructus Gardeniae (Zhi-zi). Journal of ethnopharmacology, 114984. Advance online publication.
- Wong, A. R., Yang, A., Li, M., Hung, A., Gill, H., & Lenon, G. B. (2022). The Effects and Safety of Chinese Herbal Medicine on Blood Lipid Profiles in Placebo-Controlled Weight-Loss Trials: A Systematic Review and Meta-Analysis. Evidence-based complementary and alternative medicine : eCAM, 2022, 1368576.
- Lu, C., Ke, L., Li, J., Wu, S., Feng, L., Wang, Y., Mentis, A., Xu, P., Zhao, X., & Yang, K. (2022). Chinese Medicine as an Adjunctive Treatment for Gastric Cancer: Methodological Investigation of meta-Analyses and Evidence Map. Frontiers in pharmacology, 12, 797753.
- Niu, L., Xiao, L., Zhang, X., Liu, X., Liu, X., Huang, X., & Zhang, M. (2022). Comparative Efficacy of Chinese Herbal Injections for Treating Severe Pneumonia: A Systematic Review and Bayesian Network Meta-Analysis of Randomized Controlled Trials. Frontiers in pharmacology, 12, 743486.
- Zhang, L., Huang, J., Zhang, D., Lei, X., Ma, Y., Cao, Y., & Chang, J. (2022). Targeting Reactive Oxygen Species in Atherosclerosis via Chinese Herbal Medicines. Oxidative medicine and cellular longevity, 2022, 1852330.
- Zhou, X., Guo, Y., Yang, K., Liu, P., & Wang, J. (2022). The signaling pathways of traditional Chinese medicine in promoting diabetic wound healing. Journal of ethnopharmacology, 282, 114662.
- Yang, M., Shen, C., Zhu, S. J., Zhang, Y., Jiang, H. L., Bao, Y. D., Yang, G. Y., & Liu, J. P. (2022). Chinese patent medicine Aidi injection for cancer care: An overview of systematic reviews and meta-analyses. Journal of ethnopharmacology, 282, 114656.
- Liu, H., & Wang, C. (2022). The genus Asarum: A review on phytochemistry, ethnopharmacology, toxicology and pharmacokinetics. Journal of ethnopharmacology, 282, 114642.
- Lin, Z., Zheng, J., Chen, M., Chen, J., & Lin, J. (2022). The Efficacy and Safety of Chinese Herbal Medicine in the Treatment of Knee Osteoarthritis: An Updated Systematic Review and Meta-Analysis of 56 Randomized Controlled Trials. Oxidative medicine and cellular longevity, 2022, 6887988.
- Yu, R., Zhang, S., Zhao, D., & Yuan, Z. (2022). A systematic review of outcomes in COVID-19 patients treated with western medicine in combination with traditional Chinese medicine versus western medicine alone. Expert reviews in molecular medicine, 24, e5.
- Mo, X., Guo, D., Jiang, Y., Chen, P., & Huang, L. (2022). Isolation, structures and bioactivities of the polysaccharides from Radix Hedysari: A review. International journal of biological macromolecules, 199, 212–222.
- Yang, L., Chen, X., Li, C., Xu, P., Mao, W., Liang, X., Zuo, Q., Ma, W., Guo, X., & Bao, K. (2022). Real-World Effects of Chinese Herbal Medicine for Idiopathic Membranous Nephropathy (REACH-MN): Protocol of a Registry-Based Cohort Study. Frontiers in pharmacology, 12, 760482.
- Zhang, R., Zhang, Q., Zhu, S., Liu, B., Liu, F., & Xu, Y. (2022). Mulberry leaf (Morus alba L.): A review of its potential influences in mechanisms of action on metabolic diseases. Pharmacological research, 175, 106029.
- Yuan, J. Y., Tong, Z. Y., Dong, Y. C., Zhao, J. Y., & Shang, Y. (2022). Research progress on icariin, a traditional Chinese medicine extract, in the treatment of asthma. Allergologia et immunopathologia, 50(1), 9–16.
- Zeng, B., Wei, A., Zhou, Q., Yuan, M., Lei, K., Liu, Y., Song, J., Guo, L., & Ye, Q. (2022). Andrographolide: A review of its pharmacology, pharmacokinetics, toxicity and clinical trials and pharmaceutical researches. Phytotherapy research : PTR, 36(1), 336–364.
- Zhang, L., Xie, Q., & Li, X. (2022). Esculetin: A review of its pharmacology and pharmacokinetics. Phytotherapy research : PTR, 36(1), 279–298.
- Wang, D. C., Yu, M., Xie, W. X., Huang, L. Y., Wei, J., & Lei, Y. H. (2022). Meta-analysis on the effect of combining Lianhua Qingwen with Western medicine to treat coronavirus disease 2019. Journal of integrative medicine, 20(1), 26–33. https://doi.org/10.1016/j.joim.2021.10.005
The amount of reviews alone is remarkable, I think: more than one review per day! Apart from their multitude, the reviews are noteworthy for other reasons as well.
- Their vast majority arrived at positive or at least encouraging conclusions.
- Most of the primary studies are from China (and we have often discussed how unreliable these trials are).
- Many of the primary studies are not accessible.
- Those that are accessible tend to be of lamentable quality.
I fear that all this is truly dangerous. The medical literature is being swamped with reviews of Chinese herbal medicine and other TCM modalities. Collectively they give the impression that these treatments are supported by sound evidence. Yet, the exact opposite is the case.
The process that is happening in front of our very eyes is akin to that of money laundering. Unreliable and often fraudulent data is being white-washed and presented to us as evidence.
The result:
WE ARE BEING SYSTEMATICALLY MISLED!
On this blog and elsewhere, I have heard many strange arguments against COVID-19 vaccinations. I get the impression that most proponents of so-called alternative medicine (SCAM) hold or sympathize with such notions. Here is a list of those arguments that have come up most frequently together with my (very short) comments:
COVID is not dangerous
It’s just a flu and nothing to be really afraid of, they say. Therefore, no good reason exists for getting vaccinated. This, I think, is easily countered by pointing out that to date about 5.5 million people have died of COVID-19. In addition, I fear that the issues of ‘long-COVID’ is omitted in such discussions
It’s only the oldies who die
As an oldie myself, I find this argument quite distasteful. More importantly, it is simply not correct.
Vaccines don’t work
True they do not protect us 100% from the infection. But they very dramatically reduce the likelihood of severe illness or death from COVID-19.
Vaccines are unsafe
We have now administered almost 10 billion vaccinations worldwide. Thus we know a lot about the risks. In absolute terms, there is a vast amount of cases, and it would be very odd otherwise; just think of the rate of nocebo effects that must be expected. However, the risks are mostly minor, and serious ones are very rare. Some anti-vaxxers predicted that, by last September, the vaccinated population would be dead. This did not happen, did it? The fact is that the benefits of these vaccinations hugely outweigh the risks.
Vaccines are a vicious tracking system
Some claim that ‘they‘ use vaccines to be able to trace the vaccinated people. Who are ‘they‘, and why would anyone want to trace me when my credit card, mobile phone, etc. already could do that?
Vaccines are used for population control
‘They‘ want to reduce the world population through deadly vaccines to ~5 billion, some anti-vaxxers say. Again, who are ‘they‘ and would ‘they‘ want to do that? Presumably ‘they‘ need us to pay taxes and buy their goods and services.
There has not been enough research
If those who make this argument would bother to go on Medline and look for COVID-related research, they might see how ill-informed this argument is. Since 2021, more than 200 000 papers on the subject have emerged.
I trust my immune system
This is just daft. I am triple-vaccinated and also hope that I can trust my immune system – this is why I got vaccinated in the first place. Vaccinations rely on the immune system to work.
It’s all about making money
Yes, the pharma industry aims to make money; this is a sad reality. But does that really mean that their products are useless? I don’t see the logic here.
People should have the choice
I am all for it! But if someone’s poor choice endangers my life, I do object. For instance, I expect other people not to smoke in public places, stop at red traffic lights and drive on the correct side of the street.
Most COVID patients in hospitals have been vaccinated
If a large percentage of the population has been vaccinated and the vaccine conveys not 100% protection, it would be most surprising, if it were otherwise.
I have a friend who…
All sorts of anecdotes are in circulation. The thing to remember here is that the plural of anecdote is anecdotes and not evidence.
SCAM works just as well
Of course, that argument had to be expected from SCAM proponents. The best response here is this: SHOW ME THE EVIDENCE! In response SCAM fans have so far only been able to produce ‘studies’ that are unconvincing or outright laughable.
In conclusion, the arguments put forward by anti-vaxxers or vaccination-hesitant people are rubbish. It is time they inform themselves better and consider information that originates from outside their bubble. It is time they realize that their attitude is endangering others.
We all need cheering up a bit, I’m sure.
Luckily, I found just the thing.
The New York Post reported that a former Versace model, Tom Casey, is crediting his youthful looks to drinking his own urine, and to perineum sunning (exposing your butt hole to sunshine). “I drink my own urine every morning — I call it hair of the dog!” Casey proclaimed, “the feeling is electric.” The ex-model also flushes his urine into his rectum and applies it to his skin as a moisturizer. 
“It wasn’t as bad as the mental barrier in my own mind,” the ex-catwalk star reminisced. “I felt a cool buzz. Intuitively, it just felt good. I drank my urine on and off for a while from there.”
Casey began drinking his own urine on a daily basis back in 2008 and hasn’t looked back. He has even completed a “seven-day urine fast,” drinking nothing but his own urine for an entire week. He also bottles his pee, lets it “ferment” and uses it in an enema. “I would cultivate my own urine and ferment it in a sealed Mason jar for two weeks before transferring it into my rectum,” he explained. “Aged urine enemas are so powerful for your health and I got my six-pack abs after doing them. It flushed out my gut and that’s when I got really ripped.”

Casey uses his urine also as a moisturizer, which he believes helps maintain his appearance. “What it did for my mood and muscle building was amazing. I put it on my skin, especially when I’m on the beach, and it’s so electrifying and strengthening,” he cooed. “It’s a big psychological leap for people to use their own urine as a moisturizer but it’s so euphoric and anti-aging. Uric acid is used in high-end skin care products.”
“I’m 55 years old and most people don’t look and feel like I do at my age. No one can deny that I’m ripped, and that’s down to the fact that I love being extremely healthy and practicing natural healing methods.”
Casey claims Big Pharma is terrified of people learning that the secret to their health lies within themselves.
“What so many pharmaceutical companies don’t want to tell you is that we as humans are the secret to health. That’s what I try to teach people in everything I do,” he stated.
“People should be scared if they’re eating s–tty food and doing pharmaceutical drugs. Why should they be scared to try their own urine?”
____________________________
Personally, I feel that Casey believes the sun might be shining out of his arse. In any case, it is hard to deny that the former Versace model is suffering from proctophasia and/or is taking the piss.
This study assessed the effectiveness of Oscillococcinum in the protection from upper respiratory tract infections (URTIs) in patients with COPD who had been vaccinated against influenza infection over the 2018-2019 winter season.
A total of 106 patients were randomized into two groups:
- group V received influenza vaccination only
- group OV received influenza vaccination plus Oscillococcinum® (one oral dose per week from inclusion in the study until the end of follow-up, with a maximum of 6 months follow-up over the winter season).
The primary endpoint was the incidence rate of URTIs (number of URTIs/1000 patient-treatment exposure days) during follow-up compared between the two groups.
There was no significant difference in any of the demographic characteristics, baseline COPD, or clinical data between the two treatment groups (OV and V). The URTI incidence rate was significantly higher in group V than in group OV (2.9 versus 1.2 episodes/1000 treatment days, difference OV-V = -1.7; p=0.0312). There was a significant delay in occurrence of an URTI episode in the OV group versus the V group (mean ± standard error: 48.7 ± 3.0 versus 67.0 ± 2.8 days, respectively; p=0.0158). Limitations to this study include its small population size and the self-recording by patients of the number and duration of URTIs and exacerbations.
The authors concluded that the use of Oscillococcinum in patients with COPD led to a significant decrease in incidence and a delay in the appearance of URTI symptoms during the influenza-exposure period. The results of this study confirm the impact of this homeopathic medication on URTIs in patients with COPD.
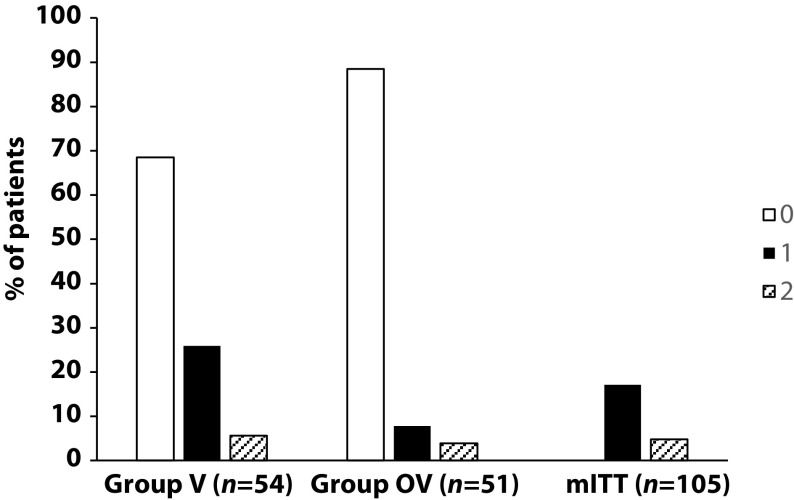
Primary endpoint, comparison of the number of upper respiratory tract infections in the two treatment groups during follow-up
This prospective, randomized, single-center study was funded by Laboratoires Boiron, was conducted in the Pneumology Department of Charles Nicolle Hospital, Tunis, and was written up by a commercial firm specializing in writing for the pharmaceutical industry. The latter point may explain why it reads well and elegantly glosses over the many flaws of the trial.
If I did not know better, I might suspect that the study was designed to deceive us (Boiron would, of course, never do this!): The primary endpoint was the incidence rate of URTIs (number of URTIs/1000 patient-treatment exposure days) in the two groups during the follow-up period. This rate is calculated as the number of episodes of URTIs per 1000 days of follow-up/treatment exposure. The rates were then compared between the OV and V groups. The following symptoms were considered indicative of an URTI: fever, shivering, runny or blocked nose, sneezing, muscular aches/pain, sore throat, watery eyes, headaches, nausea/vomiting, diarrhoea, fatigue and loss of appetite.
This means that there was no verification whatsoever of the primary endpoint. In itself, this flaw would perhaps not be so bad. But put it together with the fact that patients were not blinded (there were no placebos!), it certainly is fatal.
In essence, the study shows that patients who perceive to receive treatment will also perceive to have fewer URTIs.
SURPRISE, SURPRISE!
Yesterday, it was announced that the new German health secretary will be Dr. Karl Lauterbach. This seems a most reasonable choice (when did the UK last have a physician in that post?), and I certainly wish him the best of luck in his new position.
Lauterbach studied medicine at the RWTH Aachen University, University of Texas at San Antonio and University of Düsseldorf, where he graduated. From 1989 to 1992, he studied health policy and management as well as epidemiology at the Harvard School of Public Health in Boston, graduating with a Doctor of Science in 1992. From 1992 to 1993, he held a fellowship at the Harvard Medical School.
From 1998 until 2005, Lauterbach served as the director of the Institute of Health Economics and Clinical Epidemiology (IGKE) at the University of Cologne. He was appointed adjunct professor at the Harvard School of Public Health in 2008. He was a member of the Sachverständigenrat zur Begutachtung der Entwicklung im Gesundheitswesen (the council of experts advising the federal government on developments in the German healthcare system) from 1999 until he was elected to the Bundestag in September 2005.
But why does his appointment put the German defenders of homeopathy in a panic? The reason is simple: Lauterbach has in the past repeatedly argued against the reimbursement of homeopathy in Germany. This is, for instance, what DER SPIEGEL wrote in 2019 (my translation):
SPD parliamentary group vice-chairman Karl Lauterbach wants to prohibit public health insurance companies from reimbursing the costs of homeopathy. “We have to talk about this in the coalition,” he told the “Tagesspiegel”. Health insurance companies in Germany are not obliged to cover the costs of homeopathic treatments. However, they can pay for it voluntarily.
Voluntary benefits by health insurers must also be economically and medically reasonable, Lauterbach argues, referring to a similar push in France. According to the French Supreme Health Authority (HAS), the funds do not have sufficient scientific effect. The Ministry of Health had previously commissioned the HAS with the examination. It is considered likely that the French government will soon abolish the coverage of costs.
“In the spirit of reason and education as well as patient protection, it is also wrong in Germany for insurance companies to pay for homeopathy for marketing reasons,” Lauterbach wrote on Twitter in reaction to the decision in France. His demand is not new. Lauterbach had already spoken out in 2010 for a ban on the assumption of costs.
Many observers expect that Lauterbach – after getting the pandemic under control (not an easy task by any measure) – will indeed stop the reimbursement of homeopathy. Germany’s largest homeopathy producer reacted swiftly and is currently running an expensive campaign with full-page advertisements in German newspapers trying to improve the much-damaged public image of homeopathy:

In the advertisement above, for instance, it is implied that homeopaths are all in favor of vaccination. Regular readers of my blog will know that this is not true…
… and so does Dr. Lauterbach!
Anthony Fauci is the American physician, scientist, and immunologist who serves as the director of the National Institute of Allergy and Infectious Diseases (NIAID) and the Chief Medical Advisor to the President. I have never met him in person but, from all that I know about him, I have great respect for him and his work (he also happens to share with me a John Maddox Prize for standing up for science; he received it in 2020 and I in 2015). Not everyone, however, shares my admiration for Fauci.

This week Lara Logan, a host on Fox News’ streaming platform Fox Nation, confirmed Godwin’s law by comparing Dr. Anthony Fauci to Josef Mengele, the Nazi doctor who performed some of the most horrific experiments on Jewish twins at Auschwitz Concentration Camp during the Third Reich: “This is what people say to me: He doesn’t represent science,” the former “Logan of Fauci, the longtime director of the National Institute of Allergy and Infectious Diseases. He represents Josef Mengele … the Nazi doctor who did experiments on Jews during the Second World War in the concentration camps. And I am talking about people all across the world are saying this! Because the response from COVID. What it has done to countries everywhere. What it has done to civil liberties. The suicide rates. The poverty.”
She made the comment during an appearance on “Fox News Primetime,” following a rant about how there was “no justification for putting people out of their jobs or forcing mandates” for a disease that has death rates “that compare very much to seasonal flu.” (The death rate from COVID-19 is up to 10 times higher than that of most strains of the flu.)
Only hours after the comments by Logan, the Fox News host, Tucker Carlson has compared Dr Anthony Fauci to Italian fascist World War II dictator Benito Mussolini. Holocaust comparisons have become a common feature of protests against COVID-19 strategies. Conservative politicians and media personalities have repeatedly compared vaccine mandates and pandemic restrictions to the treatment of Jews during the Holocaust.
The US is sadly not alone. In Germany and Austria, such comparisons between the atrocities of the Third Reich and COVID vaccinations have become common too. In Germany, this has gone so far that the judiciary is now taking action against people who compare Corona politics with the crimes of Nazis.
Personally, I find these comparisons not just stupid but despicable, and I agree that they should be outlawed. Journalists, in particular, must know that by employing this type of rhetoric, they act against all decency and undermine our efforts to protect the public from the pandemic. I, therefore, feel that Logan, Carlson, and anyone else who descends that low should be prosecuted.
“There is a battle raging for humanity”, claims Dr Carrie Madej, a US osteopathic doctor (in the US, osteopaths are [almost] conventional physicians). She thinks she has discovered how Big Tech collaborates with Big Pharma introduced new technologies in the coming vaccines, that will alter our DNA and turn us into hybrids. This, she submits, will end humanity as we know it, and start the process of transhumanism: HUMAN 2.0 They use vaccines to inject nanotechnology into our bodies and connect us to the Cloud and artificial intelligence. This will enable corrupt governments and tech giants to control us, without us being aware of it.

Dr. Carrie Madej is from Dearborn, Michigan, and received her medical degree from Kansas City University of Medical Biosciences in 2001. She then completed her traditional internship at The Medical Center in Columbus, Georgia, and internal medicine residency at Mercer University in Macon Georgia. Dr. Madej served as a private clinician and medical director of clinics in Georgia until 2015. Dr. Madej also served as an attending physician for the Pennsylvania College of Osteopathic Medicine. She has served as a public speaker and was featured in the documentary, “The Marketing of Madness” about the overuse of prescription psychotropic medicines. Dr. Madej now dedicates her time educating others on vaccines, nanotechnology, and human rights via multiple platforms and speaking engagements.
IN HER NEWEST SCORCHED EARTH DISCUSSION, Dr. Carrie Madej simply Can NOT stay silent about the ABSOLUTE DANGERS of the Covid-19 “vaccines” any longer! In fact, in this SCATHING PRESENTATION, she literally describes the ‘Killer Concoctions’ as ‘THE FRANKENSTEIN CODE” and HAMMERS the ‘Purveyors of the Poison Jab’ as ‘Murdering Psychopath Witch Doctors’ who are HELL BENT on the TOTAL DESTRUCTION & ANNIHILATION of the ENTIRE HUMAN RACE, as we know it today.
The ‘Kung Flu’ (as it’s been referred to by none other than POTUS Trump), is only ‘KILLING PEOPLE who are already suffering from cancer, diabetes, heart disease and a plethora of other autoimmune problems’ – so now WHY IN THE WORLD IS EVERYBODY being told to get the ‘Killer Jab’ when the risk of DIRE & GROTESQUE INJURY FAR OUTWEIGHS the risk of dying from Covid-19 or the fake Delta Variant, or Beta, or Gamma or WHATEVER ELSE THE DEMONIC FAUCI & GATES CONCOCT NEXT?! Get ready for a BEATING unlike you’ve seen in recent days, as Dr. Madej RIPS THE THROATS straight out of these Deep State Demons in this ‘DO NOT MISS’ Epic Video! Grab the popcorn, and get ready for a trip down the Rabbit Hole and a takedown of Satan’s Army!
This was published by the ‘REPUBLIC BROADCASTING NETWORK’ (RBN) who also published articles such as ‘Who are the Jews behind the coronavirus vaccines?‘
Dr. Carrie Madej is certainly no fan of COVID vaccines: Doctor Carrie Madej says she personally examined multiple vials of the vaccines that are being forced into people’s arms, and she was horrified by what she saw. She says she cried harder than she ever has before. Elsewhere she explained in detail:
“First it looked just translucent. And then as time went on, over two hours, colors appeared. I had never seen anything like this. There wasn’t a chemical reaction happening. It was a brilliant blue, and royal purple, yellow, and sometimes green,” she said.
She later shared that when she asked nanotech engineers what the emerging brilliant colors might come from, the engineers said the “only thing they knew that could do that” was a white light, over time, causing a reaction on “a super-conducting material.” In this case, Madej noted, white light came from the microscope itself.
She pointed out that an example of a super-conducting substance would be “an injectable computing system.”
Madej went on, “These fibers were appearing more and more. Some of the fibers had a little cube structure on them, I’m not sure what that was. And also metallic fragments were in there. They were not metallic fragments I’m used to seeing. They were exotic. They were very opaque.”
In time, Madej said, “all the particulates, all these colors started moving to the edge” of the cover slide. “There was self-assembling going on, things were growing. They looked synthetic.”
Madej noticed something else quite strange: “There was one particular object or organism, I’m not sure what to call it, that had tentacles coming from it. It was able to lift itself up off of the glass slide. It appeared to be self-aware, or to be able to grow or move in space.”
She found it disturbing but said she thought, “Maybe that was a fluke in a way, maybe that was just that one vial.”
Some time later, the same lab obtained more vials from a different batch of Moderna shots, as well as a J&J vial. Madej was concerned to see the same things she had observed in the first vial.
“Another one of those tentacle-like structures appeared,” she said. “This was now completely under the cover slip, so there was no movement because it wasn’t on the edge, but I just couldn’t believe I saw another one. Same thing.” Madej also saw the “same colors” appear over time, as well as the fibers.
In the J&J vial, Madej said, there was “definitely a substance that looked like graphene. They all had graphene-like structures in there. Whether or not they were, I don’t have the capability of testing them in order to know at this lab, but that’s what they appeared to be.”
The vial’s contents also had “fatty substances, a sticky glue-like substance that would be considered a hydrogel in those, both of them.”
The J&J vial “also had colors appear.” “Their colors were different, like a fluorescent pastel kind of color. Again, a lot of synthetic structures in there as well.” Madej also noticed many “spherical ring structures” in the J&J contents.
“I’ve never seen anything like this before. They’re not supposed to be in these injections. What are they going to do to somebody? What are they going to do to a child? I started crying when I saw these the second time under a microscope, because it was confirmation of everything I saw the first time,” Madej said.
Madej again appeared on the Stew Peters show on October 20 to discuss her findings from a Pfizer jab vial as well as another J&J vial. “What I’m seeing in all of these manufacturers are synthetic substances, graphene-like, also these nano-carbon tubes,” Madej said.
“In this particular J&J” vial, Madej saw “round spheres, which were not air bubbles.” She continued, “There’s many of these rings, and as time went on they would get thinner and thinner and expand out and then finally extrude out some gelatinous material — I’m not sure what it was, but different kinds of things were inside these spheres. So they’re almost like a delivery structure, that’s what they were doing.”
On one of these rings, Madej saw what “looked like a translucent organism that went around, and back and forth.” Madej first “thought it was another water parasite,” but after continuing to observe its movements, “thought perhaps it was moving in a more robotic way.”
Madej saw the “same kind of synthetic things” in the Pfizer jab, as well as “something that looks similar to teslaphoresis. That’s when these little graphite-like black, metallic particles start to coalesce into strings, like a spider web. They do that through any external force — it could be light, it could be a magnetic force, it could be an impulse, like a frequency. Anyhow, all these little particles would then coalesce and form their own neural network, or their own fibers, or wires.”
After listening to Madej’s findings and seeing the photo and video documentation she provided, Peters commented, “It’s like I’m watching a seriously bad B-movie, a horror thriller.”
Madej believes the tentacled entity she found in the Moderna jabs has a connection with the organism hydra vulgaris. “It is one of the model organisms that the transhumanists like to study and look at. They feel that this is an amazing organism for humanity,” said Madej, in part because “it’s immortal in the lab setting” and “continuously produces its own stem cells.”
“It never stops. You can chop it up into little bits, put it in a petri dish and it forms itself again and again,” she continued. “They’re thinking, wouldn’t this be great if we could put this inside of a human body’s genome, and then if your hand was chopped off by a trauma, you could grow a new hand.”
My friend Joe Schwarcz recently wrote a brilliant article about Dr. Madej. He concluded by asking: Is Dr. Madej a maddeningly malicious malfeasant, or does she just have a few loose marbles? I fear that it might be both.
Medscape and Ernst deserve each other. What a sad old fellow, desperate to live down his homeopathic past by producing a steady stream of deeply prejudicial anti-homeopathy propaganda. What kind of person dedicates his life to hate speech against the second most popular medical therapy worldwide? No doubt, he’s convinced himself that it’s a noble endeavor. Sad and comical.